


Abstract
The accurate noninvasive diagnosis and functional evaluation of coronary artery disease is an important step in selecting the appropriate management strategy. Dobutamine stress myocardial perfusion imaging is an alternative to exercise in patients with limited exercise capacity. In many centers, the test is performed on patients who have a contraindication for vasodilator stress testing. Recent studies have shown hyperemia induced by the standard dobutamine-atropine stress test is not less than hyperemia induced by dipyridamole. The feasibility of the test is 90% and is often higher in patients without β-blocker therapy. The safety of the test has been well studied and was also demonstrated in specific patients groups, such as patients with left ventricular dysfunction, the elderly, and heart transplant recipients. The diagnostic accuracy has been demonstrated in patients with and without myocardial infarction and in specific groups such as those with hypertension, left ventricular hypertrophy, and heart transplant recipients and after revascularization. The technique has a high sensitivity for prediction of functional recovery in patients with myocardial dysfunction referred for revascularization. The presence and severity of myocardial perfusion abnormalities assessed by this method are powerful predictors of cardiac events, incremental to clinical data. This article describes the methodology, safety, feasibility, diagnostic accuracy, and prognostic value of dobutamine stress myocardial perfusion imaging in patients with known or suspected coronary artery disease, with additional considerations for the application of the test in specific patient groups.
Noninvasive diagnosis and functional evaluation of coronary artery disease (CAD) should be accomplished by a safe method with a high accuracy to guide the physician in planning the appropriate management of patients with known or suspected CAD (1–3). Exercise stress testing is the most widely used method for that purpose (3). The addition of myocardial perfusion imaging (MPI) in conjunction with exercise stress improves the diagnostic accuracy and provides prognostic information incremental to that obtained by clinical and exercise stress test parameters (1). However, many patients are unable to exercise as a result of certain conditions, such as degenerative joint disease, physical deconditioning, neurologic disorders, chronic obstructive airway disease, or peripheral vascular disease. In addition, a substantial proportion of patients can perform only submaximal exercise stress testing. The test is often inconclusive in these patients when they have no objective evidence of myocardial ischemia. In such patients, pharmacologic stress testing is an alternative (2). It is important to recognize that patients with limited exercise capacity generally represent a sicker population and have a higher mortality rate than patients who are able to exercise (2). Therefore, noninvasive evaluation of CAD in patients with limited exercise capacity should identify a larger proportion of patients at risk of death and cardiac events. Experience with pharmacologic stress MPI has been largely with vasodilators (adenosine or dipyridamole). Dobutamine-atropine stress testing represents a feasible alternative, particularly in patients who have contraindications for vasodilators, such as reactive airway disease or high-grade atrioventricular nodal block (4–6). Earlier studies have shown that the grade of hyperemia induced by dobutamine is less than that induced by vasodilators such as dipyridamole and adenosine (7,8). However, recent studies have shown that with standard dobutamine-atropine stress testing, the extent of hyperemia is not less than that observed with dipyridamole (9). MPI has been approved recently for use with dobutamine stress in the United States.
The objective of this article is to discuss the methodology, safety, feasibility, and clinical applications of dobutamine stress MPI in the diagnosis and prognostic stratification of CAD.
METHODOLOGY OF DOBUTAMINE STRESS MPI
Background and Pharmacokinetics
Dobutamine is a synthetic catecholamine with a potent β1-receptor and mild α1- and β2-receptor agonist activity (10,11). After intravenous administration, the drug undergoes extensive rapid metabolization in the liver, resulting in a short half-life of approximately 2 min. Low-dose dobutamine (2.5–10 μg/kg/min) is used therapeutically in patients with heart failure and severe impairment of systolic function because of the marked inotropic effects mediated by both β1- and α1- receptor activity. This also represents the basic principle for the use of this agent in the evaluation of myocardial viability by eliciting contractile response of dysfunctional myocardium. Higher doses of dobutamine induce a progressive increase of heart rate mediated by α1-receptor stimulation. The result is an increase in the cardiac output as a result of both positive inotropic and chronotropic response. The drug also causes reduction of systemic vascular resistance mediated by β2-receptor stimulation. The net result is usually a mild increase of systolic blood pressure, because the increase of cardiac output is partially counteracted by the reduction of systemic vascular resistance.
The increase in heart rate and myocardial contractility results in an increase in myocardial oxygen demand, with subsequent hyperemia. This causes a secondary dilation of the coronary arteries and an increase in blood flow in normal coronary arteries (12). A minor direct vasodilator effect on coronary vessels is also achieved by dobutamine. In myocardial regions supplied by a coronary artery with significant stenosis, the increase in oxygen demand cannot be met by an adequate increase in blood flow (12). A steal phenomenon also occurs, in which blood flow is horizontally diverted from stenotic to normal arteries and vertically from the subendocardial to subepicardial layer as the former is subjected to the highest wall stress. Therefore, induction of flow heterogeneity between myocardial regions subtended by normal coronary arteries and those subtended by stenotic coronary arteries represents the mechanism for diagnosis of CAD by dobutamine MPI (12).
For proper evaluation of flow heterogeneity, the radionuclide tracer must be distributed in the myocardium in proportion to blood flow over the range of flows induced by dobutamine. Earlier studies (7,8) showed that dobutamine-induced myocardial 201Tl uptake expressed as a percentage of whole-body uptake is intermediate between exercise and direct vasodilator stress and that heart-to-background ratios of 201Tl uptake are similar to direct vasodilator stress (but less than exercise stress). In the study by Fung et al. (12) in an open-chest dog model, a critical stenosis of the left circumflex coronary artery (LCX) was produced with total ablation of hyperemic response to a 15-s period of complete occlusion. Eight dogs received 15 μg/kg/min dobutamine intravenously for 10 min, and 9 dogs received 0.14 mg/kg/min dipyridamole intravenously for 4 min. Subendocardial blood flow to the left circumflex area was unchanged after both dobutamine and dipyridamole when compared with baseline blood flow. However, subendocardial blood flow increased markedly after dipyridamole in the control area. Regional subendocardial blood flow ratio was higher after dipyridamole than after dobutamine. It was concluded that dipyridamole induces more flow heterogeneity in regional perfusion than dobutamine. In contrast to these findings, Tadamura et al. (9) compared the absolute myocardial blood flow after intravenous dipyridamole infusion with that during dobutamine-atropine administration in healthy male volunteers. Myocardial blood flow was measured with PET and 15O-labeled water in 20 healthy young men at baseline, after dipyridamole infusion (0.56 mg/kg over 4 min), and during dobutamine (40 μg/kg/min) and atropine (0.25–1.0 mg) infusion. The myocardial blood flow was significantly increased during dipyridamole infusion and during dobutamine-atropine stress compared with that at rest. Dobutamine-atropine infusion produced greater myocardial blood flow compared with dipyridamole, whereas coronary vascular resistance did not differ significantly after dipyridamole administration and during dobutamine-atropine infusion. It was concluded that near maximal coronary vasodilatation caused by dipyridamole is attainable using dobutamine and atropine in young, healthy volunteers. Dobutamine in conjunction with atropine is no less effective than dipyridamole in producing myocardial hyperemia (9).
