


Abstract
To enhance the therapeutic efficacy of radioimmunotherapy of cancer, several pretargeting strategies have been developed. In pretargeted radioimmunotherapy, the tumor is pretargeted with an antibody construct that has affinity for the tumor-associated antigen on the one hand and for a radiolabeled hapten on the other. The radiolabeled hapten is administered in a later phase, preferably after the antibody construct has cleared from the circulation. In pretargeted radioimmunotherapy, 2 main approaches can be distinguished: pretargeting strategies based on the avid interaction between streptavidin (SA) or avidin and biotin, and pretargeting strategies based on the use of bispecific antibodies. In pretargeting strategies based on biotin and SA or avidin, the use of a clearing agent that could remove the pretargeting construct from the circulation markedly improved the targeting of the radiolabeled biotin to the tumor. Thus, multistep injection schemes in which 3–5 different agents are subsequently injected were developed. In bispecific antibody-based pretargeting strategies, the use of bivalent haptens improved the efficacy of the tumor targeting, and a 2-step pretargeted radioimmunotherapy strategy is now being tested in cancer patients. Preclinical studies as well as studies on cancer patients have shown that these pretargeting strategies can result in higher radiation doses to the tumor than can directly radiolabeled antitumor antibodies. Here, the development and state of the art of the most effective approaches for pretargeted radioimmunotherapy are reviewed.
The concept of targeting radionuclides to tumors using radiolabeled monoclonal antibodies (mAbs) against tumor-associated antigens was proposed more than a century ago (1). With the development of the hybridoma technology (2) and the availability of mAbs against tumor-associated antigens, this concept was investigated scientifically in animal models and in cancer patients. These studies showed that targeting mAbs to tumors is an inefficient process. On intravenous injection, mAbs accumulate in tumors relatively slowly, and several days after injection only a few percent, at most, of the injected dose is localized in the tumor. The inefficiency of this accumulation has been attributed to the presence of various physiologic barriers between the circulation and the tumor cell surface (3). The vascular endothelium, the relatively large transport distances in the tissue, and the enhanced interstitial pressure in the tumor tissue hamper the penetration of mAbs into the tumor tissue to bind to their target antigen. Despite inefficient targeting, good response rates have been obtained with radioimmunotherapy in patients with hematologic tumors. B-cell lymphomas can be treated effectively with radiolabeled mAbs. Overall response rates of 60%–70% have been reported in patients with refractory non-Hodgkin’s lymphoma using radiolabeled anti-CD20 mAbs. The murine anti-CD20 mAb (2B8) labeled with 90Y, designated as 90Y-ibritumomab tiuxetan (Zevalin; IDEC Pharmaceuticals Corp., San Diego, CA), has recently been approved for the treatment of relapsed or refractory low-grade, follicular non-Hodgkin’s lymphoma (4).
Response rates in patients with solid tumors are modest; thus, for these less radiosensitive tumors, more effective targeting of tumors with mAbs is required. The efficacy of radioimmunotherapy therefore has to be further optimized. The driving force of the penetration, diffusion, and accumulation of radiolabeled mAbs in tumor tissue is their sustained high level in the circulation. In contrast, the high residence time of radiolabeled mAbs in the blood correlates with the radiation dose to the bone marrow, the dose-limiting organ in radioimmunotherapy. In fact, this is the most important dilemma in radioimmunotherapy: On the one hand, one aims to optimize the accumulation of the mAb in the tumor; on the other hand, the radiation dose to the bone marrow and, thus, the residence time in the circulation should be minimized.
Several strategies to improve targeting of tumors with radiolabeled mAbs have been developed, such as the use of mAb fragments, the use of high-affinity mAbs, the use of labeling techniques that are stable in vivo, active removal of the radiolabeled mAb from the circulation, and pretargeting strategies.
In pretargeting, the radionuclide is administered separately from the tumor-targeting mAb. In the first step, the unlabeled antitumor mAb is administered and allowed to accumulate in the tumor. In a later phase, preferably when the mAb has cleared from the circulation, the radionuclide is administered as a rapidly clearing agent with high affinity for the unlabeled molecule that was injected in the first phase. Pretargeting can be regarded as in vivo mAb labeling, because the antitumor mAb is radiolabeled after in vivo administration, preferably in the tumor. Here, the pretargeting strategies that have been developed are reviewed.
THE CONCEPT OF PRETARGETING
Conventional mAb targeting using directly radiolabeled mAbs is characterized by slow pharmacokinetics: the half-life of a mAb in the circulation is usually between 2 and 4 d. Such a long residence time in the blood may facilitate the optimal driving force for optimal accretion of the mAbs in the tumor. On the other hand, it also causes relatively high residence times of the radiolabeled mAbs in the nontarget tissues. In pretargeting, the unlabeled mAb is injected in the first phase. After clearance from the blood, the radionuclide is injected in a later phase. The radionuclide is generally administered linked to a relatively small molecule that is cleared rapidly from the blood, in an attempt to maximize accumulation in the tumor while minimizing exposure to the nontarget organs. The radiolabeled ligand should distribute rapidly throughout the body and is to be bound to the prelocalized mAb in the target tissue, whereas the unbound radiolabeled molecule should clear rapidly from the body, preferably through the kidneys. The pretargeting concept was proposed 15 y ago by Goodwin et al., who suggested that tumors be pretargeted with agents with dual specificity (bifunctional mAbs or mAb–avidin conjugates) with affinity for the tumor on the one hand and for the radiolabeled ligand on the other (5,6). Since then, various research groups have tested and optimized a series of pretargeting approaches. Two main approaches based on the interaction between the first and second injectates can be distinguished: avidin–or streptavidin–biotin interaction and mAb–hapten interaction.
PRETARGETING BASED ON BIOTIN AND AVIDIN
Avidin, a minor constituent of the egg white of reptiles, amphibians, and birds, is a glycosylated and positively charged protein that can bind up to 4 molecules of vitamin H, D-biotin (7). The interaction with biotin is noncovalent but extremely avid, the affinity constant (1015 per mole) is 1,000,000-fold higher than that of the antigen–mAb interaction. Functional avidin is a tetramer of identical subunits. Streptavidin is a bacterial analog of avidin with similar biotin-binding characteristics, with less normal tissue retention than that of avidin (8,9).
The first pretargeting studies with biotinylated mAbs aimed to exploit the extremely high affinity of avidin for biotin. In mice and rabbits, the target was pretargeted with biotinylated mAbs, and radiolabeled avidin was administered in the second step. These studies provided proof of principle that radiolabeled avidin could accumulate in the biotinylated target (5,10,11). The radiolabeled avidin also bound to the biotinylated mAb in the circulation. An avidin “chase” was given before injection of the radiolabeled avidin to lower the concentration of the biotinylated mAb in the blood. In nude mice with human tumor xenografts, injection of unlabeled avidin before injection of the radiolabeled avidin or streptavidin accelerated the tumor uptake as well as the blood clearance of the radiolabeled avidin or streptavidin (12,13). Furthermore, investigators realized soon thereafter that the rapid pharmacokinetics of biotin would be fully exploited if one pretargeted the tumor with avidin and administered radiolabeled biotin in the last step (14,15).
THE MILAN EXPERIENCE
Since 1988, an Italian group of investigators under the direction of Paganelli has been testing pretargeting strategies based on biotin and avidin, mainly in clinical studies (10). In ovarian cancer patients, they tested a 2-step approach. Biotinylated antifolate receptor mAbs (MOv18) were injected intraperitoneally in 15 patients. Three to 5 d later, 111In-labeled streptavidin (SA) (100–150 μg) was injected intraperitoneally. Tumors were imaged between 2 and 48 h after injection of the radiolabel. Ex vivo measurements of resected tumor samples indicated that activity uptake in the tumors was at least as high as obtained with directly labeled mAbs (0.005–0.3 percentage injected dose per gram [%ID/g]) (16).
