


Abstract
The procedure of sentinel lymph node biopsy in patients with malignant cutaneous melanoma has evolved from the notion that the tumor drains in a logical way through the lymphatic system, from the first to subsequent levels. As a consequence, the first lymph node encountered (the sentinel node) will most likely be the first affected by metastasis; therefore, a negative sentinel node makes it highly unlikely that other nodes in the same lymphatic basin are affected. Although the long-term therapeutic benefit of the sentinel lymph node biopsy per se has not yet been ascertained, this procedure distinguishes patients without nodal metastases, who can avoid nodal basin dissection with its associated risk of lymphedema, from those with metastatic involvement, who may benefit from additional therapy. Sentinel lymph node biopsy would represent a significant advantage as a minimally invasive procedure, considering that an average of only 20% of melanoma patients with a Breslow thickness between 1.5 and 4 mm harbor metastasis in their sentinel node and are therefore candidates for elective lymph node dissection. Furthermore, histologic sampling errors (amounting to approximately 12% of lymph nodes in the conventional routine) can be reduced if one assesses a single (sentinel) node extensively rather than assessing the standard few histologic sections in a high number of lymph nodes per patient. The cells from which cutaneous melanomas originate are located between the dermis and the epidermis, a zone that drains to the inner lymphatic network in the reticular dermis and, in turn, to larger collecting lymphatics in the subcutis. Therefore, the optimal route for interstitial administration of radiocolloids for lymphoscintigraphy and subsequent radioguided sentinel lymph node biopsy is intradermal or subdermal injection. 99mTc-Labeled colloids in various size ranges are equally adequate for radioguided sentinel lymph node biopsy in patients with cutaneous melanoma, depending on local experience and availability. For melanomas along the midline of the head, neck, and trunk, particular consideration should be given to ambiguous lymphatic drainage, which frequently requires interstitial administration virtually all around the tumor or surgical scar from prior excision of the melanoma. Lymphoscintigraphy is an essential part of radioguided sentinel lymph node biopsy because images are used to direct the surgeon to the sites of the nodes. The sentinel lymph node should have a significantly higher count than that of the background (at least 10:1 intraoperatively). After removal of the sentinel node, the surgical bed must be reexamined to ensure that all radioactive sites are identified and removed for analysis. Virtually the entire sentinel lymph node should be processed for histopathology, including both conventional hematoxylin–eosin staining and immune staining with antibodies to the S-100 and HMB-45 antigens. The success rate of radioguidance in localizing the sentinel lymph node in melanoma patients is approximately 98% in institutions that perform a high number of procedures and approaches 99% when combined with the vital blue-dye technique. Growing evidence of the high correlation between a sentinel lymph node biopsy negative for cancer and a negative status for the lymphatic basin—evidence, therefore, of the high prognostic value of sentinel node biopsy—has led to the procedure’s being included in the most recent version of the TNM staging system and starting to become the standard of care for patients with cutaneous melanoma.
- sentinel lymph node
- malignant cutaneous melanoma
- radiocolloid
- interstitial administration
- lymphoscintigraphy
- intraoperative γ-probe guidance
The incidence of malignant cutaneous melanoma has increased 3-fold since the early 1970s (1), and melanoma is now the sixth most common cancer in the United States (2). The National Cancer Institute Surveillance, Epidemiology and End Results Survey found that, in 1993, approximately 54,300 new cases of melanoma were diagnosed and 9,400 patients died of melanoma (3). If present trends continue, the lifetime incidence of cutaneous malignant melanoma may reach 1 in 75 persons by 2005. Major risk factors for melanoma include increased age, a large number of moles, a family history of melanoma, immunosuppression, and sun sensitivity (4). Death is more likely when the disease is diagnosed at an advanced stage; in fact, the 5-y mortality averages approximately 20% in stages I–II cumulatively but is higher in stage III (35%) and stage IV (90%) (3).
Melanoma can be cured by surgery alone when the disease is localized, but advanced disease is almost invariably fatal, even after aggressive antitumor combination therapy. The main prognostic factors for primary melanoma of the skin are the thickness of the lesion (in millimeters), the presence of ulceration (absence of intact epidermis overlying the melanoma, assessed histologically) (5), and metastatic involvement of the sentinel lymph node (6). Among these, the number of metastatic lymph nodes and whether they are microscopically or macroscopically involved is by far the most important prognostic factor (7–11). The rationale for histopathologic evaluation of the first lymph node draining the tumor, the sentinel lymph node, stems from the predictable lymphatic spread of melanoma (12). Lymphoscintigraphy provides the road map to identify the nodes to interrogate (13,14).
Although the importance of regional lymph nodes in the dissemination of cutaneous melanoma was recognized at the beginning of the 20th century (15,16), use of radiolabeled colloids injected interstitially (17–20) to identify these nodes did not begin until approximately 10 y ago. This application of radiocolloids is an extension of the observations of Cabanas (21), who applied the technique to patients with penile cancer, and of Bennett and Lago (22), who used the technique to locate the major nodal basins draining cutaneous melanomas.
Metastatic spread of cancer through the lymphatic system occurs as a sequence of events (23) starting with penetration of neoplastic cells through the basal lamina into the connective tissue spaces. Neoplastic cells then approach and penetrate the lymphatic endothelial barrier, are carried by lymph flow to the lymph node, proliferate in the sinusoids of the node but are mostly confined to the subcapsular space, and destroy the lymph node through further proliferation, occasionally followed by penetration into surrounding tissue. Finally, seeding of secondary nodes occurs.
Neoplastic cells leaving the metastatic first-tier lymph node can follow lymph flow up the lymphatic chain, even at a relatively early stage of tumor growth. At any stage, tumor cells can enter the bloodstream by penetrating venous capillaries in the tumor bed, following lymph flow through the thoracic duct, or traversing lymphovenous anastomoses in the metastatic lymph node. The common embryologic origin of the lymphatic and venous systems inextricably links neoplastic spread through these conduits. In fact, cancer cells can invade the lymphatics or the blood vessels directly, readily passing from blood to lymphatic channels and back again through venolymphatic communications through the interstitial space of lymph nodes or of other tissues (24,25).
When viewed using lymphoscintigraphy and radioguided surgery, a sentinel lymph node is not necessarily the node with the highest level of radioactivity. If only the hottest node were considered, approximately 13% of nodal metastases would be missed, especially if the lesion involves the cervical nodes. These metastases would be identified if all radioactive nodes were harvested for immunohistochemical evaluation (26). The very high positive and negative predictive value of sentinel node biopsy has led to wide acceptance of the procedure as an integral part of tumor staging. This acceptance was summarized by Ell (27): “Sentinel lymph node biopsy is calling into question the practice of wide lymph node basin dissections for staging cancer, and challenging not only the established concepts of dissemination of cancer via lymphatics but also the present standards of histopathological examination of lymph nodes, the functional significance of micrometastases and the conventional wisdom and practice of cancer staging.”
Sentinel lymph node evaluation distinguishes patients without nodal metastases, who can avoid nodal basin dissection and its associated risk of lymphedema, from those with metastatic involvement, who might benefit from additional therapy such as complete lymphadenectomy and adjuvant therapy (28). Patients with negative results from sentinel lymph node biopsy also benefit psychologically (29). The possible therapeutic benefit of the sentinel lymph node biopsy procedure per se and of sentinel node–based therapeutic decisions is currently under investigation in several prospective clinical trials (especially the so-called Sunbelt Melanoma Trial) (30).
CLINICAL PROBLEM
Patients with early-stage malignant cutaneous melanomas < 1 mm thick have an excellent prognosis, with a 10-y survival > 90% and a recurrence rate < 5% (31,32). Conversely, only 40% of patients with a melanoma thicker than 1.5 mm survive 5 y after primary treatment (dropping to 10% if distant metastases are present at the time of initial diagnosis). Patients with cutaneous melanomas thicker than 4 mm have an ominous prognosis, with a high risk of both locoregional lymph node recurrence (in more than one third of the patients) (33) and systemic disease in more than three fourths of the patients (68% overall 10-y survival) (34).
The level of invasion is a strong prognostic factor only for thin melanomas. In patients with melanomas thicker than 4 mm, the clinical benefit of prophylactic lymph node dissection is questionable, even though the 5-y survival rate for patients with stage III cutaneous melanoma with 1 positive node is 40% (decreasing to 24% with involvement of 4 nodes). Lymphatic metastasis lowers the survival rate of these patients by approximately half. It has also been reported that the prognostic impact of Breslow thickness is less important when adjusted for status of regional lymph nodes (35).
