


Abstract
The purpose of this study was to evaluate the clinical utility of whole-body PET with 18F-FDG in patients with multiple myeloma and related monoclonal diseases. Methods: Between July 1, 1996, and July 2000, 98 18F-FDG PET scans were obtained for 66 patients, with 25 patients having 2 or more scans. The results were compared with routine clinical and staging information, including CT and MRI scans, as indicated. Of the 66 patients, 16 had previously untreated active myeloma, 14 had monoclonal gammopathy of undetermined significance (MGUS), 10 had disease in remission, and 26 had relapsing disease. Results: Negative whole-body 18F-FDG PET findings reliably predicted stable MGUS. Of the 14 MGUS patients with follow-up of 3–43+ mo, myeloma has developed in only 1 (7%), at 8 mo. Conversely, the 16 previously untreated patients with active myeloma all had focal or diffusely positive scan findings. Four (25%) of 16 previously untreated patients with positive 18F-FDG PET findings had negative full radiologic surveys. Another 4 (25%) of 16 patients had focal extramedullary disease. This was confirmed by biopsy or other imaging techniques. Extramedullary uptake also occurred in 6 (23%) of 26 patients with relapse. This extramedullary uptake was a very poor prognostic factor both before treatment and at relapse. For example, median survival was 7 mo for patients with disease relapse. Persistent positive 18F-FDG PET findings after induction therapy predicted early relapse. In 13 (81%) of 16 patients with relapsing disease, new sites of disease were identified. The 18F-FDG PET results were especially helpful in identifying focal recurrent disease in patients with nonsecretory or hyposecretory disease amenable to local irradiation therapy, which was used in 6 patients. Conclusion: Whole-body 18F-FDG PET provides important prognostic information, which is clinically useful and complementary to conventional methods of evaluating plasma cell disorders. 18F-FDG PET is a unique tool for evaluation of nonsecretory myeloma. Residual or recurrent disease after therapy, especially extramedullary disease, is a poor prognostic factor.
Multiple myeloma is the major plasma cell neoplasm. Myeloma staging and monitoring are central to management decision making. Traditional staging (1) depends heavily on the extent of disease evident on a radiologic full skeletal survey. Radiographs can significantly underestimate the extent and magnitude of bone and bone marrow involvement. 99mTc-diphosphonate bone scanning (2) and gallium scanning (3), although occasionally useful, are unreliable for staging and monitoring. MRI (4–8) is extremely useful for assessing suspected disease sites but is cumbersome as a whole-body screening technique. CT (9,10) is also useful for evaluation of regional or focal disease. MRI and CT frequently do not readily distinguish between active disease and scar tissue, necrosis, bone fracture, or benign disease (11).
A reliable whole-body technique with both functional and morphologic information is necessary to identify the extent and activity of multiple myeloma for staging and monitoring purposes. In this study, we evaluated whole-body 18F-FDG PET as a clinical tool. The results were compared with those of a standard radiologic skeletal survey. Reliability was assessed using standard blood and urine markers of disease activity, MRI, CT, and direct biopsy of questionable sites of disease.
MATERIALS AND METHODS
Clinical Data
Between July 1996 and July 2000, 98 whole-body 18F-FDG PET scans were obtained for 66 patients with multiple myeloma or related monoclonal gammopathies. We undertook a retrospective review of the 98 whole-body scans; 33 used dedicated PET, 39 used coincidence SPECT, and 26 used collimated SPECT. Sixteen patients had previously untreated active myeloma, 10 patients were in remission, 26 patients had relapsing disease, and 14 patients had monoclonal gammopathy of undetermined significance (MGUS) or primary systemic amyloidosis without myeloma. Twenty-five patients had 2 or more whole-body scans for monitoring.
The whole-body 18F-FDG PET was used in addition to standard testing to assess disease stage and activity for baseline evaluation or for follow-up monitoring. The whole-body 18F-FDG PET results were compared with radiologic skeletal surveys as the primary comparison. Additional imaging such as MRI and CT was used adjunctively to confirm or clarify sites of suspected disease. Six patients had direct biopsy of suspected sites as a basis for local irradiation therapy. All patients had standard blood and urine testing including use of M component measurements and serum β2-microglobulin to determine disease status in addition to the clinical findings (12).
Whole-Body 18F-FDG PET
All patients underwent whole-body 18F-FDG surveys using either a dedicated PET system (CPET; ADAC Laboratories, Milpitas, CA [33 scans]), a coincidence camera (MCD; ADAC Laboratories [39 scans] ), or a collimated SPECT system (Meditech; Park, U.K. and Canada [26 scans]). All patients fasted for a minimum of 6 h before their 18F-FDG whole-body study. For dedicated PET, patients received a 170.2-MBq injection of 18F-FDG and were scanned 90 min after injection. A minimum of 6 bed positions was obtained, with a 50% overlap. Whole-body scans, including attenuation correction, required approximately 1 h of imaging time. Coincidence studies were performed after 222–296 MBq of 18F-FDG and a delay of approximately 3 h before scanning. Three overlapping bed positions were obtained, with scan times of approximately 2 h, for a whole-body study. Collimated studies were performed after 370–444 MBq of 18F-FDG, using 2 nonoverlapping bed positions, for a whole-body survey. The total scan time was approximately 2 h.
