


Abstract
The aim of this study was to evaluate the impact of whole-body 18F-FDG PET on staging and managing patients with small cell lung cancer (SCLC). Methods: The treatment records of 42 consecutive patients (27 men, 15 women; mean age, 62 y; age range, 45–83 y) with SCLC were reviewed. Whole-body 18F-FDG PET was performed for initial staging in 24 patients and for restaging after chemotherapy or radiation treatment in 20 patients. Two patients of the initial staging group were restaged with PET after therapy. PET findings were correlated with clinical and radiologic findings (CT of the chest and abdomen, bone scan, and CT or MRI of the brain). The impact of PET on staging and management decisions was determined. Results: For 12 of 42 patients (29%), PET results changed the patient’s management. In 8 patients (19%), PET resulted in a change of radiation therapy because of the detection of previously unknown tumor foci. Adjuvant radiation therapy was cancelled in 3 patients. A change of radiation field and volume was necessary in 5 patients. In 1 patient, PET results excluded extensive disease, which permitted surgical resection of the tumor. Chemotherapy was discontinued in 2 patients and restarted in 1 patient on the basis of the PET findings. In 5 patients (12%), PET excluded malignancy as the suspicious lesions found with conventional cross-sectional imaging did not take up 18F-FDG. Conclusion: The results of this study show that 18F-FDG PET has a major impact on the management of patients with SCLC, influencing both the stage and the management in 29% of patients. PET is a highly valuable tool for accurate target definition of radiation treatment by reducing the probability of overlooking involved areas.
Small cell lung cancer (SCLC) is the most aggressive type of lung cancer. At presentation, 30%–40% of patients with SCLC present with limited disease (LD) and 60%–70% present with extensive disease (ED) (1). LD is defined as disease confined to 1 hemithorax, mediastinum, and regional lymph nodes, which can be targeted with a single radiation portal field. Disease extension outside the thorax or the existence of malignant pleural effusion is considered ED (2,3).
Currently, most patients with LD SCLC are treated with a combination of chemotherapy and chest irradiation. This dual-modality therapy was shown to increase complete response rate and to decrease local therapy failure (4,5). In selected patients with very limited-stage disease (T1–T2, N0), surgical resection may be feasible (6,7). In extensive-stage SCLC, chemotherapy remains the main therapeutic approach (8). For patients who achieved complete response, prophylactic cranial irradiation is believed to improve the overall disease-free survival through reducing the risk of brain metastases (9).
Therefore, accurate pretreatment evaluation is a key prerequisite for choosing the appropriate therapeutic pathway in SCLC. The primary role of diagnostic imaging is to separate accurately LD from ED. On the basis of the widespread dissemination of SCLC, a battery of imaging tests is performed, such as CT of the chest and abdomen, CT or MRI of the brain, and a bone scan (10).
Although the conventional cross-sectional imaging modalities are sensitive to morphologic changes, identification of tumor tissue can be difficult in some settings (e.g., in normal-sized lymph nodes). Furthermore, morphologic imaging modalities are mostly used to evaluate a given region of the body rather than the entire body because of the enormous amount of data acquired. Metastases outside the imaging field are thus missed.
Radiation treatment planning based only on CT or MRI findings is likely to miss regions of macroscopic tumor in some patients and lead to the irradiation of unnecessarily large volumes in others (11,12). Incomplete irradiation may cause poor local control and a high rate of relapse (13). One imaging modality with the potential to distinguish accurately between benign and malignant lesions and to define the extent of disease is whole-body PET with 18F-FDG PET.
Recently, preliminary studies have shown that whole-body 18F-FDG PET is a useful tool for staging SCLC (14–16). Therefore, we were interested in determining whether staging with PET has an effect on referring physicians to change the pre-PET treatment intent. This study was designed to evaluate the impact of whole-body 18F-FDG PET on staging and managing patients with SCLC.
