


Abstract
The aim of this study was to evaluate quantitatively the heterogeneity of lung perfusion scans in patients with primary pulmonary hypertension (PPH) and to compare it with the severity of disease. Methods: Lung perfusion scans were obtained on 22 patients with PPH and 12 age-matched control subjects. The perfused area rates (PARs) were calculated by dividing the lung area in each 10% threshold width from 10% to 100% of maximal counts by total lung area. The total absolute difference in the PAR between each patient and the mean control value was assumed as the perfusion index of the lung (P index). The P index was compared with hemodynamic parameters and the right ventricular ejection fraction (RVEF), including 7 patients who received long-term vasodilator therapy. Results: The P index correlated significantly with mean pulmonary arterial pressure (P < 0.001) and RVEF (P < 0.05). In patients with vasodilator therapy, the P index was improved significantly after therapy (P < 0.05) and was associated with a reduction in pulmonary arterial pressure. Conclusion: Quantitative assessment of lung perfusion irregularity might provide useful information about the severity of disease and the effect of therapy in addition to the routine visual representation.
Primary pulmonary hypertension (PPH) is characterized by a progressive increase in pulmonary vascular pressure and resistance that leads to right ventricular hypertrophy and cor pulmonale (1). Histopathologic studies on PPH revealed medial smooth muscle hypertrophy and intimal endothelial proliferation in small pulmonary arteries (2). Because PPH usually takes a long time to diagnose, the prognosis probably depends on making a diagnosis when the pulmonary circulation is responsive to vasodilator therapy. Thus, noninvasive methods to assess the severity of pulmonary hypertension and the effects of various therapies are needed in the management of patients with PPH. The ventilation—perfusion scan is obtained primarily to exclude thromboembolisms in patients with PPH, but lung perfusion scans often show patchy loss of lung perfusion, which is known commonly as a mottled pattern (3,4). However, the pathogenesis and etiology of this phenomenon have not been established.
The aim of this study was to evaluate quantitatively the nonuniform distribution of lung perfusion scans in patients with PPH and to assess the association between lung perfusion scan heterogeneity and the severity of PPH.
MATERIALS AND METHODS
Patients
Between 1997 and 2000, 196 patients who had symptomatic pulmonary hypertension (New York Heart Association functional class II though class IV) (5) underwent lung perfusion scanning. Of them, 22 patients (7 men, 15 women; mean age, 36.4 ± 12.1 y; age range, 17–65 y) were diagnosed as having PPH and recruited for this study. PPH was defined as pulmonary hypertension (mean pulmonary arterial pressure of >25 mm Hg and pulmonary wedge pressure of <12 mm Hg at rest) on the basis of the criteria of the National Institutes of Health registry on PPH (6). We excluded patients with signs of collagen vascular disease, positive antinuclear antibody, history of drug abuse, use of diet pills, or history of liver disease. Four patients (18%) were classified as New York Heart Association functional class II, 15 (68%) as class III, and 3 (14%) as class IV. Serial lung perfusion scanning and right heart catheterization were performed on 7 patients before and during continuous infusion of prostacyclin (PGI2) for vasodilator therapy (7). Six to 24 ng/kg/min of intravenous PGI2 were given to these patients (8). The mean follow-up period of the lung perfusion scan was 283 d (range, 163–448 d). Follow-up right heart catheterization was also performed within 2 wk of the second lung perfusion scan.
All patients were given an explanation of the purpose of the study and provided written informed consent according to a protocol approved by the Human Investigations Committee of our institute.
Lung Perfusion Scans
A 150-MBq dose of 99mTc-labeled macroaggregated albumin (99mTc-MAA) (Daiichi Radioisotope Laboratory, Inc., Tokyo, Japan) was injected into an antecubital vein with the patient in a supine position. Just after tracer administration, lung scanning was performed using a gamma-camera system (VERTEX; ADAC Laboratories, Milpitas, CA) equipped with a high-resolution collimator. Image acquisition parameters were a 512 × 512 matrix and a 20% main window centered at the 99mTc photopeak energy (140 keV). Anterior, posterior, both lateral, and posterior oblique views were collected. Each view was acquired for 1,000,000 counts. To allow quantitative analysis of lung perfusion scans, the images of 12 age-matched healthy subjects (5 men, 7 women; mean age, 30.6 ± 8.6 y; age range, 19–44 y) were used as the control group.
