


Abstract
This study assessed the clinical performance of a combined PET/CT system using 18F-FDG in oncologic patients. Methods: 18F-FDG PET/CT was used to evaluate 204 patients with 586 suspicious lesions. All patients had available follow-up data, enabling assessment of the clinical significance of hybrid PET/CT findings. Differences in interpretation between PET, CT, and fused PET/CT data were prospectively documented for detection, localization, and characterization of each evaluated site. The additional value of PET/CT for data interpretation over that of separate PET and CT was classified into several criteria, including change in lesion characterization to either definitely benign or definitely malignant, precise anatomic localization of malignant 18F-FDG uptake, and retrospective lesion detection on PET and CT. The clinical impact of information provided by PET/CT on patient management was assessed on the basis of follow-up data concerning further diagnostic or therapeutic approach. Analysis of data was performed for the whole study population, for different types of cancer, and for different anatomic sites. Results: PET/CT provided additional information over the separate interpretation of PET and CT in 99 patients (49%) with 178 sites (30%). PET/CT improved characterization of equivocal lesions as definitely benign in 10% of sites and as definitely malignant in 5% of sites. It precisely defined the anatomic location of malignant 18F-FDG uptake in 6%, and it led to retrospective lesion detection on PET or CT in 8%. The results of PET/CT had an impact on the management of 28 patients (14%). Hybrid PET/CT data obviated the need for further evaluation in 5 patients, guided further diagnostic procedures in 7 patients, and assisted in planning therapy for 16 patients. Conclusion: Hybrid PET/CT improves the diagnostic interpretation of 18F-FDG PET and CT in cancer patients and has an impact on both diagnostic and therapeutic aspects of patient management.
Over the last 2 decades, 18F-FDG PET has dramatically increased the accuracy of metabolic mapping of numerous malignancies, with significant impact on the management of cancer patients at different stages of their disease (1–3). Discrepancies between the functional information provided by 18F-FDG PET and morphologic information of conventional imaging procedures have indicated that changes in size or texture of tissues and organs cannot be used as the sole expressions of malignancy (4,5). PET, on the other hand, is inferior to conventional imaging in terms of spatial resolution and localization of abnormalities. The absence of clear anatomic landmarks is a disadvantage of PET, hampering its diagnostic usefulness (6,7). Identification of regions of normal biodistribution of 18F-FDG is usually helpful for anatomic orientation but is neither optimal nor as accurate as CT.
Correlating information from 2 different imaging modalities is important for improving the diagnostic results of both tests (8–11). The recognition of the complementary role of morphologic and functional imaging has motivated the search for optimized integration of 2 different sets of imaging data. Coregistration of separately performed imaging procedures has been successful for the brain. For other parts of the body, coregistration poses a greater challenge because of changes in patient position and in organ content and location between the 2 procedures. In addition, time-consuming, complicated fusion models and algorithms made such techniques clinically impractical (12).
The recent development of a hybrid PET/CT scanner for the simultaneous acquisition of anatomic (CT) and functional (PET) data overcomes technical hardships and offers image fusion for routine clinical practice (12–14). This study presents the initial evaluation of the clinical performance of the PET/CT system in oncologic patients. The study assesses the additional value of hybrid PET/CT data, over that of separate PET and CT, for improving diagnostic imaging and cancer patient management.
MATERIALS AND METHODS
Patient Population
Two hundred four consecutive patients with suspected or known malignancy, evaluated by 18F-FDG imaging using a combined PET/CT system (Discovery LS; General Electric Medical Systems) between June 2001 and March 2002, who had available follow-up data to assess the clinical significance of hybrid PET/CT findings, were included in the study. The PET/CT device is the only current available PET imaging device at our institution and is always used as a combined system for 18F-FDG imaging. The Institutional Review Board of the hospital approved the study, and each patient signed a written informed consent form.
Patients included 93 women and 111 men with a mean age of 59 y (range, 5–89 y). Sixty-four patients had lung cancer, 34 had gastrointestinal tumors, 33 had lymphoma, 16 had genitourinary tract malignancies, 13 had breast cancer, 10 had skin tumors, 5 had sarcoma, and 4 had cancer of the head and neck. Two patients each had neuroendocrine cancer or metastatic disease of unknown origin and 1 patient had a mesothelioma. Twenty patients with no prior history of malignancy were referred for further evaluation of a single pulmonary nodule (SPN) seen on CT. 18F-FDG was performed for initial staging in 35 patients and for restaging of recurrent malignancy in 11 patients. Twenty patients had 18F-FDG performed to assess cancer response to therapy. In 118 patients, 18F-FDG was performed after therapy as a routine follow-up procedure or for further evaluation of suspected recurrence.
Six hundred eight suspicious sites were evaluated in the 204 included patients. Twenty-two of the 608 sites evaluated were excluded from analysis because the final diagnosis in these sites could not be confirmed. The final study group therefore included 204 patients with 586 suspicious sites. Thirty-seven lesions were located in the head and neck region, 293 in the chest, 147 in the abdomen and pelvis, and 109 were soft-tissue and skeletal sites. The mean number of lesions per patient was 3.1 (range, 1–16 lesions); 59 patients had a single suspicious site.
Imaging Protocol
Patient Preparation.
Patients were instructed to fast for 4 h before injection of 18F-FDG (except for glucose-free oral hydration). Blood glucose was measured before injection of the tracer to ensure glucose blood levels of <11.1 mmol/L. The injection dose of 18F-FDG ranged between 370 and 555 MBq (10–15 mCi) in adults and was weight-adjusted in children (5.3 MBq/kg [0.144 mCi/kg]). After injection, patients were kept lying comfortably. No urinary bladder catheterization was performed and no oral muscle relaxants were administered.
Acquisition Protocol.
The hybrid PET/CT system used to perform 18F-FDG imaging combines a third-generation multislice spiral CT with a dedicated full-ring bismuth germanate PET scanner. For PET/CT acquisition, the CT scanner with a transaxial field of view (FOV) of 50 cm and is operated in 4-slice helical mode with a rotational speed of 0.8 s per 360°. The x-ray tube is operated with a voltage peak of 140 kV, 80 mA, 6:1 pitch, with slice thickness of 4.25 mm. The PET scanner has a transaxial FOV of 55 cm and an axial FOV of 15.2 cm, with 35 image slices at an axial sampling of 4.25 mm per slice. PET scanning is performed in a 2-dimensional mode for 5 min per FOV.