Dobutamine Stress Test
It is usually recommended that β-blockers be withheld for at least 48 h before the test, because β-blockers reduce the inotropic and chronotropic effects of dobutamine and, therefore, may reduce the sensitivity of the technique. Dobutamine is infused through the antecubital vein starting at a dose of 10 μg/kg/min (3-min stages), increasing by 10 μg/kg/min every 3 min to a maximum of 40–50 μg/kg/min. In some patients, the target heart rate (85% of the maximal heart rate predicted for age) cannot be reached at the maximal dobutamine dose, particularly in patients receiving β-blockers (4,13,14). In these patients, atropine should be administered at incremental doses up to 2 mg to increase the heart rate by virtue of vagolytic action, and dobutamine infusion should be continued. Heart rhythm should be monitored throughout the stress test and recovery. Cough blood pressure measurements and electrocardiograph recordings should be performed every 3 min. Criteria for termination of the test are severe chest pain, ST-segment depression > 2 mm, ST-segment elevation > 1 mm in patients without previous myocardial infarction (MI), significant ventricular or supraventricular arrhythmia, hypertension (blood pressure ≥ 240/120 mm Hg), systolic blood pressure drop of >40 mm Hg, and any intolerable side effect regarded as being the result of dobutamine (4–6). Side effects of dobutamine can be reverted by metoprolol (1–5 mg) or esmolol intravenously, if chest pain or arrhythmias do not resolve after termination of dobutamine infusion. Nitroglycerine also can be used to treat chest pain, but it does not have the specific antidote properties of β-blockers. Nitrates might be reserved for patients in whom β-blockers are contraindicated. Contraindications to dobutamine stress testing include acute coronary syndrome, severe aortic stenosis, hypertrophic obstructive cardiomyopathy, uncontrolled hypertension, uncontrolled atrial fibrillation, uncontrolled heart failure, and known severe ventricular arrhythmias. Atropine is contraindicated in patients with narrow-angle glaucoma, myasthenia gravis, obstructive uropathy, or obstructive gastrointestinal disorders.
Radionuclide Imaging
Radioactive isotopes that have been studied with dobutamine include 201Tl, 99mTc-sestamibi, and 99mTc-tetrofosmin. The isotope should be injected 1 min before termination of the test (55.5–111 MBq 201Tl- or 370–740 MBq 99mTc-labeled agents; sestamibi and tetrofosmin). If 201Tl is used, stress images should be acquired immediately after the test, because this tracer exhibits significant redistribution. Redistribution images are acquired 4 h after the stress study (4). Reinjection of thallium and acquisition of reinjection images also were shown to enhance detection of reversible perfusion abnormalities in segments with fixed defects on redistribution images. This protocol, however, requires 3 sets of images and may be tedious (15). An alternative is to acquire images of stress and reinjection without acquiring redistribution images (16,17). Although some reversible defects may be missed with this protocol, a study of dobutamine stress thallium reinjection showed that this method does not significantly underestimate reversible perfusion abnormalities with dobutamine as compared with the protocol of stress, redistribution, reinjection (17). To minimize the interfering effect of hepatobiliary uptake, stress images are acquired 1 h after the test if 99mTc-labeled agents were used. These tracers do not exhibit significant redistribution, and, therefore, myocardial uptake after 1 h is almost representative of the uptake at maximal dobutamine stress, when the tracer was injected. Rest images require injection of a similar dose of the tracer. To facilitate the interpretation and comparison of cardiac tomographic images, a standardized nomenclature and display of images is recommended by the Society of Nuclear Medicine (18). A positive test is defined as a completely or partially reversible perfusion defect. In patients without a history of MI, the finding of a fixed defect may represent undiagnosed MI or myocardial hibernation with severe impairment of resting perfusion (19). A fixed defect is often considered diagnostic of significant CAD in these patients. In patients with previous MI, a fixed perfusion abnormality may persist after recanalization of the infarct-related artery or after revascularization. A fixed defect in this scenario, therefore, is not highly specific for significant stenosis of the related coronary artery (20). The severity of myocardial perfusion abnormalities can be estimated by using a sum of perfusion scores in all myocardial segments. This can be performed semiquantitatively by visual analysis or quantitatively by circumferential profile analysis (4).
Electrocardiograph (ECG) Changes.
ECG changes lack sensitivity for the diagnosis of CAD during dobutamine stress testing in contrast to the moderate sensitivity with exercise stress testing (21–23). The low sensitivity of ECG changes with dobutamine may be related to the lower rate-pressure product with dobutamine compared with exercise and the tendency to select patients with resting ECG abnormalities for pharmacologic stress tests (2,3). The specificity (and, thus, positive predictive value) of dobutamine stress-induced ST-segment depression, however, seems excellent, ranging from 88% to 93% (21–23), but the low sensitivity warrants performing the test in conjunction with a more sensitive imaging technique such as MPI. ST-segment elevation is associated with severe myocardial perfusion abnormalities, which are often reversible in patients without previous MI. Although often associated with high-grade stenosis of the related artery, ST-segment elevation in patients with previous infarction should not be used as a criterion for termination of the test, because ST-segment elevation in these circumstances is not consistently associated with a reversible perfusion abnormality (24). T-wave normalization during dobutamine stress testing is associated with a higher prevalence of reversible perfusion abnormalities in patients with non-Q-wave MI (25).
Heart Rate Response.
In the majority of patients, incremental doses of dobutamine induce a progressive increase in heart rate, which is more prominent at higher dobutamine doses (4–6). Some patients have a plateau of heart rate response, particularly those receiving β-blockers and occasionally younger patients with high vagal tone (26). The increase of myocardial contractility obtained at the low dose may initiate reflex vagal activation, which tends to counteract and even reverse the chronotropic response of the heart to dobutamine (27). Another pattern of heart rate response is the sinus node deceleration, defined as an initial increase and subsequent decrease in heart rate with progressive dobutamine infusion (28,29). Although this pattern may be associated with ischemia, it has a low specificity and cannot be considered to be a reliable sign of ischemia in the absence of other markers (26,28,29). Atropine often induces a significant increase in heart rate in these patients and, therefore, enhances the feasibility of the test. In patients with a flat heart rate response to dobutamine at lower doses (20 μg/kg/min), earlier administration of atropine may reduce the duration of the stress test.
Hypotension.
In most individuals, an increase in cardiac output compensates for the reduction of systemic vascular resistance induced by dobutamine. Unlike the situation in exercise stress testing, the relationship between hypotension and functional abnormalities during dobutamine stress testing is controversial, reflecting individual variations in peripheral vasodilator response to dobutamine (30–33). Predictors of hypotension are high baseline systolic blood pressure, advanced age, high left ventricular ejection fraction, impairment of systolic reserve, and dynamic left ventricular obstruction (30–33). However, a correlation was found between dobutamine-induced hypotension and extent of myocardial dysfunction in patients with previous MI (32). An increase of systolic blood pressure ≥ 30 mm Hg during dobutamine stress testing is associated with less fixed perfusion defects and a tendency toward a lower annual event rate (33).
Safety and Feasibility of Dobutamine Stress MPI
The test is considered feasible if the patient achieved 85% of the maximal heart rate predicted for age (220 minus age, in years). In patients who fail to achieve the target heart rate, the test is still considered feasible, if an ischemic endpoint is reached (angina, ST-segment depression, or reversible perfusion abnormality) (4,5).
Approximately 10% of dobutamine stress myocardial perfusion studies are nondiagnostic (4–6). A large proportion of these nondiagnostic tests are encountered in patients receiving β-blockers and who cannot achieve the target heart rate. Other causes are the occurrence of limiting side effects that require termination of the dobutamine stress test. In our experience, failure to achieve the target heart rate is rare in patients without β-blocker who can tolerate the maximal dobutamine-atropine dose.
Noncardiac side effects (nausea, headache, chills, urgency, and anxiety) are not uncommon but are usually well tolerated and rarely require termination of the dobutamine stress test. The most common cardiovascular side effects are angina, hypotension, and cardiac arrhythmias. Dobutamine stress-induced hypotension (defined as a 20-mm Hg decrease in systolic blood pressure) occurs in approximately 15% of patients (4–6). This is often well tolerated. Severe, symptomatic hypotension necessitating test termination, however, occurs only rarely. In our laboratory, we do not terminate the test unless hypotension is severe (systolic blood pressure drop of >40 mm Hg) or symptomatic. Prolonged angina can be treated with an intravenous β-blocker (34). In patients with reversible perfusion abnormalities and CAD, the occurrence of angina is not related to the severity of reversible perfusion abnormalities (35).