The quantitative analysis of lung perfusion scans was performed by applying a modification of the previously described method (9). Briefly, the posterior planar image was transferred from the gamma-camera workstation to a personal computer. On the public domain, image-analysis program (National Institutes of Health image program, version 156b18), the area of pixels was calculated at every 10% cutoff level of the maximal pixel radioactivity, from 10% to 100%, as the perfused area (PAn). The threshold width number (n) was taken from 1 to 9 for every additional 10% threshold. For example, letting t be the threshold, the threshold number is 1 for 10% ≤ t < 20%, 2 for 20% ≤ t < 30%, … 9 for 90% ≤ t < 100%, successively. Then, the total areas above 10% of the maximum were summed as the total lung area (L). The perfused area rate (PARn) was calculated separately for the threshold width number as:

The mean PAR curve of the lung derived from the 12 control subjects is shown in Figure 1. For instance, we found that the area of ≥10% but <20% of maximal activity (PAR1) is 31.6% ± 3.1% of the total lung area in the control subjects. In the same way, PAR2 = 20.0% ± 1.2%, PAR3 = 15.2% ± 1.6%, and so the rest. There were no apparent differences among the control subjects for each threshold width number.
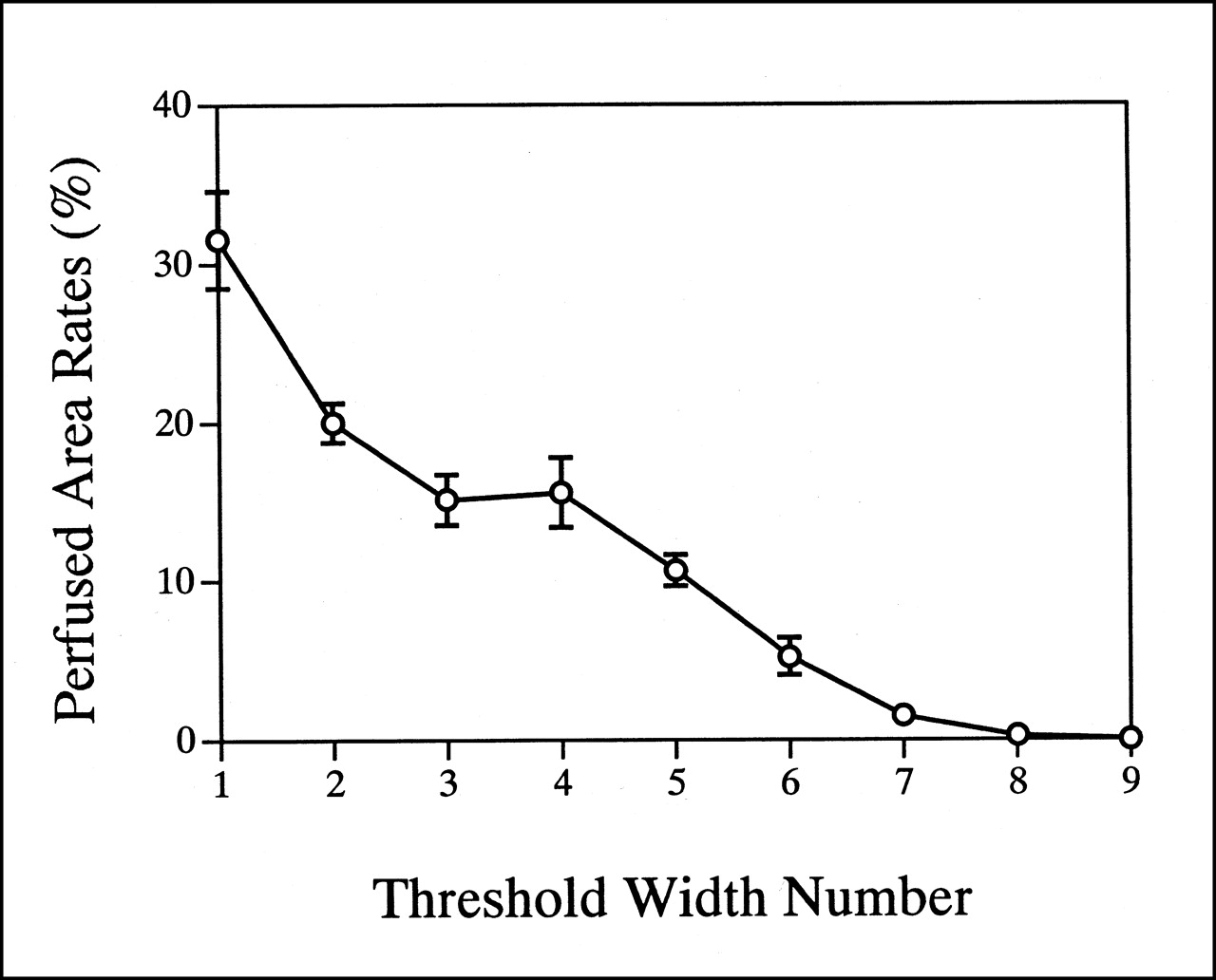
Mean PAR curve in 12 control subjects. Error bars represent ±1 SD of mean value at each threshold width number.
To assess the diffuse lung perfusion irregularity, the total absolute difference in PAR between each patient and the mean control value (perfusion index of the lung [P index]) was calculated as:
 where PARnc is the mean of PARn of the 12 control subjects.
where PARnc is the mean of PARn of the 12 control subjects.
Hemodynamic Measurements
Within 1 mo of lung perfusion scans (mean, 11.2 ± 11.0 d; range, 1–30 d), right heart catheterization was performed on all patients after an overnight fast. The mean pulmonary arterial pressure (mPAP) was recorded and cardiac output (CO) was determined by Fick’s method (10). Total pulmonary resistance (TPR) was calculated by dividing mPAP by CO.
First-Pass Radionuclide Angiography
Sixteen patients underwent radionuclide angiography to assess the right ventricular ejection fraction (RVEF). A rapid bolus injection of 740 MBq 99mTc-labeled red blood cells was performed using the first-pass technique (50 ms per frame × 600 frames) in a right anterior oblique position for best delineation of the right ventricle. After defining the right ventricular region of interest, 1–3 cardiac cycles were evaluated and the average of these cycles was used to estimate the RVEF with background correction. First-pass radionuclide angiography was performed with a MultiSPECT3 (Siemens Medical Systems, Iselin, NJ), and the RVEF was calculated on an ICON workstation (Siemens Medical Systems).
Statistical Analysis
Data are expressed as the mean ± 1 SD. Simple regression or logistic analysis was used to correlate the P index with the hemodynamic parameters and the RVEF. The effects of long-term vasodilator therapy on the P index and mPAP were analyzed by the Student t test. P < 0.05 was considered significant.