The PET and CT components share a common table. The centers of the FOV of PET and CT are offset axially by 68 cm. The entire system is housed within a single casing with a common path, 110-cm-long tunnel, which narrows down from 70 cm at the CT side to 60 cm at the PET side. Three positional laser beam sources provide external and internal landmark definition. Patient positioning is performed only once before acquisition of both modalities. The positional information of the table and patient is shared for both the CT and PET acquisitions to ensure proper registration of the 2 images. Two translation mechanisms of the table prevent differential vertical deflections of the table between the CT and PET acquisition planes. Accurate mechanical alignment is ensured during installation, by acquiring a dedicated phantom with multiple landmarks, which appear in both the CT and PET studies. The system image alignment is within 1.3 mm at the center and 2.0 mm at 20 cm from the center of the FOV in the x-, y-, and z-directions. Optimized reconstruction parameters can compensate for any residual mechanical misalignment. Both PET and CT are operated from an integrated console using a single extended keyboard and mouse.
PET/CT scanning is started 60 min after 18F-FDG injection. The protocol includes an initial CT acquisition with no administration of oral or intravenous contrast agents, followed by the PET scan. Imaging is performed with the patient breathing normally during both parts of the procedure. The patient’s arms are positioned above the head, unless head and neck lesions are known or suspected or patients are unable to hold this position for the whole study period. The radiation dose for the patient from the CT is about 5 mGy (500 mrad) for a routine clinical protocol, which is about 20% of the typical radiation dose of a diagnostic CT scan. After completing the CT, the table is moved toward the FOV of the PET, and PET acquisition of the same axial range is initialized with the patient in the same position on the table.
Processing Protocol.
The CT images are acquired and reconstructed using optimized parameters for attenuation correction. Data obtained from the CT acquisition are used for low-noise attenuation correction of PET emission data and for fusion of attenuation-corrected PET images with the corresponding CT images. CT Hounsfield units are converted into 511-keV attenuation coefficients, using a special bilinear conversion algorithm. PET images are reconstructed using ordered-subset expectation maximization software, with measured CT attenuation correction.
After completion of PET acquisition, the reconstructed attenuation-corrected PET images, CT images, and fused images of matching pairs of PET and CT images are available for review in axial, coronal, and sagittal planes and in maximum-intensity projections, 3-dimensional cine mode, using the manufacturer’s review station (eNTegra; General Electric Medical Systems). The reconstructed PET and CT images are displayed using a matrix of 128 × 128 pixels for the PET and 512 × 512 pixels for the CT. Fused images are displayed on a matrix of 128 × 128 for coronal and sagittal images and 512 × 512 for the transaxial images, with PET images in a predefined color map on top of the gray-scale CT.
Data Interpretation
Data generated after the PET/CT acquisition, including 18F-FDG PET, CT, and fused PET/CT images of the same body range, were reviewed directly from the computer screen of the workstation. Independently performed high-resolution contrast-enhanced CT scans, obtained up to 2 mo before the PET/CT, were also reviewed. Any site questioned as possibly malignant on physical examination, CT, or PET was defined as a suspicious site. Two experienced nuclear medicine physicians, aware of patient clinical history and results of previously performed conventional imaging tests, including the diagnostic CT study, initially interpreted the stand-alone 18F-FDG PET images. The presence and localization of any area of increased 18F-FDG uptake and its characterization as benign, malignant, or equivocal were recorded prospectively. A site of increased 18F-FDG uptake was defined as benign when related to physiologic biodistribution of 18F-FDG or to a known nonmalignant process. Any area of focal 18F-FDG activity, of intensity higher than that of surrounding tissues, not related to normal physiologic or benign 18F-FDG uptake, was defined as malignant. Any other area of increased 18F-FDG uptake that could not be clearly characterized was defined as an equivocal site on PET. Two experienced radiologists, aware of the patient’s history and clinical data, but blinded to current 18F-FDG PET results, reviewed the separately performed diagnostic CT and the CT component of the PET/CT study and compared them to previous studies when available. A combined team of nuclear medicine physicians and radiologists interpreted the fused PET/CT images thereafter. Fused PET/CT data were prospectively recorded using the same criteria as for PET, including characterization and localization of all suspicious sites. Disagreements concerning final interpretation were resolved by a majority opinion for PET, CT, and PET/CT images.
Data Analysis
Differences in interpretation between PET, CT, and fused PET/CT data were prospectively documented for detection, localization, and characterization of each suspicious site. The principal advantage of fusion of PET and CT images is its ability to accurately localize abnormal 18F-FDG uptake detected on the PET study to anatomic structures defined by CT. The additional value was defined as new information provided by PET/CT, not previously gleaned from separate PET or CT studies, resulting in a change in image interpretation. The additional diagnostic value of PET/CT was therefore assessed by the combined team of experts using one or more of the following criteria regarding changes in image interpretation: (a) Characterization of a suspicious site, previously considered malignant or equivocal on PET stand-alone, as physiologic or benign. (b) Characterization of a suspicious site, previously considered benign or equivocal on PET stand-alone, as malignant. (c) Change in the anatomic localization of abnormal 18F-FDG uptake considered malignant on PET stand-alone. (d) Retrospective detection of a lesion previously missed on PET. (e) Retrospective detection of a lesion previously missed on CT.
Analysis of the changes in PET and CT interpretations attributed to the fused PET/CT data was performed on a per-patient and per-site basis. The additional value of PET/CT imaging was assessed for the whole study group, for different types of cancer, for different anatomic regions, and for different time points of evaluation in relation to the course of disease.
The clinical impact of PET/CT data was evaluated by the combined team of experts, with respect to alterations in further patient management attributed to the additional information provided by the hybrid imaging results. Modifications in the diagnostic approach included sparing or guiding further diagnostic procedures. Therapeutic modifications of the surgical, chemotherapy, or radiotherapy strategy included replacing a previously planned therapeutic modality by a different one or optimizing a previously considered treatment protocol.
Statistical Analysis
We used the χ2 test to determine the type of malignancy and the region of the body for which the additional value of PET/CT was most significant and the relationship of additional data obtained from PET/CT to different time points of evaluation during the course of disease. P values < 0.05 were considered statistically significant.
RESULTS
The additional value of combined PET/CT for image interpretation and its clinical impact on patient management was assessed in 204 patients with 586 suspected sites by comparing PET/CT data with those from separate PET and CT studies (Fig. 1).

Summary of data: additional value of PET/CT for single-step detection of malignancy, definition of its location and extent, and improved management.
Impact of PET/CT on Image Interpretation
Image interpretation using PET/CT provided additional information beyond that provided by the separate interpretations of PET and the contrast-enhanced diagnostic CT in 99 patients (49%). Hybrid PET/CT imaging resulted in changes in lesion detectability, localization, and characterization of 178 sites (30%). The presence or absence of malignancy was confirmed by histopathology in 24 of the sites and by further clinical follow-up and imaging data (including CT, MRI, and bone scintigraphy) in 154 sites. The mean follow-up period for benign sites was 6.7 mo (range, 3–12 mo).