Patients with intermediate-thickness cutaneous melanoma (between 1 and 4 mm) constitute the population most likely to benefit from elective lymph node dissection when biopsy of the sentinel lymph node shows metastatic involvement. In fact, this surgical treatment ensures significant therapeutic benefit and increased survival (36), especially in patients with micrometastases only (37,38).
The incidence of sentinel lymph node metastasis is approximately 5% for melanomas between 0.76 and 1.5 mm thick but increases to almost 20% for melanomas between 1.5 and 4 mm thick (33). Several other reports describe the incidence of sentinel lymph node involvement as 12%–36%, with an average value of approximately 20% (12,17,39–41).
Drainage of the tumor is usually predictable when the lesion is located in the extremities. Lower-extremity melanomas drain toward the homolateral groin, and upper-extremity lesions drain toward the homolateral axilla; if the melanoma is located in the hand/forearm or in the foot/leg, intercalated lymph nodes in epitrochlear or popliteal regions, respectively, can be imaged at lymphoscintigraphy. The pattern of lymphatic drainage from lesions of the head, neck, and trunk is much less predictable (14,22,42–46).
Sentinel lymph node biopsy with detailed histologic evaluation of the node is necessary to define metastatic involvement, because noninvasive methods, including CT (47–49), cannot provide this information. An alternative staging modality is to consider lymph node dissection of the draining basin in all patients. This approach is not advisable, however, because metastases will be found in a minority of patients (approximately 20%), and all patients will be at risk of the immediate and long-term complications of surgery, including chronic lymphedema and nerve injury. Absence of tumor in the sentinel lymph node has a very high negative predictive value, because skip metastases (involvement of second- or third-tier lymph nodes with sparing of the sentinel node) have been reported as very low (<2% of the patients) in melanoma (17,50–52). This factor strongly supports the concept of orderly progression of lymph node metastases (12) and therefore validates the clinical role of sentinel lymph node biopsy, especially in patients with melanoma (53). On the other hand, prior sentinel lymph node biopsy does not compromise regional nodal basin control (54) and is associated with a very low incidence (<2%) of late lymphedema (55).
LYMPHATICS IN RELATION TO MELANOMA
As reviewed earlier (56), the lymphatic vessels follow a distribution that tends to accompany the routes of blood supply because of a common embryologic origin with the venous structures that creates the potential for lymphovenous anastomoses under certain conditions of lymph flow and pressure (57,58). The review (56) provides details on the embryologic origin of the lymphatic system and on lymphatic neoangiogenesis in tumors and in the peritumoral space, with special reference to the main topic of this article, radioguided biopsy of the sentinel lymph node.
The epidermis, consisting of epithelial cells arranged from the basal to the keratinocyte layer, is virtually devoid of lymphatic structures. In contrast, the dermis has abundant lymph vessels. Dermal lymph vessels are subdivided into 2 networks, a superficial papillary and subpapillary fine-meshed network and a deeper network filling the reticular dermis. Under physiologic conditions of flow and pressure, lymph flows from the superficial to the deeper network. The inner network in turn drains lymph into somewhat larger vessels that take a curving course to penetrate into the subcutis, where they merge into larger collecting lymphatics (Fig. 1A). This subcutaneous plexus and the deep fascial plexus communicate efficiently along fibrous strands spaced approximately 1 mm apart. The density of communicating lymphatic vessels, as well as of the overall lymphatic system, varies in different regions of the body. Lymphatic vessels are rarely detectable in a region up to 50 μm below the epidermis. The next 3 layers, up to 200 μm, exhibit the highest density of lymphatic vessels in the dermis. The uppermost quarter of the dermis depthwise contains 42%–64% of all lymphatic vessels observed in the skin (59).

(A) Low-magnification view of histologic section (hematoxylin–eosin staining) extending from epidermis to underlying muscle (modified from Ackerman (157)). Locations of papillary–subpapillary plexus, dermal lymphatics, subcutaneous lymphatics, communicating lymphatics along fibrous strands, and deep epifascial lymphatics are indicated. (B) Schematic representation of regions with ambiguous lymphatic drainage around midline of body as derived from classic anatomic notions (Sappey’s concept, dark gray) and from lymphoscintigraphic, functional studies (light gray). In Sappey’s notion, ambiguous lymphatic drainage (i.e., possibility of draining toward either left- or right-sided lymph nodes) corresponds to restricted area extending only approximately 5 cm on each side of midline of body. More recent lymphoscintigraphic studies show instead that ambiguous lymphatic drainage can extend to much wider area: Head, neck, and shoulders are virtually entirely included in this area, as is relevant abdominal area around waist.
The density of lymphatic vessels does not always mirror the rate of lymph flow or the capacity of lymphatic drainage. The highest values of lymph flow are observed in the distal regions of the limbs. This may be a physiologic mechanism ensuring good return of fluid and protein leaked by the blood capillaries back to the systemic circulation, along with metabolic waste products and cell debris. Conversely, the lowest lymph flow values are observed in the head and neck, with intermediate values being found in the upper arms and shoulders (60,61).
There are some remarkable regional differences in lymphatic density (59). The highest overall lymphatic vessel density is observed in the skin of the head and neck, whereas the lowest is in the extremities. Intermediate levels are observed in the trunk, with the exception of the chest, where lymphatic vessel density is somewhat lower. These regional differences may account for the poorer prognosis of cutaneous melanoma originating in the head, where the density of lymphatic vessels is highest, compared with lesions arising elsewhere in the body.
Factors that influence the amount of lymph flow include, at least, the volume of lymph produced per unit time (which can be higher in the distal limbs because of gravitational effects on hydrostatic pressure within the blood capillaries), mechanical pump effects caused by skeletal muscle contractions, intrinsic rhythmic pulsation of the lymph vessels, and temperature.
Not only does lymph travel faster from the periphery than from central regions, but the lymph nodes themselves appear to be more “porous” to radiocolloids when the lymph channels originate in the leg, foot, thigh, hand, or forearm. This effect is shown by more frequent lymphoscintigraphic visualization of second-tier lymph nodes after ready passage of the tracer through the sentinel lymph node in these regions of the body (62).
Lymphatic mapping with radiocolloids has revealed unsuspected routes of lymphatic drainage that contradict Sappey’s anatomic drawings. The main advantage of lymphoscintigraphy over classic anatomic notions is that the lymphoscintigraphic pattern reflects the functional status of lymphatic drainage specifically in each patient and is more accurate than the typical distribution defined by the average anatomic appearance in a series of patients. Primary melanomas located in the trunk show a pattern of ambiguous drainage that is greatly expanded in comparison with the classic Sappey’s watershed areas (14,43,61) (Fig. 1B).
These considerations explain why lymphoscintigraphy must be considered an essential part of radioguided sentinel lymph node biopsy. In fact, the imaging phase performed on interstitial injection of the radiocolloid tracer should provide 3 pieces of information. The first is the identification of all lymph node basins at risk for metastatic disease, including those in unexpected locations (14,46,63). If the primary site is a watershed area of lymphatic drainage to more than one nodal basin (64), preoperative lymphoscintigraphy provides the surgeon with a map of lymphatic flow from the primary site, so that all (and only) the nodal basins at risk for metastatic disease will be dissected. The second piece of information is the precise location of the sentinel lymph node (or nodes), so that biopsy can be performed using a very limited skin incision and local anesthesia. The third is the identification of in-transit (or intercalated) nodes, defined as lymph nodes along the channel from the primary site to the regional basin, and marking of these for possible harvesting and histologic evaluation.
RADIOPHARMACEUTICALS
In radioguided surgery for sentinel lymph node biopsy, the radiopharmaceutical should ensure good visualization of the lymphatic channels leading from the site of interstitial administration to the corresponding lymph node while at the same time being preferentially retained in the first lymph node (or nodes) encountered along such a lymphatic pathway (56). Tracer is retained in the lymph nodes because of the clearing function of macrophages based on active, saturable phagocytosis (65).
The biologic clearing mechanism of lymph nodes is lost when a node is massively involved with metastases. When few normal cells remain in the node, lymphoscintigraphy does not show that node. Attempts to visualize tumor-involved nodes with interstitial injection of specific tumor-seeking radioactive tracers (such as an antimelanoma monoclonal antibody) have, unfortunately, so far been disappointing (66,67).