In patients with carcinoembryonic antigen (CEA)–producing tumors, the group in Milan tested a 3-step mAb-targeting methodology. This 3-step strategy is schematically summarized in Figure 1. Nineteen patients received a biotinylated anti-CEA mAb (FO23C5) intravenously. After 3 d, unlabeled avidin was injected to clear the biotinylated mAb from the blood. Another 2 d later, patients received 111In-labeled biotin. In all patients with tumors, tumors were detected with reasonable tumor-to-background ratios (17). Similarly, for patients with pulmonary carcinoma on whom the same 3-step injection scheme was used (FO23C5-biotin/avidin/111In-biotin), tumors were imaged in 8 of 10 patients (18). This injection scheme was also applied successfully to detect tumor lesions intraoperatively in rectal cancer patients using a γ-detection probe (19).
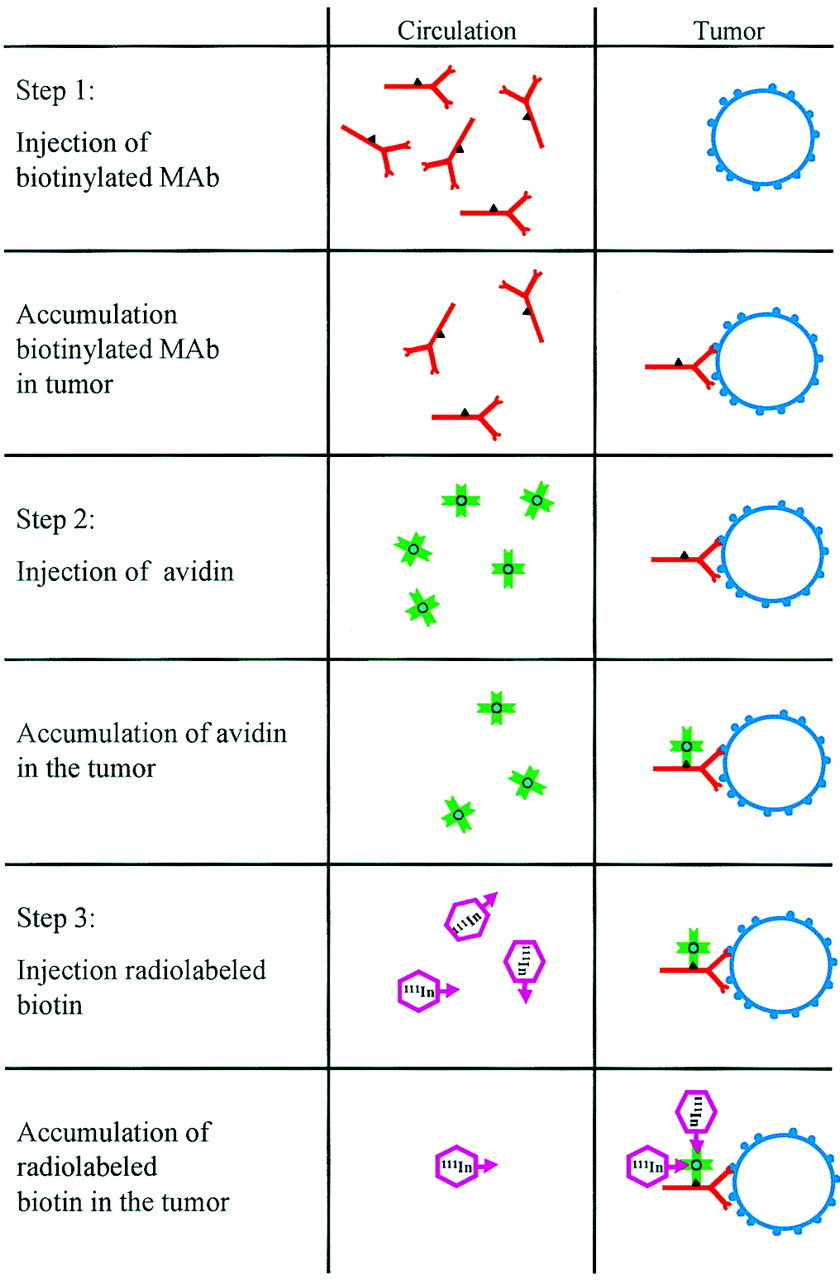
Schematic representation of 3-step avidin/biotin-based pretargeting. Biotinylated antitumor mAb is injected in first step. Subsequently, avidin is administered to avidinylate tumor, and in last step radiolabeled biotin is injected.
The group in Milan studied this 3-step strategy (mAb-biotin/avidin/radiolabeled biotin) using at least 5 different antitumor mAbs. Neuroendocrine tumors could be visualized using a biotinylated anti–chromogranin A mAb (A11) in the first step and 99mTc-biotin in the last step (20–22). In patients with uveal melanoma, the 3-step approach, using a biotinylated mAb against a melanoma-associated antigen (HMW-MAA, 225-28S), was compared with the 1-step method (99mTc-labeled 225-28S mAb) (23). Intrapatient comparisons for 15 patients showed that the 3-step method effectively reduced background activity, resulting in tumor-to-nontumor ratios that were twice as high as those for the 1-step method (24).
The group’s 99mTc-labeled biotin, although less suitable for imaging abdominal tumor masses because of its hepatobiliary route of clearance, was successfully used in combination with biotinylated antitenascin mAb (BC2) to visualize cerebral gliomas (25).
These studies in cancer patients showed that biotin–avidin pretargeting could improve tumor-to-background ratios. In addition, the studies demonstrated that the results are markedly affected by the dosing and timing of the reagents: In general, a 1- to 2-mg dose of the mAb followed by approximately 5 mg of avidin and a low dose (<0.1 mg) of radiobiotin, with at least a 2-d interval between the injections, was optimal. Furthermore, the characteristics of the antitumor mAb also determined the targeting efficiency. Obviously, mAbs that are rapidly internalized by the tumor cell are less suitable for application in the 3-step approach, because with these mAbs, the biotin residues are not optimally presented on the surface of the tumor cells. Moreover, in vitro studies indicated that biotinylated MOv18 was internalized by the target cell after binding of SA. The relatively low tumor-to-background ratios obtained with the 3-step method in ovarian cancer patients using biotinylated MOv18 may be due to the internalization of the antigen–MOv18–SA complex (26).
The circulatory half-life of avidin is much shorter than that of SA. Therefore, avidin has more optimal characteristics as a clearing agent: It can rapidly bind the biotinylated mAbs in the circulation, and the avidin that does not bind any biotinylated mAb also clears to the liver. In contrast, the relatively long-circulating SA has more optimal characteristics to avidinylate the tumor that was pretargeted with biotinylated mAb. During the course of their studies, the group in Milan further optimized the 3-step pretargeting injection scheme (mAb-biotin/avidin/radiolabeled biotin) by replacing the second step with the sequential injection of avidin and SA. With this 4-step injection scheme (mAb-biotin/avidin/SA/111In-biotin), tumor lesions were visualized in 30 ovarian cancer patients (27). Lesions were visualized in all patients with tumors, and no false-negative results were obtained.