Cardiac Arrhythmias
Premature atrial or ventricular contractions occur commonly during dobutamine stress tests. Supraventricular and ventricular tachycardias each occur in approximately 4% of patients (4–6). Supraventricular tachycardia can be controlled with the injection of a β-blocker or, in patients with obstructive airway disease, verapamil. Digoxin is not the primary choice for the acute management of atrial fibrillation because of a delayed onset of action. Ventricular tachycardias are usually nonsustained. Patients at high risk of dobutamine-induced arrhythmias are those with a history of arrhythmias, hypokalemia as a result of previous diuretic use (in addition to dobutamine-induced reduction in plasma potassium concentrations) (4,36–38), and left ventricular dysfunction or extensive fixed perfusion defects. Sustained ventricular tachycardias may be managed with an injection of a β-blocker or lidocaine. In the case of hemodynamic instability, electrical cardioversion is indicated. In 5 major reports on the safety of dobutamine stress MPI (4–6,39,40) in a total of 3,578 patients, there were no reports of death, MI, or ventricular fibrillation. However, these complications have occurred sporadically in patients undergoing dobutamine stress echocardiography (41,42). Atropine intoxication is a central anticholinergic syndrome causing confusion or sedation, treated by 0.5–2.0 mg physostigmine intravenously. Although this syndrome occurs after high doses of atropine (5 mg), it has been reported during dobutamine stress echocardiography in a few patients receiving 1 mg atropine (41,42).
Does Ischemia Monitoring Contribute to the Safety of the Test?
The diagnosis of myocardial ischemia with MPI cannot be established during the test unless ST-segment depression occurs, because the scintigraphic diagnosis requires interpretation of both stress and rest images. This puts techniques capable of monitoring ischemia, such as echocardiography, at a theoretic advantage with regard to safety. However, no data indicate that termination of dobutamine stress testing with the onset of wall motion abnormalities contributes to the safety of the test. In most case reports describing dobutamine-induced complications such as cardiac arrest or nonfatal MI, such events were not heralded by prior ischemia on the stress echocardiogram. Continuation of the test in patients without other side effects allows detection of ischemia in multiple vascular distributions, which has an important diagnostic and prognostic implication (1).
Safety in Specific Patient Groups
The Elderly.
Cardiovascular disease is the leading cause of morbidity and mortality in the elderly. Recent advances in revascularization procedures have led to an increase in the number of elderly patients undergoing coronary artery bypass grafting (CABG) or coronary angioplasty, with clear benefits in short- and long-term survival. A larger proportion of the elderly population is unable to perform exercise stress testing. Elderly patients are at a higher risk for developing spontaneous and exercise-induced arrhythmias and for impairment of compensatory mechanisms for hypotension. A recent study demonstrated that dobutamine myocardial perfusion scintigraphy is a highly feasible method for the noninvasive evaluation of CAD in elderly patients (>65 y old). Ninety-five percent could achieve the endpoint of target heart rate or an ischemic endpoint (40). The prevalence of hypotension during the test was significantly higher in the elderly than in younger patients. However, most of the episodes of hypotension were asymptomatic, and the test was terminated because of hypotension in only 2% of patients. During the test, elderly patients had a higher prevalence than younger patients of supraventricular tachycardia (7% and 1%, respectively), atrial fibrillation (3% and 0.4%, respectively), and ventricular tachycardia (5% and 2%, respectively). However, the tachycardia was terminated spontaneously, by termination of the dobutamine infusion or by metoprolol administration. No MI or death occurred (40).
Heart Transplant Recipients.
Cardiac allograft vasculopathy remains one of the major factors that interfere with long-term survival in heart transplant recipients (43). The disease is often silent as a result of autonomic denervation, and the initial presentation may be sudden death. Exercise performance remains impaired in heart transplant recipients, compared with healthy subjects. Dobutamine myocardial perfusion scintigraphy is a feasible alternative to exercise in these patients. A recent study showed that dobutamine stress MPI is a safe and feasible method for evaluation of cardiac allograft vasculopathy in heart transplant recipients (39). The prevalence of arrhythmias and minor complications of dobutamine stress testing were lower in heart transplant recipients than in control patients. There was an independent association between heart transplantation and reduced risk of arrhythmias and minor side effects of dobutamine stress testing. These findings indicate that cardiac sensory and autonomic nerve function plays a major role in the induction of these complications during the test.
DIAGNOSIS OF CAD
Assessments of the accuracy of dobutamine stress MPI for the diagnosis of CAD varied among previous studies (44–68). Many variables may underlie these differences and can be summarized as follows: (a) Study patients: number of patients receiving β-blocker therapy (sensitivity), presence of previous MI (high sensitivity and low specificity of a fixed defect), prevalence of CAD in the study population (predictive value), and extent and severity of CAD (sensitivity is higher with multivessel disease and with more severe obstructive lesions). (b) Methodology: maximal dose of dobutamine, use of atropine, planar versus SPECT imaging, and possibly type of radionuclide tracer. (c) Verification bias: patients with a positive test are more likely to be referred for coronary angiography than patients with a negative test. This tends to increase sensitivity (including more true positives and excluding more false negatives) and reduce specificity (including more false positives and excluding more true negatives). For these reasons, the normalcy ratio (percentage of individuals with low pretest probability of CAD who had a normal study) is considered a better indicator of specificity than angiographically derived data. (d) Definition of an abnormal perfusion study: In general, a reversible perfusion abnormality is the hallmark of a positive stress myocardial perfusion study. Many studies consider a fixed perfusion abnormality diagnostic of a positive test, particularly in patients without previous MI. (e) Definition of significant CAD (50% vs. 70% stenosis) and possibly the accuracy of the method with which the severity of CAD was determined (visual vs. quantitative analysis).
The overall (weighted mean) sensitivity, specificity, and accuracy of dobutamine stress MPI in a total of 1,208 patients among previous studies were 85% (95% confidence interval [CI], 83–90), 72% (95% CI, 70–77), and 83% (95% CI, 80–87), respectively (21,22,44–60) (Fig. 1).
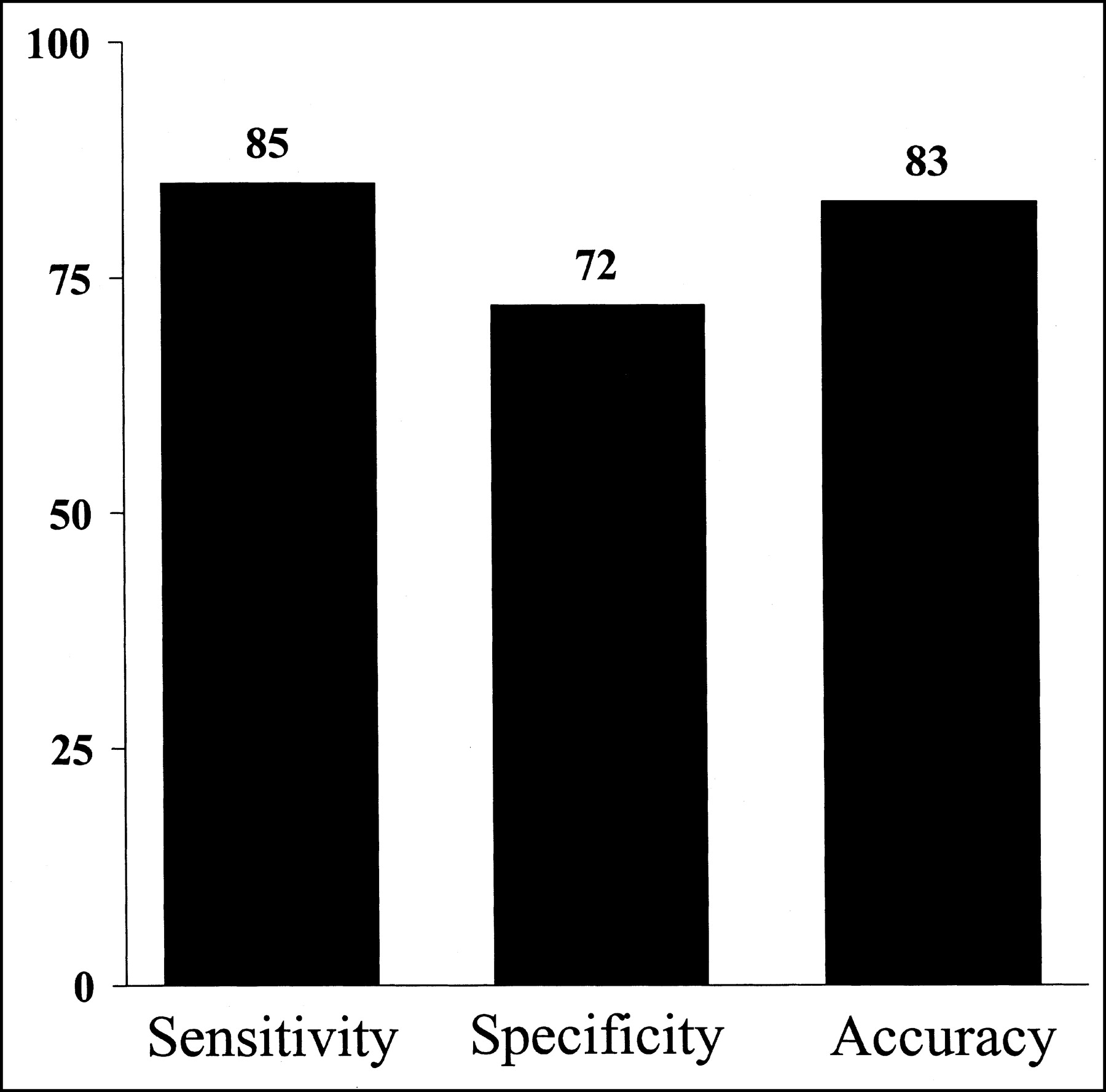
Sensitivity, specificity, and accuracy of dobutamine stress MPI for diagnosis of CAD. Results represent pooled data from 13 studies in 1,208 patients.