A colloidal particle size of 2.5–1,000 nm is a prerequisite for efficient uptake of radiolabeled particles by macrophages, as are a net negative surface charge and opsonization of such micellae, thanks to the action of complement components C3, C4B, and C5 and of some α- and β-globulins (68,69). Several formulations (such as 198Au-colloid, 99mTc-antimony sulfide, 99mTc-sulfur colloid, 99mTc-stannous fluoride, 99mTc-rhenium sulfide, and nanocolloid or microcolloid of human serum albumin) undergo opsonization.
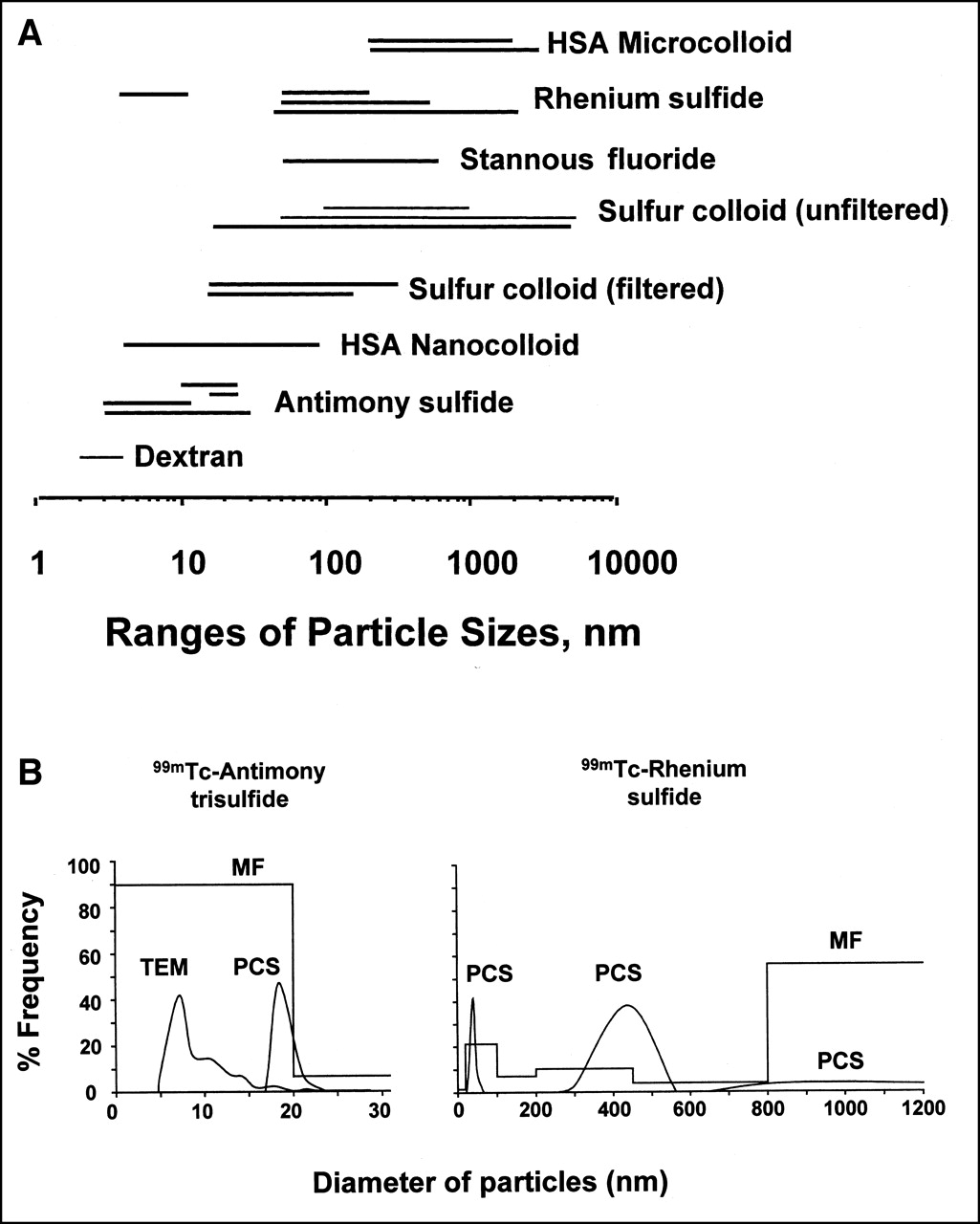
Radioactive colloids injected interstitially are cleared from the injection site by lymphatic drainage in a fashion related to the particle size, with small particles being cleared first and large particles being cleared later or, if they exceed 400 nm, not being cleared at all. Inconsistencies in the range of particle size reported by different authors (Fig. 2A) stem from several interfering factors, such as differences in the method of assessment (Fig. 2B), in the timing of the determination (before radiolabeling vs. after radiolabeling), in the stability of the agent after labeling, in the method of incubation (with serum vs. with physiologic saline), and in the labeling method (use of regular elution vs. technetium elution after a long interval of ingrowth). The pore size of any filters used (as with 99mTc-sulfur colloid) and in-house modifications of the reconstitution procedures represent additional variables to be considered (71–75).

(A) Diagrammatic representation on logarithmic scale of approximate ranges of particle size of different 99mTc-labeled colloids for lymphoscintigraphy, as derived from various sources (manufacturers, publications). Discrepant data (indicated by additional lines in graph) are occasionally reported by different authors for some radiopharmaceuticals, depending on factors such as measurement method, stability of agent after radiolabeling, and in-house modifications of reconstitution procedure. The 2 ranges represented for filtered sulfur colloid refer to presumed ranges obtained after filtration through 100- or 220-nm filter. (B) Examples of variable estimates of particle size distribution for 99mTc-antimony sulfide and 99mTc-rhenium sulfide when assessed by different methods. HSA = human serum albumin; MF = membrane filtration; PCS = photon correlation spectroscopy; TEM = transmission electron microscopy (modified from Tsopelas (70)).
Although sufficient for lymphoscintigraphic visualization and for γ-probe identification, the amount of radioactivity retained in the sentinel lymph node 15–18 h after interstitial injection of radiocolloid is generally low. Depending on the different radiocolloids used, approximately 0.34%–0.92% of the injected dose is retained per node when the tracer is injected subdermally in patients with cutaneous melanoma (76,77), although values have ranged from as low as 0.0013% to as high as 6.8% in a single study (78).
99mTc-Sulfur colloid is most commonly used in the United States. Microfiltration through 100- or 220-nm filters has been proposed, with a goal of using particles in the range of approximately 50–100 or 50–200 nm. Filtered 99mTc-sulfur colloid is generally preferred for sentinel lymph node studies (79), although some authors still claim the superiority of the unfiltered agent (80,81). The high lymph flow in the skin (particularly of the extremities) and the somewhat higher porosity of the lymphatic system (61,62,82) suggest that radiocolloids of larger particle size (between 200 and 300 nm) may yield satisfactory results in patients with cutaneous melanoma.
Most European investigators have used 99mTc-nanocolloid human serum albumin with particles of between 4 and approximately 100 nm (95% of the particles < 80 nm). This radiopharmaceutical offers the additional benefits of instant labeling at room temperature and stability both in vitro and in vivo.
Besides particle size, the number of particles injected is an important parameter in radioguided sentinel lymph node localization. This feature, which has to do with saturation of the clearing capacity of the sentinel lymph node based on active phagocytosis by macrophages, was earlier discussed at length (56). In particular, the specific activity of the preparation is important for administration of a preparation with the fewest particles. Therefore, methods of high-specific-activity labeling should be sought.
TECHNIQUES
Tracer Injection
A general consensus has developed over the last few years on the main parameters that define the optimal techniques for injecting radiocolloid for lymphatic mapping and sentinel lymph node biopsy in patients with malignant cutaneous melanoma (50,69,83–91).
The cells that give rise to cutaneous melanomas, melanocytes, are located between the dermis and the epidermis. Transformed melanocytes initially grow in this space, and from it they spread elsewhere. Therefore, there is no doubt that lymphatic drainage from these tumors follows the general pattern of lymph flow from the papillary and subpapillary plexus to the inner network in the reticular dermis and, in turn, to the larger collecting lymphatics in the subcutis. The subcutaneous plexus (terminal component of the overall superficial lymphatic circulation) communicates with the deep, epifascial lymphatic circulation collecting lymph from muscles, bones, and so forth (Fig. 1A).