MATERIALS AND METHODS
Forty-five consecutive patients with SCLC referred for whole-body 18F-FDG PET at our institution between February 1999 and January 2003 were included in the study after signing an informed consent. Three patients were excluded from further analysis because of incomplete data. Thus, 42 patients with SCLC (27 men, 15 women; mean age, 62 y; age range, 45–83 y) remained in the study. The histologic verification of the tumors was available in all cases. SCLC coexisted with other malignancies in 4 patients: non-SCLC and neuroendocrine tumor in 2 patients, respectively.
Conventional staging by means of patient history, physical findings, blood tests, bronchoscopy, contrast-enhanced CT scan of the chest and upper abdomen, and bone scan was available in all patients. In 9 patients, CT or MRI of the brain was performed as a part of the staging work-up. All available clinical information, including results of surgical staging or histopathologic staging, was reviewed. Lymph nodes were regarded as positive for tumor on CT or MRI if they were >1 cm in size.
On the basis of all available information, and according to the TNM staging system (17), the clinical tumor stage in each patient was determined, and an initial treatment management plan was proposed. Pre-PET staging (staging using all information except PET) and post-PET staging (staging using all information including PET) were always performed independently.
In addition to conventional staging, PET scanning was performed for initial staging in 24 patients and for restaging after therapy in 20 patients. Two patients were scanned for initial staging as well as restaging. The PET scans were interpreted with all available clinical information, including CT scans. After obtaining the PET scan, each patient was assigned a post-PET tumor stage, which relied on the results of PET when there was discordance with other imaging studies. When possible, biopsies or further imaging studies were performed to resolve discrepancies between imaging modalities. It was considered unethical not to use clear but unconfirmed PET findings for further management decisions, especially in patients with previously unknown ED. An experienced radiation oncologist compared pre-PET and post-PET tumor stages, and the changes in radiation treatment decision were determined.
PET
To increase image quality and to suppress myocardial glucose utilization, patients were asked to fast for at least 4 h before undergoing the 18F-FDG PET examination. No patients had a history of diabetes mellitus. Patients received an intravenous injection of 300–400 MBq 18F-FDG and rested for 40–50 min for the organ uptake of 18F-FDG. 18F-FDG was produced in our own radiopharmaceutical laboratory using standard techniques. Before PET scanning, patients were encouraged to void to minimize activity in the bladder due to renal excretion of 18F-FDG. Then, patients were transferred to the table of the PET scanner.
At 50–60 min after injection of 18F-FDG, a static whole-body emission PET scan was started to cover the patient from the pelvic floor to the head. Throughout our study, all cerebral 18F-FDG examinations were done as part of the whole-body PET and not as dedicated 3-dimensional brain studies. Transmission scans were acquired in all patients. During our study, 2 different imaging techniques were applied. Until February 2001, 18F-FDG PET scanning was performed using an Advance NXi PET scanner (General Electric Medical Systems) with an axial field of view of 14.6 cm.
Emission scans were performed with a 4-min acquisition time at every table position, typically requiring 6 or 7 bed positions to cover the entire field of view. After emission scanning, a transmission scan was started using 68Ge pin sources rotating around the body. Transmission scans were performed from the head to the pelvic floor with a 2-min acquisition time at every table position. Image datasets were reconstructed iteratively with segmented attenuation correction. Twenty-six patient studies were acquired in this way.
Starting in March 2001, all imaging and data acquisition were performed with a combined PET/CT in-line device (DISCOVERY LS; General Electric Medical Systems), which consists of an Advance NXi PET scanner and a 4-slice LightSpeed Plus CT scanner that are integrated into this dedicated system. The axes of both systems are mechanically aligned so that simple translation of the patient table by approximately 60 cm between CT and PET data acquisitions moves the patient from the CT into the PET gantry.
The resulting PET and CT images are “hardware” coregistered to an accuracy in the range of 1 mm in all body areas without physiologic motion, if the patient does not move between both examinations. Data acquisition in the combined system was as follows. At 50–60 min after injection of 18F-FDG, a multidetector CT scan was performed from the head to the pelvic floor (scan length, 86.7 cm) with 140 kV, 80 mA, tube-rotation time of 0.5 s per evolution, pitch of 6, and a section thickness of 5 mm, which was matched to that of the PET section thickness. Immediately after CT scanning, a PET emission scan was obtained covering the identical axial field of view. Acquisition time was 4 min at each table position.