Site-Based Analysis.
The site-based analysis of the additional value of fused PET/CT over PET or CT alone is presented in Table 1. Data derived from hybrid imaging led to a change in interpretation of PET in 115 sites, of CT in 43 sites, and of both PET and CT in 20 sites. PET/CT results led to changes in interpretation of 61 of 147 sites in the abdomen and pelvis (41%), of 12 of 37 sites in the head and neck (32%), of 34 of 109 sites in soft tissues or bone (31%), and of 71 of 293 sites in the chest (24%). The impact of PET/CT on the diagnostic interpretation was significantly greater for abdominopelvic sites (41%) than for any other sites (P < 0.003).
Site-Based Analysis of Changes in Image Interpretation After PET/CT
The additional value of PET/CT for data interpretation over that of separate PET and CT was classified into several criteria. (Table 1). PET/CT led to a change in characterization of 91 of the 586 evaluated sites (16%):
(a) Characterization of a suspicious site as definitely benign: Sixty sites of increased 18F-FDG uptake (10%), previously considered malignant or equivocal on PET, were defined as benign using fused data. These included 34 sites in the chest, 19 of them foci of increased 18F-FDG activity precisely localized to physiologic uptake in hilar or mediastinal vessels. Sixteen sites were located in the abdomen and pelvis, 8 sites in soft tissues or bone, and 2 in the head and neck. Fifty-seven of these 60 sites (90%) were confirmed as benign on further imaging and clinical follow-up (Fig. 2). Three sites of increased 18F-FDG uptake were falsely interpreted as benign on the basis of PET/CT fused data. One site of uptake at the gastroesophageal junction was localized by fused images to a region of hiatal hernia but was found by biopsy, several weeks later, to represent esophageal cancer. Two other sites in the chest wall and lung hilus, defined by fused images as postsurgical changes and hilar blood vessels, were diagnosed as local recurrence and metastatic adenopathy, respectively, 4 mo later.
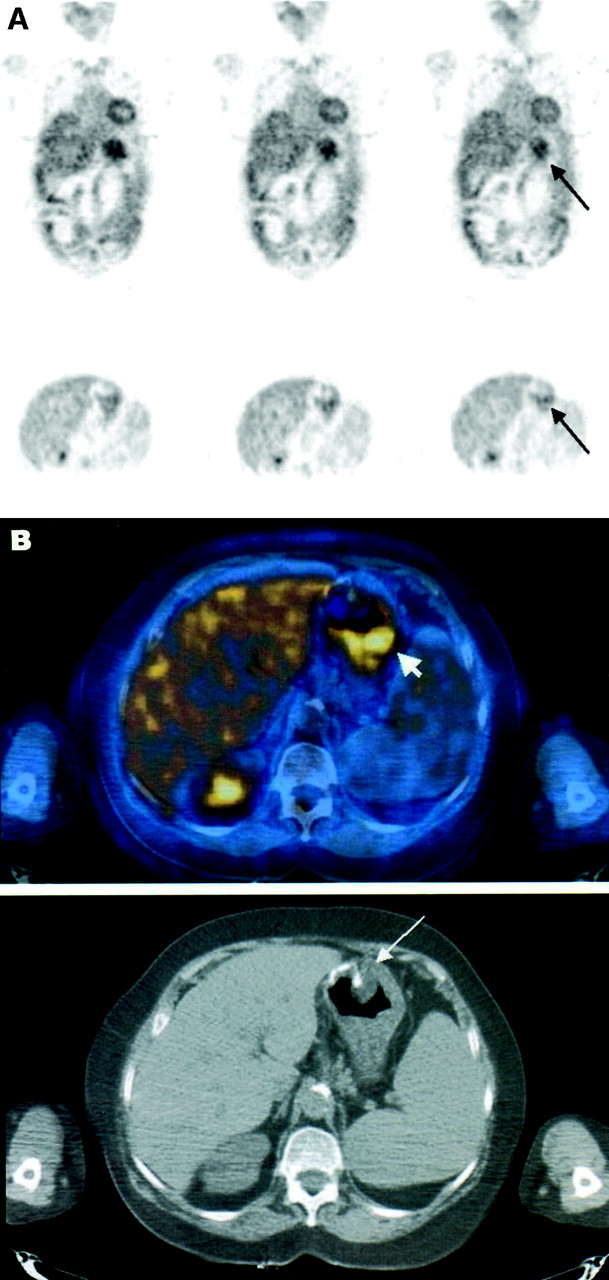
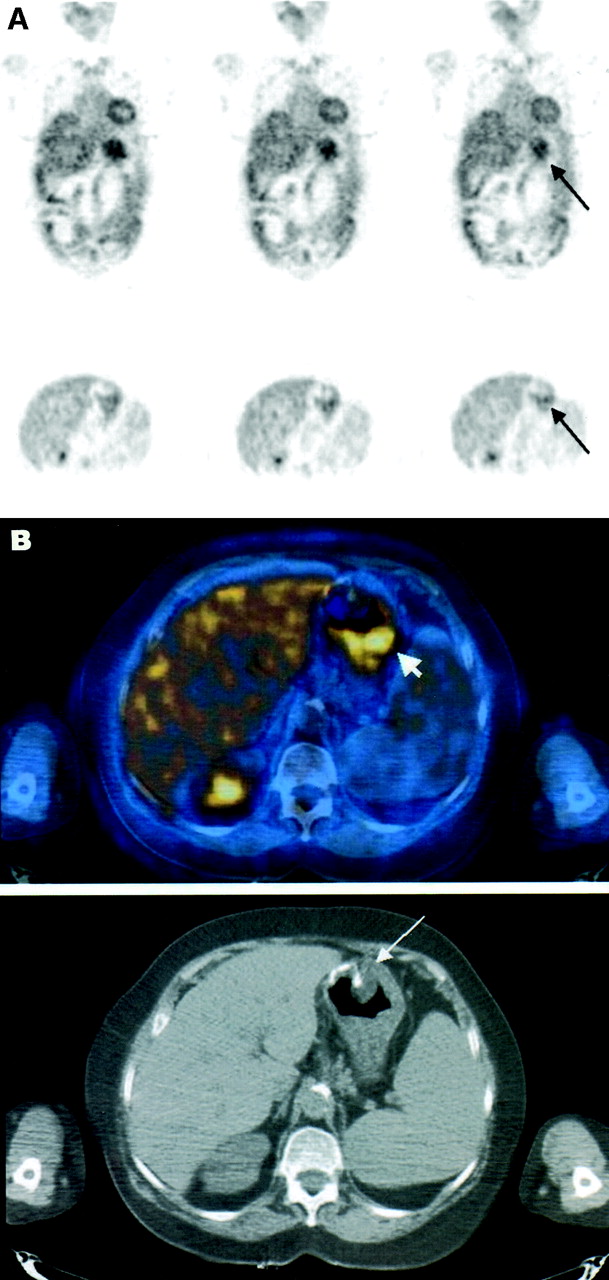
Precise localization of increased 18F-FDG uptake and exclusion of malignancy, after PET/CT. A 68-y-old man, 3 y after partial gastrectomy for adenocarcinoma of stomach, was referred for 18F-FDG PET/CT for further evaluation of polypoid mass in gastric stump detected on routine follow-up gastroscopy, with equivocal biopsy results. (A) 18F-FDG PET coronal images (top) and axial images (bottom) show increased 18F-FDG uptake in region of stomach (arrow). (B) Hybrid PET/CT axial image (top) precisely localizes and defines uptake as physiologic activity at gastric stump (arrowhead). Suspicious polypoid mass in anastomotic region (arrow), seen on corresponding hybrid and CT slices (bottom) obtained during same acquisition, shows no uptake of 18F-FDG. Findings on PET/CT were interpreted as physiologic 18F-FDG uptake in stomach and nonviable residual mass. Patient showed no evidence of disease for follow-up of 7 mo.