These considerations explain why the concept of intradermal or subdermal injection of radiocolloid for lymphatic mapping in patients with cutaneous melanoma is generally accepted and applied routinely. Intradermal or subdermal injection is performed using 25- or 27-gauge needles, inserting the needle in a direction as tangent as possible to the skin surface for a few millimeters inside the skin; this modality of interstitial administration entails small volumes of injectate, just enough to produce a visible wheal in the skin (Fig. 3). Small volumes (0.05–0.2 mL, depending on the thickness of the skin in a specific anatomic region) are recommended in order not to collapse lymphatics (85); when the doses for injection are prepared (radioactive preparation containing 37 MBq/mL, or 1 mCi/mL), 0.1–0.2 mL of air is drawn into the syringe behind the radiocolloid to ensure that no tracer is left in the dead space of the syringe and needle. Care must be taken to avoid contamination of the patient’s skin during the procedure, because interstitial pressure builds up on intradermal or subdermal injection; contamination should be prevented by placement of a swab over the needle before it is withdrawn from the skin.

Intradermal–subdermal injection of radiocolloid for lymphatic mapping in patient recently scheduled for excision of malignant cutaneous melanoma on patient’s back.
The number and specific site of radiocolloid aliquots to inject varies according to the anatomic region being explored and whether the primary lesion is still present or has already been excised, always observing the general rule of injecting the tracer approximately 0.5–1 cm away from the scar or the tumor margin. One or 2 injections close to the center of the surgical scar (corresponding to the approximate original location of the excised tumor) can be sufficient for reliably visualizing the pattern of lymphatic drainage encountered by tumor cells leaving the melanoma; in cases of wide excisions or of a large melanoma still present in the skin, a total of 4, 6, or even 8 separate injections can be necessary, depending on different factors.
Often, we study patients 2–3 wk after tumor excision, when the histologic findings indicate a thin or intermediate-thickness cutaneous melanoma. Size and orientation of the surgical scar are dictated by both location and size of the tumor. If the melanoma is not exceedingly large, the surgeon makes the incision along the predominant lines of contraction of skeletal muscles directly underneath the tumor (Fig. 4). This recommended pattern may occasionally not be followed in cases of wide lesions, which may force the surgeon to adapt the incision so that an adequate 1- to 2-cm margin of apparently healthy skin is removed on each side of the melanoma (1 cm for lesions < 1 mm thick, 2 cm for lesion thicker than 1 mm).
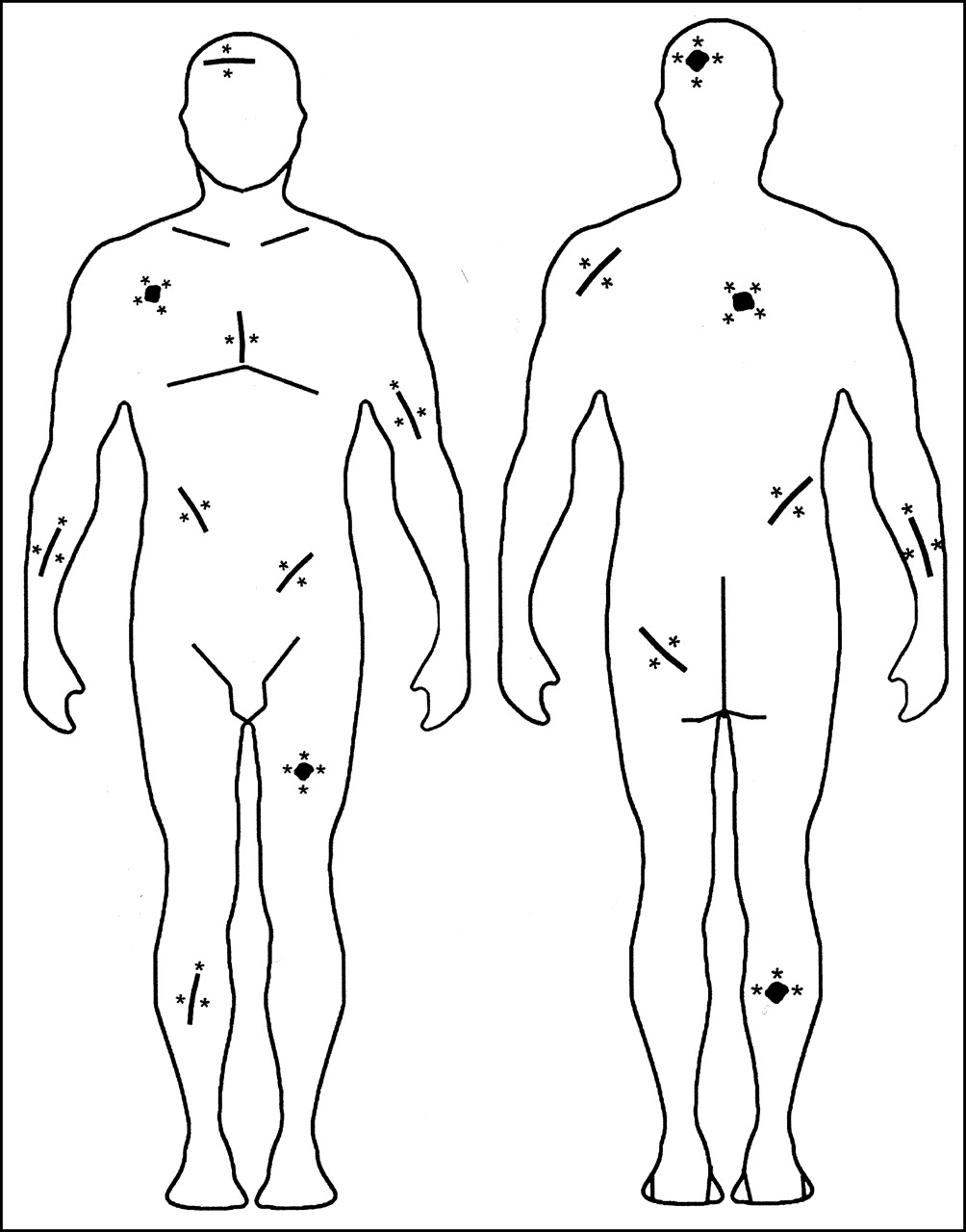
Diagrammatic representation of recommended injection sites for lymphatic mapping with radiocolloid according to region of body and orientation of surgical scar.
Keeping as a reference the orientation of the surgical scar, one should inject the tracer either on each side or on only one side of the scar, depending on location. If the scar is located in the upper limbs, the lymphatics can reliably be mapped by injecting 1 or 2 aliquots proximal to the scar. In fact, lymph flows unidirectionally from the more distal regions (hands and forearms) to the proximal regions (arms and axilla), unless a highly invasive melanoma has disrupted the normal lymphatic pattern (but this event will be clinically evident and should exclude sentinel lymph node biopsy). In the lower limb, there is a fundamental difference between drainage of lesions in the foot and drainage of lesions in the leg or thigh. Lymph flows unidirectionally from distal to proximal regions in the foot and leg, but lesions in the thigh can drain either proximally toward the groin or distally toward lymph nodes in the popliteal region. Therefore, tracer is injected only proximal to lesions in the foot and leg but both proximal and distal to lesions in the thigh to detect possible sentinel lymph nodes in the popliteal region (86). When the primary melanoma lesion (or surgical scar) is located in the trunk, selection of right or left side of the body for tracer injection should be based on proximity to the zone of ambiguous lymphatic drainage (Figs. 2B and 4). This consideration is particularly important for melanomas located in the head or neck, a region characterized by ambiguous lymphatic drainage not only in relation to right or left side with respect to the midline but also in terms of frontal-oriented versus dorsal-oriented lymph flow. Therefore, at least 4 separate tracer injections should be performed, roughly equatorially around the lesion or surgical scar, in patients with malignant cutaneous melanomas located in the head or neck.
If no migration of radioactivity is noted within 10 min of injection, gentle massage of the injection site or exercise of the extremities is recommended. Usually, failure to migrate occurs when tracer injection is too deep, becoming frankly subcutaneous. Inflamed, indurated, or scarred skin can be problematic; therefore, an alternative adjacent site should be selected to avoid such areas. If the area is inflamed and infected, the procedure should be rescheduled until after resolution of the local disease.
