


Abstract
We examined mandibular invasion of intraoral squamous cell carcinoma by simultaneous bone and tumor dual-isotope SPECT using 99mTc-hydroxymethylene diphosphonate (99mTc-HMDP) and 201Tl-chloride (201Tl) and by CT. Methods: Early and delayed simultaneous bone and tumor dual-isotope SPECT and CT were performed on 39 patients suspected of having tumor invasion of the mandible by intraoral squamous cell carcinoma. SPECT images were superimposed to project tumor location from tumor SPECT onto the osseous structures shown by bone SPECT. The CT imaging protocol consisted of 5-mm contiguous axial images. Results: Histopathologic examination revealed invasion of the mandible in 13 patients and no tumor invasion in 26 patients. The results of delayed dual-isotope SPECT were exactly the same as those of early dual-isotope SPECT. On early and delayed dual-isotope SPECT, the sensitivity, specificity, and accuracy in detecting mandibular invasion by intraoral squamous cell carcinoma were 100% (13/13), 88.5% (23/26), and 92.3% (36/39), respectively. The corresponding values using CT were 45.5% (5/11), 94.7% (18/19), and 76.7% (23/30), respectively, when 9 patients were excluded because of dental artifacts. Conclusion: Our results suggest that superimposed early bone and tumor dual-isotope SPECT images alone may be sufficient in the diagnostic evaluation of mandibular invasion by intraoral squamous cell carcinoma.
- dual-isotope SPECT
- 99mTc-hydroxymethylene diphosphonate
- 201Tl-chloride
- mandibular invasion
- intraoral squamous cell carcinoma
The treatment of intraoral squamous cell carcinoma is in part influenced greatly by the degree of tumor invasion of the mandible. It is recognized that when the mandible is free of tumor, mandibular continuity can usually be preserved. However, once invasion has occurred, a much more extensive and lengthy operation involving partial or total mandibulectomy plus bone grafting is necessary to provide an adequate clear bony margin and to maintain functional and cosmetic integrity.
The use of the physical examination and radiographic studies in the preoperative assessment of tumor invasion in the oral cavity cancer has been examined in several studies (1–5). Bone scanning, plain radiography, CT, and MRI have all been used, although at this time there is no consensus about which technique is the gold standard. Conventional radiography, including orthopantomography, provides an excellent general survey of the entire mandible. However, mineral loss in bone must be as high as 30%–50% before any change is visible (6). CT images can give more detailed cortical resolution, but this is often obscured by ubiquitous dental artifacts. MRI has the inherent drawback of weak signal detection from the bone cortex.
Several studies have shown that planar bone scintigraphy is a useful technique for demonstrating mandibular invasion (7–10). However, the exact sites of accumulation in the mandible that are involved by oral cancer have not yet been ascertained. Chan et al. (11) reported that the normal and abnormal transaxial anatomy of the face and skull could be defined clearly by SPECT. For tumor imaging, SPECT with 201Tl-chloride (201Tl), a radiophamaceutical that displays preferential accumulation in a variety of tumor types, is commonly used. Several reports have demonstrated the efficacy of 201Tl SPECT in evaluating and localizing malignant tissue, especially in the lung (12,13), the thyroid (14), and the skull base (15).
The purpose of this study was to use simultaneous bone and tumor dual-isotope SPECT for colocalization of bone- and tumor-specific radiopharmaceuticals—namely, 99mTc-hydroxymethylene diphosphonate (99mTc-HMDP) and 201Tl—in patients with suspected mandibular invasion by intraoral squamous cell carcinoma. In addition, the results of dual-isotope SPECT were compared with those obtained by CT.
MATERIALS AND METHODS
Patients
This study was conducted on 39 consecutive patients (21 men, 18 women; mean age, 63.2 y; age range, 34–90 y) suspected of having mandibular invasion by intraoral squamous cell carcinoma who were referred to our institution during the past 5 y. The tumor site was tongue (n = 22 patients), gingiva (n = 8 patients), buccal mucosa (n = 6 patients), and oral floor (n = 3 patients). All tumors were staged according to the classification of the International Union Against Cancer (16). Nine patients had T1 lesions, 16 had T2 lesions, 6 had T3 lesions, and 8 had T4 lesions. Tumor invasion of the mandible was confirmed by surgical resection or biopsy. All patients underwent CT and simultaneous dual-isotope SPECT of the mandible with 99mTc-HMDP and 201Tl for routine preoperative assessment. SPECT and CT findings were compared with histopathologic results obtained within 20 d. All patients gave their informed consent after the purpose of the study had been explained.