(b) Characterization of a suspicious site as definitely malignant: Thirty-one sites of increased 18F-FDG uptake (5%), previously considered benign or equivocal on PET alone, were characterized as definitely malignant after reviewing the PET/CT study (Fig. 3). Fourteen of these 31 lesions (45%) were abdominopelvic sites, most of them initially interpreted as physiologic 18F-FDG uptake in the gastrointestinal tract, 10 chest sites, 5 head and neck sites, and 2 skeletal sites. Cancer was confirmed in 29 of these 31 sites. Two sites of abnormal mediastinal and cervical uptake, initially considered benign or equivocal on PET alone, were incorrectly interpreted as malignant on PET/CT after being localized to a cluster of mediastinal lymph nodes, and to normal-sized cervical lymph nodes, and showed no evidence of disease on follow-up of 7 and 12 mo, respectively.
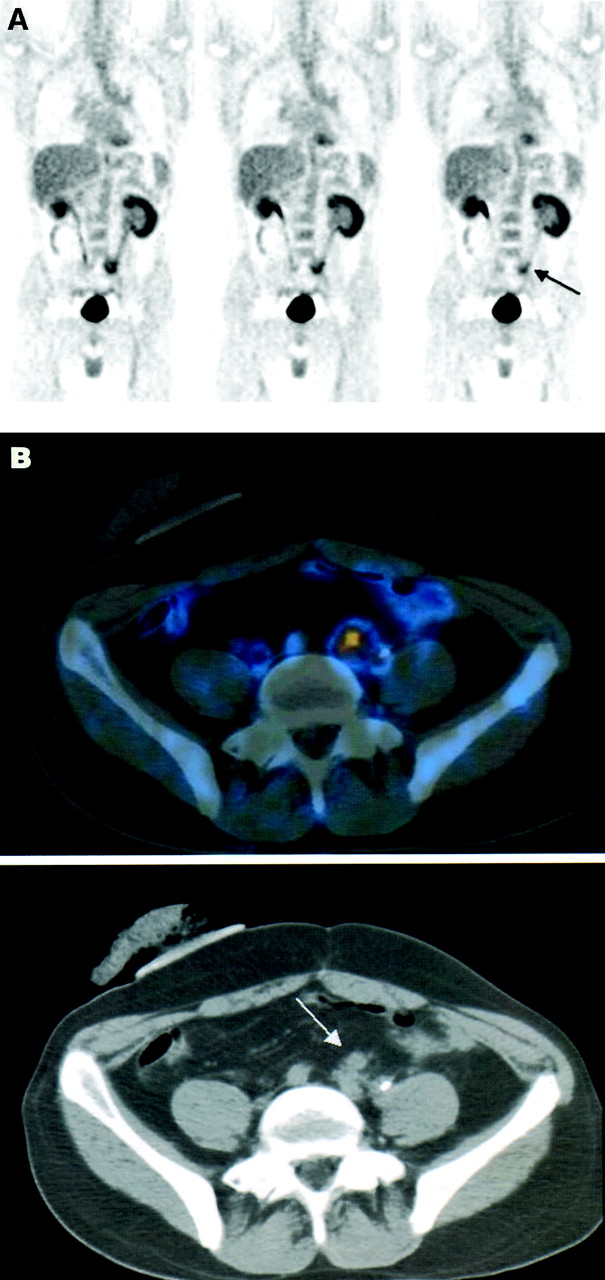
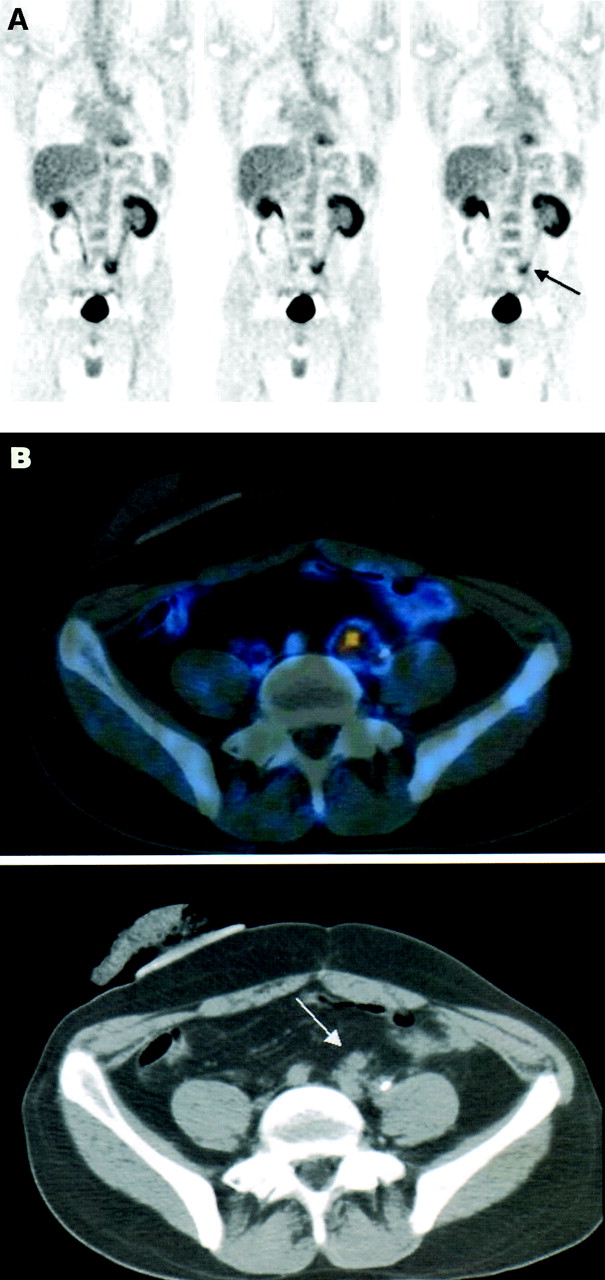
Precise characterization of increased 18F-FDG uptake and retrospective lesion detection on CT, after PET/CT. A 35-y-old man, 22 mo after treatment for colon cancer, with negative high-resolution contrast-enhanced CT and normal levels of serum tumor markers, was referred for 18F-FDG PET for further assessment of pelvic pain. (A) Coronal PET images show area of increased 18F-FDG uptake in left pelvic region (arrow), interpreted as equivocal for malignancy, possibly related to inflammatory changes associated with ureteral stent or to physiologic bowel uptake. (B) Hybrid PET/CT axial image (top) precisely localizes uptake to soft-tissue mass adjacent to left ureter, anterior to left iliac vessels. Mass (arrow) was detected only retrospectively on both diagnostic CT and CT component of hybrid imaging study (bottom). Patient received chemotherapy, resulting in pain relief and decrease in size of pelvic mass on follow-up CT.