RESULTS
Quantification of Lung Perfusion Scans
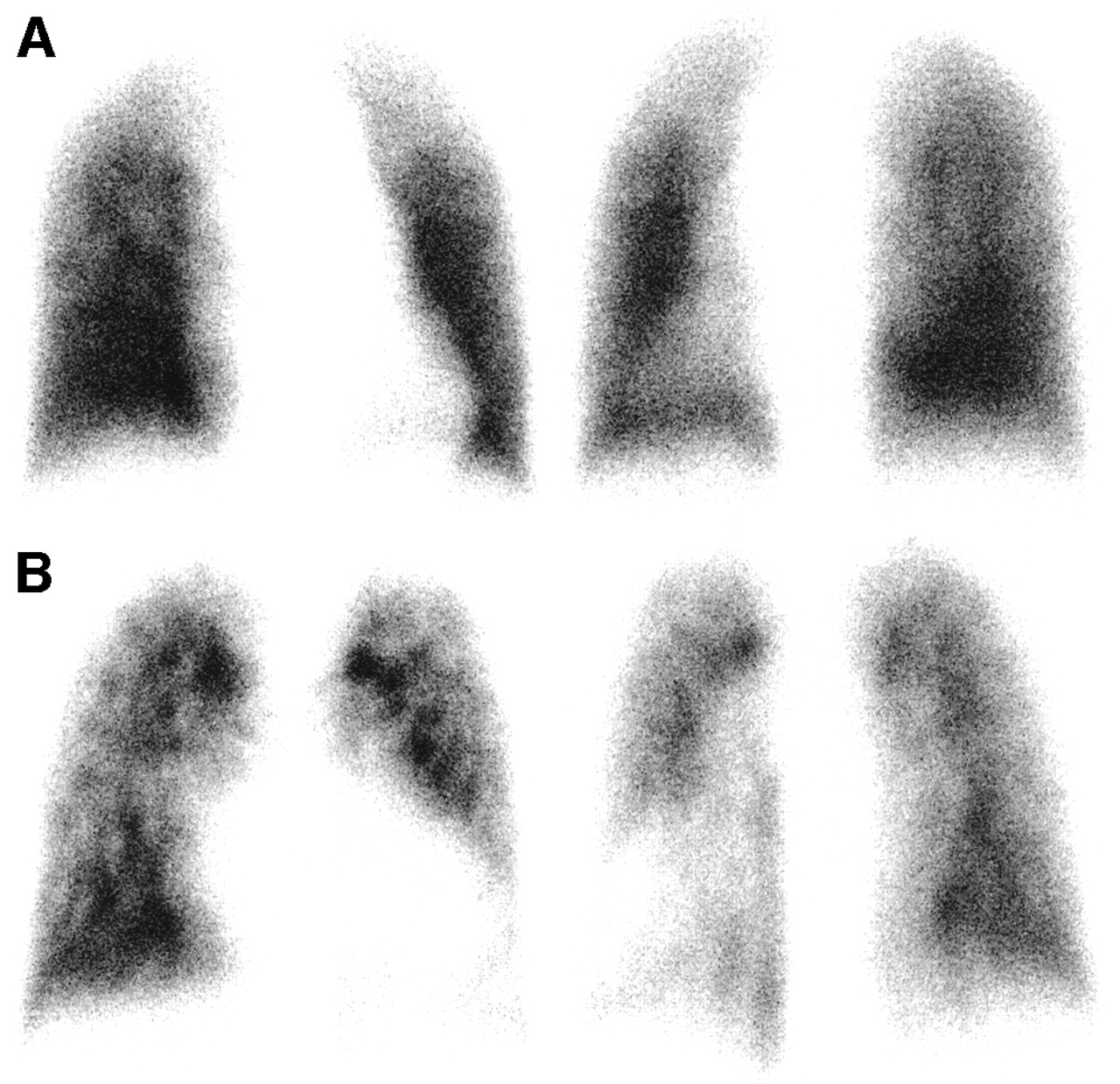
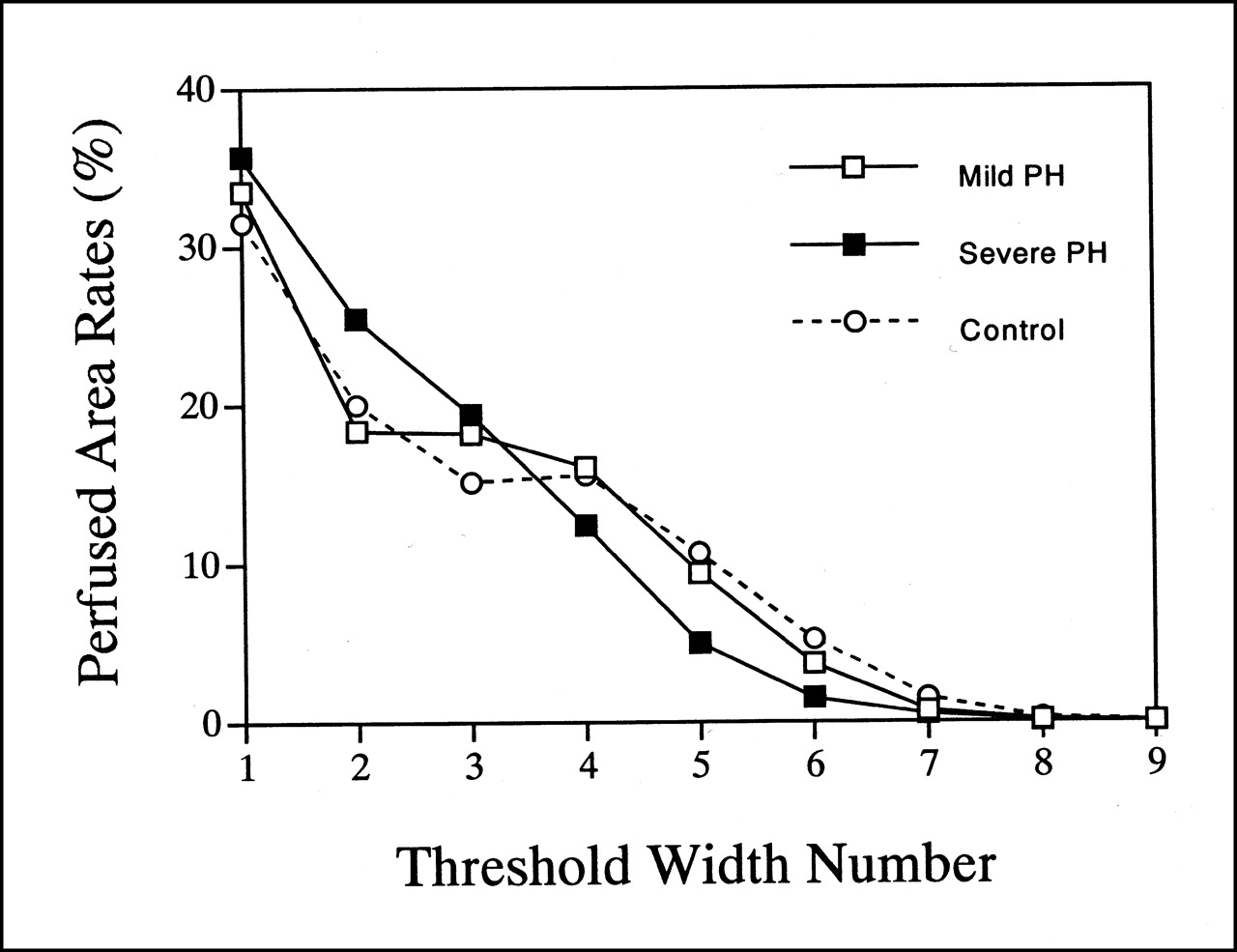
Thirty lung perfusion scans were obtained on 22 patients with PPH. None of the patients had significant segmental or subsegmental perfusion defects but they did have various degrees of diffuse patchy defects. Figure 2 presents representative examples of the lung perfusion scan in patients with mild and severe PPH. In a patient with mild PPH (mPAP = 31 mm Hg), a slightly patchy distribution of lung perfusion was depicted. In contrast, the mottled pattern of lung perfusion could be seen clearly in a patient with severe PPH (mPAP = 71 mm Hg). Figure 3 shows the PAR curves of the patients in Figure 2 and the mean PAR curve derived from the 12 control subjects. The PAR curve of mild PPH had a relatively small difference from the mean PAR curve of the 12 control subjects for each threshold width number. In contrast, a relatively large difference was found between the PAR curve of the patients with severe PPH and the mean PAR curve of the control subjects.

Representative anterior and posterior views of lung perfusion scan derived from patient with mild pulmonary hypertension (A) and from patient with severe pulmonary hypertension (B).

PAR curve derived from patients with mild and severe pulmonary hypertension (PH). Both cases are same as those in Figure 2. Control curve is averaged PAR curve of 12 control subjects.