Simultaneous Dual-Isotope Imaging
Dual-isotope imaging was performed with triple-head gamma cameras (Picker Prism 3000; Picker International, Cleveland, OH) fitted with high-resolution, parallel-hole collimators. This camera was interfaced to a dedicated computer (ODYSSEY; Picker International). The imaging protocol included (a) intravenous injection of 740 MBq 99mTc-HMDP with a 3-h waiting period, (b) 20-min whole-body planar bone scintigraphy, (c) intravenous injection of 111 MBq 201Tl, (d) 10-min injection of 201Tl (3.5 h after injection of 99mTc-HMDP) early dual-isotope SPECT of the mandible, and (e) 2-h injection of 201Tl (5.5 h after injection of 99mTc-HMDP) delayed dual-isotope SPECT of the mandible.
For SPECT images of the mandible, 72 projections were obtained using a 128 × 128 matrix for 60 s per view in a step-and-shoot mode. Using a triple-head camera, the total actual acquisition time was 24 min. Three energy analyzers were used for acquisition. These were set at 71 keV with a 15% window for 201Tl images, 90 keV with a 10% window for scatter images, and 140 keV with a 15% window for 99mTc images. The projection data were processed with a 2-dimensional low-pass filter and then corrected for the contamination scatter. Image reconstruction was performed using filtered backprojection with a ramp filter. Transverse, coronal, and sagittal sections were reconstructed. The system was 7.2-mm full width at half maximum, and the slice thickness was 6.88 mm.
Contamination Scatter Correction for Each Radionuclide
Because the study involved simultaneous dual-isotope imaging, the raw data at the 71-keV window were contaminated by 99mTc Compton scatter, and that at the 140-keV window included the 167-keV γ-ray count for 201Tl. To eliminate such contamination scatter, the raw 99mTc and 201Tl data were corrected according to the equations in each pixel. Measurements of scatter and cross-talk coefficients were performed according to our previous reported method (17).
Visual Analysis of SPECT
The study involved superimposing the bone and tumor SPECT images, which could be done easily using another dedicated computer (FX; Shimadzu, Kyoto, Japan). Because bone and tumor images were acquired simultaneously, the slice pitch and position were exactly the same. Two independent and experienced nuclear medicine physicians, who were unaware of histopathologic and CT findings, visually evaluated the abnormal accumulation in superimposed dual-isotope SPECT on color films, and a consensus was reached regarding the findings. Diagnosis of the mandibular invasion by superimposed SPECT images was made by analysis of bone and tumor images. Tumor SPECT was evaluated for the presence of increased activity in the mandible compared with that in adjacent structures. A positive accumulation in the same area of the mandible on bone and tumor SPECT was interpreted as invasion. A positive accumulation only on bone or tumor SPECT was interpreted as no invasion. A negative accumulation on bone and tumor SPECT was also interpreted as no invasion.
Visual Analysis of CT
CT studies were performed with a HiSpeed Advantage (model 9800; General Electric Medical Systems, Milwaukee, WI) or Aquilion (Toshiba, Tokyo, Japan) scanner. Imaging protocol consisted of 5-mm contiguous axial images through the entire mandible. Bone window settings were obtained in all patients. The CT criteria used were no invasion if the mandible was intact, and invasion in case of destruction of the outer cortex or bone marrow. CT scans were evaluated by 2 independent and experienced radiologists, who were unaware of the results of other modalities. In case of disagreement, they had to reach a consensus.
RESULTS
Of the 39 patients studied, histopathologic examination revealed invasion of the mandible in 13 and no tumor invasion in 26 patients. The results of evaluation of mandibular invasion using dual-isotope SPECT and other modalities (CT and histopathologic findings) are given in Table 1. Results from delayed dual-isotope SPECT were exactly the same as those from early dual-isotope SPECT. Of the 13 patients in whom histopathology revealed invasion of the mandible, all showed abnormal accumulation in the mandible on dual-isotope SPECT. Only 5 of these patients showed conclusive mandibular invasion on CT. Of the 26 patients without tumor invasion of the mandible, 22 showed no abnormal accumulation on dual-isotope SPECT. Three patients showed abnormal accumulation on dual-isotope SPECT but these findings were false-positive. One of these 3 patients also had false-positive findings on CT. In the remaining patient in whom bone SPECT revealed abnormal accumulation but tumor SPECT was negative, mandibular invasion was absent. In 9 patients, the CT image was obscure because of dental artifacts. On both early and delayed dual-isotope SPECT, the sensitivity, specificity, and accuracy in detecting mandibular invasion by intraoral squamous cell carcinoma were 100%, 88.5%, and 92.3%, respectively. The corresponding values using CT were 45.5%, 94.7%, and 76.7%, respectively, when 9 patients were excluded because of dental artifacts.