(c) Precise anatomic localization of a site of malignant 18F-FDG uptake: Hybrid PET/CT imaging changed the anatomic localization of 37 sites of abnormal 18F-FDG uptake (6%) considered as definitely malignant lesions by PET alone (Fig. 4). These included 17 abdominopelvic sites, 12 sites in the chest, and 8 soft-tissue or skeletal sites. Cancer was confirmed in 35 of the 37 sites. In 2 sites there was no evidence of disease on further imaging and clinical follow-up of 8 mo.
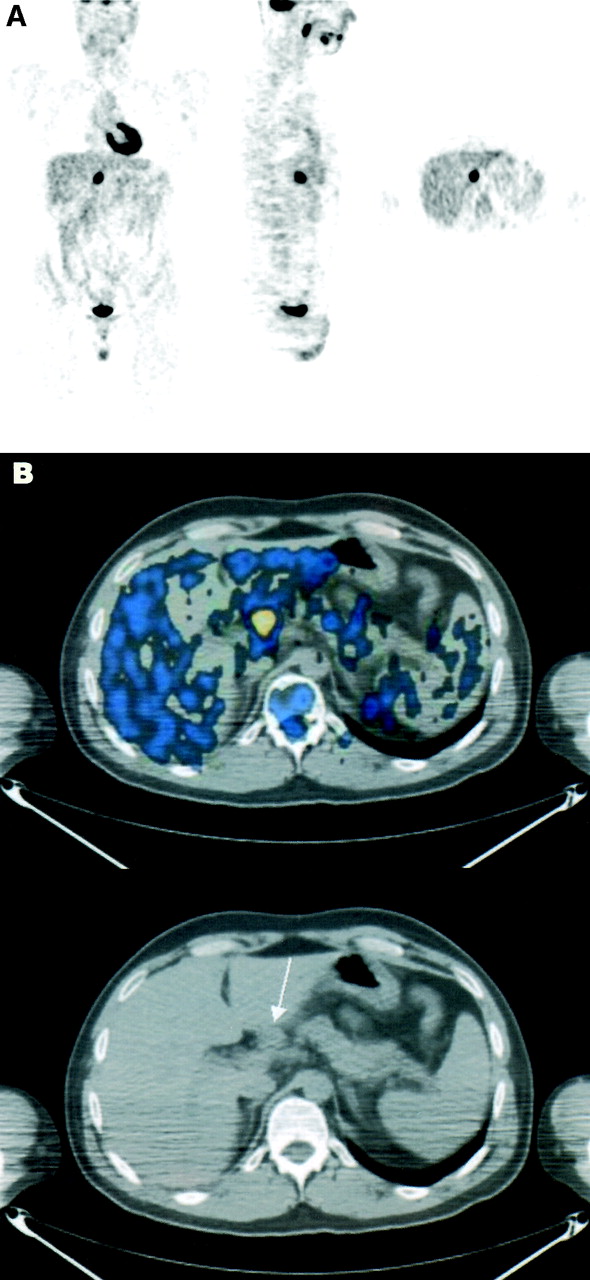
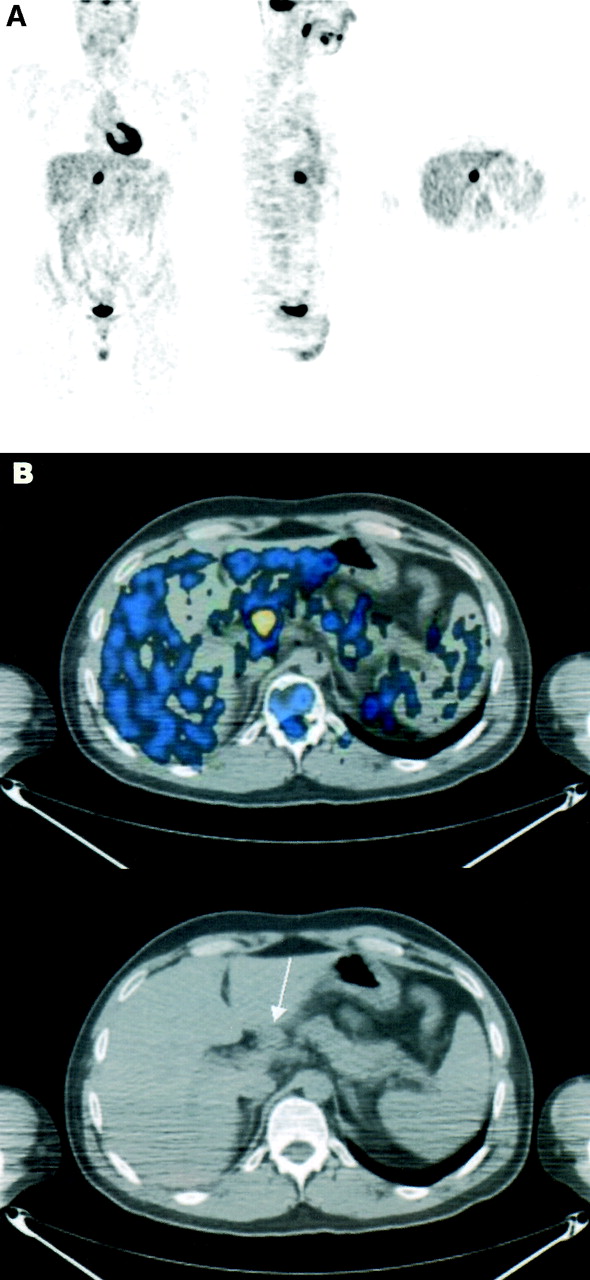
Precise anatomic localization of malignant 18F-FDG uptake and retrospective lesion detection on CT, after PET/CT. A 33-y-old man with Hodgkin’s disease in left cervical region was referred for 18F-FDG PET for staging. No other sites of disease were reported on CT. (A) PET images show infradiaphragmatic focus of abnormal 18F-FDG uptake in medial border of liver, consistent with either liver involvement (stage IV disease?) or nodal disease in porta hepatis (stage III disease?). (B) Hybrid PET/CT axial image (top) precisely localizes 18F-FDG uptake to adenopathy at porta hepatis, only retrospectively detected on corresponding CT image (bottom) (arrow). Patient was treated as having stage III disease and achieved complete response, showing no evidence of disease for follow-up of 12 mo.