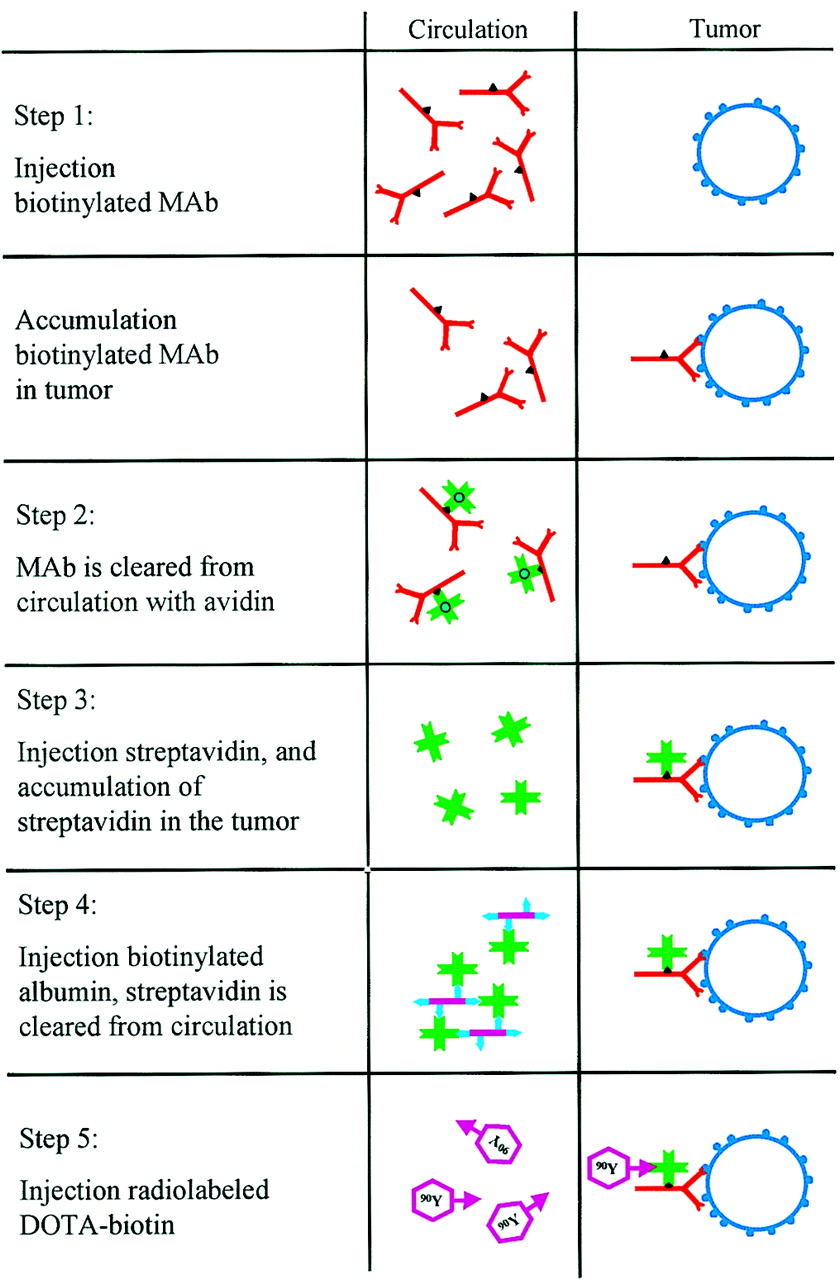
Subsequently, an extra clearing agent was introduced to remove the remaining SA from the circulation. Biotinylated albumin was injected just before administration of the radiolabeled biotin. Optimal tumor-to-background ratios were obtained with this 5-step injection scheme (mAb-biotin/avidin/SA/biotinylated albumin/radiolabeled biotin), as represented schematically in Figure 2.

Schematic representation of 5-step SA/biotin- or avidin/biotin-based pretargeting strategy. First, biotinylated mAb is injected. Then, avidin is administered to clear biotinylated mAb from circulation. Streptavidin is injected in third step to avidinylate tumor. Circulating SA is cleared with biotinylated albumin, and radiolabeled biotin is then injected.
This 5-step strategy has now been developed for radioimmunotherapy of cancer (28,29). Patients with grade III or IV glioma received biotinylated antitenascin mAb (BC4, 35 mg/m2) intravenously. One day later (24–36 h), they received 30 mg of avidin followed 30 min later by 50 mg of SA. Yet another day later (18–24 h), patients received 20 mg of biotinylated human albumin to reduce the levels of circulating SA. Ten minutes after this second chase, the radiolabeled biotin was injected (2 mg of biotin labeled with 4.4- to 5.9-GBq 90Y, mixed with 50 μg of biotin labeled with 74- to 111-MBq 111In) (Fig. 3) (28,29). The use of dodecanetetraacetic acid (DOTA) as a chelator to label biotin with 90Y was shown to be inevitable, because with diethylenetriaminepentaacetic acid (DTPA)–biotin approximately 5% of the 90Y was released in vivo, causing a considerable additive radiation dose to the red marrow (30). The treatment of 48 glioma patients with therapeutic doses of 90Y-DOTA–biotin (2.20–2.96 GBq/m2) has been reported. Therapeutic responses were observed during the phase I dose escalation study (4 complete responses, 2 partial responses) (29). The approach has also been tested in patients with recurrent glioma after a second surgical debulking. In these patients, the reagents were administered directly into the surgical cavity. During dose escalation (0.55–1.11 MBq) in 24 patients, the overall response rate of this locoregional pretargeted radioimmunotherapy was 25% (2 partial responses, 4 moderate responses) (28). Recently, a radioimmunotherapy study was completed using the same therapeutic regimen in high-grade glioma patients with no evidence of disease after surgery and radiotherapy. In this nonrandomized study, the median disease-free interval in patients with glioblastoma (n = 19) and grade III glioma (n = 17) was 28 mo (range, 9–59 mo) and 56 mo (range, 15–60 mo), respectively (31). These median survival intervals are much longer than those of glioma patients who did not receive this adjuvant treatment; thus, a randomized trial is warranted.

Anterior whole-body images of patient with recurrent glioma who underwent 5-step pretargeted radioimmunotherapy (2.22 MBq/m2 90Y-DOTA-biotin). 111In-DOTA-biotin (74 MBq) was coadministered to allow scintigraphic imaging. Images were acquired 1 h (left) and 22 h (right) after administration of radiolabeled biotin. On image acquired 22 h after injection, tumor is clearly visualized (arrow).
The relatively slow pharmacokinetics of SA make this molecule more suitable than avidin to avidinylate the tumor. However, Chinol et al. have shown that SA is more immunogenic (32). Streptavidin is a bacterial protein that does not have a mammalian analog and, thus, cannot be humanized. Pegylation of avidin increased the plasma half-life and reduced the immunogenicity of avidin; however, pegylation reduced the biotin-binding capacity of the molecule.