Assessment of Mandibular Invasion by Intraoral Squamous Cell Carcinoma Using Bone and Tumor Dual-Isotope SPECT, CT, and Histologic Findings
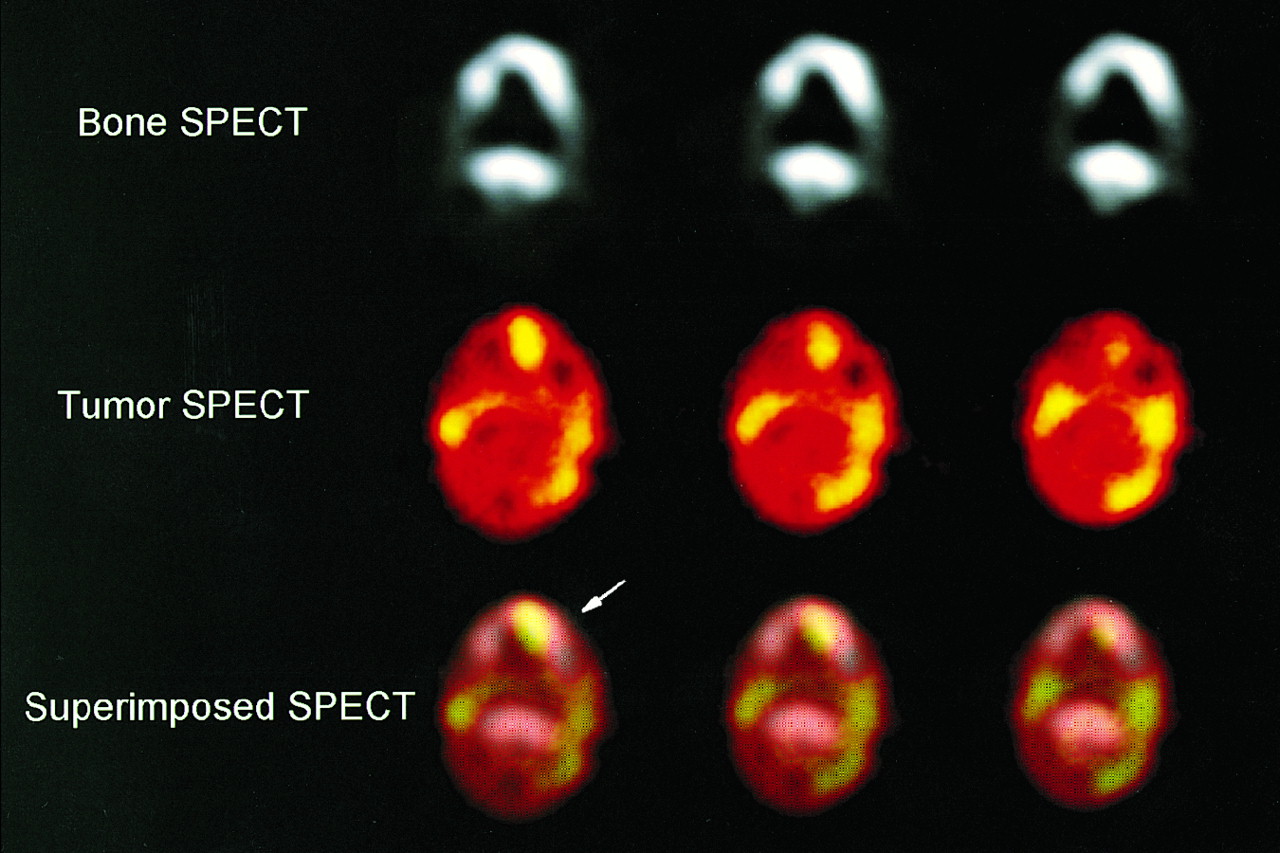
Radiologic findings in a representative case are shown in Figure 1.