Imaging and External γ-Probe Counting
A large-field-of-view gamma camera equipped with a high-resolution collimator, adjusted to record both dynamic and static images with a 10% window centered on the 140-keV energy peak of 99mTc, should be used. Both dynamic and static scintigraphic acquisitions are essential to indicate the drainage basin, determine the number of sentinel lymph nodes, locate sentinel nodes outside the usual nodal basins, and differentiate sentinel nodes (first-echelon nodes) from nonsentinel nodes (second-echelon nodes) (92). Starting immediately after radiotracer injection, dynamic acquisition over 20–30 min (20 s per frame, with a 128 × 128 matrix) serves to reveal the progression of lymphatic flow (drainage pattern) and to distinguish first-tier from second-tier lymph nodes. The draining lymphatic basins are outlined, and the number and position of sentinel nodes are depicted (Fig. 5); the site of these nodes can be marked on the overlying skin by the nuclear medicine physician, thus localizing the nodes for the surgeon. If necessary, acquisition is continued until a total of 45 min to adequately visualize the sentinel lymph nodes. Subsequently, orthogonal (anterior or posterior) and oblique (as needed) static images are acquired (300 s, with a 256 × 256 matrix) to localize the nodes in 3 dimensions. To facilitate topographic localization, a 57Co flood source (or, when available, a CT scan) can be used for simultaneous transmission imaging, or the body silhouette can be outlined by moving a radioactive point source along the contour of the body while recording the scan. This procedure helps to identify sentinel lymph nodes and to mark their cutaneous projection in each draining basin. Static images (spot views or whole-body scans) can be repeated at 2 h and, when nodes are not clearly depicted, again at 4–6 h after injection or even just before operation. The study in the nuclear medicine department is completed by further confirming the exact location of the sentinel lymph nodes by external counting with the handheld γ-probe detector.

Representative scans illustrate variable patterns of lymphatic drainage in patients with primary melanomas in different regions of body. Imaging times were between 30 and 60 min after intradermal or subdermal injection of various aliquots of 99mTc-human serum albumin nanocolloid. Upper left panel shows lymphoscintigram (anterior projection) obtained from patient who recently underwent surgery for cutaneous melanoma on elbow: Lymph flows toward single sentinel node in left axilla. Upper right panel shows lymphoscintigram (anterior projection) obtained from patient with cutaneous melanoma on right thigh (just above knee): Lymph follows at least 2 main channels converging at sentinel node in right groin. Lower left panel shows lymphoscintigram (posterior projection) obtained from patient who recently underwent surgery for cutaneous melanoma on his back (just about midline): Lymph flows through several channels toward sentinel nodes in both axillae. Right lower panel shows lymphoscintigram (posterior projection) obtained from patient who recently underwent surgery for cutaneous melanoma on his back (just left of midline): Lymph follows channels to both axillae and to right groin (visualized faintly in posterior projection because of photon attenuation through body).
Intraoperative γ-Probe Counting
With the patient positioned on the operating table, external γ-probe counting should be repeated to confirm the location of the sentinel lymph nodes before the procedure. Depending on the site of the primary lesion, different lymphatic basins may have been identified by preoperative lymphoscintigraphy. In each site, the area with highest activity (counts per second) is identified and topographically correlated with the intradermal tattoo that has been positioned during lymphoscintigraphy. Furthermore, counts are taken over the sites of tracer injection and along the lymphatic channels draining to the lymphatic basins. All such external measurements are recorded for subsequent comparison with intraoperative count rates (which should obviously be correspondingly higher than external count rates). The patient is then prepared and draped in the usual sterile fashion. Attention is turned to all the lymphatic basins that have been identified as at risk for metastasis according to the lymphoscintigraphic pattern. Surgeons usually search for the sentinel lymph nodes first and then proceed to remove the primary melanoma (if it is still in place) or to excise a wider skin margin around the previous surgical scar (if this indication has emerged from the histopathology of the primary lesion).
In vivo radioactivity (counts per second) is measured in the surgical bed opened by making a 2- to 4-cm incision over the area with highest activity as determined by external counting. Intraoperatively, the γ-probe is moved carefully and slowly, because the counting rate changes almost instantly from hundreds of counts per second to nearly zero on minimal movement of the probe. Sentinel lymph nodes may be only a few millimeters in diameter, and the radiocolloid is retained in the sinusoidal spaces near the afferent lymph channels. Thus, recognition of the node may be difficult if the probe is moved too quickly.
Hot nodes are usually identified by comparison with background radioactivity, which is defined as the average count rates of the surrounding nonsentinel nodes and lymph node basin. Ratios of sentinel lymph node counts to background counts are typically on the order of 10:1, 15:1, or even 20:1. This wide range of values depends on the dose injected, the type of tracer injected, the elapsed time between tracer injection and surgery, and the type of γ-probe used. In particular, if a small-particle radiocolloid is injected, lymphatic vessels are visualized within a few minutes after injection and radioactive lymph quickly progresses to show second-tier or third-tier nodes as well. In this case, the ratio of sentinel counts to nonsentinel counts will be relatively lower than that observed after injection of a larger-particle radiocolloid (which is preferentially retained in the true sentinel node). This factor should be considered to avoid unnecessary biopsy of radioactive but nonsentinel lymph nodes.
After the sentinel lymph node is identified through both in vivo imaging and counting and ex vivo probe measurements, the γ-probe is used to measure residual counts in the lymphatic basins so as to identify and remove any additional hot nodes (93). In this regard, several different definitions based on radioactivity contents have been proposed for the sentinel lymph node (94), including a counting rate > 300 in 10 s (93), a ratio > 2 for in vivo sentinel to nonsentinel counts (95), and a ratio > 10 for ex vivo sentinel to nonsentinel counts (41). These multiple definitions and methodologies complicate evaluation of published data and do not provide a standard for discussion in the medical forum.
In our experience, any lymph node whose counting rate is at least 20% of the counting rate of the hottest node in the basin should be considered an additional sentinel node. As already noted, in approximately 13% of patients with lymph node metastasis, the node involved with tumor had substantially less activity than the hottest node (26). After all sentinel nodes are removed for histopathologic examination, residual radioactivity should be <10% of the counting rate in the hottest node. This procedure is performed in all lymphatic draining basins identified by preoperative lymphoscintigraphy.
In addition to γ-probe–guided sentinel lymph node biopsy, many surgeons also inject a vital blue dye around the lesion a few minutes before starting the surgical procedure. This technique can usefully complement the radioguided procedure by providing a visual road map to the sentinel node and can be important because a noninvolved lymph node may be only a few millimeters in diameter and very soft to palpation. When blue dye is used, the surgeon removes for biopsy all hot lymph nodes and possibly all blue-stained nodes as well, even if not hot. However, the blue dye is usually only a visual aid to the identification of sentinel nodes by γ-probe (96,97).
The success rate of lymphoscintigraphy for sentinel node identification is approximately 98%, whereas use of the vital blue-dye technique alone identifies 75%–80%. The addition of blue dye improves radioguided identification of sentinel nodes to a 98%–99% success rate, especially if the sentinel lymph node is diffusely metastatic, when its capacity to retain the radiocolloid is impaired.
The criteria for γ-probe identification of a sentinel lymph node are based on detecting a focal zone of radioactivity accumulation with a ratio of counts (hot spot to background) > 10 (typically in the 10–100 range). The operative site should then be reexamined to ensure that the area of radioactivity has been removed and that a second node is not also active; if one is, it should be removed and the surgical bed reexamined until no areas of increased counts are found. Complete removal of sentinel lymph nodes is confirmed by reduction of the counting rate in the surgical area to background levels. Histopathologic examination is performed on the lymph node with the highest counting rate and on any additional lymph node with a counting rate at least 20% of that in the hottest node.
Histopathologic Examination
The detection of tumor cells in the lymph node requires special stains and detailed evaluation of the sentinel node. In contrast to routine histopathology, in which only a few sections stained with hematoxylin–eosin are evaluated, sentinel node evaluation should include 10–20 sections (if not the entire node) and specific immune staining to identify tumor involvement. The importance of detailed histologic examination is apparent from retrospective studies on nodal recurrences in patients whose sentinel nodes were reported as uninvolved and negative for tumor on conventional pathologic examination. When additional sections were evaluated and special stains were applied, tumor cells were shown in approximately 12% of the patients (51–53).
These observations stress the importance of detailed histologic examination of sentinel node biopsy samples. From a clinical perspective, application of this time-consuming, rigorous approach to all biopsies is difficult, but it is now apparent that patients with other tumors, such as breast cancer, also benefit when evaluated by this compulsive approach (98).
Histopathologic assessment of the excised sentinel nodes should be as complete as possible (99,100). The harvested node should be bisected along its main axis, starting at the hilus, and multiple sections should be taken from each half. Some sections are used for hematoxylin–eosin staining, whereas others are processed by immunohistochemistry; additional sections can be kept unstained for additional processing, as needed (99–102).
