


Abstract
PET is a unique form of diagnostic imaging that observes in vivo biologic changes using radiopharmaceuticals that closely mimic endogenous molecules. 18F-FDG, which allows the evaluation of glucose metabolism, is the most commonly used tracer in oncology because of the practical half-life of 18F (110 min), compared with other short-lived positron emitters. 18F-FDG uptake in tumors is proportional to the glycolytic metabolic rate of viable tumor cells indicating the increased metabolic demand of tumors for glucose. 18F-FDG PET significantly improves the accuracy of imaging tumors in initial staging, management of recurrent cancer, and monitoring of therapy response. The information provided by this technique is more sensitive and specific than that provided by anatomic imaging modalities. 18F-FDG PET is particularly superior to CT or MRI in the ability to evaluate the effectiveness of various treatment regimens early during therapy or after therapy. In this review, we discuss the role of 18F-FDG PET in evaluating the response to therapy and the impact of this information on patient management.
The primary goal of nonsurgical therapy of cancer is the complete eradication of tumor cells through the cytocidal effect of chemotherapy, radiotherapy, hormonal therapy, or biologic therapy. The tumor response to therapy varies widely, however. Differences in tumor response can be caused by disparities in tumor biology, such as growth phase, tumor volume, oxygenation, heterogeneity, presence of drug resistance mechanisms, and radio- or chemosensitivity. It would be most advantageous to identify resistant or nonresponding tumors early during or immediately after therapy to institute a timely alternative treatment that may be more effective. In advanced cancers in particular, systemic anticancer therapy has an evolving role in efforts to increase survival. High-dose chemotherapy with growth factors to stimulate bone marrow recovery after chemotherapy can be an option, as has been shown in breast cancer. Another alternative therapy, so-called tailor-made drug selection, can be based on tumor characteristics specific to the individual patient by determining tumor cell viability after incubation with various cytotoxic agents. Furthermore, emerging novel therapies, including immunotherapy, cancer vaccines, and biologic therapy with cytokines, are entering the oncologic arena as alternative approaches.
The efficacy of a treatment is a direct function of tumor burden (1). Hence, detection of residual tumors at a subclinical level or at a small volume is beneficial to optimize the efficacy of subsequent therapy. Unnecessary morbidity associated with treatment toxicity could also be avoided in patients with a short expected survival and at high risk of experiencing serious side-effects if it is determined that the therapy will fail. Response to therapy is currently evaluated using conventional imaging (CI) modalities. However, the definition of tumor response or progression, using anatomic imaging modalities, is based on size criteria. The disease activity may have completely resolved after therapy, but residual masses may persist on morphologic imaging as resolution of therapy-induced anatomic changes lags behind tumor cell mortality. PET is currently the most sensitive and specific imaging method to obtain information about tumor physiology and metabolism. Tumor cells have increased glucose metabolism due to increased expression of glucose transporters and hexokinase (glucose phosphorylating enzyme) as a result of oncogenic transformation. After phosphorylation, 18F-FDG is essentially trapped within the cell because of 2 phenomena: 18F-FDG is not a substrate for subsequent pathways that take place in glycolysis, and dephosphorylating enzyme—glucose-6-phosphatase—is either scarce or absent in cancer tissue. Therefore, the cellular concentration of 18F-FDG in tumor represents the glycolytic activity of viable tumor cells. Additionally, the results of a recent study revealed that the activity of tumor hexokinase is a marker of tumor growth rate that can be determined by 18F-FDG PET. Consequently, 18F-FDG PET may provide important prognostic information about the proliferative rates and, therefore, the antiproliferative effect of cancer therapy (2). There is now convincing evidence that reduction or resolution of 18F-FDG uptake in the tumor is an early indicator of response at a clinical or subclinical level (3–7).
Anticancer therapy is frequently individualized, as it is directed toward specific targets depending on the characteristics of the tumors. 18F-FDG PET may provide better and more timely assessment of the efficacy of various specific therapies that may result in significant clinical management alterations.
ASSESSMENT OF RESPONSE TO THERAPY
Monitoring response to therapy requires acquisition of a baseline 18F-FDG PET study before therapy and repeating 18F-FDG PET during or after the completion of therapy. The exact timing of 18F-FDG PET reimaging can be challenging because of the variability in tumor sensitivity to different treatment modalities. In fact, this matter is still in evolution. The method of quantifying tumor 18F-FDG uptake also varies greatly. Some guidelines have been developed in an attempt to standardize acquisition and response criteria for post-therapy changes in 18F-FDG tumor uptake to predict response to therapy (8). Biodistribution of 18F-FDG can be affected by various physiologic factors. Blood glucose levels have an impact on 18F-FDG uptake through the competitive displacement of 18F-FDG by plasma glucose. Patients should fast 4–6 h to reduce competition with plasma glucose and thus optimize and standardize tumor 18F-FDG uptake. There is no consensus on the optimal procedure for adjusting glucose levels in diabetic patients. In patients with type I diabetes, insulin is not recommended; in patients with type II diabetes, insulin may be administered at the discretion of the physician, although physiologic muscle uptake is exaggerated by insulin administration. Because the primary route of 18F-FDG excretion is renal, good hydration is required before imaging to encourage urinary excretion. It is recommended that patients drink 500 mL of water after injection of 18F-FDG. Muscle relaxants may be used to reduce muscle uptake, especially in patients with head and neck tumors, in whom uptake by tense cervical muscles may occur. Patients should remain silent during and after injection to reduce laryngeal muscle uptake, which may be confused with a residual or recurrent head and neck tumor.
Evaluation of response to therapy involves careful comparison of pretreatment and post-treatment 18F-FDG PET scans. Imaging 1–2 wk after completion of therapy is recommended to avoid transient fluctuations in 18F-FDG metabolism. When 18F-FDG PET is performed during the course of chemotherapy, current data indicate that images can be obtained as early as after 1 or 2 cycles of therapy (5,6,9–12). The relationship between radiotherapy and changes in tumor 18F-FDG uptake has yet to be established.
Interpreting 18F-FDG tumor uptake after therapy may be confounding at times because of therapy-related changes. In the post-therapy setting, approximately 25% of 18F-FDG uptake can occur in nontumor tissues such as macrophages, neutrophils, fibroblasts, and granulation tissue (13). In vitro assays demonstrate that irradiated tumor cells might have a tenfold increased 18F-FDG uptake (14). In colon cancer, it is recommended that 18F-FDG PET studies be delayed for 60 d after the completion of radiotherapy to accurately assess its outcome (14–16). Generally 18F-FDG uptake 6 mo after radiotherapy is associated with tumor recurrence. Transient and reversible cell damage as well as minimal residual disease may obscure assessment of the true cell kill in the tumor mass (13,14). The negative predictive value of post-therapy 18F-FDG PET is therefore usually lower than the positive predictive value. More important, tumor perfusion and delivery of 18F-FDG into the tumor may be affected to the same extent by both necrosis and therapy-induced changes.
There are essentially 2 types of methods to analyze 18F-FDG uptake by tumor: visual, or qualitative, assessment and quantitative analysis. The most straightforward method is dichotomous visual evaluation to differentiate malignant processes from benign lesions. This approach, however, is subjective, requires substantial experience, and is not sufficient for subtle findings. Alternatively, graded visual assessment results in less interobserver variability, provided that well-defined criteria are available for positive and negative findings.
Although visual evaluation is valuable and practical, 18F-FDG PET benefits significantly from quantitative assessment of uptake, particularly in predicting outcome by determining tumor aggressiveness and monitoring therapy response. Nevertheless, the optimal method for quantitating prognosis and assessing response to therapy has not yet been defined. Quantitation can be approached in several ways, from simple tumor-to-background calculations to intricate kinetic analyses with dynamic PET acquisitions and blood sampling (17). Currently, it is not clear whether more advanced quantitation techniques are superior to more basic methods in the prediction of prognosis and therapy response, mainly because of the insufficient 18F-FDG PET data obtained thus far on the assessment of various tumors.
All quantitation methods entail attenuation correction to avoid the variability in 18F-FDG uptake due to the differences in tumor depth in the body. Determination of ratios of tumor to normal tissue is the simplest means of quantitation. This method can be applied to images even after reconstruction without the requirement of additional procedures or information. Although this approach is more objective than visual assessment, it significantly limits the placement of regions of interest versus background and the use of count statistics and reconstruction algorithms. A more accurate way of measuring tumor 18F-FDG uptake involves the determination of standardized uptake value (SUV), which has been widely used for the measurement of 18F-FDG uptake by tumors. This value normalizes 18F-FDG tumor uptake with injected activity (Qinj) and body weight (W), providing a semiquantitative index of 18F-FDG uptake (SUV = Q × W/Qinj) (18). SUV depends, however, on body weight. Correction with lean body mass is therefore required to avoid erroneous comparisons that can stem from changes in pre- and post-therapy body weight in the same patient. In calculating SUVs, the administered dose, corrected for residual activity in syringe and tubing, must also be accurately determined and the dose must be decay corrected to the time of imaging.