The effect of the number of diseased coronary arteries was assessed in 11 studies (13,44–46,49,50,54,60,62,65,66) for a total of 435 patients with CAD. Mean sensitivity was 80% for single-vessel disease, 92% for double-vessel disease, and 97% for triple-vessel disease (Fig. 2).
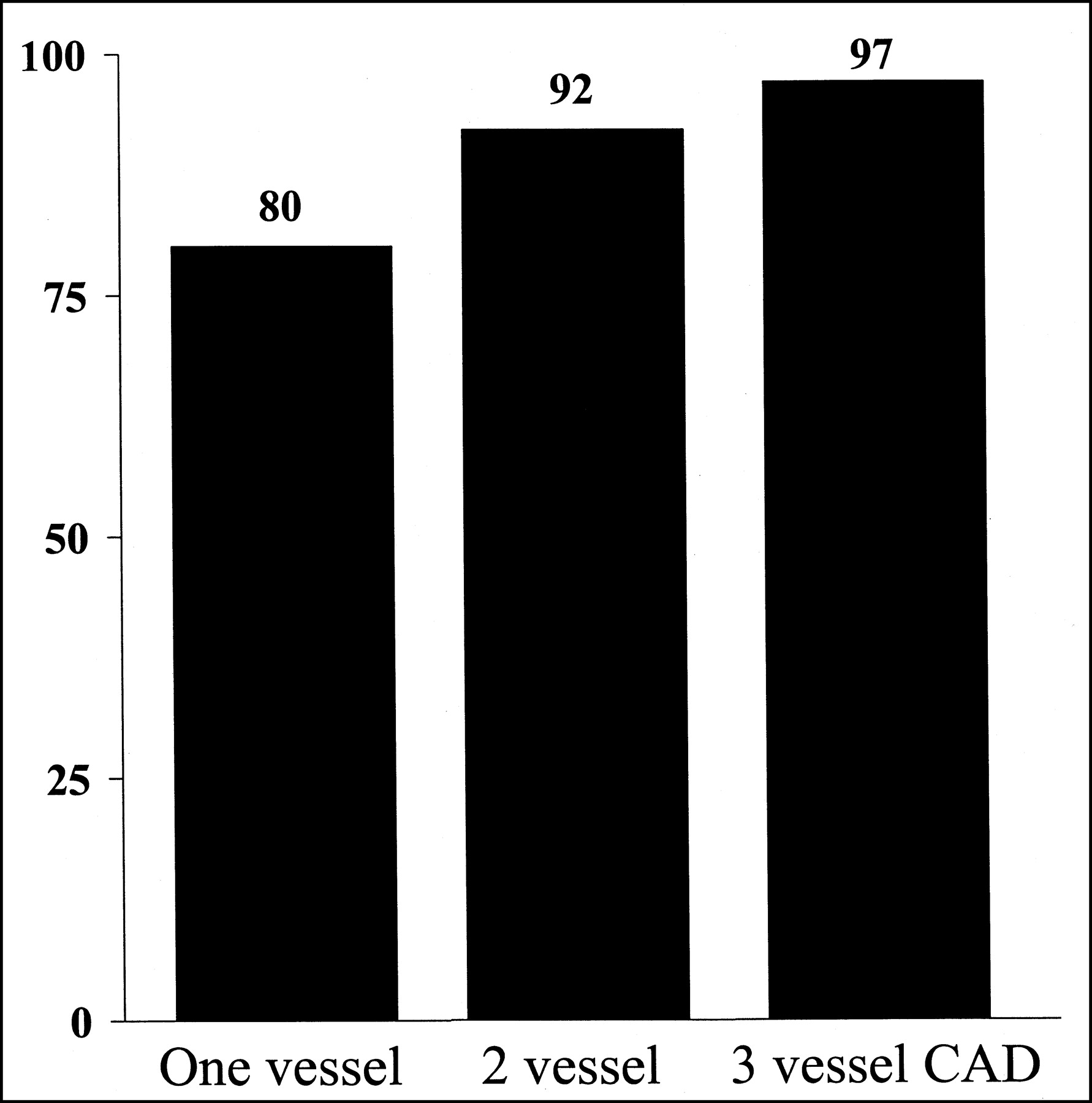
Sensitivity of dobutamine stress MPI according to extent of CAD. Results represent pooled data from 11 studies in 535 patients with CAD.
Localization of Stenotic Coronary Arteries
One of the major advantages of MPI is the ability to identify the diseased coronary artery by detecting abnormalities in the corresponding myocardial territories. SPECT imaging provides a unique and accurate method for tomographic localization of perfusion abnormalities. The anterior, apical, septal, and anteroseptal walls are assigned to the left anterior descending coronary artery (LAD). The posterior and lateral walls are assigned to the LCX. The inferior and basal septal segments are assigned to the right coronary artery (RCA). The apical lateral segment is considered an overlap segment between the LAD and the LCX. The apical inferior segment is considered an overlap segment between the LAD and the RCA. Overlap segments are assigned to the regions with concomitant abnormalities.
The sensitivity of dobutamine MPI among previous studies is 68% for the LAD, 50% for the LCX, and 88% for the RCA (13,44,46,49,50,54,60,65,66). Corresponding specificities were 90%, 94%, and 81%, respectively. Specificity for detection of right CAD was lower than that for left anterior descending CAD (P < 0.02) and left circumflex CAD (P < 0.0001). The lower specificity in the RCA region may be explained by false-positive results related to diaphragmatic attenuation of the inferior wall. Sensitivity for detection of left circumflex CAD was lower than that for left anterior descending CAD (P < 0.005) and right CAD (P < 0.0001). The lower sensitivity for detection of disease in the LCX may be related to variation in coronary anatomy, with a small circumflex territory in some patients and the potential vascular overlap in the posteroinferior wall with the RCA.
Identification of Extent of CAD
The extent of CAD can be predicted by observing the number of vascular regions with perfusion abnormalities. The diagnosis of multivessel CAD has important therapeutic and prognostic implications, because these patients are at highest risk of cardiac events and represent the group in which invasive studies with subsequent revascularization are likely to improve outcome.