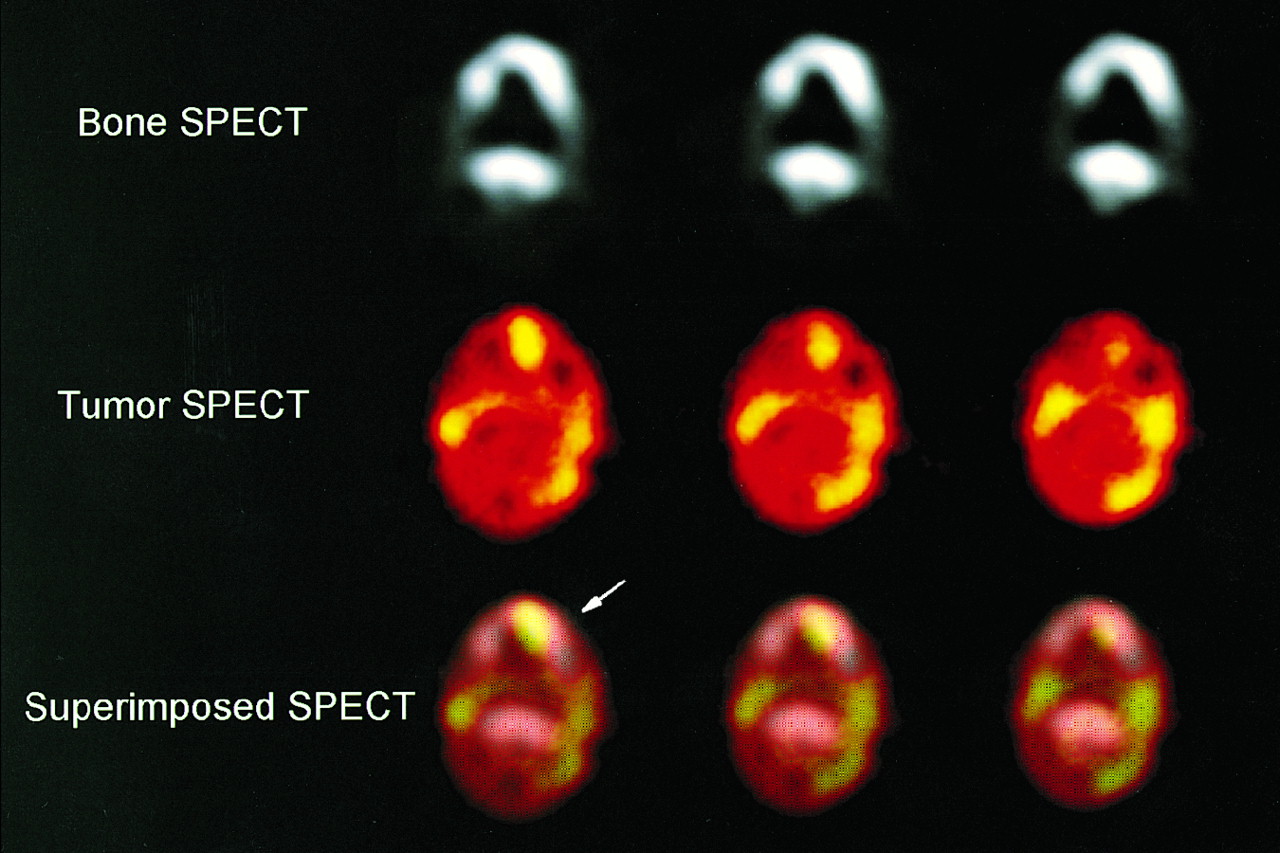
SPECT findings of 73-y-old woman with squamous cell carcinoma of left oral floor. Superimposed bone and tumor SPECT images show abnormal 99mTc-HMDP accumulation corresponding to tumor-positive sites in left mandible (arrow). Dual-isotope SPECT evaluation indicated invasion. Surgical result also indicated invasion.
DISCUSSION
Preoperative evaluation of bone invasion by oral carcinoma has always been a difficult problem. Various methods have been used, including clinical evaluation, pantomography, routine mandible radiography, bone scintigraphy, CT, and MRI. Close et al. (18) reported that, of the 11 patients in whom pathologic examination confirmed mandibular invasion, CT verified osseous involvement in all 11 of these cases. However, in our study, only 5 of the 13 patients in whom histopathology revealed mandibular invasion were identified on CT. This difference might be due partially to imaging techniques, because our CT scans were 5-mm thick, which might have been too much for the depiction of minimal erosion. Shaha (19) compared the diagnostic effectiveness of CT in patients with carcinoma of the floor of the mouth. CT was not shown to be very helpful mainly because of the presence of irregular dental sockets and artifacts (19). Ator et al. (20) compared MRI with conventional imaging, including pantomography and CT, and found that MRI most accurately determined the full extent of tumor invasion in the mandibular marrow spaces. Pellissier et al. (21) also assessed the impact of MRI and CT compared with physical examination in the choice of the type of surgery for advanced oral carcinomas. MRI and CT were found to have high sensitivity, as did physical examination, but none had good specificity (21). Furthermore, dental amalgam artifacts and beam-hardening artifacts from the dense mandible may obscure CT imaging, and the subsets of ferromagnetic metals and certain other metals causing radiofrequency and power tissue maldistribution cause artifacts on MRI (22). Another disadvantage of MRI is its susceptibility to motion artifacts by tongue movement and swallowing.