More objective and reliable quantitative methods are available, including simplified kinetic analysis (19), Patlak graphical analysis (20), and kinetic analysis with parameter optimization. Nonetheless, considering the practical constraints, these methods are unlikely to find clinical applications. Kinetic modeling has been used to determine the rate of glucose metabolism over time, expressed in μmol/min/mL. This technique is more demanding because it requires arterial catheterization and rapid blood sampling. Using dynamic PET, the net metabolic clearance of 18F-FDG is calculated by the time course of the radioactivity concentrations in tissue and arterial blood. A more promising development has been the demonstration that blood sampling can be replaced by time-activity curves based on dynamic scanning of the blood pool. This type of analysis requires that the aorta be in the field of view during the acquisition of dynamic PET for calculation of the net metabolic clearance of 18F-FDG (21,22). In quantitative analysis, heterogeneous tumor constitution with varying 18F-FDG kinetics may affect the measurement of glucose metabolic rate.
In the post-therapy setting, high sensitivity is preferable to specificity because the consequences of a false-negative interpretation are less desirable than those of a false-positive interpretation. In this regard, the threshold set for positivity depends on multiple variables such as tumor type, interval after therapy, and type of therapy. The required interval for post-therapy evaluation with 18F-FDG PET may be longer for radiotherapy than for chemotherapy, during which treatment response can be assessed even early.
PET is the most favorable noninvasive diagnostic means to assess tumor metabolic status after therapy and determine the presence of residual tumor. Several studies have illustrated that 18F-FDG uptake is an independent predictor of outcome and survival. Findlay et al. showed that pretreatment SUVs do not correlate with tumor response, although response is associated with lower 4- to 5-wk SUVs in patients with liver metastases from colorectal cancer (5). In studying lung cancer, Dhital et al. reported that SUV is of prognostic value before surgical resection (23). An SUV of 20 or more was associated with a 4.7 times increase in poor prognosis, compared with lower levels of SUV; however, Dhital et al. found no significant correlation between tumor histology and SUVs. In patients with lymphoma, Cremerius et al. found that a tumor SUV of greater than 11 is associated with poorer progression-free survival than are lower tumor SUVs (24). Although these studies indicate that quantitative PET has considerable potential in predicting prognosis and therapy outcome, they also suggest that different types of tumors require different methods of analysis.
Alterations in 18F-FDG uptake as measured by various methods, including visual and quantitative analyses, provide useful information on response to anticancer therapy. The area in which quantitative PET will have its greatest impact is, in fact, the assessment of response to therapy. However, determining which method is more specific and superior for monitoring response is difficult because of the inconsistencies in these analytic methods between investigators. As more tumor-specific markers are developed, more accurate information will be obtained from quantitative analysis of PET images.
CLINICAL STUDIES MONITORING RESPONSE TO THERAPY
Lymphoma
Hodgkin’s disease (HD) and non-Hodgkin’s lymphoma (NHL) compose only 8% of all malignancies, and they are frequently curable. Histology and the extent of the disease (staging) are important factors influencing prognosis and therapy success (25,26).
Patients Who Will Benefit from Monitoring Response to Therapy.
Surgical treatment is not an option in lymphoma. Therapeutic implications for patients with HD and NHL emphasize the importance of initially staging the disease accurately. Patients diagnosed with early-stage HD and NHL are treated with combination chemotherapy and radiotherapy or radiotherapy alone, whereas those with stage III or IV disease are typically treated with aggressive chemotherapy. In early-stage lymphoma, 75%–90% of patients respond to therapy regardless of the histologic subtype; however, in advanced-stage lymphoma, less than 50% of newly diagnosed patients are curable with standard treatments (27,28). Hence, evaluation of response to therapy is vital in patients with advanced-stage disease. There is an advantage to assessing the response to therapy early during chemotherapy, since early evidence of persistent disease may suggest that innovative intervention such as bone marrow transplantation be used in advanced-stage lymphoma. Early recognition of resistance to chemotherapy can also result in lower cumulative treatment toxicity and tumor burden at the start of salvage therapy, potentially improving clinical outcome.
Prediction of Response to Therapy After Its Completion.
Residual abnormalities frequently occur after therapy in up to 64% of patients with lymphoma (29). Although residual masses are usually considered to be persistent disease, a maximum of 18% of residual masses are found to harbor viable lymphoma after therapy (29). Currently, 18F-FDG PET is considered to be more accurate than anatomic imaging modalities in assessing treatment effects to correctly identify patients with residual disease and predict therapy outcome (Table 1; Figs. 1 and 2) (9,10,24,30–38). As a CI modality, 67Ga imaging is an independent predictor of outcome in lymphoma early during chemotherapy (39,40). The value of 67Ga in evaluating response to therapy in intra-abdominal tumors and low-grade lymphoma, however, is unclear. 18F-FDG PET can identify nonresponders more accurately than can CT. Nevertheless, after completion of chemotherapy, 18F-FDG PET may not exclude the presence of minimal residual disease, which may lead to a later relapse. In a previous study, comparing 18F-FDG PET and CT in a post-therapy setting, relapse occurred in all patients with positive post-therapy 18F-FDG PET findings and in only 26% of patients with residual masses observed on CT. Consequently, the positive predictive values for 18F-FDG PET and CT were 100% and 42%, respectively, after the completion of therapy (36). In this study, positive 18F-FDG PET findings after therapy were consistently associated with poorer survival than were negative findings, with 1-y progression-free survivals of 0% and 86%, respectively (36). The prognostic significance of post-therapy 18F-FDG PET has been assessed, so far, in patients with various lymphoma subtypes and stages. In a study by Cremerius et al., the population consisted of patients referred for reevaluation within 3 mo of completion of therapy, as well as those with suspected relapse or residual masses who presented within 12 mo of completion of therapy (24). In this mixed group, progression was observed in 84% of patients after a median interval of 2 mo. Among patients with negative 18F-FDG PET findings, only 13% had disease progression after a median follow-up of 21 mo. Positive post-therapy 18F-FDG PET findings were associated with poorer progression-free survival. Although the results of this study indicate that 18F-FDG PET has a high prognostic value in lymphoma, the study design suffers from a heterogeneous patient population. 18F-FDG PET may prove more useful in patients who are at a higher risk for disease recurrence. 18F-FDG PET evidence of persistent disease may prompt alternative therapy regimens in the poor-prognosis group. Supporting this view was the finding that 18F-FDG PET predicted complete remission better in moderate-risk patients (stage I–III, no relapse, no more than 2 different prior therapy regimens) than in high-risk patients, with negative predictive values of 90% versus 50%–67% (30).

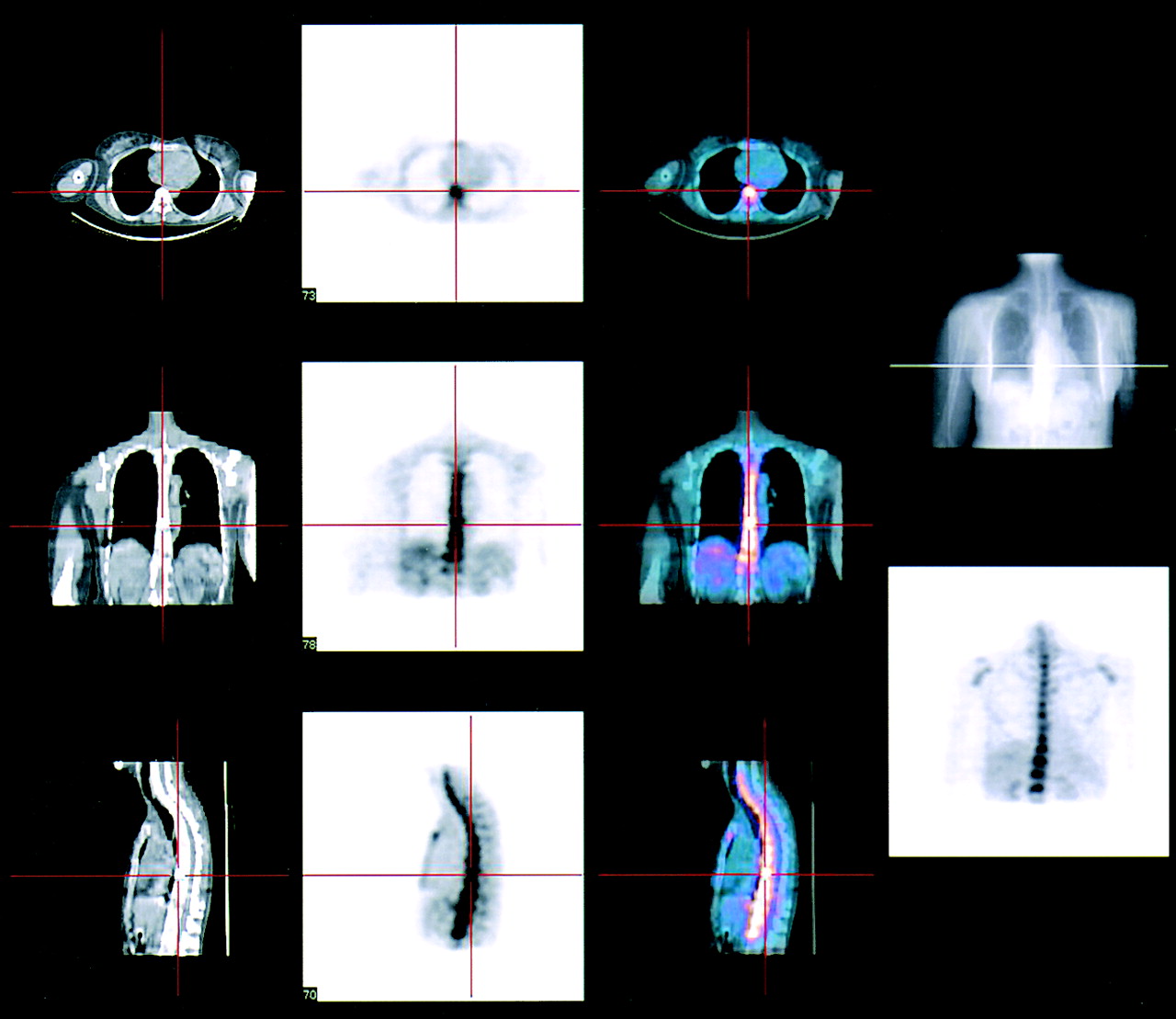
A 45-y-old man with NHL (diffuse large cell) underwent 18F-FDG PET simultaneously with CT using dual-head system (Millennium VG, Hawkeye [inbuilt CT scanner]; General Electric Medical Systems, Milwaukee, WI) before and after completion of chemotherapy (cyclophosphamide, hydroxydaunomycin, vincristine sulfate, and prednisone). Pretherapy 18F-FDG PET/CT images reveal intense 18F-FDG uptake in right supraclavicular region and right anterior mediastinum. Note physiologic uptake in myocardium.