THE NeoRx APPROACH
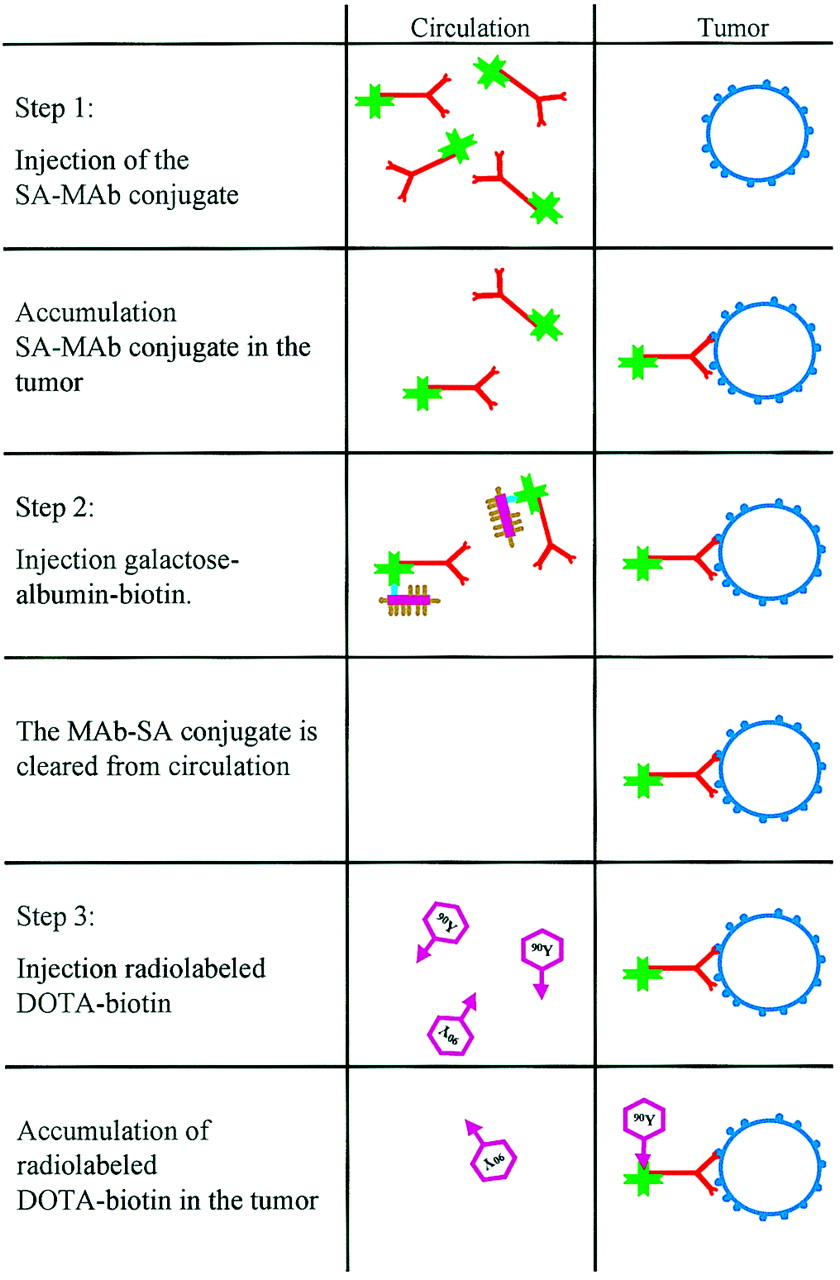
Another pretargeting strategy based on SA and biotin was developed at NeoRx Corp. (Seattle, WA) (Fig. 4). In this 3-step approach, the tumor is pretargeted with a mAb–SA conjugate. In the second step, this conjugate is cleared from the circulation with a chase of galactosylated biotin-albumin. This agent complexes with the mAb–SA conjugate in the circulation. Subsequently, the complex is rapidly cleared and metabolized in the liver because of the interaction of the galactose groups with the asialoglycoprotein receptor on hepatocytes (33). In the last step, radiolabeled DOTA-biotin is administered. This injection scheme was tested using an anti-Ep-CAM mAb (NR-LU-10) in nude mice with LS180 human colon carcinoma xenografts (34). In this model, tumor uptake 1 and 2 d after injection of the radiolabeled DOTA-biotin (%ID/g) was in the same range as that of the directly labeled NR-LU-10 mAb, whereas blood levels were at least 10 times lower. Dosimetric analysis of the biodistribution data indicated that at equal blood and marrow doses, the radiation dose to the tumor obtained with the pretargeting approach was 28 times (!) higher than the dose obtained with the 90Y-labeled mAb. In 10 of 10 mice with established human small cell lung cancer or colon cancer xenografts, a single dose of pretargeted radioimmunotherapy with 90Y-DOTA-biotin (22.2–29.6 MBq) ablated the tumors.

Schematic representation of 3-step SA/biotin-based pretargeting strategy. mAb–SA conjugate is injected, followed by galactosylated albumin-biotin as clearing agent. In third step, radiolabeled biotin is injected.
On the basis of the excellent targeting and therapeutic efficacy of the pretargeting approach based on NR-LU-10 and SA in nude mice, this 3-step approach was further developed in clinical studies. Forty-three patients with adenocarcinomas received 3 subsequent injections: NR-LU-10 mAb–SA conjugate, biotin-galactose-albumin as a clearing agent, and 111In/90Y-DOTA-biotin. The injection schema was optimized with respect to dosing and timing as follows: mAb–SA conjugate (168–600 mg)  clearing agent (110–600 mg)
clearing agent (110–600 mg)  DOTA-biotin (0.5–2 mg).
DOTA-biotin (0.5–2 mg).
Initially, one aimed to saturate the tumor with mAb–SA conjugate. However, at higher doses (>400 mg), high uptake of the radiolabel in the kidneys was observed, most likely because of the known antigen expression in the kidneys (35). A bolus injection of a 10-fold molar excess in the circulation of the clearing agent effectively cleared the mAb–SA conjugate to the liver (400 mg). Finally, optimal tumor doses were obtained at a relatively low dose of DOTA-biotin (0.5 mg). When this injection was given relatively early after injection of the clearing agent (4 h), uptake of the radiolabel in the liver was relatively high. Thus, the optimal injection scheme was defined as 400 mg of mAb–SA conjugate, followed at 48 h by 400 mg of clearing agent. The radiobiotin (0.5 mg) is administered 24 h after the clearing agent (36). A subsequent activity dose escalation study found that at doses exceeding 4.1 GBq/m2, 90Y-DOTA-biotin dose-limiting gastrointestinal toxicity (grade III/IV diarrhea) occurred because of reactivity of the mAb with normal gastrointestinal tract epithelium (37).
The therapeutic efficacy of the optimized 3-step strategy was determined in a phase II study on 25 patients with metastatic colon cancer. The patients received 400 mg of NR-LU-10–SA conjugate intravenously; 2 d later, 400 mg of biotin-galactose-albumin were administered; and another day later, 4.1 GBq/m2 of 90Y-DOTA-biotin were given (38). Two patients had a partial response (overall response rate, 8%): In the 2 patients who responded, the estimated dose to the tumor was 4,000 and 6,000 cGy (39). Within 4 wk, antibodies against the murine mAb, SA, and mAb–SA conjugate were detected in the serum of all patients who received the 3 consecutive injections (38).
In the phase II study, patients received a relatively high dose to the small-intestine wall (mean dose, 13,334 cGy) because of the reactivity of the NR-LU-10 mAb with the bowel epithelium, and consequently, one third of the patients experienced grade III/IV diarrhea. In addition, the radiation dose to the kidneys in these patients was also relatively high (1,606–3,454 cGy) because of Ep-cam antigen expression in the tubular epithelium. From these phase I/II studies, it was concluded that with this 3-step pretargeting radioimmunotherapy approach, the radiation doses to the tumor can be enhanced. However, the NR-LU-10 mAb is unsuitable for this application because of its reactivity with the normal gastrointestinal epithelium and collecting tubules in the kidneys. Therefore, the approach was tested using an anti-CD20–SA conjugate for the treatment of patients with non-Hodgkin’s lymphoma. Press et al. showed that the therapeutic efficacy of the 3-step approach in mice with Ramos lymphoma xenografts was superior to that of the 90Y-labeled anti-CD20 mAb (40). The 3-step strategy was tested using the chimeric anti-CD20 mAb (C2B8 = rituximab) conjugated with SA in patients with non-Hodgkin’s lymphoma (41). Dosimetric analysis of the images obtained after injection of 111In-DOTA-biotin indicated that pretargeting improved the radiation absorbed doses to the tumor lesions; the median tumor–to–whole-body dose was 35:1 in these patients. Forty percent of the lesions in these patients (n = 30) would have received a dose exceeding 3,000 cGy if 1.85 GBq had been administered. In the 7 patients who actually received a therapeutic activity dose of 90Y-DOTA-biotin (1.11–1.85 GBq/m2), 3 complete responses and 1 partial response were observed (42).