(d) Retrospective detection of a lesion on PET: Seven sites (1%) were retrospectively detected on PET after reviewing PET/CT data, including 2 sites in the oropharynx, 3 pulmonary nodules, and 1 site each of subcarinal and iliac adenopathy. Five of these sites were confirmed as malignant. There was no evidence of malignancy in 2 sites on follow-up of 9 and 14 mo, respectively.
(e) Retrospective detection of a lesion on CT: Sixty-three sites (11%) were detected on diagnostic CT and on the CT component of PET/CT imaging, only retrospectively, after evaluation of the fused PET/CT images (Figs. 3 and 4). The anatomic distribution included 21 sites in the abdominopelvic region, 19 in the chest, 17 soft-tissue and skeletal sites, and 6 sites in the head and neck. In 43 of these sites (7% of all sites), PET/CT data affected only the interpretation of CT, whereas in the remaining 20 sites fusion was beneficial for the interpretation of both PET and CT (Table 1).
Overall, of 178 sites in which PET/CT changed the initial diagnostic interpretation of PET and CT, fusion data were accurate in 169 sites. In only 9 sites (1.5% of all sites evaluated, 5% of the 178 sites) were the changes in interpretation attributed to PET/CT data found to be erroneous.
Patient-Based Analysis.
Patient-based analysis showed that PET/CT provided additional information beyond that provided by the separate interpretations of PET or CT in 99 of the total number of patients (49%). These 99 studies included 89 of 146 positive PET studies (60%) and 10 of 58 negative PET studies (17%). PET/CT was of additional value for image interpretation in 23 of 34 patients with primary gastrointestinal tumors (68%), in 42 of 84 patients with an SPN and lung cancer (50%), and in 12 of 33 patients with lymphoma (36%). The impact of PET/CT on diagnostic interpretation was significantly greater for patients with gastrointestinal malignancies than for patients with any other malignancy (P < 0.05).
PET/CT was of additional value in imaging interpretation in 5 of 20 patients referred for diagnosis of malignancy (25%), in 22 of 46 patients referred for staging or restaging (48%), in 8 of 20 patients referred for assessment of therapy response (40%), and in 64 of 118 patients evaluated during follow-up (54%). There was no statistically significant difference in the number of studies showing an additional value of PET/CT in patients evaluated at different time points during the course of disease.
Clinical Impact of PET/CT on Patient Management
PET/CT results had an impact on the management of 28 of the 204 patients (14%) evaluated. This included 12 patients with lung cancer or an SPN, 8 with colon cancer, and 8 patients with other tumors. Six of the 28 patients were evaluated for staging, 2 during therapy, and 18 for suspected recurrence. Changes in management were induced by changes in PET interpretation in 16 patients, by modification of CT reports in 2 patients, and by different review of both PET and CT in 10 patients.
The additional information provided by PET/CT obviated the need for further evaluation of 5 patients with equivocal findings on PET stand-alone. PET/CT localized these suspicious sites of 18F-FDG uptake to hilar vessels in 3 patients, to a calcified abdominal aorta in 1 patient, and to physiologic gastric activity in 1 patient. Four of these patients had no evidence of disease on further follow-up of 7 mo. The fifth patient, with recurrent lung cancer, was referred for radiotherapy of a single bone metastasis after PET/CT excluded malignancy in an area of increased hilar 18F-FDG uptake with no further evidence of malignancy in the mediastinum on follow-up.
In 7 patients, PET/CT guided further invasive diagnostic procedures. In 4 patients, malignancy was confirmed, by intestinal biopsy in 2 patients, by biopsy of a supraclavicular adenopathy in 1 patient, and by biopsy of a pancreatic mass in 1 patient. In 3 patients, malignancy was excluded by PET/CT-guided biopsy, with a histologic diagnosis of an anthracotic mediastinal lymph node, a thyroid adenoma, and a benign pelvic inflammation.
In 16 patients, PET/CT assisted in planning of the therapeutic strategy. Four patients were referred for previously unplanned surgery, including 3 patients with recurrent colon cancer referred for an explorative laparotomy of abdominopelvic lesions precisely characterized and localized on fused images. Thoracotomy was performed in 1 high-surgical-risk patient with an SPN, only after abnormal 18F-FDG uptake was retrospectively detected by PET/CT in that lung lesion, further diagnosed after surgery as a bronchoalveolar cancer. In 1 patient with a single liver metastasis, PET/CT induced retrospective identification of an additional hepatic lesion and modified the surgical approach to include resection of both lesions.
In 5 of the 16 patients, PET/CT results led to the administration of previously unplanned chemotherapy. In 2 of these patients, recurrent disease was diagnosed, with subsequent initiation of chemotherapy. In 3 patients, fusion data up-staged recurrent disease, and chemotherapy was administered instead of the previously planned surgery.
In 6 of the 16 patients, radiotherapy was initiated or modified on the basis of the PET/CT data. Two patients were referred for previously unplanned radiotherapy. In 1 patient, radiotherapy was administered to a single iliac bone metastasis retrospectively detected on PET/CT. In the second patient, radiotherapy was administered to a residual nasopharyngeal tumor detected retrospectively on PET after the review of fused data. In 3 patients, the identification and exact localization of additional malignant sites by PET/CT extended the initially planned radiation field to include mediastinal, retroperitoneal, and pelvic adenopathy, respectively. Exclusion of hilar disease, suspected on PET alone, allowed for a decrease in size of the radiation field in 1 patient. The clinical and imaging details of the patients in whom PET/CT had an impact on management are presented in Table 2.