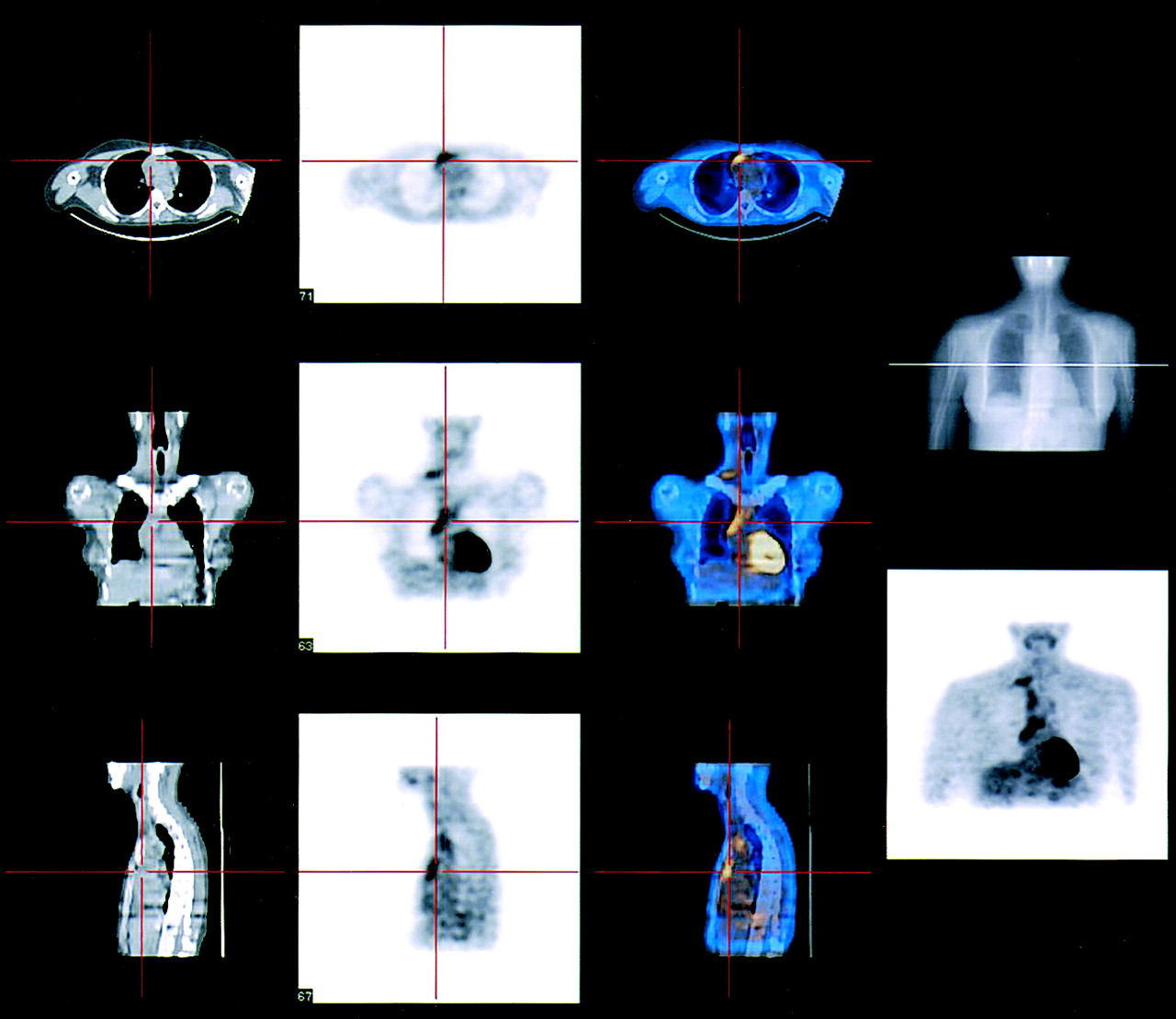
Post-therapy 18F-FDG PET/CT study of same patient as in Figure 1, acquired using same system. There is no appreciable 18F-FDG uptake in mediastinum (especially in transverse and sagittal images) to suggest residual lymphoma. Note intense 18F-FDG uptake in bone marrow in shoulder joints, sternum, and thoracic vertebrae, consistent with post-therapy reactive bone marrow changes. Patient is still in remission after progression-free survival of 18 mo.
18F-FDG PET in Detection of Residual Lymphoma After Therapy
In a more recent study, Spaepen et al. evaluated the value of 18F-FDG PET in detecting residual disease and, thus, predicting relapse after completion of first-line chemotherapy in 93 patients (32). After first-line chemotherapy, 83.5% of patients with negative 18F-FDG PET findings remained in complete remission after a median follow-up of 653 d. Only 16% of patients had relapse of disease after negative 18F-FDG PET findings, with a median progression-free survival of 404 d. 18F-FDG PET showed persistent uptake in 26 patients, all of whom had relapse, with a median progression-free survival of 73 d. The authors concluded that persistent 18F-FDG uptake after first-line chemotherapy in NHL was highly predictive of residual or recurrent disease. Among patients with disease relapse, disease-free survival was clearly shorter in patients with positive 18F-FDG PET findings than in those with negative findings.
The prognostic value of pretherapy 18F-FDG PET was also evaluated in patients with HD and aggressive NHL undergoing high-dose therapy with stem cell transplantation. In 18F-FDG PET-negative patients, relapse-free survival was 100% at 12 mo, whereas in 18F-FDG PET-positive patients, the respective value was 18%. The authors concluded that 18F-FDG PET is accurate in the prediction of relapse before high-dose therapy with stem cell transplantation in patients with lymphoma (33).
In 1 study, HD was evaluated in an unmixed patient group. Weihrauch et al. studied the diagnostic and prognostic value of 18F-FDG PET performed at least 3 mo after therapy on 28 HD patients with residual mediastinal masses determined by CT (34). The results indicated that patients with negative 18F-FDG PET findings after therapy were unlikely to have disease relapse within a year. The negative and positive predictive values at 1 y for 18F-FDG PET were 95% and 60%, respectively. This particular study emphasized the high false-positive rates obtained in HD with post-therapy 18F-FDG PET (34). These results were, however, derived from a very small population that had positive post-therapy 18F-FDG PET findings. Additionally, in this younger age group false-positive findings may be due to thymus hyperplasia, which is a well-known phenomenon (41).
Early Prediction of Response to Therapy.
Preliminary studies suggest that 18F-FDG PET can distinguish responders from nonresponders early into the course of chemotherapy or immunotherapy in patients with lymphoma. The extent and time course of changes in 18F-FDG uptake in response to chemotherapy were studied by Romer et al. (9). Dynamic 18F-FDG PET was performed on 11 patients at baseline and 1 and 6 wk after the initiation of chemotherapy. One week after the initiation of chemotherapy, tumor 18F-FDG uptake decreased by 60%. A further decrease of 42% was observed at 6 wk, resulting in a total decrease of 79% from baseline. During a follow-up of 16.0 ± 4.2 mo, approximately 54% of patients continued to show complete remission. Seven days after initiation of chemotherapy, this group of patients displayed a significantly lower mean 18F-FDG metabolic rate than did the group of patients with relapse. At 6 wk, all parameters of 18F-FDG uptake showed a significant difference for both patient groups. The relative change of 18F-FDG metabolic rate from baseline to week 6, as well as from week 1 to week 6, was significantly larger, compared with SUV parameters. Standard chemotherapy of patients with NHL causes a rapid decrease of tumor 18F-FDG uptake as early as 1 wk after treatment, and uptake continues to decline during therapy, indicating the sensitivity of metabolic signals to chemotherapeutic interventions.