THE ROLE OF ENDOGENOUS BIOTIN AND BIOTINIDASE
As indicated above, biotin or vitamin H has a physiologic role in vertebrates. Several studies have shown that endogenous biotin levels (10−8–10−7 mol/L) could affect the efficacy of SA- or avidin-based pretargeting strategies (43,44). In a study on mice, Rusckowski et al. observed that a tumor pretargeted with a mAb–SA conjugate could bind biotin (exogenously administered) only when the mice were depleted of endogenous biotin (by sequential intraperitoneal injections of avidin) (43). Sharkey et al. tested a 3-step pretargeting approach similar to that developed by the NeoRx group, using an SA–anti-CEA mAb (MN-14) conjugate in nude mice with CEA-expressing GW-39 tumors. In that model, the mAb–SA conjugate could not be cleared from the circulation using galactosylated albumin-biotin, unless the animals were fed a biotin-deficient diet (44). These experiments showed that endogenous biotin levels can markedly interfere in avidin- or SA-based pretargeting strategies. Whether this also applies in studies of cancer patients is still a matter of debate.
In addition, it has been suggested that radiolabeled biotin compounds (DTPA-biotin, DOTA-biotin) can be hydrolyzed by endogenous biotinidase. The primary function of the enzyme is to cleave the biotin amide bond linking biotin and lysine in biocytin in such a way that the essential vitamin H can be recycled. Biotinidase is present in serum and tissues of both animals and humans in nanomolar concentrations. Several investigators have successfully changed the structure of the biotin derivatives used in pretargeting to make the compound unsusceptible toward biotinidase. Chemically modifying the carbon atom α to the biotin amide bond has been shown to effectively block biotinidase cleavage of the biotin amide bond (45,46).
Improved reagents for this 3-step pretargeting radioimmunotherapy strategy have been developed. In the study on patients with non-Hodgkin’s lymphoma, a synthetic clearing agent (biotin-N-acetyl-galactosamine) was used (47). Studies with radiolabeled anti-CD20–SA conjugates showed that this clearing agent removed more than 95% of the conjugate from the circulation. Recently, the synthesis of mAb–SA fusion proteins by genetic engineering has been described (48–50). A fusion protein of the humanized NR-LU-10 single-chain mAb and SA (scFv–SA) was produced and was shown to specifically trap radiolabeled biotin in the tumor in nude mice with SW1222 human colon carcinoma xenografts (48). In addition, for lymphoma targeting, a tetravalent single-chain mAb fusion protein of the murine single-chain CD20 mAb and SA was produced (50). In contrast to the chemical mAb–SA conjugates, these agents have a well-defined homogeneous composition and are relatively easy to manufacture. The latter construct is now in clinical trials.
In summary, 3-step radioimmunotherapy using mAb–SA conjugates, a clearing agent, and radiobiotin can enhance the radiation dose to the tumor, in comparison with the dose delivered by radioimmunotherapy using directly labeled mAbs. The first phase-I/II radioimmunotherapy studies have shown that the approach can induce therapeutic responses. The approach requires the use of mAbs that can specifically avidinylate the tumor. Well-defined agents (mAb–SA conjugate, clearing agent, and biotinidase-resistant biotin-DOTA) and accurate dosing and timing of the injections are crucial. The role of endogenous biotin in patients has yet to be determined. Development of anti-SA mAbs will preclude multiple treatments.
PRETARGETING WITH BISPECIFIC mAbs (bsmAbs)
The first studies to use mAb constructs with dual reactivity in a pretargeting strategy were reported in 1985. A group of investigators at Stanford University and the University of California (51,52) produced mAbs against chelated radiometals and tested the concept in mice with syngeneic KHJJ tumors. In the initial studies, antibenzyl ethylenediaminetetraacetic acid (EDTA) mAbs were complexed with the 111In-labeled chelate in vitro and subsequently were injected into tumor-bearing mice. Complex formation with the mAb markedly enhanced the circulatory half-life of the 111In-labeled chelate. Consequently, uptake of the mAb–chelate complex in the tumor was 50-fold higher than that of the 111In-labeled chelate alone (52). In later studies, an actual pretargeting approach was tested with these antichelate mAbs. The unlabeled antichelate mAb was injected intravenously in mice with KHJJ tumors, followed by an injection with the radiolabeled chelate (53). These studies showed that tumor targeting could be markedly improved when the antichelate mAb was cleared from the circulation before injection of the radiolabeled chelate. For this purpose, Goodwin et al. used transferrin substituted with multiple EDTA haptens as a clearing agent. Use of the clearing agent caused a 3-fold reduction of uptake in the tumor. However, because of more rapid clearance of the radiolabeled chelate from the blood, tumor-to-blood ratios increased 13-fold (54). This approach was further developed for radioimmunotherapy by developing a mAb specifically reactive with DOTA labeled with yttrium. KHJJ tumors in mice were pretargeted with the anti-DOTA mAb. One day later, circulating mAb was cleared by injection of transferrin substituted with multiple DOTA haptens, followed by injection of 88Y-DOTA 1 h later (55). Three hours after injection of the radiolabel, tumor uptake was 1.7 %ID/g and a tumor-to-blood ratio of 16 was measured, indicating specific targeting of the tumor.
In the experiments described above, the mAbs used to pretarget the tumor did not have any affinity for the tumor, and accumulation of the antichelate mAbs in the tumor was dependent on the nonspecific accumulation in the tumor caused by enhanced vascular permeability in the tumor. Specific pretargeting of tumors requires the production of mAbs with dual specificity: affinity for the tumor-associated antigen on the one hand and affinity for the radiolabeled hapten on the other. Several methods have been developed to produce such bifunctional mAbs: Heteroconjugates can be produced by chemical cross-linking of 2 mAbs; in general, 1:1 heteroconjugates of mAbs are relatively difficult to synthesize. By chemical cross-linking of the Fab′ fragments of 2 mAbs, F(ab′)2 bsmAb fragments can be produced (56). By fusion of 2 hybridoma cell lines producing 2 different mAbs, quadroma cell lines can be selected that secrete (among others) bispecific IgG molecules (57); in general, purification of the bsmAbs from the quadroma supernatant (containing 10 different IgG-like molecules) is laborious, but this method does not suffer from batch-to-batch variation, as do the chemical methods. By genetic engineering techniques, fusion proteins can be produced containing the antigen-binding regions of 2 mAbs (58).
At Hybritech Inc. (San Diego, CA), a 2-step system based on an anti-CEA (ZCE-025) × anti-111In-benzyl-EDTA Fab′ × Fab′ chemically synthesized bsmAb and an 111In-labeled EDTA derivative (111In-EOTUBE) was developed (59). In mice, the radiolabeled chelate, complexed with bsmAb F(ab′)2 to prolong the plasma half-life of the chelate, was administered 24 h after injection of the bsmAb. One day after injection of 111In-EOTUBE, uptake in the tumor was 18.5 %ID/g, and the blood level was as low as 1.3 %ID/g, indicating efficient tumor targeting. This approach was tested on 14 patients with recurrent colon carcinoma. Scintigraphic imaging visualized 20 of 21 known lesions. Nine occult lesions were imaged, of which 8 could be confirmed.