The PET and CT datasets were acquired on 2 independent computer consoles, which were connected by an interface to transfer CT data to the PET scanner. PET image datasets were reconstructed iteratively using CT data for attenuation correction (18), and coregistered images were displayed using eNTEGRA software (General Electric Medical Systems).
RESULTS
Impact on Management
For 12 of 42 patients (29%), PET findings changed the patients’ management. The treatment management was changed in 9 of 24 patients (37%) with PET for initial staging and in 3 of 20 patients (15%) with PET for restaging after therapy (Tables 1 and 2). In 3 patients, PET unmasked the existence of occult osseous and hepatic metastases; therefore, chemotherapy was started without adjuvant radiotherapy. The radiation field and radiation volume were changed in 5 patients due to additional PET findings (Fig. 1). In 1 patient, a curative surgical approach was taken because PET results excluded mediastinal involvement and distant metastases (Table 1, patient 1). Chemotherapy was reinstituted in 1 patient because PET demonstrated residual tumor tissue in the lung parenchyma (Fig. 2), whereas it was discontinued in 2 patients, who had enlarged residual mediastinal lymph nodes without increased 18F-FDG uptake (Table 2, patients 1 and 2).
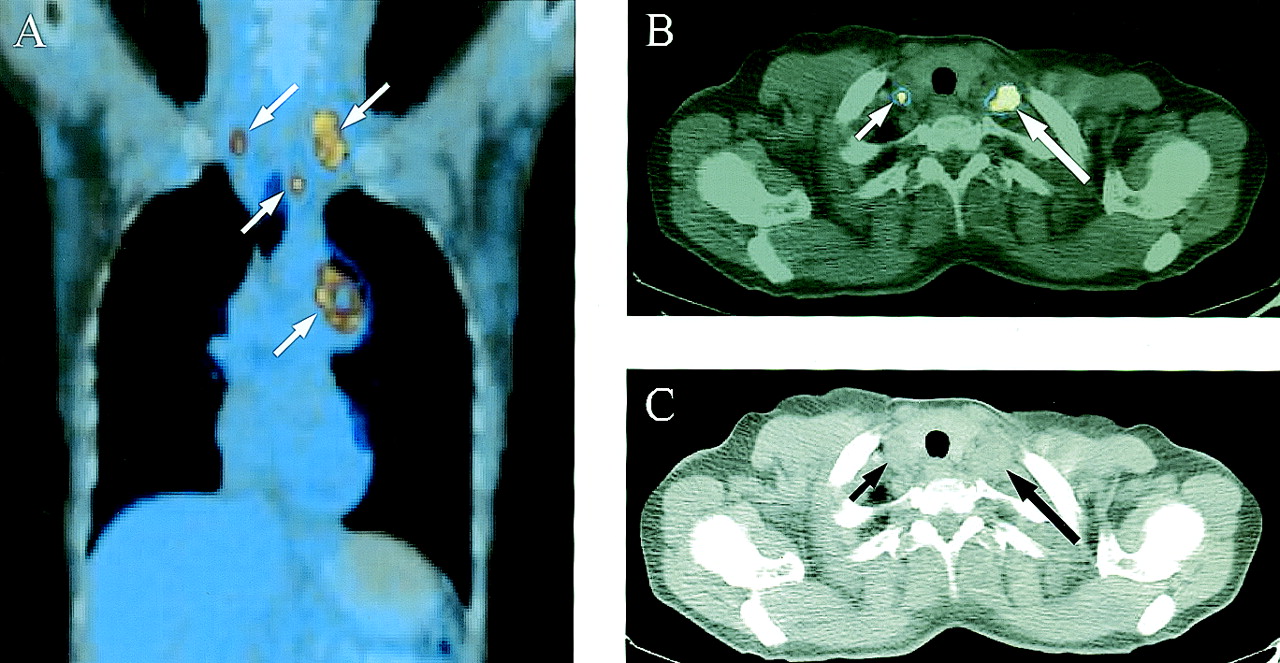
Coronal (A) and transaxial (B) PET/CT scans of chest and thoracic aperture in 47-y-old female patient show left central LD SCLC with ipsilateral paratracheal and bilateral supraclavicular lymph node metastases (white arrows). (C) Transaxial CT scan at level of thorax aperture shows pathologically enlarged ipsilateral (large black arrow) and normal-sized contralateral (small black arrow) supraclavicular lymph nodes.