A recent study demonstrated that 18F-FDG PET has a high prognostic value for evaluation of therapy as early as after 1 cycle in aggressive NHL and HD (10). Ninety percent of patients with positive 18F-FDG PET findings after 1 cycle had disease relapse with a median progression-free survival of 5 mo, whereas 85% of patients who had negative 18F-FDG PET findings remained in complete remission after a minimum follow-up of 18 mo. All patients with persistent 18F-FDG uptake both after the first cycle and at completion of therapy had relapse, except 1 patient who had a thymic rebound. The progression-free survival was significantly different between patients with negative and patients with positive 18F-FDG PET findings after 1 cycle of treatment. After completion of chemotherapy, although there was a statistically significant difference in progression-free survival between patients with negative and patients with positive findings, the findings after completion of chemotherapy yielded a significantly lower sensitivity and negative predictive value than did the findings after the first cycle (Fig. 3). In this study, the relapse rate for patients with negative 18F-FDG PET findings at the completion of therapy was higher than the relapse rate for patients with negative 18F-FDG PET findings after the first cycle (35% vs. 15%). The potential of 18F-FDG PET to predict outcome in patients with aggressive lymphoma and HD early during therapy, compared with after completion of therapy, is most likely due to the sensitivity of these lymphomas to chemotherapy. A positive 18F-FDG PET result after 1 cycle reflects the metabolic activity of potentially resistant clones, which, although responding to chemotherapy, do so more slowly than do those homogeneously sensitive tumor cells. This study provides a strong argument for consideration of further trials to evaluate a subsequent change in treatment based on the 18F-FDG PET results (10).

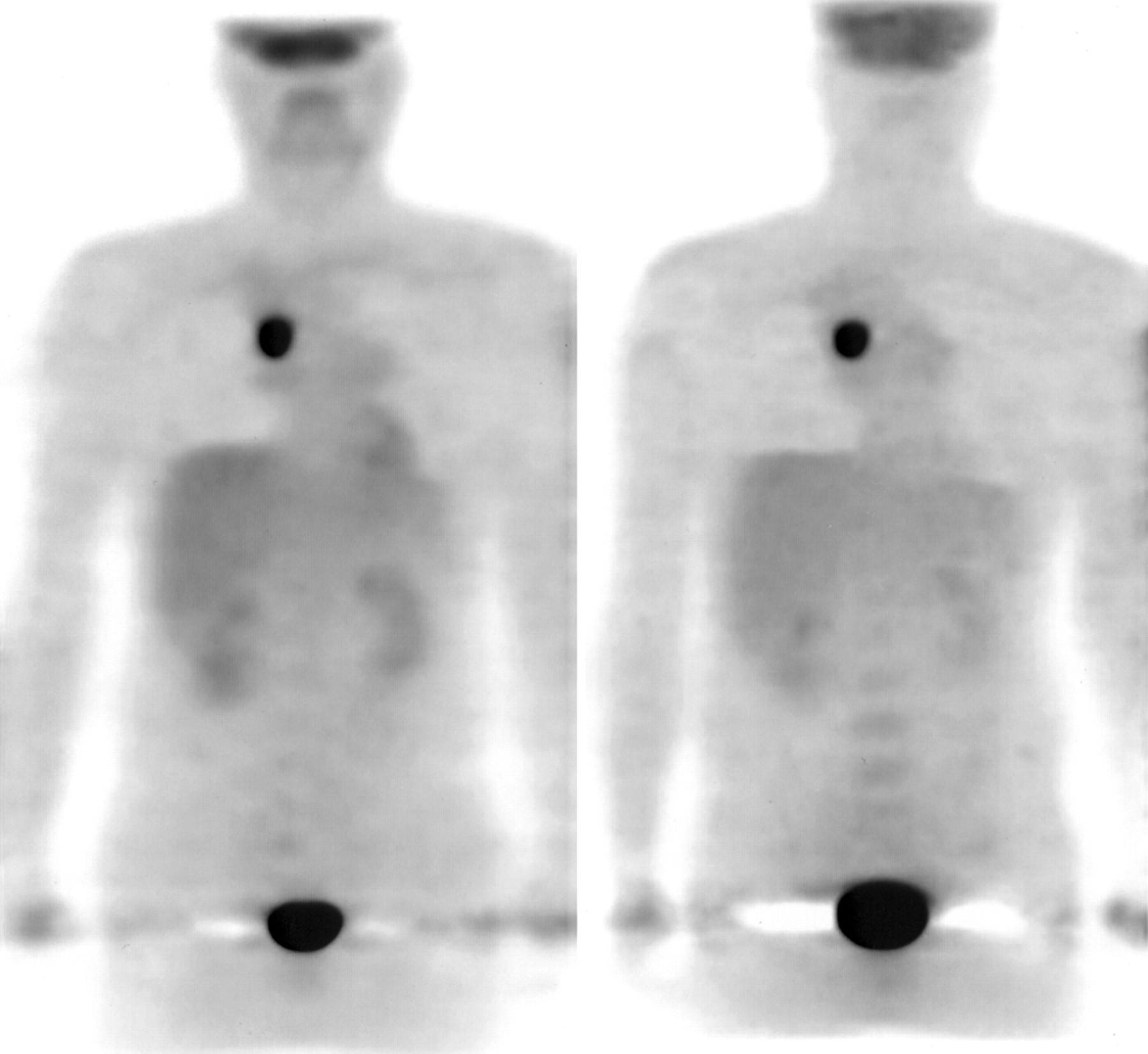
A 55-y-old man with NHL (diffuse large cell) underwent 18F-FDG PET using dual-head gamma camera with attenuation correction (MCD-AC; ADAC Laboratories, Milpitas, CA) before, after first cycle of, and at completion of chemotherapy. Pretherapy 18F-FDG PET image reveals extensive radiotracer uptake in anterior mediastinum. Note physiologic uptake in supraclavicular cervical muscles. Patient underwent chemotherapy with cyclophosphamide, hydroxydaunomycin, vincristine sulfate, and prednisone. After first cycle, residual disease was seen in anterior mediastinum (not shown). 18F-FDG PET image after last cycle (middle image) demonstrates no residual mass in mediastinum, consistent with complete resolution of disease. 18F-FDG PET image 8 mo after completion of therapy, however, reveals recurrence of disease in anterior mediastinum. Note physiologic uptake in heart in all images.
18F-FDG PET has been compared with CT in the assessment of remission after treatment of aggressive NHL (35). In a subset of patients, the prognostic value of interim 18F-FDG PET performed after 2–3 cycles of chemotherapy was also evaluated. Not surprisingly, post-treatment 18F-FDG PET was more accurate than CT in assessing remission status after treatment. The respective relapse rates were 100% and 18% for positive and negative 18F-FDG PET results, compared with 41% and 25% for patients with positive and negative CT results, with a median follow-up of 30 mo. Interim 18F-FDG PET revealed no relapses in patients with no or minimal residual uptake, compared with an 87.5% relapse rate in patients with persistent PET activity. The authors concluded that 18F-FDG PET is a more accurate method than CT in assessing remission and estimating prognosis after treatment of aggressive NHL. An interim PET scan after 2–3 cycles of chemotherapy may assist in separating good-prognosis patients, who are likely to be cured with standard chemotherapy, from patients with a poorer prognosis, who require alternative treatment (35). In another study with a similar design, 28 NHL patients were studied for early evaluation of response by 18F-FDG PET performed after a median of 3 cycles of chemotherapy. Persistent tumor 18F-FDG uptake after several cycles of chemotherapy was predictive of clinical remission, progression-free survival, and overall survival. All patients with residual 18F-FDG uptake and 33% of patients without residual 18F-FDG uptake had disease relapse or progression, with a positive predictive value of 100% and a negative predictive value of 67%. Mean progression-free survivals at 1 and 2 y were, respectively, 20% and 0% for 18F-FDG PET-positive patients and 81% and 62% for 18F-FDG PET-negative patients. However, the sensitivity of qualitative 18F-FDG PET in identifying patients with a poor outcome was insufficient (36).
Radioimmunotherapy, with 131I-labeled anti-B1 antibody developed against the surface antigen CD20, has been recognized as a promising approach for treatment of low-grade NHL (42). The tumor response to radioimmunotherapy may be more gradual than the tumor response to chemotherapy. The prognostic value of 18F-FDG PET was evaluated in 14 patients with NHL treated with 131I-anti-B1 therapy. All patients underwent 18F-FDG PET at baseline, 5–7 d, and 1–2 mo after radioimmunotherapy to estimate the response to radioimmunotherapy. 18F-FDG PET metabolic data obtained 1–2 mo after radioimmunotherapy correlated well with the ultimate response of NHL to radioimmunotherapy. The correlation was more significant than that of the early 18F-FDG PET data obtained 5–7 d after radioimmunotherapy (37).
False-Positives.
Reactive lymph nodes and inflammatory or infectious processes may cause false-positive findings. Anti-inflammatory cells such as activated macrophages or granulation tissue that are present in areas of inflammation have been shown to avidly take up 18F-FDG. Although 18F-FDG PET is sensitive for identifying disease sites in the chest, false-positive 18F-FDG uptake after therapy can be seen at the site of thymic hyperplasia (41). Also, infectious or inflammatory processes such as toxoplasmosis, Mycobacterium tuberculosis, fungi, and sarcoidosis in the extranodal organs, particularly the spleen, can cause false-positive findings (43). Post-therapy reactive bone marrow changes may at times be a potential source of confusion about disease involvement (Fig. 2).