P index of Lung Scan, Hemodynamic Variables, and Right Ventricular Function
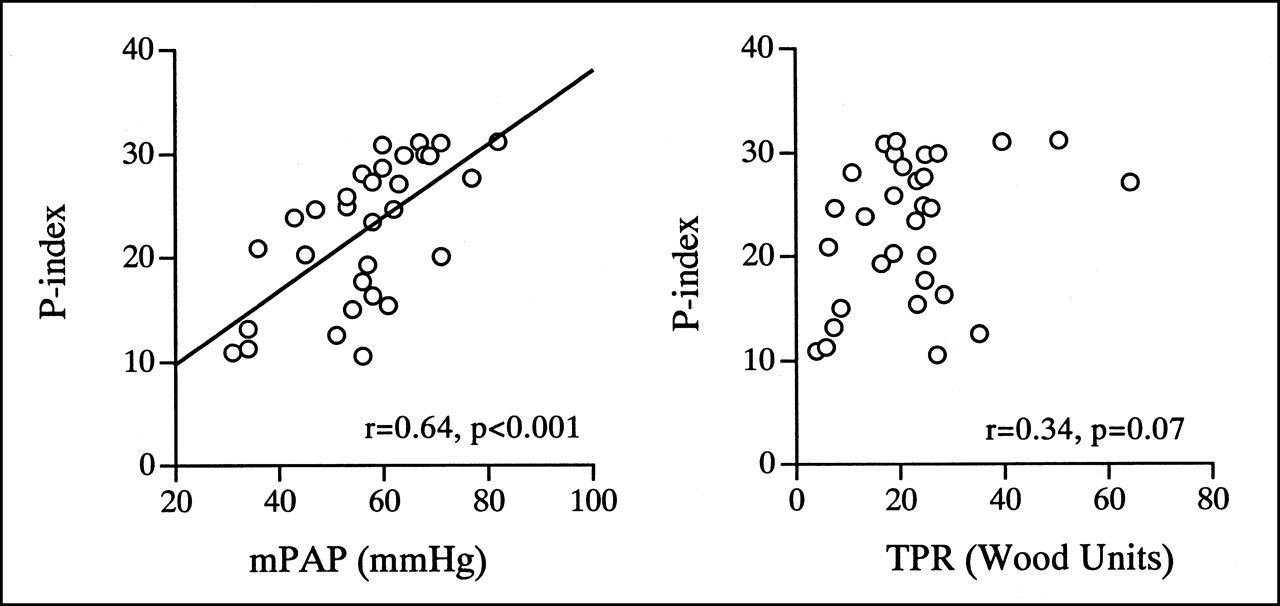
The relationship between the P index and hemodynamic studies is shown in Figure 4. The P index correlated significantly with the mPAP (r = 0.64; P < 0.001). On the other hand, no significant correlation was found between the P index and the TPR (r = 0.34; P = 0.07). To assess the influences of right ventricular afterload and lung perfusion inhomogeneity, the relationship between the P index and the RVEF was plotted in Figure 5. A significant inverse correlation was found between the P index and the RVEF (r = 0.51; P < 0.05).

Correlation between P index of lung perfusion scan and hemodynamic variables in patients with PPH.

Correlation between P index of lung perfusion scan and RVEF from first-pass radionuclide angiography of 16 patients.
Effects of Vasodilator Therapy
During long-term PGI2 therapy, the mean value of the mPAP in 7 patients decreased significantly from 66.0 ± 8.3 mm Hg to 57.3 ± 8.1 mm Hg (P < 0.05). Under these conditions, the mean P index of lung perfusion scans also decreased significantly from 26.1 ± 5.2 to 21.5 ± 7.4 (P < 0.05) (Fig. 6).