Impact of PET/CT on Management of Patients: Clinical Details
DISCUSSION
The extensive use of imaging in the management of cancer patients has not only defined the particular advantages of both anatomic and functional modalities but also highlighted their inherent limitations. The biologic significance of the high-resolution anatomic details provided by CT is compromised by the use of size criteria (5). The metabolic information of PET lacks accurate topographic orientation (6,11). The need for coregistration of anatomic and functional imaging data arose from the recognition of the complementary, not competitive, roles of both modalities as a means of obtaining the most complete and accurate noninvasive data for improved clinical management (9,10,15).
Several reports have stressed the value of side-by-side visual comparison of PET and CT (16–18). Correlation of these different datasets, using various coregistration software programs, provided a more accurate fusion of separately performed PET and CT studies (15,17,18). Such methods, however, were imprecise, technically complicated, and time-consuming and, therefore, impractical for routine clinical use (6,19). Simultaneous acquisition of PET and CT using a combined PET/CT system provides the best method for the precise alignment of these 2 datasets and emerges as the most accurate and, at the same time, user-friendly technology for both patients and physicians (9,12). Accumulating data reveal improved diagnostic image interpretation using fused data of a hybrid device over the conventional interpretation of separate PET and CT (20–28). However, current available studies using hybrid PET/CT systems have assessed relatively small numbers of patients and report only some of the criteria by which fused imaging made its contribution for image interpretation and, especially, for patient management (20–28).
This study evaluated 204 patients with 586 sites suggestive of malignancy. The prospective comparison of PET/CT with separately performed PET and diagnostic CT in this large population found PET/CT to have additional value in 49% of patients and in 30% of sites. The principal advantage of combined PET/CT imaging is its ability to accurately localize abnormal metabolic changes detected on the PET study to anatomic structures defined on CT. Our study prospectively investigated whether PET/CT using a single device has an additional value, beyond that obtained from side-by-side evaluation of the separate PET and CT images, for the detection, localization, and characterization of malignant sites in cancer patients. To obtain a detailed analysis of the modifications in image interpretation associated with better localization of 18F-FDG uptake, we assessed the changes attributed to the fused data in several categories. We further analyzed whether additional diagnostic improvement also had an impact on different aspects of the clinical management of patients.
Analysis of the categories in which combined PET/CT was beneficial for image interpretation showed that fusion data excluded malignancy by localizing 18F-FDG uptake to structures with physiologic or benign uptake in 10% of suspected sites. Hybrid imaging precisely characterized 34 thoracic sites as nonmalignant. Benign increased 18F-FDG uptake of unclear etiology has been described in the chest in 7% of PET studies in 58 lymphoma patients (29). Nonmalignant hilar and mediastinal 18F-FDG uptake in blood vessels has been described as a possible source of false-positive PET results (30). As shown by our results, PET/CT imaging overcomes this pitfall and enables benign characterization of these foci. In our study, malignancy was also excluded in 16 gastrointestinal sites, for which activity was related to physiologic 18F-FDG uptake.
Fusion was of value in changing the characterization of areas of 18F-FDG uptake from benign or equivocal to malignant in 5% of evaluated sites. About half were abdominopelvic sites, initially considered to be physiologic bowel 18F-FDG uptake. Because physiologic intestinal 18F-FDG uptake is common, it may be more difficult to define 18F-FDG uptake in this area as definitely malignant. Precise coregistration using PET/CT reduces the number of lesions falsely considered as physiologic 18F-FDG activity on PET alone. This is probably the reason for the significant contribution of hybrid imaging, found in our study, for the assessment of abdominopelvic sites and in gastrointestinal malignancies.
Hybrid PET/CT imaging is of potential special value in the head and neck region, with its complex anatomy, both before and, even more so, after therapy (26–28). Although in our study, one third of head and neck lesions were redefined as benign or malignant or were detected, following PET/CT, after having been missed previously (Table 1), our study population included only relatively few such patients and sites. No conclusion, therefore, could be drawn concerning the contribution of fused imaging in the head and neck region in this study.
Although the initial scope of our study was to evaluate the value of fused imaging over PET alone, PET/CT was found to be of value for interpretation of CT as well, in concurrence with other reports (11,21). In this large study group, data from combined PET/CT images led to retrospective detection of malignant lesions previously missed on both the separately performed diagnostic CT and the CT component of the PET/CT, in 11% of evaluated, most of them nodal sites of disease.
Overall, combined PET/CT led to modified interpretation of one third of the total number of sites evaluated. This modified interpretation of the 178 sites was determined to be accurate in 169 sites (95%). PET/CT induced 6 false-positive and 3 false-negative interpretations, for an overall diagnostic error of 1.4% of all sites evaluated.
The advantages of PET/CT for improved image interpretation are of clinical significance only if they affect patient management as well. In the present study, PET/CT affected the clinical management of 28 of 204 patients (14%) with a broad-spectrum impact. It indicated the need for, and guided further diagnostic assessment. It affected therapeutic decisions indicating both the most appropriate therapy modality and protocol. To the best of our knowledge, this is one of the first reports assessing such an impact of PET/CT in a large, although heterogeneous, group of patients. The high sensitivity of PET renders even equivocal sites of increased 18F-FDG uptake highly suspicious of malignancy, requiring further evaluation. By excluding malignancy in sites of increased physiologic or benign 18F-FDG uptake, combined PET/CT obviates the need for further assessment, decreasing risks of morbidity and reducing medical costs. In cases where fusion increases the confidence that findings on 18F-FDG PET are malignant, its clinical impact is even more important, allowing for a single-step definition of disease, its extent and its adequate evaluation and treatment. The heterogeneous group of patients assessed in the present study emphasizes the large range of possible implications of PET/CT in the management of cancer patients.
Further evaluation of the additional value of combined PET/CT imaging in different tumor types and specific clinical indications is likely to provide additional insights regarding the important attributes of this imaging modality. As PET becomes widely and intensively used for the assessment of cancer patients, so, too, will combined PET/CT imaging become increasingly important. Appropriate patient selection for, and economical use of combined PET/CT, to yield optimal diagnostic and clinical information will therefore also be an important field of investigation.
CONCLUSION
The present report assessed the additional value of combined PET/CT imaging over separate PET and CT imaging in 204 cancer patients with 586 sites suspicious of disease. Categorization of changes in interpretation and detailed analysis of impact on diagnostic and therapeutic management were performed, to assess different aspects of the value of fused imaging, not previously described in detail. Hybrid PET/CT improved the diagnostic interpretation of 18F-FDG PET and CT in 49% of cancer patients and 30% of sites. The additional value of fusion was characterized by several specific categories, including precise lesion characterization, precise localization, and retrospective lesion detection. PET/CT data was found of benefit in various tumors, in various sites and in different stages of disease course. In 14% of patients, combined PET/CT imaging had an impact on patient management affecting both the diagnostic and therapeutic approach.