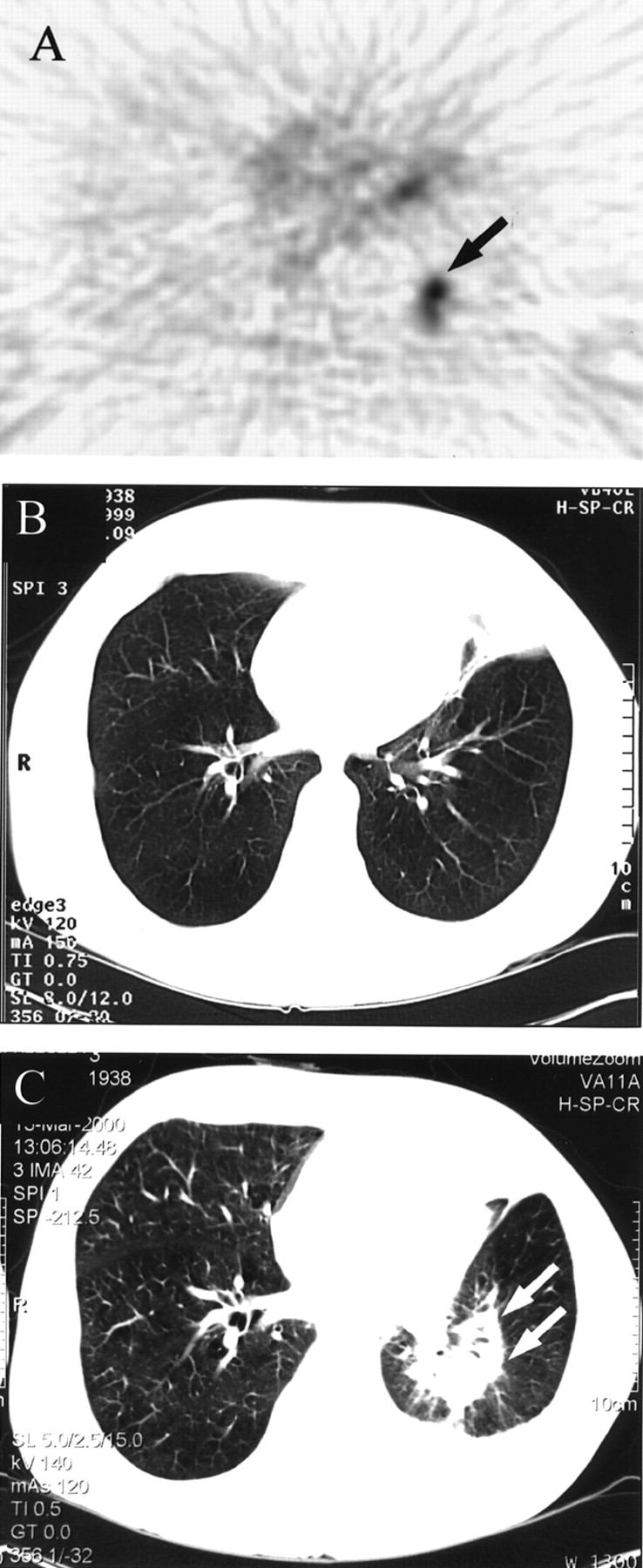
Transaxial thoracic 18F-FDG PET scan (A) in 64-y-old male patient shows pathologic 18F-FDG uptake at lower lobe of left lung consistent with residual disease after 5 chemotherapy cycles (black arrow) with no corresponding CT scan abnormality (B). Follow-up CT scan at 7 mo (C) shows local recurrence at lower lobe of left lung (white arrows).