Studies have shown that the diagnosis of multivessel CAD on the basis of perfusion abnormalities in ≥2 vascular regions can be accomplished with a high specificity (13,46,50,60,65,66) (range, 89%–94%) and a modest sensitivity (range, 44%–89%). Several factors may contribute to the underestimation of the extent of multivessel CAD: inadequate stress protocols, premature termination of stress because of the development of limiting side effects or angina, presence of collateral circulation, and improper assignment of myocardial perfusion regions to coronary arteries, particularly in regions of vascular overlap, such as the apex, posteroinferior wall, and posterior septum.
Comparison with Dobutamine Stress Echocardiography
Myocardial ischemia is manifested as mechanical dysfunction, which can be detected by echocardiography. Myocardial perfusion abnormalities occur earlier than wall motion abnormalities in the ischemic cascade (69,70). Therefore, dobutamine MPI is more sensitive than echocardiography at lower stress levels. The absence of transient wall motion abnormalities in patients who demonstrate reversible perfusion abnormalities with dobutamine stress should not be interpreted as a sign of less severe ischemia, because quantitative analysis shows that these patients have an extent of hypoperfusion similar to that of patients with concomitant wall motion abnormalities (70).
The advantages of dobutamine stress MPI over echocardiography include higher sensitivity, less subjective interpretation of images, availability of quantitative methods, and feasibility in patients with poor echocardiographic windows. The advantages of echocardiography include wider availability at lower cost, obtaining the rest and stress studies in the same setting over a shorter time, higher specificity, and the ability to monitor myocardial ischemia. However, interpretation of images requires considerable experience and is subjective. In 30% of the studies, 1 or more of the 16 myocardial segments used for echocardiographic interpretation cannot be visualized.
In 12 studies (22,46–50,52,54,56,59,65,66) comparing dobutamine stress MPI with echocardiography in the same 593 patients, sensitivities were 86% and 80%, respectively (P < 0.05); specificities were 73% and 86%, respectively (P < 0.005); and accuracies were 82% and 82%, respectively (Fig. 3).
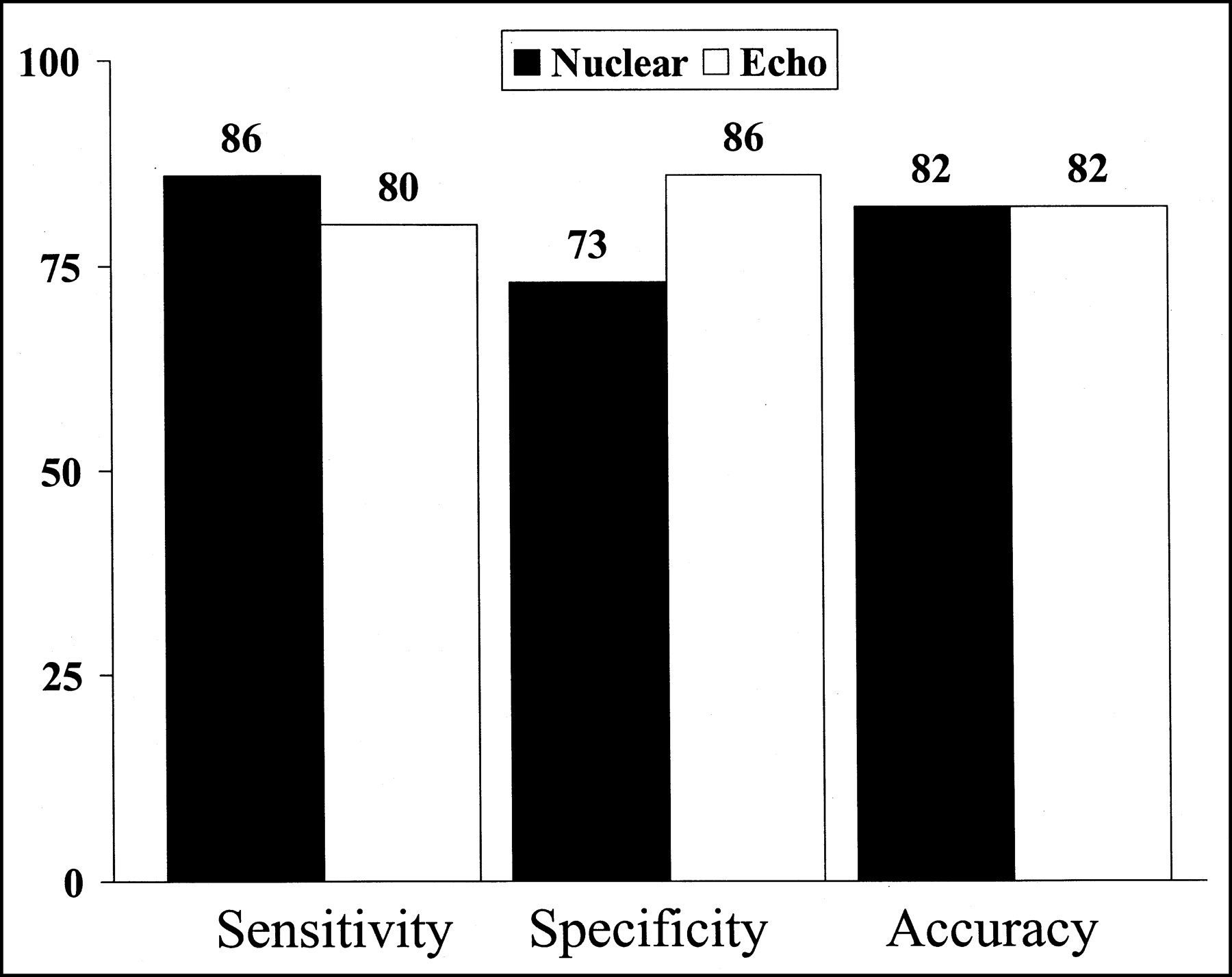
Comparison of accuracy of dobutamine stress MPI and simultaneous echocardiography for diagnosis of CAD. Results represent pooled data from 12 studies in 593 patients.
In patients with single-vessel disease, the use of 99mTc-labeled agents provides the advantages of improved imaging quality, increased consistency of image analysis, and a larger injectable dose because of the shorter half-life than 201Tl (1). However, recent experimental studies demonstrated that 99mTc-sestamibi underestimates flow heterogeneity induced by dobutamine, because its uptake plateaus at a lower flow rate than that of vasodilator agents (71). In addition, dobutamine may interfere with sestamibi uptake in the normally perfused myocardium, leading to further underestimation of flow heterogeneity (72). The implications of these experimental studies were that sestamibi scintigraphy might suffer limited sensitivity in patients with single-vessel CAD (72). Echocardiographic imaging during dobutamine infusion was proposed to overcome this potential limitation. However, a recent study from our laboratory showed that both echocardiography and sestamibi have a similar modest sensitivity (56%) for the diagnosis of single-vessel CAD in conjunction with dobutamine-atropine stress testing (62). The mean number of ischemic segments was not different in the 2 techniques. Despite the modest sensitivity of sestamibi, echocardiography did not provide an advantage in the overall or regional diagnosis of CAD in these patients. There was no improvement of accuracy by the synergetic use of both techniques for the diagnosis of single-vessel CAD compared with the accuracy of either technique alone. The prevalence of flow malperfusion in myocardial regions in the distribution of a diseased LCX or RCA was significantly lower compared with LAD disease (40% vs. 75%). This can be explained by the larger myocardial mass in the LAD region, which may facilitate the detection of flow heterogeneity compared with the smaller myocardial mass supplied by the LCX or the RCA.