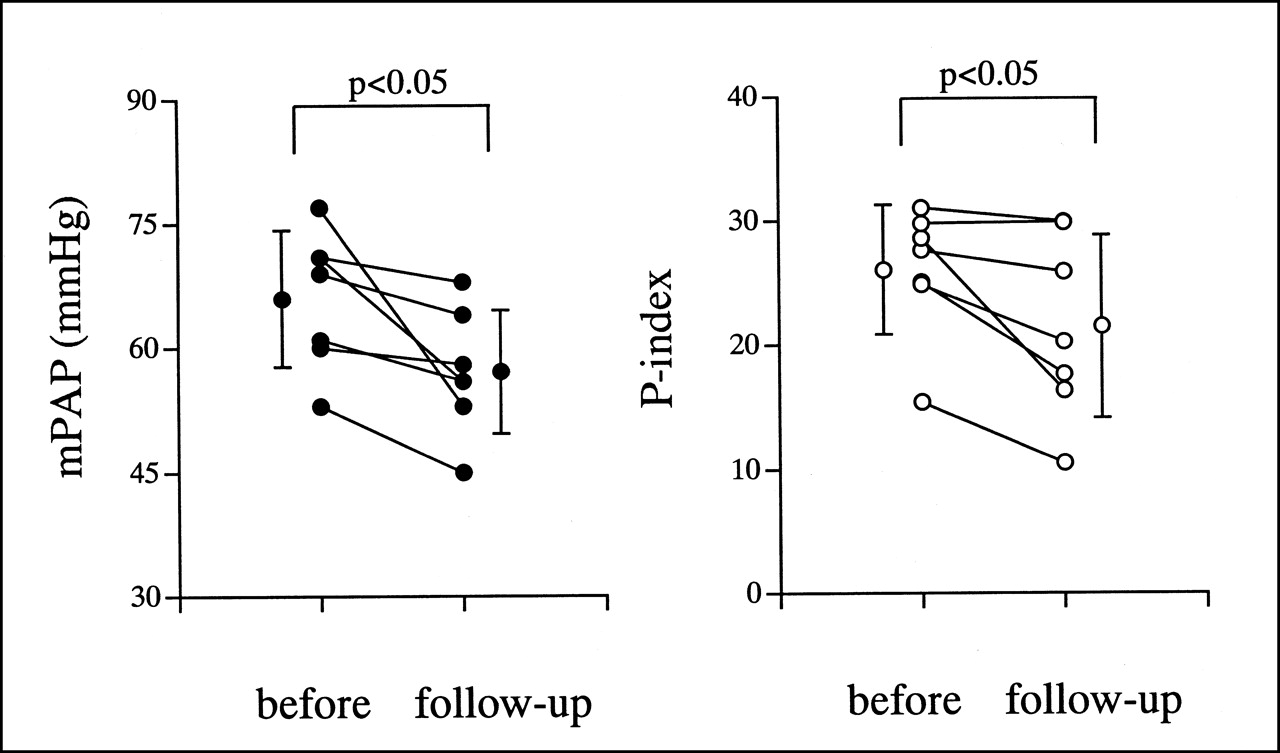
P index of lung perfusion scan and mPAP at baseline and during PGI2 therapy (follow-up) in 7 patients with PPH. SD is expressed by vertical bars beside each time grouping.
DISCUSSION
In this study, the heterogeneous distribution of lung perfusion scans in patients with PPH was analyzed quantitatively, and the P index correlated positively with the mPAP and the RVEF. We also found that the P index decreased during long-term vasodilator therapy. These results suggest that assessment of scintigraphic uniformity is useful for the evaluation of disease severity and can be used in supplementary diagnosis in addition to visual evaluation of patients with PPH.
The lung perfusion scan permits a better assessment of the integrity of the microcirculation than pulmonary angiography and also indicates the status of the entire pulmonary vasculature, as opposed to the limited regional evaluation possible with a lung biopsy. Despite this advantage of lung perfusion scans, their main role in patients with PPH is exclusively diagnosis, because there are no specific findings in PPH; scans can only permit correct differentiation of patients with PPH from patients with chronic thromboembolic pulmonary hypertension (11). However, diffuse perfusion abnormalities with normal ventilation can often be seen in PPH (3,4). The characteristic pattern of lung perfusion scans in PPH is a nonsegmental patchy defect, the so-called mottled pattern. This scintigraphic characteristic is well known, but no studies have explained this abnormality. To our knowledge, this study provides the first quantitative evaluation of lung perfusion scan heterogeneity in patients with PPH.