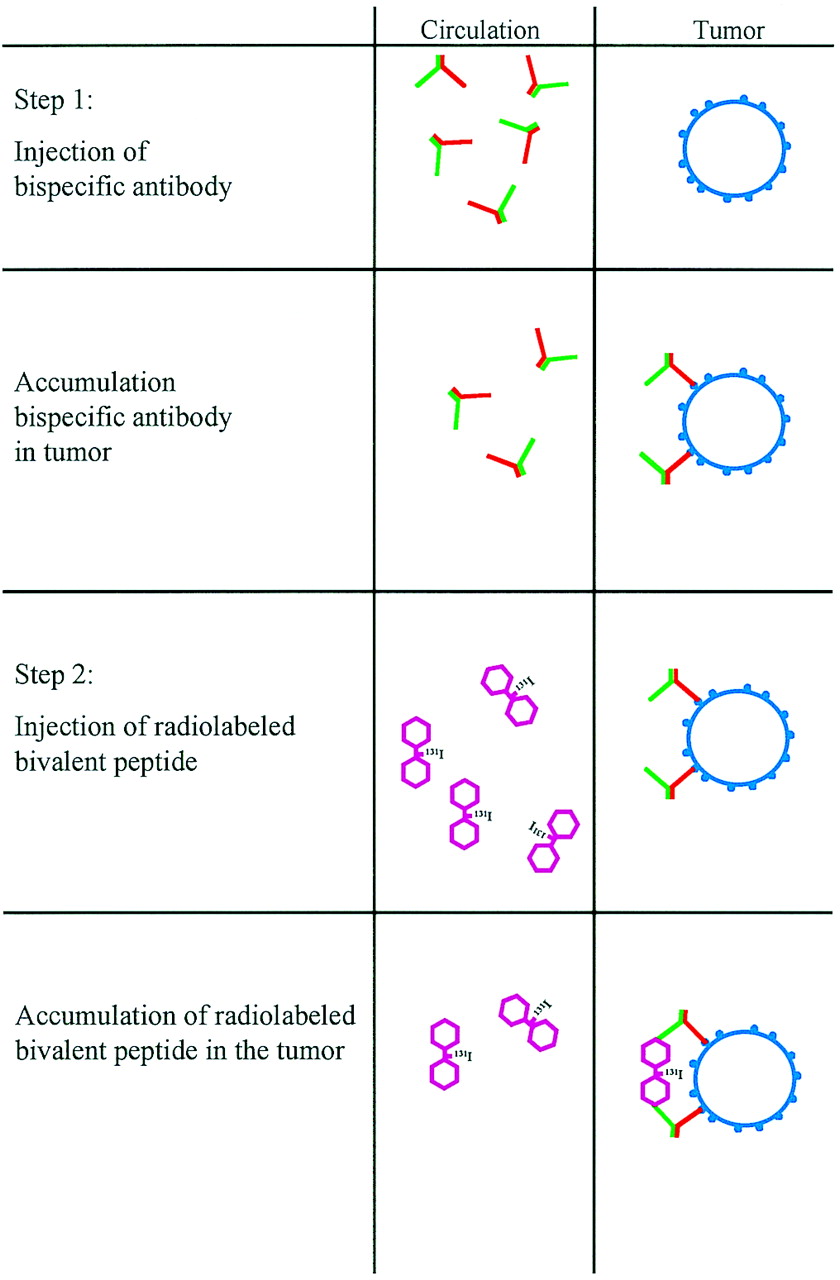
A similar approach was developed by a group in France (Fig. 5). Chemically produced Fab′–Fab′ bsmAbs were constructed from antitumor mAbs on the one hand and antichelate mAbs on the other. Subcutaneous A375 melanoma tumors pretargeted with antitumor × anti-DTPA F(ab′)2 bsmAb could be targeted with 111In-labeled DTPA. Interestingly, this study showed that the use of a peptide substituted with 2 DTPA moieties (DTPA-Tyr-Lys-DTPA) accreted more efficiently in the tumor (3.5 %ID/g 24 h after injection) than did monovalent DTPA-111In (2.8 %ID/g 24 h after injection) (60). It was hypothesized that at the tumor cell surface, the bivalently substituted peptide is bound by 2 bsmAbs, resulting in more avid binding of the radiolabeled peptide, as depicted in Figure 5. This so-called affinity enhancement system also improved the tumor uptake in other mouse tumor models using bsmAb-based 2-step targeting (61,62). Le Doussal et al. demonstrated improved binding and retention of bivalent peptides (i.e., with 2 haptens) to pretargeted tumor cells in vitro (60,61,63) and elegantly showed that the spacing between the 2 haptens needs to be designed with care: Di- and tripeptides such as tyrosyl-lysine and lysyl-tyrosyl-lysine with 2 hapten-substituted amino groups had ideal characteristics for this application (62,64). Goodwin et al., in their murine KHJJ model, also obtained improved tumor uptake using a bivalent DOTA construct (1.7 %ID/g vs. 4.4 %ID/g 3 h after injection) named Janus-DOTA, after the Roman deity with 2 faces (55). In our renal cell carcinoma nude mouse model using biologically produced bsmAbs, application of a bivalent hapten, Phe-Lys(DTPA-111In)-Tyr-Lys(DTPA-111In), improved uptake of the radiolabel in the tumor by a factor of 30 (!) (2.2 %ID/g vs. 77.5 %ID/g at 1 h after injection) (Fig. 6) (52). That study also showed that pretargeting with bsmAbs (in comparison with directly labeled mAbs) could improve not only tumor-to-background ratios but also uptake of radiolabel by tumor in terms of %ID/g during the first 24 h.

Schematic representation of 2-step bsmAb-based pretargeting strategy. Tumor is pretargeted with antihapten × antitumor F(ab′)2 bsmAb. In second step, radiolabeled bivalent hapten is administered. Note bivalent binding of bivalent hapten at tumor cell surface.

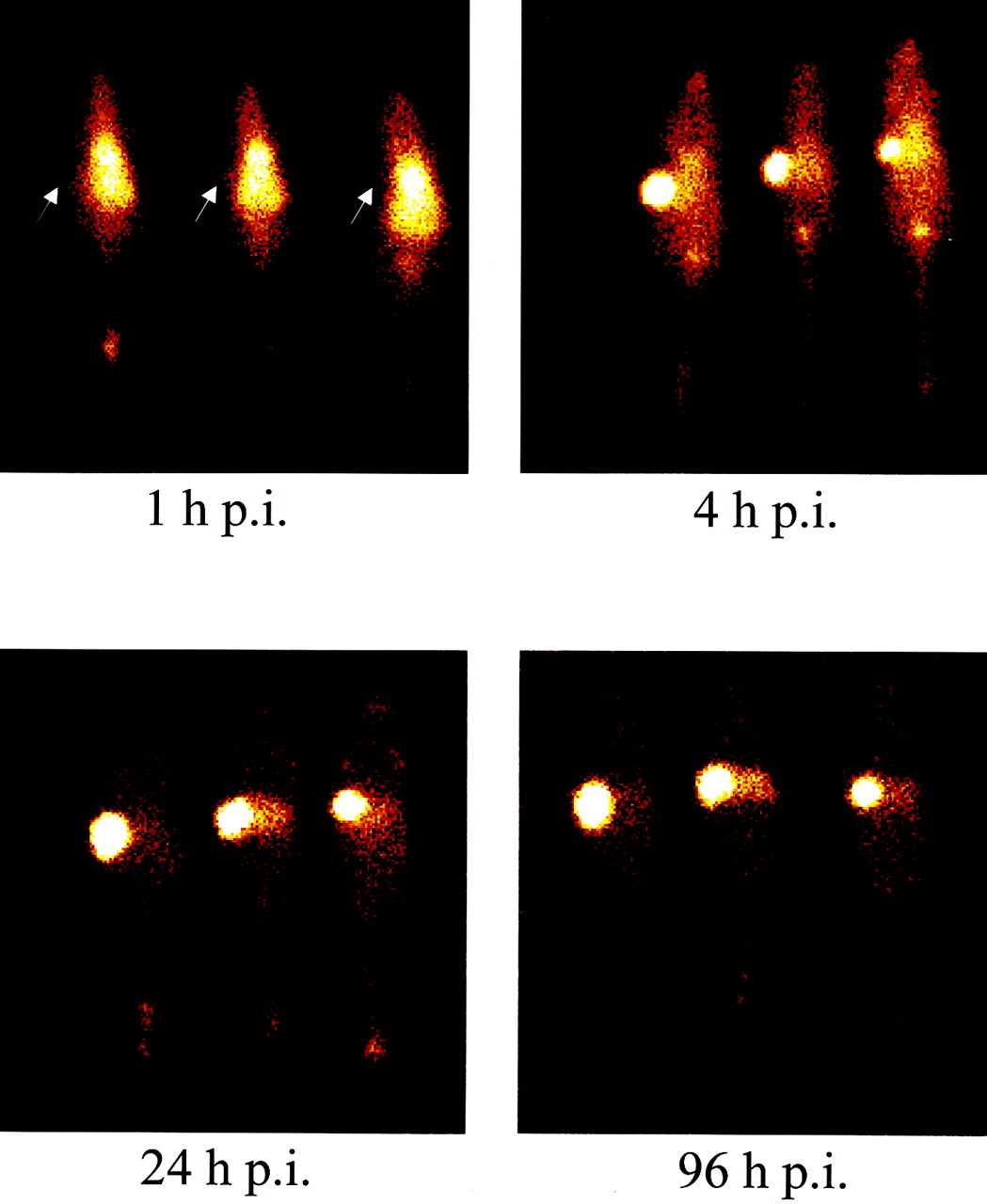
Scintigraphic images of nude mice with subcutaneous human renal cell carcinoma xenografts in right flank (arrows). Mice were injected intravenously with 15 μg G250 × DTIn-1 bsmAb. Three days later, mice intravenously received 10 ng of tetrapeptide substituted with 2 DTPA moieties and labeled with 1.85 MBq of 111In. Images were acquired at 1, 4, 24, and 96 h after injection (p.i.).