Comparison with Vasodilator Perfusion Scintigraphy
The accuracy of MPI in conjunction with dobutamine was compared with vasodilator agents in 2 studies including a total of 157 patients (48,56). Sensitivities of MPI and dobutamine were 84% and 90%, respectively; specificities were 77% and 78%, respectively; and accuracies were 81% and 85%, respectively (Fig. 4). Earlier experience suggested the use of vasodilators as the agent of choice for MPI in patients with limited exercise capacity, unless contraindicated. However, recent studies have shown that dobutamine is no less effective than vasodilators in inducing flow hyperemia (9). There is no clear evidence to indicate superiority of direct vasodilator over dobutamine stress MPI in terms of diagnostic or prognostic accuracy. The cost of vasodilators, particularly adenosine, is higher than dobutamine. This, however, represents a small proportion of the total cost of the radionuclide study. Side effects of dobutamine and vasodilator perfusion agents are shown in Table 1 (14–16,73,74).
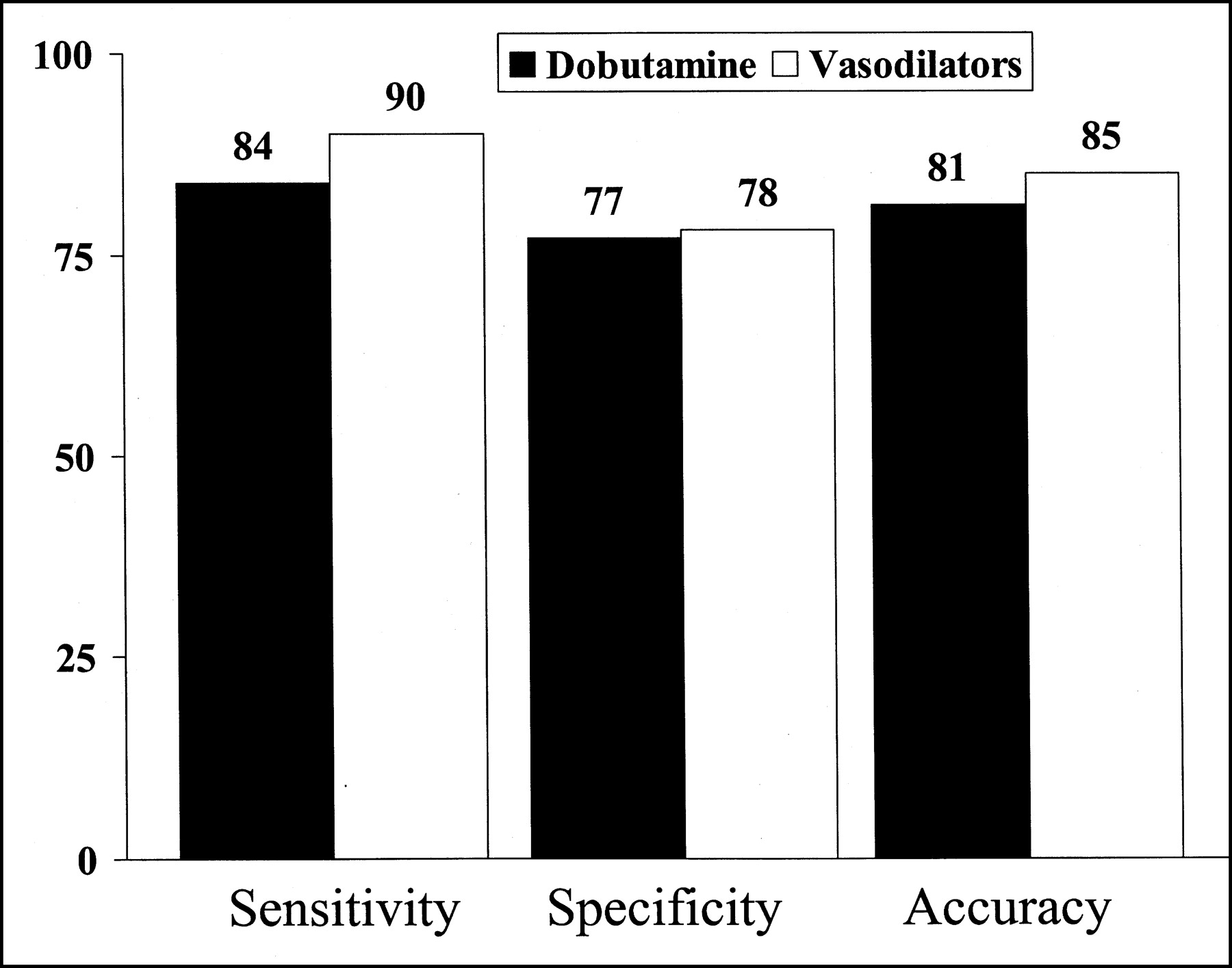
Comparison of accuracy of dobutamine and vasodilator stress MPI for diagnosis of CAD. Results represent pooled data from 2 studies in 157 patients.
Side Effects and Complications of Dobutamine, Dipyridamole, and Adenosine Stress Myocardial Perfusion Imaging
Gated SPECT
Technetium-labeled myocardial perfusion tracers allow simultaneous assessment of myocardial perfusion and left ventricular function by ECG-gated SPECT. This procedure has the potential to provide comprehensive information for evaluation of patients with ischemic heart disease, can enhance the sensitivity of dobutamine MPI, and improves identification of myocardial viability in hypokinetic segments (75,76).
Special Subgroups
Patients with Hypertension.
CAD is a major cause of morbidity and mortality in patients with systemic arterial hypertension. Exercise ECG has a limited specificity in hypertensive patients. Abnormalities of myocardial perfusion were reported in hypertensive patients with or without left ventricular hypertrophy in the absence of significant epicardial CAD (77). The occurrence of myocardial ischemia in these patients has been attributed to microvascular CAD, impaired vasodilator reserve, increased myocardial oxygen demand as a result of left ventricular hypertrophy, increased afterload, and diastolic dysfunction (77). The accuracy of stress myocardial perfusion for the diagnosis of CAD in patients with left ventricular hypertrophy is a subject of controversy, with some studies indicating a low specificity and others demonstrating preserved specificity (77–81). Stress echocardiography was reported in some studies to be more specific than MPI in hypertensive patients (80). In contrast, we found that dobutamine stress echocardiography and simultaneous sestamibi SPECT have similar accuracy for the diagnosis of CAD in hypertensive patients with and without left ventricular hypertrophy. The prevalence of myocardial perfusion abnormalities with dobutamine stress was similar in patients with hypertension and clinically matched population at various grades of pretest probability of CAD (81).
Although myocardial perfusion abnormalities have been reported in hypertensive patients without significant epicardial CAD, the exact prevalence of these findings in hypertensive patients with suspected CAD is not known, because previous studies evaluated a highly selected population. It is possible that the prevalence of these abnormalities is not high enough to account for a difference in the specificity of MPI between patients with and without hypertension. Increased awareness of the cardiovascular complications of hypertension and advances in medical treatment, including the introduction of safe and effective antihypertensive medications, are expected to have an impact on the attenuation of the pathophysiologic effects of hypertension on the myocardium and thereby reduce the severity of structural changes used in the genesis of ischemia in the absence of epicardial CAD.
Assessment of Vascular Compromise After Revascularization.
We recently assessed the accuracy of dobutamine stress myocardial perfusion SPECT for the diagnosis of vascular stenosis in 71 patients 3.7 ± 3.5 y after CABG (64). Sensitivity, specificity, and accuracy of reversible perfusion defects at dobutamine SPECT for the overall diagnosis of vascular stenosis were 81%, 79%, and 80%, respectively. Sensitivity, specificity, and accuracy for regional vascular stenosis were 66%, 83%, and 74% respectively.
There is some disagreement about the specificity of MPI for the diagnosis of restenosis after percutaneous transluminal coronary angioplasty (PTCA). Early studies after PTCA may reveal perfusion defects in the absence of restenosis because of micovascular plugging. We studied 40 patients 185 ± 80 d after successful PTCA with dobutamine stress sestamibi SPECT (67). The sensitivity for the detection of restenosis in arteries with previous PTCA was 69%, specificity was 76%, and accuracy was 72%. The overall sensitivity for the diagnosis of significant coronary stenosis (including arteries without previous PTCA) was 79%, with specificity of 82% and accuracy of 80%.