Performance of 18F-FDG PET vs. Conventional Imaging Modalities Among Initial Staging Patient Group (n = 24)
Performance of 18F-FDG PET vs. Conventional Imaging Modalities Among Restaging Patient Group (n = 20)
Initial Staging
According to the final staging decision, 15 patients were classified as LD and 9 patients were classified as ED (Table 1). In comparison with the other staging methods, PET upstaged 3 patients from LD to ED due to the presence of occult osseous (n = 2) and hepatic (n = 1) metastases. PET results downstaged 1 patient from ED to LD after excluding a contralateral lung metastasis that was described by conventional staging.
In 20 patients, the final staging classification by PET and conventional imaging modalities was similar. However, in 9 patients, incongruence between functional and anatomic imaging was observed (Table 1). Findings mismatch that did not change the final staging decision of these 9 cases were distributed as follows. In 5 patients with LD, PET detected additional metastatic foci: ipsilateral pulmonary metastasis (n = 1) and contralateral mediastinal (n = 1), contralateral supraclavicular (n = 2), and contralateral cervical (n = 1) lymph node metastases. Being limited-stage disease, the patients were all treated with combined radiochemotherapy. However, according to the additional PET findings, essential radiotherapy field (n = 3) and volume (n = 2) modifications were performed.
In another 4 patients with ED, PET identified unknown visceral and soft-tissue metastases in 1 patient and ruled out tumor extension into bilaterally enlarged adrenal glands in another patient as confirmed by clinical and radiologic follow-up. In 2 patients, PET missed brain metastases. In these 4 patients, PET results did not change the therapeutic decision, which consisted of chemotherapy alone.
Restaging
For restaging after therapy, 18F-FDG PET was available in 20 patients. According to the definitive restaging categorization, PET correctly identified the 5 patients with total remission, 11 of 12 patients with residual disease (Fig. 3), and the 3 patients with progressive disease. Complete response was verified by clinical (n = 2) and radiologic (n = 3) follow-up (range, 6–26 mo; mean, 13 mo; median, 6 mo). In 6 of these 20 patients (30%), discordant results were found between PET and the other imaging methods. Findings mismatch in these 6 patients (Table 2) was distributed as follows. In 3 patients, no abnormal 18F-FDG accumulation could be detected despite the persistence of mediastinal lymph node enlargement after induction chemotherapy. On the basis of the negative PET findings, further chemotherapy was considered unnecessary.

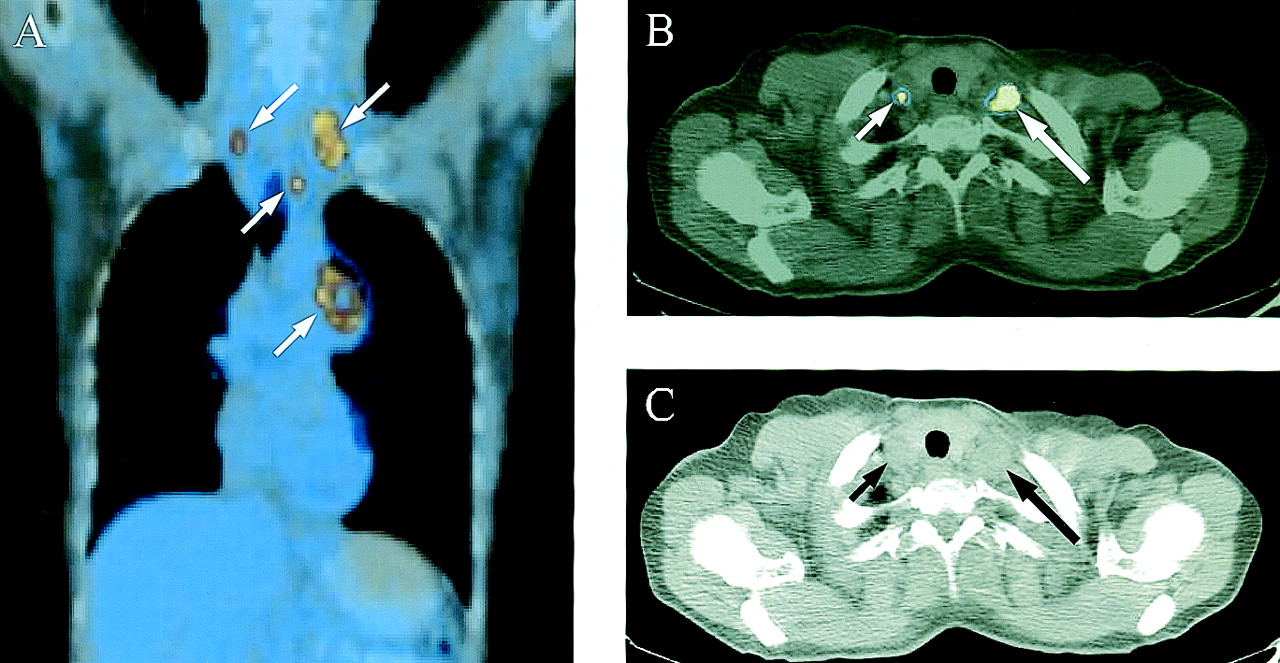
Transaxial thoracic slices obtained by 18F-FDG PET (A), CT (B), and PET/CT (C) image fusion in 59-y-old female patient show residual disease after induction chemotherapy (arrows).