Images were reconstructed using iterative algorithms and were interpreted in a masked fashion by 2 observers using computer displays consisting of volume-rendered images and coronal, sagittal, and transverse images of the entire body. For the dedicated PET and coincidence studies, attenuation-corrected and non-attenuation-corrected images were interpreted.
Areas of focal uptake were interpreted as positive for myeloma unless they were at sites of known accumulation, including the kidney and bladder, gastrointestinal tract, and certain skeletal areas showing symmetric joint uptake, especially within the shoulder girdle. A diffuse increase in bone marrow activity was interpreted as positive for myeloma if the intensity of activity relative to the background was considered greater than that seen using comparable imaging in patients without bone marrow disease.
RESULTS
Sixty-six patients had 98 whole-body 18F-FDG PET scans as part of this phase I–II evaluation in multiple myeloma and related disorders (Table 1). There were 39 men and 27 women. The median age was 63 y, and the age range was 43–82 y. Image quality was subjectively determined and found to be clinically useful in all studies. Quality was highest in the dedicated PET group, was lower in the coincidence group, and was least acceptable but clinically useful in the collimated group.
Study Population
Previously Untreated Active Myeloma
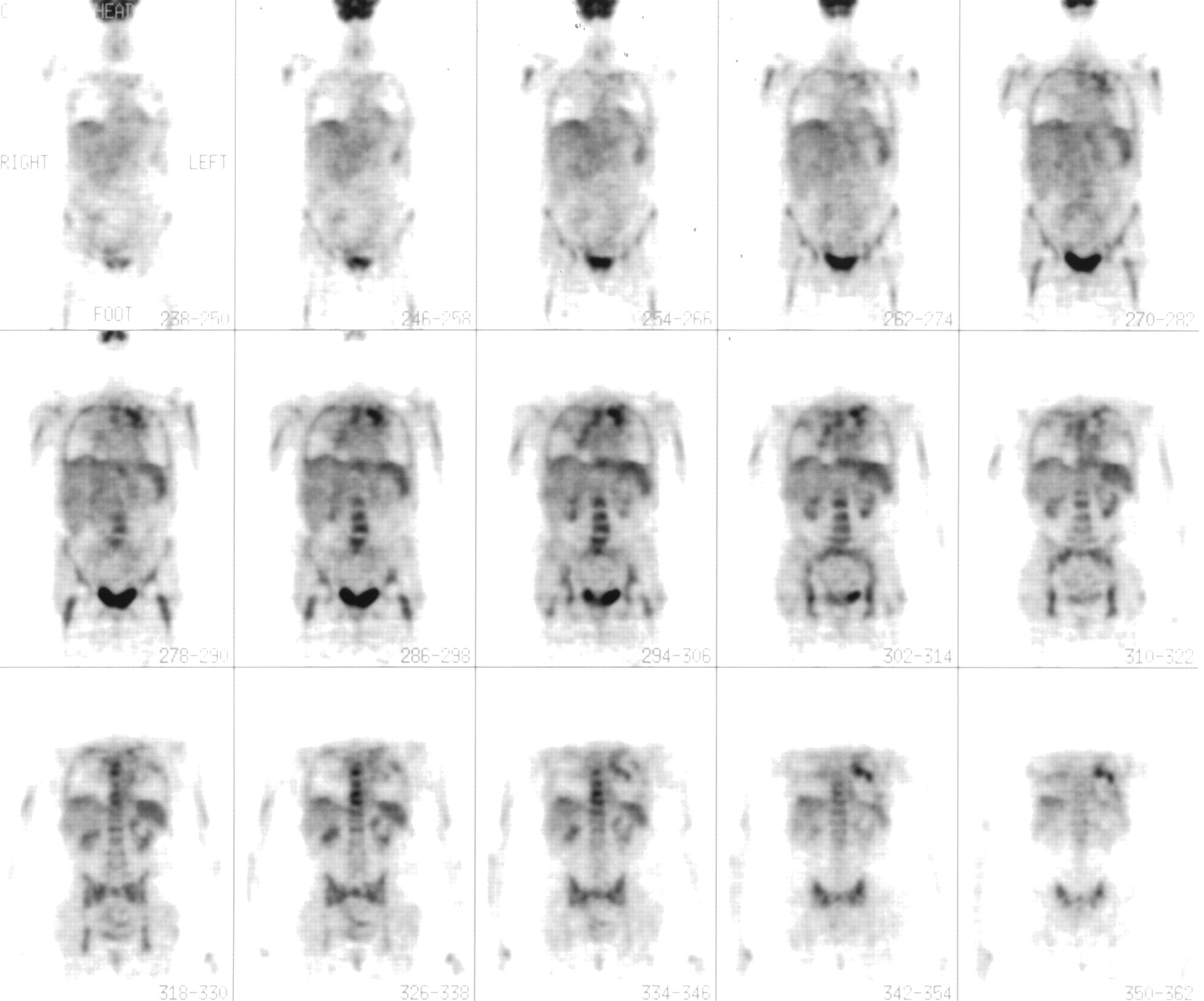
All 16 patients (100%) with previously untreated active myeloma had positive scan findings. Thirteen (81%) of 16 had both focal and diffuse increased bone marrow uptake on the scan, whereas 3 (19%) of 16 had diffuse uptake only, without discrete areas of focal disease. Figures 1 and 2 are dedicated PET studies showing patients with both diffuse and focal disease with no prior therapy.