False-Negatives.
18F-FDG PET has been reported to have false-negative results in mucosa-associated lymphoid tissue (44) and in lesions smaller than 1 cm, particularly low-grade lymphoma, although in our series we detected lesions as small as 0.6 cm (45). Although 18F-FDG PET is sensitive in low-grade lymphomas, the degree of uptake can be lower than that observed in intermediate- or high-grade lymphomas. The sensitivity of 18F-FDG PET to detect bone marrow infiltration has been reported to be low (46,47). Because 18F-FDG PET may yield false-positive or -negative results, evaluation of bone marrow should be performed using bone marrow biopsy and MRI, or should be complemented by these, when indicated. Nevertheless, in the evaluation of bone marrow, no single technique is completely reliable. Bone marrow is associated with a high rate of false-negative findings, which can also be obtained with MRI in cases of bone marrow hyperplasia, diffuse lymphoma infiltration, and infectious processes.
Summary.
18F-FDG uptake is predictive of the response to therapy after its completion or early during its course. Patients with a negative PET result after 1 cycle, indicating a good prognosis, would continue with a full course of their first-line treatment, because negative 18F-FDG PET findings may not be sufficiently sensitive in patients with minimal residual disease. Selected patients with a positive 18F-FDG PET result after 1 cycle, and thus a less favorable prognosis, could be randomized to receive second-line chemotherapy with stem cell transplantation without completing a full course of initial chemotherapy.
Breast Carcinoma
Breast carcinoma is the most frequently diagnosed malignancy in women in North America and the second most frequent cause of cancer death (48). The relatively constant mortality, despite increases in incidence, may be the result of improved outcome secondary to earlier diagnosis and advances in treatment and follow-up. If diagnosed early, it is a curable disease.
Patients Who Will Benefit from Monitoring Response to Therapy.
18F-FDG PET should be used as a monitoring tool in patients undergoing induction therapy for advanced disease as well as in those receiving preoperative chemo- or radiotherapy for inoperable localized tumors. Large or locally advanced breast cancer (LABC) may account for 15%–25% of cases of breast cancer (49). The definition of LABC is variable. The investigators include, as LABC patients, all patients with inoperable stage IIIB cancer, whereas patients with operable stage IIIB or stage IV cancer can also be included by virtue of positive supraclavicular lymph nodes. Treatment of LABC should include neoadjuvant or preoperative chemotherapy, since there is evidence that such therapy will significantly increase the number of patients who will benefit from breast-conserving surgery (50,51). Early administration of systemic chemotherapy before local treatment in patients with large or LABC is intended to downstage the primary tumor to render subsequent local treatment (surgery or radiotherapy) more effective and less morbid, as well as to eliminate occult distant metastases. Despite the experimental data indicating the survival benefits of neoadjuvant chemotherapy over postoperative adjuvant chemotherapy, the survival rate is still poor because of failure of chemotherapy (51). Studies have also demonstrated that patients with unresponsive tumors may achieve an improved survival with alternative or more prolonged courses of chemotherapy and the timely initiation of radiotherapy (52). It is essential, therefore, to accurately identify patients who would benefit from alternative treatments during the course of chemotherapy.
Prediction of Response to Therapy After Its Completion.
In a retrospective study of 61 patients, Vranjesevic et al. compared the value of 18F-FDG PET with CI to predict outcome in breast cancer patients who had previously undergone primary therapy. 18F-FDG PET was more accurate than combined CI modalities for predicting outcome, with positive and negative predictive values of 93% and 84%, respectively, for 18F-FDG PET versus 85% and 59%, respectively, for CI modalities (53). The prognostic accuracy of 18F-FDG PET was superior to that of multiple procedures with CI (90% vs. 75%). Disease-free survival differed significantly between patients with negative and patients with positive 18F-FDG PET findings. The estimates of disease-free survival stratified by CI results, however, showed a marginally significant difference between CI-positive and CI-negative patients. The results of this study should be interpreted in a different context because of the significant differences in its design, compared with the designs of other studies. Briefly, this study is retrospective and the population includes patients with different histologic types and stages of breast cancer. The patients underwent a variety of treatments, including chemotherapy and radiotherapy, and follow-up was performed long after the completion of therapy. 18F-FDG PET performed long after therapy can be used to predict the clinical outcome of previously treated patients relative to what is achievable by CI alone.
Early Prediction of Response to Therapy.
The complete pathologic resolution of the tumor after chemotherapy is of considerable prognostic importance and frequently does not correlate with observed clinical response (54,55). In contrast to morphologic imaging modalities, 18F-FDG PET has been reported to detect metabolic changes in breast cancer as early as 8 d after initiation of therapy, preceding appreciable anatomic changes (56). Several studies also indicate that responders may be differentiated from nonresponders using 18F-FDG PET after the first course of chemotherapy (6,11,12). Schelling et al. investigated the predictive value of 18F-FDG PET for evaluating histopathologic response during chemotherapy in patients with LABC (11). Significant differences in tracer uptake were obtained as early as after the first course of chemotherapy between nonresponding and responding tumors. After the first course of chemotherapy, all responders were correctly identified, with a sensitivity of 100% and a specificity of 85%.
Bassa et al. found that 18F-FDG PET was useful in evaluating response to presurgical chemotherapy for the primary LABC tumor in 16 patients (12). The sensitivity for detection of pathologically proven primary lesions was better with 18F-FDG PET (100%) than with mammography (62.5%) or ultrasonography (87.5%). After therapy, however, the sensitivity for 18F-FDG PET was 75%, compared with 71% and 87.5% for mammography and ultrasonography, respectively, for detection of residual primary tumor. A substantial decrease in tumor glucose metabolism of the primary tumor, measured by SUVs, was visible on the 18F-FDG PET images of 69% of patients as early as after the first cycle of chemotherapy. Because of microscopic residual disease, however, the decrease in 18F-FDG uptake did not correlate with favorable clinical outcome for all patients. Thus, 18F-FDG PET was false-negative in 25% of patients with progression of disease at a later course. The main emphasis of this study was that an elevated 18F-FDG uptake at the completion of chemotherapy before surgery correlated with a poor clinical outcome. Patients with persistent 18F-FDG uptake after chemotherapy should be selected for more aggressive therapy and a closer follow-up (12). Similarly, in another study, 18F-FDG PET was able to predict complete pathologic response after a single course of chemotherapy in 30 patients with large tumors (>3 cm), or LABC, with a sensitivity of 90% and a specificity of 74% (57). The mean reduction in relative 18F-FDG uptake after the first course of chemotherapy was significantly greater in lesions that achieved a partial or complete pathologic response than in those with no response or progression. Mean pretreatment glycolytic rates were significantly higher in ultimately responsive cancers. The mean change in relative 18F-FDG uptake and glycolytic rates after the first course of chemotherapy was significantly greater in responding lesions. These conclusions were derived, however, from a small number of patients; thus, the ultimate clinical significance of these results is unknown.
Tiling et al. compared 18F-FDG PET with 99mTc-sestamibi scintimammography (MIBI) in the assessment of tumor response to chemotherapy after the first and second cycles of chemotherapy in 7 patients with LABC (58). These preliminary data demonstrated that MIBI is as useful as 18F-FDG PET for monitoring the response to chemotherapy. Patients with complete remission showed decreased 18F-FDG and MIBI uptake as early as 8 d after therapy, followed by complete disappearance of uptake at the end of therapy. In patients with partial or no response, both techniques showed persistent tumor uptake during chemotherapy. An early decline in glucose or MIBI uptake 8 d after initiation of therapy did not necessarily predict complete remission in all patients. After the second chemotherapy cycle, both techniques were able to distinguish between complete and partial or no response. The results of this study, however, should be evaluated in light of 2 shortcomings: Only 7 patients were studied, and MIBI may have limitations as an imaging agent, particularly in the post-therapy setting. MIBI is a transport substrate for the P-glycoprotein pump system, which confers multidrug resistance (59). Thus, the accumulation and retention of MIBI are reduced in multidrug-resistant tumors, especially after chemotherapy. Prior studies have shown an inverse relationship between the levels of P-glycoprotein expression and the magnitude of MIBI uptake and washout in breast cancer cells (60,61). After chemotherapy, the percentage of breast cancers overexpressing P-glycoprotein increases dramatically (62). In the absence of immunohistologic information on P-glycoprotein expression in the tumor, it is impossible to tell whether a decrease in MIBI uptake is due to the effective chemotherapy or to chemotherapy-induced P-glycoprotein overexpression causing extrusion of MIBI out of tumor cells.
In a recent study, the factors influencing the response of LABC to presurgical chemotherapy were investigated using 18F-FDG PET and blood flow measured by 15O-water PET (63). The authors hypothesized that low tumor perfusion would predict poor response to systemic therapy; however, blood flow alone was not predictive of response. There was a strong association between pretherapy metabolism, reflected by the association of the metabolic rate of 18F-FDG, and the degree of response. Tumors with higher rates of glucose metabolism before therapy manifested a poor therapy response. Furthermore, a low ratio of 18F-FDG metabolic rate to blood flow was the best predictor of a better prognosis, as confirmed by survival analysis.