In 2 of these 3 patients, true-negative PET results were confirmed by clinical and radiologic follow-up (Table 2, patients 1 and 2); however, 4 wk after the PET examination, the third one (Table 2, patient 6) developed hemoptysis that necessitated a mediastinal radiotherapy dose to control bronchial erosion by an active disease-harboring subcarinal lymph node. In this patient, the PET finding was classified as false-negative because follow-up CT confirmed an increase in size of this lesion, which was attributed to tumor progression.
In the remaining 3 patients, chemotherapy was continued in 1 of them because PET demonstrated residual tumor tissue in the lung parenchyma that was missed by CT (Fig. 2). In another patient, PET excluded a falsely suggested sclerotic metastasis by both CT and bone scanning in the sternum. Fine-needle biopsy confirmed the PET finding. In 1 patient with residual disease, PET scanning identified additional unknown soft-tissue metastases in the breast and axilla as confirmed by histopathology (Table 2, patient 9).
Detection of Brain Metastases
In 9 patients, CT or MRI of the brain was performed around the time of PET scanning (±2 wk) to exclude brain metastases. These cerebral PET examinations were done as part of the whole-body 2-dimensional PET. No brain metastases were found in 5 patients. PET identified 1 patient with cerebellar metastases as suggested by CT. PET missed multiple cerebral metastases in 2 patients as verified by CT and MRI, but the false-negative findings did not affect the final patient classification, which remained ED (Table 1, patients 21 and 22). In 1 patient, MRI revealed an intrasellar mass, which was proven to be a functioning prolactinoma on the basis of the laboratory findings. In PET, this tumor presented as a photopenic focus that lacked 18F-FDG uptake.
DISCUSSION
Whole-body 18F-FDG PET has been proven to be a very effective imaging modality for initial staging and restaging of many malignant tumors (19). Preliminary studies have shown that 18F-FDG PET is a reliable imaging technique for staging and restaging patients with SCLC (14–16). The high sensitivity of 18F-FDG PET may impose a strong impact on patient management through unmasking the existence of occult metastatic foci (20). In a recent prospective study, Chin et al. suggested that whole-body 18F-FDG PET may be able to replace the combination of conventional imaging modalities for staging SCLC in a cost-effective manner even if CT or MRI is included to rule out brain metastases (21). In another study involving 25 patients with SCLC, Shen et al. reported that 18F-FDG PET may allow fast identification of patients with ED and, thus, spare additional radiologic or invasive diagnostic procedures (22).