The need for high-quality histopathologic examination has led to reconsideration of the role of frozen sections in these patients. The possibility of performing both a selective lymphadenectomy and, if necessary, a full excision of the draining basin has prompted surgeons to ask for intraoperative histopathology. However, examination of frozen sections is not recommended for nonpalpable nodes because of the relatively poor quality of frozen-section histology (102). Permanent sections allow more accurate morphologic evaluation; moreover, immunohistochemistry can be used to identify the melanocytic cells. Immunohistology is considered crucial by most groups, particularly to detect subtle micrometastases (103). In fact, immunohistochemistry enables differentiation between melanized and nonmelanized macrophages, which may closely resemble melanoma cells (102).
Several monoclonal and polyclonal antibodies are now commercially available and can consistently be applied to formalin-fixed and paraffin-embedded tissues. Because of the large experience acquired by pathologists worldwide with antibodies to the S-100 protein and the HMB-45 antigen, these are especially reliable. Antibodies to the MelanA/Mart1 and NKC1 antigens are additional reagents that seem particularly useful for increasing the effectiveness of immunohistochemistry for detecting micrometastases (102).
However, each antibody has a different specificity and sensitivity; therefore, accurate assessment of the classic morphologic features of the cells is required to avoid erroneous results. Despite its utility, immunohistochemistry should not be used as the fundamental technique to examine sentinel lymph nodes for melanoma metastases. In particular, dendritic cells—and, occasionally, even macrophages and normal structures such as nerves, if cut transversely or if close to the capsule—can be misdiagnosed for metastatic melanoma because of their strong immunoreactivity for the S-100 antibody (104). Additional benign lesions staining positive for the S-100 protein include nodal nevi inclusions (105). Although these structures are found more frequently in the capsule, they can also be found in the internal trabecula; moreover, they have been found in lymph nodes draining from malignant cutaneous melanoma, more frequently (up to 20%) in the sentinel lymph node than in nonsentinel nodes (105,106).
HMB-45 staining can be observed in areas with calcifications, which are easily found in the trabeculae of the inguinal and pelvic lymph nodes, whereas staining is negative in up to 20%–30% of melanomas (102). Thus, immunohistochemistry (possibly performed with both antibodies, S-100 and HMB-45 (107)) combined with careful conventional histopathology based on step or multiple sections is currently the most reliable method to assess sentinel lymph node status and predict the nodal status of melanoma patients.
Interest in detecting occult metastases in sentinel nodes has prompted investigators to explore the most sensitive tools available, including primary cell culture and amplification of messenger RNA for specific biologic markers by the reverse transcription polymerase chain reaction. In principle, these techniques can detect even a very few or single and isolated metastatic cells among 1–10 million normal cells (108). Such paramount sensitivity is in comparison with a detection limit of approximately 1 malignant cell in 10,000 for conventional hematoxylin–eosin staining and approximately 1 malignant cell in 100,000 for immunohistochemistry (27). Candidate markers for malignant melanoma include the tyrosinase gene (encoding an enzyme associated with melanin synthesis) and messenger RNA present in T lymphocytes infiltrating the melanoma (MART-1) (109–120).
A significant fraction of patients whose sentinel nodes are negative by careful histopathology and immunohistochemistry are polymerase chain reaction positive. However, there is no general consensus on the clinical significance of these findings. Furthermore, it is also generally recognized that these ultrasensitive methods are fraught with a relatively high false-positive rate (115), linked basically to nodal nevi inclusions and nerve structures (102,105) and even to fragments of tyrosinase messenger RNA that survive in macrophages and can only be differentiated from metastatic cells by examining cell morphology.
One problem with the current techniques using conventional reverse transcription polymerase chain reaction (more feasible than in situ reverse transcription polymerase chain reaction, which is also applicable to formalin-fixed and paraffin-embedded sections) is the requirement that a sizable fraction of the lymph node (approximately half) be processed for tissue homogenization and DNA or RNA extraction. A fraction of this size is not available for regular histology and immunohistochemistry (the only validated procedure). This large tissue requirement raises concern about the possibility of losing some diagnostic information.
A highly specific molecular marker of malignancy is currently not available for melanoma, and only a comparison of histology and molecular biology performed on the same tissue or cells may enable a comparative assessment of the actual sensitivity of each method. Although studies under way will likely increase the specificity of molecular biology techniques, no clinical decisions should yet be based on polymerase chain reaction determinations, in order to avoid unnecessary lymphadenectomy procedures and further medical treatment.
BIOPSY
The search for micrometastases in the sentinel lymph node is now consistently accepted for patients with cutaneous melanoma whose lesions are ≥1 mm thick or even <1 mm but at Clark level IV or V or with ulceration (31,32). A positive node identifies patients with a worse prognosis, even among those with cutaneous lesions thicker than 4 mm. In fact, among patients with 4-mm-thick lesions, the 5-y survival rate is 61% for those with negative sentinel lymph nodes but only 30% for those with positive sentinel lymph nodes (121). After a positive sentinel node is identified, the only widely recommended treatment is to complete the lymphadenectomy of the lymphatic basin containing the metastatic sentinel node (122). Lymphadenectomy alone has improved the 5-y survival rate from 27% to 48% (123).
To determine the incidence of false-negative studies of sentinel nodes (so-called skip metastasis), investigators have evaluated patients through use of sentinel lymph node biopsy followed by complete lymphadenectomy. Extensive histopathologic examination of all removed nodes showed that fewer than 2% of patients had negative sentinel nodes with metastases in other lymph nodes (8,12,34,40,41,50,52,76,86). Other studies based on long-term recurrences in previously mapped negative lymphatic basins have suggested that the incidence of false-negative sentinel node studies may be higher, ranging from 4% (i.e., 10/243 patients) (51) to 8% or 9% (50,124), 11% (125), 16% (126), 19% (127), and even 27% (128). Many of these studies used either frozen sections or incomplete sampling of the node or failed to examine the sections immunohistologically.
In addition to the tumor status of the sentinel node, several prognostic indices have been developed (129). Cochran et al. (122,130) combined Breslow thickness of the primary melanoma, volume of the tumor in the sentinel lymph node, and density of interdigitating cells in the sentinel node (as an index of downregulation in the lymph node) to predict outcome and tumor status of the nonsentinel nodes in melanoma patients. Microstaging of the sentinel lymph node based on accurate histomorphometric evaluation takes on an increasingly relevant role (11,131,132).
Uncertainties about the actual incidence of false-negative sentinel node biopsies and about the impact of such false-negative findings on long-term clinical outcome are only part of the controversy still surrounding the issue of whether sentinel node biopsy should be considered the standard of care for patients with malignant cutaneous melanoma (26,133–136). One reason for the debate is the lack of effective adjuvant therapy (in addition to regional lymph nodal dissection) once it has been ascertained that the sentinel lymph nodes harbor metastases (35,36,123,137,138).
The only positive trial in terms of overall survival and disease-free survival concerned the use of high-dose interferon versus no therapy in patients with stage III melanoma (28). The favorable outcome in these patients has been maintained after a median follow-up of more than 10 y but has not been confirmed by a subsequent trial comparing high-dose and low-dose interferon versus no therapy (139). However, a recent short-term trial comparing high-dose interferon with ganglioside vaccine supported the beneficial effects of interferon therapy (140), thus leaving the clinician with a therapeutic option rather than a standard treatment. Many ongoing multicenter and multinational randomized trials are assessing the impact of sentinel lymph node biopsy on the long-term survival of patients with cutaneous melanoma.
Although investigators are still debating about evidence that sentinel lymph node biopsy followed by early regional node dissection can improve regional control (and survival), lymphatic mapping definitely provides important prognostic information (8), as shown by an overall 93% 3-y survival in patients with a tumor-negative sentinel node versus 67% in patients with a tumor-positive sentinel node (125). This concept has become so accepted (137) that the tumor status of the sentinel lymph node is now becoming an essential parameter in the new staging system for patients with cutaneous melanoma (31,32,141–143) (Tables 1 and 2).
Final Version of TNM Staging System of American Joint Committee on Cancer for Malignant Cutaneous Melanoma
Survival Rates of Patients with Malignant Cutaneous Melanoma According to Initial Pathology Staging
A new exciting perspective on the sentinel lymph node biopsy procedure is that it will lead to timely diagnosis of micrometastasis in regional lymph nodes. This possibility not only makes sentinel node biopsy useful as a staging procedure but also opens new windows of opportunity to assess micrometastasis per se and its evolution within the sentinel node. In fact, sentinel nodes may be the initial sites of antigen presentation leading to an immune response, thus implying that sentinel lymph nodes without micrometastasis may be activated by submicroscopic cell debris or by soluble tumor antigens, whereas cytokine production may be suppressed by micrometastasis (144).