Metabolic Flare.
Increased tumor 18F-FDG uptake (i.e., metabolic flare) and the degree of estrogen receptor (ER) blockade early after institution of tamoxifen may predict response to antiestrogen therapy in patients with ER-positive metastatic breast cancer (64). Mortimer et al. reported that the functional status of tumor ERs can be characterized in vivo by PET with 18F-FDG and 16α-18F-fluoro-17β-estradiol (FES) (64). 18F-FDG PET was predictive of clinical response to tamoxifen therapy in patients with advanced ER-positive breast cancer. Forty women with biopsy-proved advanced ER-positive breast cancer underwent PET with 18F-FDG and FES before and 7–10 d after initiation of tamoxifen therapy. In the responders, the tumor 18F-FDG uptake increased after tamoxifen by 28.4%; only 5 of these patients had evidence of a clinical flare reaction. In nonresponders, tumor 18F-FDG uptake did not significantly change from baseline. Lesions of responders had higher baseline FES uptake than did those of nonresponders. All patients had evidence of blockade of the tumor ERs 7–10 d after initiation of tamoxifen therapy; however, the degree of ER blockade was greater in responders than in nonresponders.
False-Positives.
False-positive results occur in patients with inflammatory processes in the breast or early after biopsy or surgery. Benign breast tumors usually have low 18F-FDG uptake; only about 10% of fibroadenomas accumulate 18F-FDG (65).
False-Negatives.
False-negative results can occur when lesions are less than 1 cm or when the tumor is well differentiated, as is the case with tubular carcinoma and carcinoma in situ. A high rate of false-negative findings has also been reported for lobular carcinomas (66).
Summary.
18F-FDG PET appears to have a high prognostic value for determination of the effectiveness of therapy in LABC, although more data are necessary to confirm the existing findings in extended patient groups. After therapy, 18F-FDG PET reflects the overall biologic response to therapy but is limited in evaluating microscopic residual disease; however, early evidence of persistent disease may allow for more aggressive and novel therapy options. Thus, 18F-FDG PET should be the imaging modality of choice to monitor response to therapy in patients with LABC.
Non-Small Cell Lung Carcinoma
Lung cancer is the leading cause of cancer death in both men and women. Most developed countries have shown declines in death rates from cancer other than lung cancer. Approximately 13% of patients with lung cancer survive 5 y. This rate has been stable in the past 2 decades (48). The histologic classification of lung cancer by the World Health Organization defines 4 subtypes: squamous cell carcinoma, adenocarcinoma, large cell carcinoma, and small cell carcinoma. Small cell carcinoma accounts for 20%–25% of all lung cancers, and spread is often present at the time of diagnosis. The remainder of the lung cancer subtypes constitute the non-small cell lung cancer (NSCLC) group. In North America, adenocarcinoma of the lung is the most common histologic type of lung cancer, accounting for more than 40% of all cases of lung cancer. It appears that other than T1 N0 tumors, adenocarcinoma of the lung has a worse prognosis, stage for stage, than does squamous cell carcinoma (67).
Patients Who Will Benefit from Monitoring Response to Therapy.
Tumor shrinkage assessed by anatomic modalities is not a good indicator of response to treatment for detecting resistant clones present even in significantly shrunken masses. An accurate assessment of the impact of chemotherapy and radiotherapy would help guide treatment for patients with locally advanced lung cancer (stages IIIA and IIIB). Patients with locally advanced NSCLC who have bulky, inoperable disease will benefit most from an evaluation of the efficacy of chemotherapy. This group of patients composed 25%–40% of newly diagnosed lung cancer patients in the United States (48). In patients with locally advanced NSCLC, induction therapy followed by surgery may improve survival rates over those for surgery alone (68). In advanced-stage disease, at progression after platinum-based chemotherapy, second-line chemotherapy with docetaxel may have a survival benefit in selected patients (69). In stage IIIAN2 disease with no residual nodal disease after induction therapy and surgery, 5-y survival rates were 54%, compared with 17% in all patients treated with induction therapy regardless of the response status. Hence, it would be beneficial to offer surgery only to those patients with objective evidence of therapy response (68).
18F-FDG PET can also be useful in the assessment of the volumetric response to radiotherapy for locally advanced lung cancer. Chemotherapy-assisted novel hyperfractionated accelerated radiotherapy may be used in selected patients. Identification of nonresponders may allow physicians to limit more aggressive and toxic approaches to the subgroups of patients who would benefit from them.
Prediction of Response to Therapy After Its Completion.
The reported data on changes of 18F-FDG uptake between pretherapy and post-therapy 18F-FDG PET studies indicated a significant role for 18F-FDG PET in predicting response to therapy (Figs. 4 and 5). Patz et al. assessed the prognostic value of 18F-FDG PET in 113 patients with NSCLC who were treated with either chemotherapy, surgery, or radiotherapy (70). Patz et al. found a statistically significant difference in survival between patients with positive and patients with negative 18F-FDG PET findings. The median survival for patients with positive post-therapy 18F-FDG PET results was 12.1 mo, whereas 85% of those with negative results were alive at a median of 34.2 mo. Most early-stage patients had negative 18F-FDG PET results after therapy. Currently, there are no data for advocating adjuvant therapy in patients with stage I–II disease; however, a high-risk determination may justify further therapy in this setting. In this study, the authors did not designate a specific time after therapy for 18F-FDG PET to be performed, nor did they recruit a specific patient population in an effort to standardize the stage of disease and therapy modality. Nevertheless, this study may indicate that 18F-FDG PET is a predictor of survival independent of the time of study and the treatment modality.

A 46-y-old man with NSCLC of right upper lobe. Patient underwent 18F-FDG PET using dual-head gamma camera with attenuation correction (MCD-AC; ADAC Laboratories, Milpitas, CA) before and after completion of chemotherapy. Pretherapy 18F-FDG PET image (left) demonstrates distinct focus of increased 18F-FDG uptake in right upper lung. Post-therapy 18F-FDG PET image (right) reveals almost complete resolution of 18F-FDG uptake in corresponding region. Patient underwent resection of right upper lobe and was free of disease at 10-mo follow-up.
A 50-y-old woman with NSCLC of right upper lobe underwent 18F-FDG PET using dual-head gamma camera with attenuation correction (MCD-AC; ADAC Laboratories, Milpitas, CA) before and after completion of chemotherapy. Pretherapy 18F-FDG PET image (left) demonstrates distinct focus of increased 18F-FDG uptake in right upper lung. Post-therapy 18F-FDG PET image (right) reveals no interval change in extent of 18F-FDG uptake. Patient underwent resection of right upper lobe but, 8 mo after completion of therapy, presented with bone metastases detected on bone scan (not shown) obtained at another institution.
Bury et al. evaluated 18F-FDG PET in the detection of residual or recurrent disease in 126 patients with stage I–IIIB NSCLC treated with radiotherapy (71). 18F-FDG PET had a sensitivity and a negative predictive value of 100% and a specificity of 92%. In comparison, CT had a sensitivity of 72%, a negative predictive value of 79%, and a specificity of 95%. The authors concluded that 18F-FDG PET, with its high negative predictive value and sensitivity, is a useful adjunct to CT in monitoring the effects of radiotherapy. In a similar study, a negative postradiotherapy 18F-FDG PET finding associated with equivocal radiographic changes was a reliable indicator of a good prognosis (72). One notion has to be further clarified, however: A reduction in 18F-FDG uptake in the tumor should not be confused with complete resolution of 18F-FDG uptake after therapy. A decrease in tumor 18F-FDG uptake may reflect only partial response, whereas normalization of 18F-FDG uptake usually indicates a good prognosis (73). In accordance with this concept, Hebert et al. noted that the patients with completely negative 18F-FDG findings after therapy survived at least 2 y whereas 50% of patients with residual tumor hypermetabolism, regardless of the percentage of reduction, died within the same 2-y period (72). In a study by Frank et al., 5 patients with post-therapy residual tumor metabolism were further treated, although they were not clinically symptomatic. The results of that study were encouraging, with patients surviving beyond 3 y (74).
In a recent 18F-FDG PET study on 56 patients, Akhurst et al. retrospectively evaluated the value of 18F-FDG PET in detecting residual disease after therapy and the accuracy of restaging NSCLC after induction therapy (75). The data revealed that 18F-FDG PET had a positive predictive value of 98% for detecting residual disease after chemotherapy, radiotherapy, or chemoradiotherapy. 18F-FDG PET overstaged nodal status in 33% of patients with metastatic disease, understaged nodal status in 15%, and accurately staged nodal status in 52%. The authors concluded that although 18F-FDG PET accurately detected residual viable tumor after therapy, its potential to determine pretherapy nodal status is flawed. This study, however, had shortcomings stemming from the heterogeneous patient population that received different therapy modalities and from the various periods that had elapsed between completion of therapy and the 18F-FDG PET study. Hence, the authors could not correlate the changes in 18F-FDG tumor uptake between pre- and post-therapy 18F-FDG PET studies with pathologic response or survival. The results of this study serve as a foundation for prospective studies.