In this study, we analyzed the impact of PET on the management of patients with SCLC. Our results show that PET altered the overall management in 12 of 42 patients (29%). For initial staging and restaging, PET imaging changed the management in 9 of 24 patients (37%) and 3 of 20 (15%) patients, respectively. PET was superior to conventional staging, particularly in the detection of mediastinal lymph node metastases and of occult distant metastases. Furthermore, PET results excluded malignancy in 12% of the patients in which suspicious lesions were found with morphologic cross-sectional imaging. This finding is not surprising, owing to the high proliferation potential of SCLC, which is directly translated to avid 18F-FDG uptake by virtue of upregulating the glucose transporter microsystem to fulfill the increasing demand for energy production by this aggressive tumor (23).
Because combined radiochemotherapy is usually reserved for patients with limited-stage disease, the main goal of diagnostic imaging in SCLC is to separate accurately LD from ED. Accurate staging of SCLC can provide a better selection of candidates with unambiguous LD for the appropriate local treatment (24). However, local therapy failure in patients with limited-stage SCLC is a well-recognized limitation (13). Therefore, accurate planning of the radiation fields has been claimed to improve the overall treatment response (13,25).
Munley et al. reported that PET scans influenced the radiation treatment plans in 12 of 35 patients (34%) with lung cancer (26). In our study, PET scans had an impact on radiation treatment in 8 patients (19%). In 5 patients (12%), PET scans resulted in a change of radiation field and volume after identifying additional active tumor foci, which were not identified by the conventional staging methods (Fig. 1). In 3 patients (7%), adjuvant radiotherapy was not started because of the additional detection of osseous and hepatic metastases.
Because commercial PET scanners provide a nominal spatial resolution of 4.5–6 mm in the center of the axial field of view, even small (<1 cm) 18F-FDG–accumulating lesions can be detected (20). This represents a critical advantage of PET over CT and MRI in identifying tumor spread to normal-sized lymph nodes. Our data suggest that PET imaging has the potential to improve the results of combined chemoradiotherapy by preventing futile treatment of patients with unknown distant metastases or advanced locoregional disease and by optimizing the radiation treatment for patients with limited-stage disease.
It has been shown that, in selected patients with SCLC, surgery might be of value with a curative intent (6,7). In our series, 1 patient was downstaged to LD after excluding a contralateral pulmonary metastasis, which was suggested on CT. This patient with very early LD SCLC (pT2 pN0) was sent to surgery for a curative resection.
Because of the high physiologic accumulation of 18F-FDG in the brain, PET scans were not sensitive enough for the detection of brain metastases. For accurate screening of brain metastases, gadolinium-enhanced MRI should be used (27,28). In our study, PET did not detect brain metastases in 2 of 3 patients. This finding suggests that, in patients who are found to have LD with PET, if brain metastases need to be excluded, an MR scan of the brain is necessary.
The metabolic characters of lesion detection by 18F-FDG PET can be used for early monitoring of therapy response to separate partial responders from nonresponders (29). This can offer nonresponders the opportunity for alternative therapies and, thereby, spare them unnecessary toxicity burden. Furthermore, confirming complete remission—besides being the main goal of any multimodality treatment—in SCLC it may also permit prophylactic cranial irradiation to be performed. This can offer complete responders a significant improvement in both overall and disease-free survival through reducing the potential occurrence of brain metastases (9).
Our results show that 18F-FDG PET is an accurate method for restaging after therapy. PET correctly identified all patients with total remission (n = 5), 11 of 12 patients with residual disease, and all patients with progressive disease (n = 3). Among the restaging group, PET had an impact on the management of 3 patients (Table 2).