It has not yet been definitely proved that application of the sentinel lymph node biopsy improves the overall clinical outcome and long-term survival of patients with cutaneous melanoma. However, the procedure is certainly becoming the standard of care for these patients as a modality of lymphatic mapping, at least for prognosis, because either the number or the percentage of metastatic lymph nodes is the strongest predictor of outcome (31,32,141–143).
The indications for sentinel lymph node biopsy in patients with malignant cutaneous melanoma are now somewhat wide, encompassing any patient who has an intact melanoma or has had an incisional or excisional biopsy of cutaneous melanoma (143). Biopsy is contraindicated in patients who have already had a wide excision with or without closure by a rotation skin flap, because lymphatic drainage of the primary site can be deeply modified by such a surgical procedure. Although patients with primary melanomas between 1 and 4 mm thick are, in principle, the most likely to benefit from sentinel lymph node biopsy, it is quickly becoming a required standard of care for staging (31,32,141,143).
LEARNING CURVE
The learning curve for sentinel lymph node biopsy reflects the time required to form a team of specialists in nuclear medicine, surgery, and pathology to work together (56). A major difference in the case of melanoma versus breast cancer concerns the role of the pathologist. Usually, when performing sentinel lymph node biopsy on a patient with breast cancer, the team in the operating room relies on the histopathologic results for the excised sentinel node in deciding impromptu whether to extend the surgery and dissect the axillary lymph node. Therefore, histopathologic evaluation of the sentinel node has to be as fast and yet as accurate as possible. Because of this stringent requirement, several approaches have been developed to optimize the speed and sensitivity of histopathologic examination (56). Moreover, the examination usually occurs near the operating room, in an environment and manner quite different from those of a regular histopathology laboratory. However, even breast cancer patients are receiving the more rigorous histopathologic examination that is applied to melanoma patients, with fixed specimens being examined by immunohistochemistry and reverse transcription polymerase chain reaction. Because this procedure takes time, a growing number of patients are undergoing sentinel node biopsy followed later by surgery for the primary tumor.
Although some controversy exists about the number of procedures that a team must complete to qualify as a routine performer of lymphatic mapping in patients with cutaneous melanoma, we agree with Morton’s suggestion of 30–50 procedures, considerably fewer than the 60–80 procedures considered necessary for breast cancer (143). We also believe that the learning phase will be shorter if all or some of the team members have prior experience with intraoperative lymphatic mapping in other clinical applications (mostly breast cancer), either under radioguidance or under visual blue-dye guidance.
As is the case for breast cancer teams (56), multidisciplinary teams for sentinel lymph node biopsy in melanoma patients must meet 2 important performance requirements to be considered as having completed their learning phase: The sentinel lymph node must be successfully identified in at least 97% of patients, and metastasis must be found in the sentinel node of between 12% and 20% of patients whose melanoma is >1 mm thick.
RADIATION PROTECTION
The low doses of radiocolloid injected interstitially for lymphoscintigraphy and for subsequent radioguided sentinel lymph node biopsy do not present a significant radiation burden to patients (72,145). However, surgeons, operating room personnel, and technologists in the pathology department are often concerned about handling radioactive substances. Measurements of handled tissues from breast cancer patients undergoing sentinel node studies confirmed that the radiation burden to non–nuclear medicine personnel involved in the procedure is minimal. Cumulative whole-body doses to the surgeon (the person with the highest radiation exposure) for 100 operations correspond, at most, to approximately 1% (mean absorbed dose) or approximately 10% (mean effective dose) of the annual dose limits for the general population. These dose limits may be slightly higher for surgeons operating on patients with cutaneous melanoma, because the radiocolloid is usually injected in relatively larger amounts (by a factor of approximately 3, considering the various aliquots injected around a surgical scar or around the primary tumor in situ).
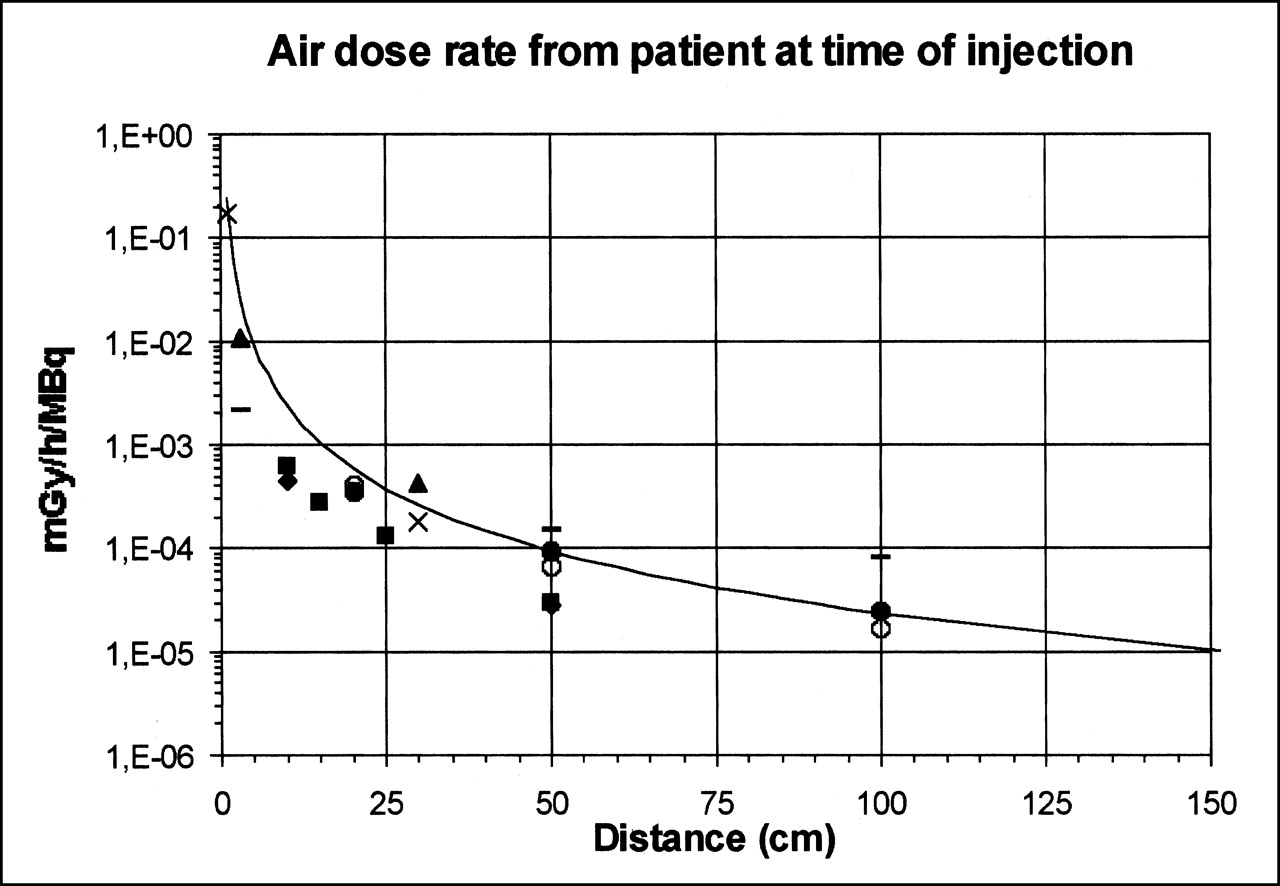
A preliminary, a priori estimate of radiation doses to personnel can be obtained using the following general formula, which encompasses the radioisotope used and total dose injected, the elapsed time between tracer injection and surgery, the duration of surgery, and other possible situations: dose = f · A0 · t/d 2 · fret · fdec(tel) · fatt(depth), where f is a conversion constant (exposure-kerma-dose factor for 99mTc), A0 is injected activity, t is the duration of the procedure (surgery or histopathology), d is the mean distance from the source during the procedure (surgery or histopathology), fret is the fraction of injected tracer retained in tissues (95% at injection site and 5% at most in lymph nodes), fdec(tel) is physical decay during the elapsed time between tracer injection and operation (surgery or histopathology), and fatt(depth) is the tissue attenuation of the source (injection site or lymph node). The validity of this formula has been preliminarily validated through calculation of the radiation dose based on the parameters described in several published articles (145–151) and through comparison of the results of these calculations with actual measurements or calculations provided in each article, as shown in Figure 6. The estimated and observed radiation doses agreed closely, thus suggesting that the formula can be applied for any preliminary calculation of the expected radiation dose to personnel involved in radioguided surgery.