Interestingly, in most studies using bsmAbs to pretarget the tumor, the bsmAbs were not cleared from the circulation before injection of the radiolabeled (bivalent) peptide. In contrast, when the tumor is pretargeted with avidin (i.e., is avidinylated), the use of a clearing agent appeared to be indispensable. Fab′–Fab′ bsmAbs rapidly clear from the blood. Therefore, blocking the remaining antihapten activity in the circulation appears to be superfluous (60,62,65). In addition, the difference in affinity between the hapten–mAb (10−8 per mole) and the biotin–avidin (10−15 per mole) interactions might also play a role. Intravenous injection of radiolabeled biotin in circulation that still contains significant levels of avidin or streptavidin will lead to the formation of stable biotin–avidin or biotin–streptavidin complexes in the circulation. Depending on the antihapten mAb used, the mAb–hapten complexes formed in the circulation are relatively labile. As a result, during the first few hours after injection of the radiolabeled peptide, the peptide–mAb complexes dissociate and the peptide is cleared through the kidneys (52). The fact that, in bsmAb-based pretargeting strategies, the clearing step can be omitted simplifies the introduction of the approach into the clinic, as dosing and timing of the clearing agent are a critical step that requires careful optimization. Overdosing of the blocking agent may block the binding sites in the tumor and may thus reduce tumor targeting (66).
In preclinical studies, the French group has shown that its pretargeting strategy could improve radioimmunotherapy (67–73). In these studies, the tumor was pretargeted with the anti-CEA × anti-DTPA Fab′–Fab′ bsmAb, and 48 h later a therapeutic dose of 131I-labeled di-DTPA-tyrosyl-lysine was administered. In mice with medullary thyroid carcinoma (70,71) or colon carcinoma (67–69), the therapeutic efficacy of 2-step pretargeted radioimmunotherapy was superior to that of 131I-labeled anti-CEA mAbs (F(ab′)2 or IgG). Recently, a di-DTPA substituted peptide was developed that could be radiolabeled with 188Re, allowing the use of this generator-produced β-emitter in pretargeted radioimmunotherapy (74,75).
These promising data obtained in nude mouse tumor models encouraged the French group to test this bsmAb-based 2-step pretargeting approach in cancer patients. In these studies, the chemically produced anti-CEA (clone F6) × anti-DTPA-In (clone 734) F(ab′)2 bsmAb is injected in the first step (0.1 mg/kg). Four to 5 d later, 111In-labeled di-DTPA-tyrosyl-lysine is injected. In the initial studies, the French group showed that the approach could improve radioimmunoscintigraphy of CEA-expressing tumors. In patients with primary colorectal carcinomas (n = 11), uptake of the 111In-labeled di-DPTA peptide (0.002–0.018 %ID/g) was in the same range as uptake of the 111In-labeled F(ab′)2 anti-CEA mAb, whereas ratios of tumor to normal tissue were significantly higher (65). An immunoscintigraphy study in patients with recurrent colorectal cancer indicated that the 111In-diDTPA was taken up mainly in the periphery of liver metastases, whereas uptake in the pelvic lesions was generally higher (76). A study of 12 patients with non–small cell lung carcinoma also showed that the 2-step approach was better than conventional immunoscintigraphy for staging (77). In patients with medullary thyroid carcinoma, uptake of 111In-diDTPA in tumor lesions was relatively high (0.003–0.139 %ID/g; mean, 0.039 %ID/g) (78). Two-step immunoscintigraphy in 44 patients with medullary thyroid carcinoma revealed that the method is sensitive for visualizing occult metastases. In 21 of 29 patients with elevated calcitonin but without known tumor sites, occult metastases were visualized (79).
bsmAb-BASED PRETARGETED RADIOIMMUNOTHERAPY IN PATIENTS
Currently, this bsmAb-based pretargeting method for radioimmunotherapy is being tested in cancer patients. In this system, 111In could not simply be substituted with 90Y, because the anti-DTPA mAb used (clone 734) is specifically reactive with cyclic anhydride DTPA, which was reacted with an amino group and subsequently labeled with 111In. First, such a DTPA moiety labeled with 90Y will not be stable in vivo. Second, the 734 mAb has a reduced affinity for DTPA labeled with 90Y. Therefore, for pretargeted radioimmunotherapy, the di-DTPA-tyrosyl-lysine peptide was labeled with 131I. Five patients with medullary thyroid carcinoma and 5 patients with small cell lung carcinoma (SCLC) whose tumors were pretargeted with the anti-CEA × anti-DTPA-indium bsmAb received a diagnostic dose (222–370 MBq) of 131I-labeled di-DTPA. Dosimetric analysis of the images revealed that the radiation dose to the medullary thyroid carcinoma lesions was much higher (range, 113–470 Gy/MBq [4.2–174 cGy/mCi]) than the radiation dose to the SCLC lesions (range, 4.6–22 Gy/MBq [1.7–8 cGy/mCi]), indicating that medullary thyroid carcinoma is a more suitable target for this pretargeted radioimmunotherapy (80). The feasibility and therapeutic efficacy of pretargeted radioimmunotherapy (pretargeting with 20–50 mg of anti-CEA × anti-DTPA-indium bsmAb and with 1.48–3.7 GBq of 131I-di-DTPA 4 d later) was tested in 26 patients with recurrent medullary thyroid carcinoma. Dose-limiting toxicity was hematologic; an activity dose of 1.78 GBq/m2 could be administered safely. The radiation dose to the tumor ranged from 7.9 to 500 Gy/MBq (2.91–184 cGy/mCi). Minor tumor responses were observed in 30% of the patients who could be evaluated (81). As expected, in a pretargeted radioimmunotherapy study in patients with SCLC (n = 14), the radiation doses to the tumor have been lower, 7.0–87 Gy/MBq (2.6–32.2 cGy/mCi) (Fig. 7) (81). Interestingly, the maximum tolerated dose of the 131I-labeled di-DTPA peptide in these patients was much higher (5.55 GBq), possibly because most medullary thyroid carcinoma patients have micrometastatic disease in the bone marrow. In that study on SCLC patients (81), the activity dose is further escalated, until second organ toxicity. From these patients, stem cells are harvested before treatment and reinfused 10–15 d after injection of the radioactivity. So far, 2 of 12 patients who could be evaluated showed a partial response.

Scintigraphic images of patient with metastasized SCLC who received 100 mg/m2 anti-DTPA × anti-CEA F(ab′)2 bsmAb. Seven days later, therapeutic dose (3.7 GBq) of 131I-labeled bivalent hapten was injected. Anterior (A) and posterior (B) images obtained 5 d after injection of radiolabel clearly show accumulation of radiolabel in SCLC lesions in liver.