Acknowledgments
This research was supported in part by a grant from the L. Rosenblatt fund of the Technion Foundation for Research in Cancer.
Footnotes
Received Dec. 2, 2002; revision accepted Apr. 22, 2003.
For correspondence or reprints contact: Ora Israel, MD, Department of Nuclear Medicine, Rambam Medical Center, Haifa 35254, Israel.
E-mail: o_israel{at}rambam.health.gov.il
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Limiting surveillance imaging for patients with lymphoma in remission: a mixed methods study leading to a Choosing Wisely recommendation
- Performance of Digital PET Compared with High-Resolution Conventional PET in Patients with Cancer
- Novel Method to Detect and Characterize 18F-FDG Infiltration at the Injection Site: A Single-Institution Experience
- Whole-Body 18F-FDG PET/CT Is Superior to CT as First-Line Diagnostic Imaging in Patients Referred with Serious Nonspecific Symptoms or Signs of Cancer: A Randomized Prospective Study of 200 Patients
- Initial Preclinical Evaluation of 18F-Fluorodeoxysorbitol PET as a Novel Functional Renal Imaging Agent
- Functional Flow Patterns and Static Blood Pooling in Tumors Revealed by Combined Contrast-Enhanced Ultrasound and Photoacoustic Imaging
- Assessment of incidental and clinically unsuspected fluorodeoxyglucose-avid foci detected on oncological positron emission tomography/CT
- Positron emission tomography/computed tomography surveillance in patients with Hodgkin lymphoma in first remission has a low positive predictive value and high costs
- PET/CT and MRI of intra-osseous haemangioma of the tibia
- Imaging techniques in lung cancer
- Uptake of 18F-FDG in Acute Aortic Dissection: A Determinant of Unfavorable Outcome
- Prospective Evaluation of Whole-Body Cancer Screening With Multiple Modalities Including [18F]Fluorodeoxyglucose Positron Emission Tomography in a Healthy Population: A Preliminary Report
- Integrated PET/CT in the staging of nonsmall cell lung cancer: technical aspects and clinical integration
- Relationship Between Cancer Type and Impact of PET and PET/CT on Intended Management: Findings of the National Oncologic PET Registry
- PET/CT assessment of clinically unsuspected, incidental FDG-avid lesions in oncological patients
- 18F-FDG PET/CT in Evaluating Non-CNS Pediatric Malignancies
- Multimodality imaging of direct ureteric involvement in non-Hodgkin's lymphoma using PET/CT, CT urography and antegrade CT pyelography
- Value of contrast-enhanced multiphase CT in combined PET/CT protocols for oncological imaging
- Detection of extrapulmonary lesions with integrated PET/CT in the staging of lung cancer
- SPECT/Multislice Low-Dose CT: A Clinically Relevant Constituent in the Imaging Algorithm of Nononcologic Patients Referred for Bone Scintigraphy
- Early Detection of Cancer Recurrence: 18F-FDG PET/CT Can Make a Difference in Diagnosis and Patient Care
- PET-Based Treatment Planning in Radiotherapy: A New Standard?
- Clinical Significance of Small Pulmonary Nodules with Little or No 18F-FDG Uptake on PET/CT Images of Patients with Nonthoracic Malignancies
- Screening for Cancer with PET and PET/CT: Potential and Limitations
- PET/CT in Lymphoma: Prospective Study of Enhanced Full-Dose PET/CT Versus Unenhanced Low-Dose PET/CT
- Additional Value of PET/CT over PET in Assessment of Locoregional Lymph Nodes in Thoracic Esophageal Squamous Cell Cancer
- 11C-Acetate Positron Emission Tomography Imaging and Image Fusion With Computed Tomography and Magnetic Resonance Imaging in Patients With Recurrent Prostate Cancer
- Focal Thyroid Lesions Incidentally Identified by Integrated 18F-FDG PET/CT: Clinical Significance and Improved Characterization
- Whole body positron emission tomography/computed tomography (PET/CT) tumour staging with integrated PET/CT colonography: technical feasibility and first experiences in patients with colorectal cancer
- Improved Detection of Second Primary Cancer Using Integrated [18F] Fluorodeoxyglucose Positron Emission Tomography and Computed Tomography for Initial Tumor Staging
- Detection and Localization of Prostate Cancer: Correlation of 11C-Choline PET/CT with Histopathologic Step-Section Analysis
- Etiology of Solitary Extrapulmonary Positron Emission Tomography and Computed Tomography Findings in Patients With Lung Cancer
- Attenuation Correction of PET Images with Respiration-Averaged CT Images in PET/CT
- Clinically Significant Incidental Findings on the Unenhanced CT Portion of PET/CT Studies: Frequency in 250 Patients
- CT in PET/CT: Essential Features of Interpretation
- Imaging of Malignant Bone Involvement by Morphologic, Scintigraphic, and Hybrid Modalities
- Concurrent PET/CT with an Integrated Imaging System: Intersociety Dialogue from the Joint Working Group of the American College of Radiology, the Society of Nuclear Medicine, and the Society of Computed Body Tomography and Magnetic Resonance
- PET/CT Detection of Unexpected Gastrointestinal Foci of 18F-FDG Uptake: Incidence, Localization Patterns, and Clinical Significance
- Progress and Promise of FDG-PET Imaging for Cancer Patient Management and Oncologic Drug Development
- Is 18F-FDG PET/CT Useful for Imaging and Management of Patients with Suspected Occult Recurrence of Cancer?
- Evaluation of 18F-FDG Uptake and Arterial Wall Calcifications Using 18F-FDG PET/CT
- PET/CT Using 18F-FDG in Suspected Lung Cancer Recurrence: Diagnostic Value and Impact on Patient Management
- Assessment of Malignant Skeletal Disease: Initial Experience with 18F-Fluoride PET/CT and Comparison Between 18F-Fluoride PET and 18F-Fluoride PET/CT
- To Enhance or Not to Enhance? 18F-FDG and CT Contrast Agents in Dual-Modality 18F-FDG PET/CT
- Why Nearly All PET of Abdominal and Pelvic Cancers Will Be Performed as PET/CT
- Acquisition Protocol Considerations for Combined PET/CT Imaging
- PET/CT Image Navigation and Communication
- Why Most PET of Lung and Head-and-Neck Cancer Will Be PET/CT
- PET/CT Today and Tomorrow
- Software Approach to Merging Molecular with Anatomic Information