Early Prediction of Response to Therapy.
There is a paucity of 18F-FDG PET data on monitoring response to radiotherapy during the course of ongoing therapy. Prospective studies are necessary to address this vital issue, as identification of nonresponders as early as possible would significantly benefit the patients by allowing timely initiation of alternative therapies. Abe et al. investigated the value of pre- and post-therapy 18F-FDG PET changes in 5 patients in the prediction of radiotherapy response (76). All patients with negative 18F-FDG PET findings after completion of radiotherapy had a complete response, and those with residual 18F-FDG uptake showed a partial response accompanying tumor regrowth 2–3 mo after completion of therapy. In another preliminary study, the prognostic value of serial 18F-FDG PET studies was evaluated during the course of radiotherapy by coregistering pre- and post-therapy 18F-FDG PET images for 2 NSCLC patients (77). The authors investigated the changes in 18F-FDG uptake for 8 wk during radiotherapy and then after therapy. The data showed a progressive decrease in all response parameters for the patient who responded to treatment and an initial decrease followed by a sharp increase starting at the 45-Gy level for the nonresponder. Although further confirmatory studies are required, the authors concluded that ideal radiotherapy monitoring should include 3 18F-FDG PET studies during therapy. In addition to pre- and post-therapy 18F-FDG PET studies, they suggested that the third study be acquired at the 50-Gy dose level or 2 wk before the last dose fraction.
False-Positives.
Some benign pulmonary lesions have high metabolic rates resulting in false-positive results. These lesions include granulomas such as sarcoidosis, tuberculosis, histoplasmosis, aspergillosis, and coccidiomycosis as well as Mycobacterium avium intracellulare and other infectious processes such as pneumonia (78).
False-Negatives.
Tumors such as bronchioloalveolar carcinoma and carcinoid tumors, with low metabolic activity, can give rise to false-negative studies. Occasionally, well-differentiated adenocarcinomas have relatively less intense 18F-FDG accumulation, particularly in lesions smaller than 1.0 cm.
Other PET Tracers.
11C-Thymidine is a PET radiotracer used to evaluate tumor DNA synthesis and thereby proliferative activity, which is closely related to the effectiveness of cytotoxic therapy (79,80). In a comparative study, PET with 11C-thymidine and 18F-FDG was performed to measure tumor response to chemotherapy early after the initiation of treatment in a small group of patients with small cell lung cancer or soft-tissue sarcoma. In the patients with a clinical response to treatment, both 11C-thymidine and 18F-FDG uptake markedly declined 1 wk after therapy. In the 2 patients with progressive disease, 11C-thymidine uptake was essentially unchanged 1 wk after therapy, whereas 18F-FDG SUV increased significantly in 1 of these patients. In this preliminary study, the authors concluded that the assessment of tumor proliferation may reflect response to therapy better than 18F-FDG measurement. Because post-therapy benign tissue changes may cause modest levels of 18F-FDG uptake, this observation is relevant; however, comparative studies with a sufficient number of patients have to be performed to confirm this observation (81).
Summary.
18F-FDG PET after induction therapy accurately detects residual viable tumor. Persistent 18F-FDG uptake after therapy in a primary tumor or metastatic site is strongly predictive of residual viable disease. Early identification of nonresponders would significantly benefit patients with locally advanced NSCLC by allowing timely initiation of alternative therapies. Patients with therapy-resistant disease may greatly benefit from a change in therapeutic regimen.
Colorectal Carcinoma
Adenocarcinoma of the colon affects 5% of the population in the United States and in most western countries. If the disease is diagnosed in early stages, surgical treatment is curative and morbidity and mortality are minimal (82). Potentially curative resection at disease presentation can be performed on only 70%–80% of the patients, and overall survival at 5 y is less than 60%. Improvements in surgical and adjuvant therapies, more extensive screening programs, and recent advances in detection techniques, including imaging modalities, have reduced colon cancer mortality in the United States (83).
Patients Who Will Benefit from Monitoring Response to Therapy.
18F-FDG PET is most useful in monitoring advanced-stage colorectal cancer. Advanced disease is associated with a poor prognosis. Chemotherapy has demonstrated effective palliation, improvement of quality of life, and improvement of symptoms in such patients. Systemic chemotherapy doubles the survival of these patients, compared with untreated controls. For nearly 4 decades, 5-fluorouracil has been the mainstay of treatment (84). The use of 5-fluorouracil in combination with radiotherapy in primary unresectable colorectal cancer is also associated with improved survival. Chemotherapeutic options in the treatment of advanced colorectal cancer have markedly improved during the last few years, partly because of the high-dose 5-fluorouracil regimen but also because of the development of new cytotoxic agents and drug combinations. Today, most patients are treated by a sequential therapeutic concept that uses the newer drugs mainly for second- or third-line therapy. Combination of oxiliplatin with 5-fluorouracil can downstage previously unresectable liver metastases for potentially curative surgery in some patients (85). Oral fluoropyrimidines mark another progression in the treatment of advanced colorectal cancer.
18F-FDG PET offers great promise in the optimization of therapy, particularly as more targeted therapies become available. 18F-FDG PET enables a very early and more specific indication of response to preoperative therapies or of the presence of residual disease after surgical tumor resection or interventional tumor ablation of metastases or recurrences (86). 18F-FDG PET may play an important role in avoiding major surgery in patients for whom curative surgery is intended after chemotherapy or radiotherapy.
Prediction of Response to Therapy After Its Completion.
Guillem et al. assessed response to preoperative radiation and 5-fluorouracil-based chemotherapy in 15 patients (87). 18F-FDG PET was obtained before therapy and at 4–5 wk after completion of both radio- and chemotherapy. 18F-FDG PET parameters included SUVs, PET-derived tumor volume and visual response score, and change in total lesion glycolysis. All patients demonstrated a pathologic response to preoperative radiation and 5-fluorouracil-based chemotherapy. This response was confirmed in 100% of the cases by PET, compared with 78% by CT. In addition, the visual response score accurately estimated the extent of pathologic response in 60% of cases, compared with 22% of cases with CT. This pilot study demonstrated that 18F-FDG PET adds incremental information to the preoperative assessment of patients with rectal cancer. However, further studies on a larger series of patients are needed to verify these findings and to determine the value of 18F-FDG PET in a preoperative strategy aimed at identifying patients suitable for sphincter-preserving rectal cancer surgery.
The effect of radiotherapy was also evaluated by 18F-FDG PET approximately 6 wk after completion of radiotherapy in a group of patients with recurrent colorectal cancer (16). Post-treatment 18F-FDG PET studies revealed a statistically significant reduction in tumor uptake in only 50% of patients despite satisfactory palliative results. These results may be explained by inflammatory reactions caused by radiation injury immediately after radiotherapy. It is recommended that response to radiotherapy be evaluated at least 6 mo after completion of therapy in colorectal cancer to avoid false-positive results (16). In contrast, normal serum carcinoembryonic antigen levels were associated with increased 18F-FDG uptake in 14 of the 41 examinations, suggesting that PET is more sensitive than carcinoembryonic antigen measurement in patients with tumor recurrence.
Early Prediction of Response to Therapy.
There are 2 reports suggesting that 18F-FDG PET can predict response to chemotherapy in patients with hepatic metastases (5). Findlay et al. studied the metabolism of colorectal cancer liver metastases using 18F-FDG PET before and during the first month of 5-fluorouracil chemotherapy in 18 patients. The investigators obtained 18F-FDG PET studies before treatment, after 1–2 wk of treatment, and after 4–5 wk of treatment. Tumor response was associated with lower tumor-to-liver ratios at the 1- to 2-wk and 4- to 5-wk assessment as well as lower SUVs after 4–5 wk of therapy. Responding lesions had a greater reduction in metabolism (67% vs. 99%). The 4- to 5-wk tumor-to-liver ratio was able to discriminate response from nonresponse in both a lesion-by-lesion assessment and an overall patient response assessment with a sensitivity of 100% and specificities of 90% and 75%, respectively (5). A clear correlation was observed between reduction of tumor metabolism 5 wk after the initiation of systemic 5-fluorouracil treatment and therapy outcome. The 4- to 5-wk tumor-to-liver ratios and SUVs were able to discriminate responders from nonresponders in both a lesion-by-lesion assessment and an overall patient response assessment with sensitivities of 100% and 75%, respectively. There was no correlation, however, between the changes in tumor metabolism at 1–2 wk and therapy outcome. This study confirmed some limitations of 18F-FDG PET follow-up studies, such as the so-called flare phenomenon seen in breast cancer patients, observed as a marked increase in 18F-FDG metabolism in lesions responding after initiation of chemotherapy, and the importance of correct timing of 18F-FDG PET after therapy.
In patients with metastatic colorectal cancer treated with novel therapies such as radiofrequency ablation or a combination of cryotherapy and hepatic artery chemotherapy, 18F-FDG PET may be more accurate than CT when CT is equivocal in distinguishing post-therapy changes from recurrent or residual tumor. In a preliminary study, the predictive value of 18F-FDG PET was evaluated in a group of patients with liver metastases treated with a combination of cryotherapy and hepatic artery chemotherapy. 18F-FDG PET was superior to CT in differentiating post-therapy changes from active tumor (88).