This pretargeting approach is being further optimized. The use of histamine-hemisuccinate, instead of DTPA, as a hapten allows the use of other more potent radionuclides, such as 188Re, in this strategy. New DOTA-conjugated peptides are being developed that will allow the use of 90Y and 177Lu (64,72,82). Furthermore, humanized bsmAb constructs are being developed that will prevent the development of human antimurine antibody against the bsmAb, as has been observed in most patients who received the anti-CEA × anti-DTPA F(ab′)2 bsmAb (65). Humanized bsmAbs will allow multiple treatment cycles of pretargeted radioimmunotherapy.
PRETARGETED PET IMAGING
A group at the German Cancer Center in Heidelberg developed agents to apply bsmAb pretargeting for PET using the short-lived positron emitter 68Ga (half-life, 68 min) (83,84). mAbs against a gallium chelate were developed (85). Using these mAbs, antichelate × antitumor bsmAbs were developed either chemically (83,86) or biologically (87). With these bsmAbs, pretargeted PET was tested on nude mice with CD44v6- and MUC1-expressing tumors (83,86,88). Recently, this approach was tested on 10 patients with breast cancer. Patients received 10 mg of anti-MUC1 × anti-Ga-chelate bsmAb intravenously, and 18 h later Ga-chelate–substituted human apotransferrin was injected as a blocking agent. Fifteen minutes afterward, 222–296 MBq 68Ga-chelate were administered. PET images were acquired 60–90 min later. Fourteen of 17 known lesions (25 ± 16 mm) were visualized (84). The relatively low uptake of the 68Ga-chelate in the tumor and the low ratios of tumor to normal breast (0.003 %ID/g and 3.0, respectively) were attributed to the shedding of the MUC1 antigen and the comparatively low affinity of the anti-MUC1 mAb (1.2 × 10−7 per mole).
CONCLUSION
In comparison with directly labeled antitumor mAbs, mAb-based pretargeting strategies can enhance the radiation dose to the tumor in radioimmunotherapy.
Therapeutic studies on various groups of cancer patients have shown that the avidin/biotin- or SA/biotin-based approach developed in Milan can induce meaningful therapeutic responses. The radioimmunotherapeutic approach using the mAb–SA conjugates has been tested in only a limited number of patients using an appropriate mAb, and the therapeutic efficacy has yet to be determined. The latter method has the advantage that only 3 injectates are used and that, therefore, the optimization of this approach in terms of dosing and timing will be less complicated. The availability of a new generation of well-defined reagents for this approach (synthetic clearing agent and mAb–SA fusion proteins) is another important step toward clinical applicability of this approach.
Although pretargeted radioimmunotherapy using bsmAb constructs is still in its early phase, promising results have already been obtained with this approach. A major advantage of this pretargeting strategy is that only 2 reagents, the bsmAb and the radiolabeled bivalent hapten, are used. In addition, with the development of humanized bsmAb constructs, this method makes use of reagents that will not evoke an antibody response in patients. The patient groups that will benefit most from this approach have yet to be determined.
Acknowledgments
The authors thank Drs. Hazel B. Breitz and Robert M. Sharkey for their thoughtful suggestions and Drs. Giovanni Paganelli and Jean-François Chatal for generously providing Figures 3 and 7.
Footnotes
Received Mar. 28, 2002; revision accepted Sep. 25, 2002.
For correspondence or reprints contact: Otto C. Boerman, PhD, Department of Nuclear Medicine, University Medical Center Nijmegen, P.O. Box 9101, 6500 HB Nijmegen, The Netherlands.
E-mail: O.Boerman{at}nucmed.umcn.nl
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/education/ce_online.html) THROUGH MARCH 2004.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- THE CONCEPT OF PRETARGETING
- PRETARGETING BASED ON BIOTIN AND AVIDIN
- THE MILAN EXPERIENCE
- THE NeoRx APPROACH
- THE ROLE OF ENDOGENOUS BIOTIN AND BIOTINIDASE
- PRETARGETING WITH BISPECIFIC mAbs (bsmAbs)
- bsmAb-BASED PRETARGETED RADIOIMMUNOTHERAPY IN PATIENTS
- PRETARGETED PET IMAGING
- CONCLUSION
- Acknowledgments
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- A Pretargeted PET Imaging Strategy Based on Bioorthogonal Diels-Alder Click Chemistry
- Effect of Small-Molecule-Binding Affinity on Tumor Uptake In Vivo: A Systematic Study Using a Pretargeted Bispecific Antibody
- 124I-huA33 Antibody Uptake Is Driven by A33 Antigen Concentration in Tissues from Colorectal Cancer Patients Imaged by Immuno-PET
- Pretargeted 177Lu Radioimmunotherapy of Carcinoembryonic Antigen-Expressing Human Colonic Tumors in Mice
- Pretargeted Immuno-Positron Emission Tomography Imaging of Carcinoembryonic Antigen-Expressing Tumors with a Bispecific Antibody and a 68Ga- and 18F-Labeled Hapten Peptide in Mice with Human Tumor Xenografts
- A comparative analysis of conventional and pretargeted radioimmunotherapy of B-cell lymphomas by targeting CD20, CD22, and HLA-DR singly and in combinations
- Introduction to the Eleventh Conference on Cancer Therapy with Antibodies and Immunoconjugates
- Optimization of Radioimmunotherapy of Solid Tumors: Biological Impediments and Their Modulation
- Bispecific Antibody Pretargeting of Tumor Neovasculature for Improved Systemic Radiotherapy of Solid Tumors
- Successful Radiotherapy of Tumor in Pretargeted Mice by 188Re-Radiolabeled Phosphorodiamidate Morpholino Oligomer, a Synthetic DNA Analogue.
- Antibody Pretargeting Advances Cancer Radioimmunodetection and Radioimmunotherapy
- Radioimmunotherapy of Solid Tumors: The Promise of Pretargeting Strategies Using Bispecific Antibodies and Radiolabeled Haptens
- Targeting, Toxicity, and Efficacy of 2-Step, Pretargeted Radioimmunotherapy Using a Chimeric Bispecific Antibody and 131I-Labeled Bivalent Hapten in a Phase I Optimization Clinical Trial
- Pretargeted Radioimmunotherapy with a Single-Chain Antibody/Streptavidin Construct and Radiolabeled DOTA-Biotin: Strategies for Reduction of the Renal Dose
- Intraperitoneal Pretarget Radioimmunotherapy with CC49 Fusion Protein
- Therapeutic Advantage of Pretargeted Radioimmunotherapy Using a Recombinant Bispecific Antibody in a Human Colon Cancer Xenograft
- Introduction to the Tenth Conference on Cancer Therapy with Antibodies and Immunoconjugates
- Improving the Delivery of Radionuclides for Imaging and Therapy of Cancer Using Pretargeting Methods
- Enhanced Efficacy of Radioimmunotherapy with 90Y-CHX-A''-DTPA-hu3S193 by Inhibition of Epidermal Growth Factor Receptor (EGFR) Signaling with EGFR Tyrosine Kinase Inhibitor AG1478
- Radioimmunotherapy of Prostate Cancer: Does Tumor Size Matter?
- Residualizing Iodine Markedly Improved Tumor Targeting Using Bispecific Antibody-Based Pretargeting
- Novel Avidin-like Protein from a Root Nodule Symbiotic Bacterium, Bradyrhizobium japonicum
- The Direct Route May Not Be the Best Way to Home
- Perspectives on Cancer Therapy with Radiolabeled Monoclonal Antibodies
- Pretargeting with Labeled Bivalent Peptides Allowing the Use of Four Radionuclides: 111In, 131I, 99mTc, and 188Re