On the basis of the true-negative PET findings, further chemotherapy was deemed unnecessary in 2 patients despite the presence of enlarged mediastinal lymph nodes. On the other hand, chemotherapy was reinstituted in 1 patient because of the presence of a metabolically active tumor residue that was missed by CT (Fig. 2). This is in accordance with the known better performance of 18F-FDG PET in differentiating posttherapeutic scarring from residual active tumor tissue (30). However, missing microscopic disease is a limitation of 18F-FDG PET as it is in morphologic imaging (31,32).
In 1 patient, 18F-FDG PET did not identify the existence of residual disease in a pathologically enlarged subcarinal lymph node 5 wk after the last chemotherapy cycle. Whether systemic therapy has eradicated or metabolically stunned the 18F-FDG–avid tumor cells in this lymph node is a matter of discussion (31). Nonetheless, it should be recognized that a sequencing radiotherapy might be of benefit when conventional restaging of a known aggressive tumor reveals postchemotherapy residual disease that lacks 18F-FDG uptake.
Despite induction chemotherapy, disease progression was observed in 3 patients of our series. Identifying patients with progressive disease is of clinical importance, because these patients do not respond to a second-line chemotherapy in most instances and are usually subject to palliative care (8). Recently, Pandit el al. reported that the prognosis of SCLC is strongly correlated with 18F-FDG PET findings after therapy (33).
It is generally accepted that 18F-FDG is not a tumor-specific molecule because it accumulates in infectious and inflammatory lesions as well (34). However, in our study, no false-positive lesions were reported. In this study, only some of the lesions detected by PET or conventional imaging were confirmed histopathologically. In patients with systemic disease, as in SCLC, where surgical therapy is generally not indicated, the ability of surgical staging or histopathologic confirmation is limited for obvious ethical reasons.
Because of the biologic behavior, natural history, and prognosis of SCLC, most PET results were accepted to be true-positive findings in this study. We believe that our results are valid, although more clinical and outcome data must be accumulated to definitively establish the value of 18F-FDG PET in SCLC.
CONCLUSION
Our results indicate that whole-body 18F-FDG PET has a considerable impact on the management of patients with SCLC. This study showed that 18F-FDG PET affected staging and management in 29% of patients with SCLC. Future studies should concentrate on the final clinical outcome of patients who were staged and treated on the basis of 18F-FDG PET findings.
Acknowledgments
The authors gratefully acknowledge Thomas Berthold, Michael Belohlavy, Conny Britt, and Michelle Farrell for technical help. This research was supported in part by the Federal Commission for Scholarships, Bern, Switzerland. Part of this work was presented at the 4th Annual Meeting of the Swiss Society of Nuclear Medicine in Lucerne, Switzerland, June 25–28, 2003, and at the 16th Annual Congress of the European Association of Nuclear Medicine in Amsterdam, The Netherlands, August 22–27, 2003.
Footnotes
Received Apr. 3, 2003; revision accepted Aug. 14, 2003.
For correspondence or reprints contact: Hans C. Steinert, MD, Division of Nuclear Medicine, University Hospital Zurich, Raemistrasse 100, 8091 Zurich, Switzerland.
E-mail: hans.steinert{at}dmr.usz.ch
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Modern Staging of Small Cell Lung Cancer
- Small Cell Lung Cancer
- Small Cell Lung Cancer
- Guidelines on the radical management of patients with lung cancer
- NCCN Task Force: Clinical Utility of PET in a Variety of Tumor Types
- Evaluation of Dual-Time-Point 18F-FDG PET for Staging in Patients with Lung Cancer
- Partnerships in Oncology and Radiology: The Role of Radiology in the Detection, Staging, and Follow-up of Lung Cancer
- PET Evaluation of Lung Cancer
- Significance of Incidental 18F-FDG Accumulations in the Gastrointestinal Tract in PET/CT: Correlation with Endoscopic and Histopathologic Results
- Positron Emission Tomography in Limited-Stage Small-Cell Lung Cancer: A Prospective Study
- Why Most PET of Lung and Head-and-Neck Cancer Will Be PET/CT