False-Positives.
False-positive results can be obtained immediately after radiotherapy, as 18F-FDG uptake can occur in macrophages, neutrophils, fibroblasts, and granulation tissue (13). In vitro assays demonstrated that irradiated tumor cells may have a tenfold increased 18F-FDG uptake (14). Delaying 18F-FDG PET studies for 60 d after radiotherapy is recommended to accurately assess therapy response in colorectal cancer (16). The so-called flare phenomenon observed shortly after the initiation of chemotherapy may also lead to an increase in 18F-FDG metabolism in responding lesions (5).
False-Negatives.
False-negative 18F-FDG PET results may occur in lesions smaller than 1 cm, particularly in the liver (89). False-negative results in metastatic lymph nodes appear to stem from the lesser extent of the involvement (micrometastases) and the proximity of the involved lymph node to the primary site.
Other PET Tracers.
It is most helpful to assess individual drug concentrations at the target area before therapy begins. 5-Fluorouracil is the most important cytostatic agent for the therapy of metastatic colorectal cancer. 18F-5-Fluorouracil is biochemically identical to unlabeled 5-fluorouracil, and PET has been reported to be a useful tool to optimize and individualize chemotherapy for metastatic colorectal cancer. The trapping of 18F-5-fluorouracil can be highly variable even for multiple metastases in the same patient. Several studies reported that patients with high tumor 18F-5-fluorouracil SUVs (>2.5) are more likely to achieve at least stabilization of disease and survive longer than those with lower SUVs (90,91). Metastases with high 18F-5-fluorouracil uptake values (SUV of >3.0) correlated with negative values for tumor growth rate, whereas metastases with low uptake values (SUV of <2.0) demonstrated positive values for growth rates. Only metastases with a 18F-5-fluorouracil SUV exceeding 3.0 at 120 min after injection demonstrated a response to therapy (91). Hence, the outcome of 5-fluorouracil chemotherapy can be predicted using a single 18F-5-fluorouracil PET study before the initiation of therapy.
In another study, a pharmacokinetic model was developed to quantify the intracellular 5-fluorouracil concentration in liver metastases of colorectal adenocarcinoma, because this concentration is expected to correlate closely with therapy response. In addition, the influence of the biomodulator folinic acid on the action of 5-fluorouracil in the metastases was investigated (92). The authors found that with the quantitative modeling approach, trapping of 5-fluorouracil could be assessed noninvasively on an individual basis, but folinic acid showed no effect on the overall clinical response. This approach may make it possible to adjust the dose for each patient to optimize the treatment schedule. The most sensitive parameters for therapy monitoring were those that characterize the transport of 5-fluorouracil in (k[in]) and out (k[out]) of the intracellular volume of the metastases. Tumor response can be expected only if k[in] is higher than k[out], resulting in trapping of 5-fluorouracil within the tumor. Trapping was observed in 22% of metastases. The same parameters were also used to investigate the influence of the biomodulating agent folinic acid on drug effect. Five of the 6 metastases that showed trapping of 5-fluorouracil were observed in patients who received folinic acid. All patients but 1 who received folinic acid, however, had multiple metastases, of which only 1 was noted to trap 5-fluorouracil. Ideally, patient response can be expected only when all metastases trap 5-fluorouracil; thus, the authors concluded that folinic acid showed no effect on the overall clinical response (92).
Summary.
18F-FDG PET may induce a change in the therapeutic concept in patients with recurrent or advanced colorectal cancer for whom locoregional therapies are considered. If the published data are expanded on the prognostic value of 18F-FDG PET in predicting therapy response in colorectal cancer, 18F-FDG PET may be an integral part of treatment planning and outcome evaluation.
IMAGING OF GENE EXPRESSION WITH PET
PET technology lends itself to being optimal for studying molecular biology through the ability to analyze cellular biochemical processes quantitatively and repetitively. Imaging gene expression is of prime importance in evaluating the delivery of genes and vector products, quantifying gene expression, and monitoring the levels of transgene expression in vivo. Several imaging technologies have been investigated as tools to assess gene expression in vivo. Compared with optical and MRI-based approaches, PET, with its superior quantitative capability and sensitivity, performs favorably for imaging gene expression. A translated enzyme or a receptor can be probed with positron-emitting ligands specific for the expression product. Briefly, reporter gene-specific receptors bind positron-emitting ligand probes or enzymes that modify the positron-emitting substrate probes to produce sequestered products. Cells expressing the PET reporter gene will sequester the radiolabel of the PET reporter probe as a ligand bound to the PET reporter receptor or as a “trapped” product of the enzymatic reaction of the PET reporter enzyme. Ideally, those cells with no expression of the PET reporter genes do not accumulate the PET reporter probe. Imaging has been investigated for marker genes encoding intracellular enzymes and for marker genes encoding extracellular or cell-surface proteins and peptides. Expression of intracellular genes does not incite an immune response or, thus, allow for repeated studies. Extracellular genes have the disadvantage of inducing an immune response, which might pose limitations for repeated applications. Exogenous PET reporter genes, with the appropriate probe, have the advantage of producing signal in only the tissues in which they are expressed. An ideal reporter gene for longitudinal studies should therefore produce no immune response and not be normally expressed in the organism, or at least not in the organs under consideration (93–95). Strategies to image gene expression by PET include herpes simplex virus 1 thymidine kinase (HSV1-Tk), which was originally used as a marker to detect viral encephalitis; cytosine deaminase, which is expressed by some tumor cells; and other reporter systems, such as naturally occurring receptors (e.g., somatostatin receptors) or channels (e.g., iodine transporter channel) (94,95). The potential advantage of using HSV1-Tk as a marker gene is that the same gene can also be used to selectively kill targeted tumor cells using therapeutic prodrugs (96). Other prodrug activation strategies are also currently under development. Cytosine deaminase is capable of converting 5-fluorocytosine into lethal 5-fluorouracyl and has been used to monitor gene therapy by PET (97,98). 5-Flourouracil, however, is subject to significant efflux from the cell, rendering detectability and therapeutic efficiency unsatisfactory. Furthermore, uptake studies revealed only a moderate and nonsaturable tumor accumulation of radioactivity, suggesting that 5-flourouracil enters the cells only through diffusion and not by mediated cell internalization. Therefore, cytosine deaminase-based imaging lacks the advantage of HSV-Tk: intracellular retention of the converted radiolabel.
Currently, PET reporter gene or probe imaging allows for quantitative evaluation of gene expression in animals, in particular with micro-PET (93). In the future, the combination of more developed PET systems and molecular probe design will eventually allow investigators to evaluate gene expression in gene-therapy patients and follow the effectiveness of gene therapy in oncologic disorders.
CONCLUSION
18F-FDG PET is a highly sensitive and specific imaging modality in the evaluation of biochemical changes that occur in tumors during or after therapy. The convincing evidence that 18F-FDG PET can predict response early during the course of therapy opens up new possibilities for optimizing therapy planning and prognostic evaluation. The information derived from 18F-FDG PET images during treatment can now be used to change the management of individual patients and modify their therapy options. 18F-FDG PET evaluation after the first cycle may need to be incorporated into standard follow-up procedures.
Footnotes
Received May 3, 2002; revision accepted Sep. 25, 2002.
For correspondence or reprints contact: Lale Kostakoglu, MD, New York Presbyterian Hospital, Weill Medical College of Cornell University, 525 E. 68th St., Starr no. 221, New York, NY 10021.
E-mail: lak2005{at}mail.med.cornell.edu
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/education/ce_online.html) THROUGH FEBRUARY 2004.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 99mTc-Duramycin SPECT Imaging of Early Tumor Response to Targeted Therapy: A Comparison with 18F-FDG PET
- Effect of Platinum-Based Chemoradiotherapy on Cellular Proliferation in Bone Marrow and Spleen, Estimated by 18F-FLT PET/CT in Patients with Locally Advanced Non-Small Cell Lung Cancer
- Metabolic Tumor Volume of [18F]-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography Predicts Short-Term Outcome to Radiotherapy With or Without Chemotherapy in Pharyngeal Cancer
- 18F-FDG PET and PET/CT in the Evaluation of Cancer Treatment Response
- 18F-FDG PET/CT in Evaluating Non-CNS Pediatric Malignancies
- Early 18F-FDG PET for Prediction of Prognosis in Patients with Diffuse Large B-Cell Lymphoma: SUV-Based Assessment Versus Visual Analysis
- 18F-FDG Small-Animal PET for Monitoring the Therapeutic Effect of CT-Guided Radiofrequency Ablation on Implanted VX2 Lung Tumors in Rabbits
- Effects of Pegfilgrastim on Normal Biodistribution of 18F-FDG: Preclinical and Clinical Studies
- Use of PET for Monitoring Cancer Therapy and for Predicting Outcome
- [18F]Fluorodeoxyglucose Uptake by Positron Emission Tomography Predicts Outcome of Non-Small-Cell Lung Cancer
- Posttherapy [18F] Fluorodeoxyglucose Positron Emission Tomography in Carcinoma of the Cervix: Response and Outcome
- F-18 Fluorodeoxyglucose Positron Emission Tomography in the Evaluation of Distant Metastases From Renal Cell Carcinoma