Another study evaluated 34 consecutive patients with dobutamine 201Tl SPECT 8 wk to 2 y after PTCA (58). Sensitivity, specificity, and accuracy for predicting restenosis were 76%, 79%, and 77%, respectively. One study compared dobutamine thallium with echocardiography in 53 patients after PTCA (59). The sensitivities of echocardiography and SPECT for detecting restenosis were 78% and 74%, respectively; specificities were 93% and 93%, respectively; and accuracies were 87% and 85%, respectively.
Patients with Left Bundle Branch Block.
The diagnosis of CAD has been challenging in patients with left bundle branch block (LBBB). ECG changes during exercise are nonspecific because of the presence of marked repolarization abnormalities (82). The ability of noninvasive tests to diagnose or localize CAD in patients with LBBB has been disappointing. Myocardial perfusion abnormalities may be detected in the septum in the absence of significant left anterior descending CAD (83–85). It is believed that the increase in heart rate and myocardial contractility achieved by exercise and dobutamine may induce septal perfusion abnormalities in the absence of left anterior descending CAD in patients with LBBB (84). The current recommendation is to use vasodilator perfusion imaging in these patients (3). Reports on the use of dobutamine stress MPI in patients with LBBB are scarce. Two small studies on 24 and 27 patients, respectively (83,85), reported contradicting results on specificity. The prognostic significance of perfusion abnormalities in these patients needs additional evaluation.
Assessment of the Extent of CAD After MI.
The role of stress imaging techniques in the functional evaluation of CAD after MI is to assess the presence of myocardial viability in patients with significant systolic dysfunction and to determine the extent of CAD as well as infarct-related and remote coronary artery stenoses. Infarct-related coronary artery patency was assessed in 2 studies. In one 201Tl study (16), sensitivity was 71% and specificity was 83%. In the other, a 99mTc study (20), sensitivity was 44% and specificity was 82%. In a study comparing dobutamine stress sestamibi SPECT and simultaneous echocardiography in 72 patients with healed MI, sensitivity and specificity of remote ischemia for diagnosis of remote coronary stenosis were 68% and 93% for echocardiography and 64% and 90% for sestamibi SPECT, respectively. The positive predictive value and specificity of peri-infarction ischemia for the diagnosis of infarct-related artery stenosis were 89% and 82%, respectively, for echocardiography and 87% and 82%, respectively, for SPECT. The agreement between both techniques was higher for the diagnosis of remote than peri-infarction ischemia (84% vs. 66%, P = 0.02).
Determination of the presence of multivessel CAD in patients with a previous MI should ideally be based on reversible perfusion defects in 2 coronary vascular territories. In 3 studies (16,20,63), sensitivity ranged from 14% to 64% and specificity ranged from 80% to 100%.
Diagnosis of Cardiac Allograft Vasculopathy.
The occurrence of graft vasculopathy is often silent as a result of autonomic denervation. Sudden death and heart failure, therefore, may be the initial presentations (43). Coronary angiography and intracoronary ultrasound imaging allow structural evaluation of graft vasculopathy. However, the associated cost and risk of these invasive techniques may limit their value for the routine consecutive evaluation of these patients. In addition, these techniques do not allow evaluation of the functional significance of the anatomic abnormality. Previous studies have reported conflicting data about the sensitivity and specificity of stress MPI. Sensitivity ranged between 22% and 100%, and specificity ranged between 55% and 100%. We have demonstrated that dobutamine stress tetrofosmin MPI had a high sensitivity (90%) and negative predictive value (79%) for the detection of cardiac allograft vasculopathy in 50 heart transplant recipients (61). The high negative predictive value of the test and the association of a normal study with a low cardiac death rate indicate that patients with normal perfusion by this method might be excluded from further invasive studies. However, the interval at which the stress test should be repeated in these patients remains to be determined.
ASSESSMENT OF MYOCARDIAL VIABILITY
In patients with left ventricular dysfunction as a result of CAD, a variable proportion of dysfunctional myocardium may be viable with potential for improvement after revascularization. Two major mechanisms of viability are recognized: myocardial stunning and hibernation (86). Identification of viable myocardium has important therapeutic implications and provides a useful step in determining which patient with left ventricular dysfunction is likely to have improvement of left ventricular function after revascularization. The diagnosis of viability using MPI is based on the detection of a relatively preserved perfusion (≥50% of the normal uptake) or a reversible perfusion abnormality in the dysfunctional segments (87). Myocardial viability can be evaluated by a resting perfusion study using 99mTc-labeled agents such as sestamibi or tetrofosmin or by rest redistribution 201Tl (88). However, these techniques do not allow evaluation of myocardial ischemia and, therefore, should be reserved for patients who have a contraindication to stress testing or in whom information regarding myocardial ischemia is available. Many patients referred for evaluation of myocardial viability are unable to exercise because of heart failure symptoms. Dobutamine stress MPI is a useful technique in these patients, because it is capable of demonstrating the presence and extent of myocardial ischemia as well as myocardial viability and, therefore, provides useful data for the clinician in deciding whether the patient should undergo revascularization or continued medical therapy. Experience in this regard has been mainly with dobutamine stress reinjection 201Tl imaging. Contractile reserve evaluation using dobutamine-gated SPECT enhances the reliability of nitrate-enhanced sestamibi SPECT when used to predict reversible dysfunction in hypokinetic segments, whereas perfusion quantification remains superior in akinetic and dyskinetic segments (76). Dobutamine stress MPI has a high sensitivity for the prediction of functional recovery after revascularization, although specificity is modest (86–88). With regard to identification of viable myocardium, highly sensitive techniques are required to ensure that none of the patients with viable myocardium will be deferred from revascularization. In general, MPI techniques are more sensitive and less specific than echocardiography in the prediction of myocardial function recovery after revascularization. This may be explained by the fact that the mechanisms related to viability assessment by perfusion imaging (intact membrane, preserved cellular uptake of thallium, intact mitochondria) require less cellular integrity than those required for eliciting viability by echocardiography (inotropic reserve) (86).
A recent study showed that improvement of global left ventricular function during low-dose dobutamine radionuclide angiography is a predictor of improvement of global function after revascularization (89). Combination of results of low-dose dobutamine radionuclide angiography and high-dose dobutamine-atropine stress 201Tl studies before and after revascularization provided useful information about the beneficial effects of CABG in patients with ischemic left ventricular dysfunction. This information led to evidence that, in addition to the stunned and the hibernating myocardium, another entity of viable myocardium exists, which we called “the reactive myocardium” (90).
We have reported that in patients with reduced ejection fraction, CABG induces a significant improvement in resting myocardial perfusion (as demonstrated by dobutamine thallium MPI) and ejection fraction response to inotropic stimulation, even if ejection fraction did not improve on resting studies after revascularization (88). Therefore, resting myocardial function should not be considered as the single endpoint in the evaluation of the effects of CABG on the left ventricular myocardium. A marked improvement of myocardial perfusion is required before an improvement of baseline ejection fraction can be observed. However, patients without improvement in baseline ejection fraction after CABG demonstrate a mild improvement of myocardial perfusion that may be sufficient to increase ejection fraction after CABG during inotropic stimulation but not at rest. We described the myocardium with these characteristics as the reactive myocardium, defined as the myocardium that does not exhibit global improvement of function after revascularization but demonstrates improvement of resting perfusion and ejection fraction response to inotropic stimulation. These effects may be useful in improving remodeling of the left ventricle, amelioration of ischemia, decreased propensity to arrhythmias, and improvement of functional capacity. These findings also indicate that absence of regional or global wall motion improvement after revascularization in patients with a positive viability study on MPI does not necessarily imply a false-positive study, considering the improvement of resting perfusion and contractile response to dobutamine after revascularization observed in these patients (90).