The diffuse heterogeneous distribution on perfusion scans in PPH is thought to be secondary to asymmetric proliferative or vasoconstrictive occlusion of the small pulmonary arteries, which can be shown pathologically (2). Thus, the degree of lung perfusion scan heterogeneity is assumed to have some relationship with the severity of the disease itself. In this study, the P index, an indicator of heterogeneous distribution, correlated significantly with the mPAP and the RVEF. Previous studies have shown that the mortality in PPH correlates with right ventricular hemodynamic variables such as the mPAP, CO, and mean right atrial pressure (12,13). It is also well known that the right ventricular systolic function, such as RVEF, decreases linearly in proportion to the increase in the mPAP (14). Thus, our findings indicate that the degree of mottled perfusion is associated with the clinical severity of PPH and is also useful in helping to make the underlying diagnosis and judge the extent of pulmonary hypertension. Although several noninvasive markers for the severity of PPH, such as neurohormones and echocardiographic parameters (10,15), have been proposed, quantitative analysis of lung perfusion scans may also provide a noninvasive indicator of pulmonary hypertension severity.
Circulating concentrations of PGI2, a potent vasodilating and antiproliferative mediator, are reduced in patients with PPH (16). Regardless of whether PGI2 deficiency causes or results from pulmonary vasculopathy, there is a rationale for replacement treatment. In fact, continuous intravenous PGI2 infusion has been shown to improve exercise tolerance and pulmonary hemodynamics in patients with PPH (17). An interesting aspect of PGI2 efficacy is that long-term decreases in pulmonary arterial pressure occur in some patients despite a lack of any acute vasodilator response, suggesting a beneficial remodeling effect on the pulmonary vasculature (7). In this study, the P index was improved significantly after PGI2 treatment associated with a reduction in the mPAP. This result suggests that lung perfusion scans can depict the improvement in the remodeling effect on the pulmonary vasculature. Although right heart catheterization is necessary for a definitive assessment of PPH, it could be useful to assess long-term PGI2 therapy in PPH in a noninvasive manner.
The quantitative method that we used is a simple and routinely available analysis, which can be performed using a public domain program on a personal computer system. Lung perfusion scans using the P index will become a useful technique for evaluating the status of various lung diseases, including PPH, and quantitative measurement of the effect of treatment.
This study has several limitations. First, we modified a previous method, which was developed to quantitate lung perfusion using SPECT (9). In this study, we did not evaluate lung perfusion SPECT in PPH. The average PAR curve of the control subjects in this study showed a slightly different pattern than that of the control subjects using SPECT in the original study (9). Some inherent differences in tracer distribution occur between planar images and SPECT. However, we believe that this method could apply to planar images because the principle of this quantitative method might be valid for 2-dimensional data (planar imaging) and volumetric data (SPECT).
Second, it is possible that lung perfusion scanning with 99mTc-MAA makes the pulmonary circulation worse in patients with PPH, because it has an additional embolic effect on the pulmonary vasculature with an already impaired pulmonary circulatory reserve. Using a standard 200,000- to 400,000-particle injection of a single dose of 99mTc-MAA, approximately 1 of 1,000 of the pulmonary capillaries is temporarily occluded (18). Thus, lung perfusion scans seem to be safe as long as the dose is within the standard amount. We used one third of the standard amount of 99mTc-MAA for patients with PPH and encountered no complications in any cases in this study.
CONCLUSION
The uniformity of lung perfusion scans in patients with PPH was well documented by our quantitative analysis. Quantitative analysis of irregular distribution on lung perfusion scans could provide useful information about the severity of disease and the effect of therapy.
Acknowledgments
The authors thank Dr. Osamu Mitomo (Department of Radiology, National Numata Hospital, Numata, Japan) for valuable advice and suggestions.
Footnotes
Received Sep. 18, 2001; revision accepted Feb. 4, 2002.
For correspondence or reprints contact: Kazuki Fukuchi, MD, Department of Radiology, National Cardiovascular Center, 5-7-1 Fujishiro-dai, Suita, Osaka, 565-8565, Japan.
E-mail: kfukuchi{at}hsp.ncvc.go.jp





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}