Planar bone scintigraphy can demonstrate pathophysiologic changes in bone earlier than conventional radiography because osteoblastic activity is increased (8). Although bone scintigraphy seems to be more accurate than pantomography, bone scanning also produces a false-positive rate of as high as 53% and a false-negative rate of 12% due to dental disease (3). Furthermore, radiotracer accumulation occurs not only in tumors but also in infarction and infection. Therefore, planar bone scintigraphy is a highly sensitive but nonspecific technique. Because of its lack of specificity, it is not recommended for evaluation of oral cancer patients because this population often has poor dental status, such as dental abscess and infection, which can simulate neoplastic infiltration (8). Planar bone scintigraphy may also not give enough information for lesion detection or anatomic localization in the evaluation of complex bony structures such as the skull base (15). By separating the overlying and underlying activity into sequential tomographic planes, SPECT can increase image contrast and improve lesion detection and localization compared with planar scintigraphy. Israel et al. (23) showed that SPECT could provide precise localization and define the extent of skull bone involvement, especially for small, deep lesions of the skull base, which are difficult to detect with planar imaging. The isolated assessment of bone SPECT had a sensitivity for osseous tumor spread of 100%, confirming the clinical practice in which bone-sparing resection of tumors close to the jaw is justified with a negative bone scan (24). The inferior dental status of most of the patients with oral squamous cell carcinomas and the consecutively high prevalence of periodontitis and other inflammatory conditions was reported to decrease the specificity of isolated bone scanning to 17.2% and osseous tumor spread could be excluded in only 6.9% of the patients on the basis of the bone scan alone (25).
In the setting of a malignant tumor adjacent to the cortical bone and a positive bone scan, an additional diagnostic usefulness for scintigraphic delineation of the malignancy by a second tracer has to be used. This has been attempted with 67Ga-citrate and 201Tl (15). Fukumoto et al. (15) reported that with simultaneous bone and tumor dual-isotope SPECT with 99mTc-HMDP and 201Tl, in patients with suspected skull base invasion, dual-isotope SPECT clearly visualized bone invasion that was undetectable by CT or MRI. Recently, 99mTc-hexakis-2-methoxyisobutylisonitrile (99mTc-MIBI) has also been established as a tumor tracer (25,26). 99mTc-MIBI combined with bone SPECT has been used by Leitha et al. (25) in diagnosing tumor invasion in patients with primary and recurrent head and neck tumors. In their study, bone SPECT had to be performed on separate days although the patient’s head was placed into a shell to prevent head movement. Thus, superimposition of both SPECT images is difficult to align the images completely. In our study, bone and tumor SPECT imaging was performed simultaneously and image fusion was easy. Glaser et al. (26) reported that an unspecific periosteal reaction in the mandible adjacent to squamous cell carcinomas in the mouth floor may be visualized as hot spots on bone SPECT. If bone scintigraphy is assessed without image fusion with a tumor-avid tracer, the tumor stage is overestimated and the patient is subjected unnecessarily to extensive and multilating surgery (26). In our study, 1 patient showed positive bone SPECT and negative tumor SPECT. Histologic work-up of the tissue in this case confirmed that malignant tissue had reached the periost of the bone, which showed the reactive changes but osseous tumor spread could be excluded. Therefore, simultaneous dual-isotope SPECT images using 99mTc-HMDP and 201Tl are useful to assess mandibular tumor invasion. Tumor image fusion with bone scanning is mandatory for the topographic orientation and increases the specificity of bone scanning to differentiate between inflammatory and malignant causes of increased bone metabolism.
CONCLUSION
In this study, the accuracy of dual-isotope SPECT was higher than that of CT. In addition, results from delayed dual-isotope SPECT were exactly the same as those from early dual-isotope SPECT. Because delayed dual-isotope SPECT did not add any information, the delayed images are unnecessary. The data suggest that superimposed early bone and tumor dual-isotope SPECT images may provide a reliable means of assessing mandibular invasion by intraoral squamous cell carcinoma.
Footnotes
Received Jan. 7, 2002; revision accepted Jul. 9, 2002.
For correspondence or reprints contact: Yuka Yamamoto, MD, Department of Radiology, Kagawa Medical University, 1750-1 Ikenobe, Miki-cho, Kita-gun, Kagawa 761-0793, Japan.
E-mail: yuka{at}kms.ac.jp
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.