PROGNOSTIC STUDIES
Dobutamine stress MPI has been shown to provide incremental data in the risk stratification of patients with known or suspected CAD (91–101). A recent study evaluated 308 patients who underwent dobutamine stress sestamibi SPECT and were followed for 1.9 ± 1.1 y. There were 33 hard cardiac events. Event rates were higher after an abnormal perfusion (10%/y) than after a normal study (2.3%/y) (P < 0.01), even after adjusting for clinical variables (91). In a study of 392 patients with known or suspected CAD who underwent dobutamine-atropine 99mTc-sestamibi SPECT in our center (90), 44 patients (11%) had a hard cardiac event (cardiac death or nonfatal MI) during follow-up. Normal scan results were associated with a favorable prognosis over the follow-up period, with an annual event rate of 0.8%. In contrast, patients with fixed perfusion defects alone, reversible perfusion defects alone, and fixed plus reversible perfusion defects had significantly increased cardiac event rates of 6.8%, 8.1% and 11.6%, respectively (93). In a multivariate analysis, only age, history of heart failure, typical angina, and abnormal scan patterns were independent predictors of cardiac events. The extent and severity of reversible perfusion defects were important predictors of events. In a study comparing dobutamine stress sestamibi with simultaneous echocardiography in 220 patients (94), no differences in prognostic value could be detected between the 2 imaging modalities. The predictive accuracy of perfusion imaging was higher in patients with submaximal heart rate, consistent with the theory of the ischemic cascade (69,70). In another very small study (95) of patients with known coronary anatomy, annual event rates of 3% for patients with a normal scan and 44% for patients with reversible perfusion defects were found. At multivariate analysis, the only predictors of events were a history of previous MI and the extent of reversible perfusion defects. In one study, the incremental prognostic value of dobutamine stress sestamibi imaging was maintained at long-term follow-up in 528 patients followed for a median of 7.5 y (98).
Two studies (96,97) described the value of dobutamine stress MPI for assessing cardiac risk associated with vascular surgery. Both studies, in 126 and 142 patients, respectively, found a significantly increased risk for perioperative major cardiac events in patients with reversible perfusion defects (50% vs. 5% and 19% vs. 3%, respectively).
Prognostic Value in Patients with Diabetes Mellitus
Diabetes mellitus is associated with an increased risk of cardiac events. Exercise tolerance in patients with diabetes mellitus is frequently impaired as a result of noncardiac disease, such as claudication and polyneuropathy. A recent study assessed the incremental prognostic value of dobutamine stress MPI in 206 diabetic patients unable to perform an exercise test. The patients underwent dobutamine-atropine stress MPI with either sestamibi or tetrofosmin. During 4.1 ± 2.4 y of follow-up, cardiac death occurred in 2 of 69 patients (3%) with normal myocardial perfusion and 34 of 125 patients (27%) with perfusion abnormalities (P < 0.0001). A multivariable Cox proportional-hazards model demonstrated that the presence of an abnormal scan was incremental to clinical data in the prediction of cardiac death (99).
Prediction of Mortality in Heart Transplant Recipients
We assessed the prognostic value of stress myocardial perfusion scintigraphy using 99mTc-tetrofosmin SPECT in 166 heart transplant recipients studied at a median of 7.4 y after transplantation. Patients underwent either high-dose dobutamine (101 patients) or symptom-limited bicycle stress testing (100).
During a median follow-up of 2.5 y, there were 54 deaths (33%), of which 16 (30%) were the result of cardiac causes. Patients with subsequent cardiac death had a higher prevalence and severity of myocardial perfusion abnormalities. Survival rate was higher in the presence of normal perfusion when the endpoints of cardiac death, cardiovascular death, and cardiovascular death plus death as a result of multiorgan failure were considered (P < 0.005). The difference was still significant but to a lesser extent (P < 0.05) when all causes of mortality were considered. Abnormalities of myocardial perfusion were incremental to clinical data in the prediction of cardiac death.
99mTc-Tetrofosmin Imaging
Experience with dobutamine MPI has been largely with 99mTc-sestamibi and 201Tl. 99mTc-tetrofosmin is a newly introduced myocardial perfusion tracer with favorable biokinetics and imaging characteristics. However, a recent study showed that the size of exercise-induced reversible perfusion abnormalities assessed by tetrofosmin is smaller than that assessed by sestamibi (102). No studies have compared these tracers in conjunction with vasodilator or dobutamine MPI.
We studied 124 patients with dobutamine-atropine 99mTc-tetrofosmin SPECT and coronary angiography (60). Sensitivity was 80%, specificity was 72%, and accuracy was 77%. Sensitivity and accuracy rates were higher using the criterion of any defect than using only the criterion of reversible defects (80% and 51%, P < 0.0001; 77% vs. 60%, P < 0.01, respectively). Therefore, optimal accuracy of the technique is achieved by using both fixed and reversible perfusion abnormalities for the diagnosis of CAD in patients without an earlier MI.
The prognostic value was also assessed in 712 patients who underwent dobutamine-atropine stress 99mTc-tetrofosmin SPECT imaging. Over a mean follow-up period of 37 ± 17 mo, 62 cardiac deaths occurred. Nonfatal MI occurred in 23 patients. The cardiac death rate was 1%/y in patients with a normal scan and 5.1%/y in patients with an abnormal scan. The presence of abnormal perfusion was independently associated with an increased risk of cardiac death, after adjusting for clinical and stress test data (101). The extent of perfusion abnormalities has also been shown to be predictive of outcome irrespective of the presence or absence of angina during dobutamine stress (103).
CONCLUSION
Dobutamine stress MPI is a safe and feasible method for the diagnosis and functional evaluation of CAD in patients with limited exercise capacity. The accuracy of this method for the diagnosis of CAD has been demonstrated in various clinical circumstances. The presence of abnormal myocardial perfusion by this method provides incremental data for the risk stratification of patients with known or suspected CAD. Patients with more extensive perfusion abnormalities are at particularly high risk of cardiac death and nonfatal MI.
Footnotes
Received Jan. 22, 2002; revision accepted Jul. 5, 2002.
For correspondence or reprints contact: Abdou Elhendy, MD, PhD, 982055 Nebraska Medical Center, Omaha, NE 68198-2055.
E-mail: aelhendy{at}unmc.edu
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/education/ce_online.html) THROUGH DECEMBER 2003.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Non-invasive assessment of functionally significant coronary stenoses through mathematical analysis of spectral ECG components
- Quantifying Cardiac Hemodynamic Stress and Cardiomyocyte Damage in Ischemic and Nonischemic Acute Heart Failure
- Non-invasive imaging in coronary artery disease including anatomical and functional evaluation of ischaemia and viability assessment
- Dobutamine stress magnetic resonance imaging for the detection of coronary artery disease in women
- Cardiac Image Fusion from Stand-Alone SPECT and CT: Clinical Experience
- Risk Stratification With Electrocardiographic-Gated Dobutamine Stress Imaging
- Prognostic Stratification of Obese Patients by Stress 99mTc-Tetrofosmin Myocardial Perfusion Imaging
- Risk Stratification With Electrocardiographic-Gated Dobutamine Stress Technetium-99m Sestamibi Single-Photon Emission Tomographic Imaging: Value of Heart Rate Response and Assessment of Left Ventricular Function
- Risk Stratification of Patients with Angina Pectoris by Stress 99mTc-Tetrofosmin Myocardial Perfusion Imaging
- Association of Ischemia on Stress99mTc-Tetrofosmin Myocardial Perfusion Imaging with All-Cause Mortality in Patients with Diabetes Mellitus
- Prognostic Stratification Using Dobutamine Stress 99mTc-Tetrofosmin Myocardial Perfusion SPECT in Elderly Patients Unable to Perform Exercise Testing
- Functional significance of stenoses in coronary artery bypass grafts: Evaluation by single-photon emission computed tomography perfusion imaging, cardiovascular magnetic resonance, and angiography
- Impact of Viability, Ischemia, Scar Tissue, and Revascularization on Outcome After Aborted Sudden Death