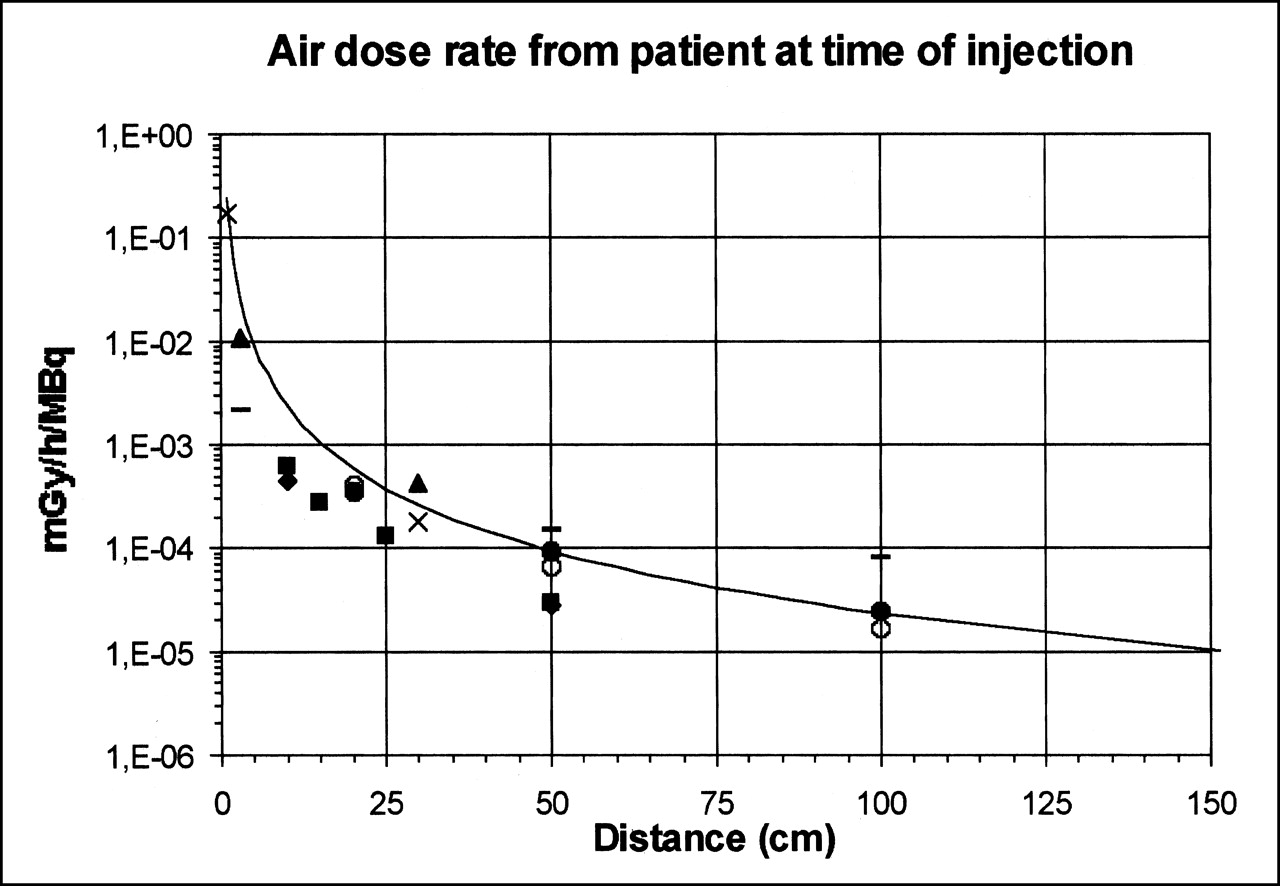
Plot of theoretic curve for air dose rate calculated according to general formula described in text and considering 99mTc point source according to Radionuclide and Radiation Protection Data Handbook 1998 (148) (2.5–5 mGy/h/MBq at 100 cm). For normalization purposes, all dose evaluations reported in plot have been derived from published data by conversion to air dose rate calculated at injection time and at different distances from source. Theoretic curve (2.3e−5 mGy/h/MBq at 100 cm, totally independent from data points plotted in graph) well describes pattern of distribution of datasets reported by other groups, either estimated according to other formulas or measured in vivo (patients) or in vitro (phantoms). By slightly overestimating reported dose rates, general formula actually approximates values in excess—a definite plus for radiation safety purposes. – = data from Cremonesi et al. (145) (measured from patients at time of tracer injection); ♦ = data from Pijpers et al. (146) (measured from patients); ▪ = data from Pijpers et al. (146) (measured with phantom); ▴ = data from Stratmann et al. (149) (measured from patients); ○ = data from Motta et al. (150) (estimated); • = data from Motta et al. (150) (measured from patients); × = data from Waddington et al. (151) (estimated).
CONCLUSION
Despite some differences in the way radioguided sentinel lymph node biopsy is being performed around the world, the excellent results that have been reported univocally point to this procedure as being the most safe, efficient, and cost-effective modality for lymphatic mapping in patients with primary cutaneous melanoma (143,152–154). This conclusion, besides being based on the high reported success rate for identification of sentinel lymph nodes, is also based on the accuracy of the procedure and, therefore, its ability to spare melanoma patients from unnecessarily extensive surgery (138,155,156).
Although the reliability of sentinel lymph node biopsy in patients with malignant melanoma is widely recognized both for staging and for prognosis, some issues are still open for discussion. The correct procedure for performing radioguided sentinel lymph node biopsy has now been clarified, from patient inclusion to choice of radiocolloid, tracer injection, acquisition of lymphoscintigraphy, intraoperative γ-probe searching, and, finally, histopathologic evaluation of the removed node. Nevertheless, the long-term impact of sentinel node biopsy (with the ensuing elective lymph node dissection of a metastatic basin) on clinical outcome has yet to be unequivocally determined. Critical metaanalysis of all long-term follow-up and survival studies published so far will likely help in the assessment of actual benefit to patients with cutaneous melanoma.
The encouraging results reported for sentinel lymph node biopsy, especially in patients with melanoma, have renewed the interest of investigators in defining a given therapeutic strategy based on the pathophysiology of each phase in the natural history of a disease. These considerations make sentinel lymph node biopsy ideal for implementation in other types of cancer as well.
Acknowledgments
The authors thank all their coworkers who, at various institutions, have helped to develop programs for radioguided sentinel lymph node biopsy and to accumulate the experience on which this article was based. In particular, the authors thank Drs. Pietro Bianchi, Ferdinando Buffoni, and Giuseppe Agnese (Nuclear Medicine Service, University of Genoa); Drs. Carmine Di Somma, Franca Carli, and Guido Nicolò (National Cancer Institute of Genoa); Drs. Gian Piero Manca and Paola Erba (Regional Center of Nuclear Medicine, University of Pisa); Drs. Concetta De Cicco and Marco Chinol (Nuclear Medicine Service, European Institute of Oncology, Milan); Dr. Alessandro Testori (Division of Surgery, European Institute of Oncology, Milan); and Dr. Roberto Gennari (Division of Surgery, “Fondazione Maugeri,” Pavia). Research was supported in part by the Italian Ministry of Education, University and Research, the Italian Ministry of Health, and the Italian Association for Cancer Research.
Footnotes
Received Dec. 6, 2001; revision accepted Feb. 28, 2002.
For correspondence or reprints contact: Giuliano Mariani, MD, Regional Center of Nuclear Medicine, University of Pisa Medical School, Via Roma 67, I-56126 Pisa, Italy.
E-mail: g.mariani{at}do.med.unipi.it
*NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/education/ce_online.html) UNTIL JUNE 2003.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Results of a Prospective Multicenter International Atomic Energy Agency Sentinel Node Trial on the Value of SPECT/CT Over Planar Imaging in Various Malignancies
- In vivo albumin labeling and lymphatic imaging
- Accuracy and Reproducibility of Lymphoscintigraphy for Sentinel Node Detection in Patients with Cutaneous Melanoma
- Optimal Detection of Sentinel Lymph Node Metastases by Intraoperative Radioactive Threshold and Molecular Analysis in Patients with Melanoma
- Role of Nuclear Medicine in the Management of Cutaneous Malignant Melanoma
- Is the "Ideal" {gamma}-Probe for Intraoperative Radioguided Surgery Conceivable?
- Staging of Regional Lymph Nodes in Melanoma Patients by Means of 99mTc-MIBI Scintigraphy
- Lymphoscintigraphy for Sentinel Node Mapping Using a Hybrid SPECT/CT System
- Patterns of Lymphatic Drainage from the Skin in Patients with Melanoma