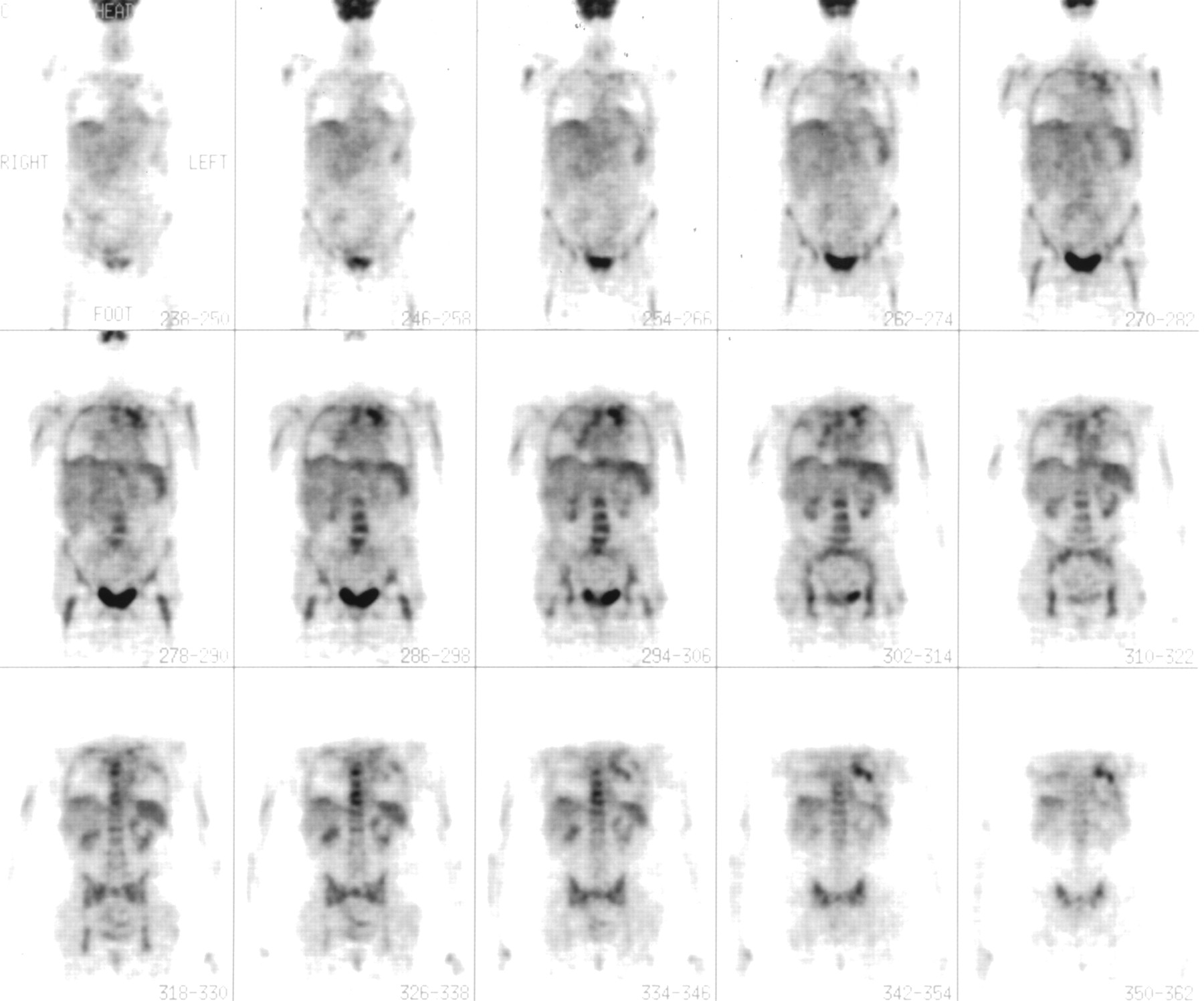
Patient with IgA λ-chain myeloma, stage IIIA. Radiographs revealed multiple lytic lesions in areas that showed positive findings on 18F-FDG PET imaging (e.g., spine, pelvis, and hips). Plasmacytoma in left lung was confirmed on biopsy. Plasmacytomas were noted in left apex and hilar regions on CT scanning. Splenic myeloma was also suspected but not directly confirmed.
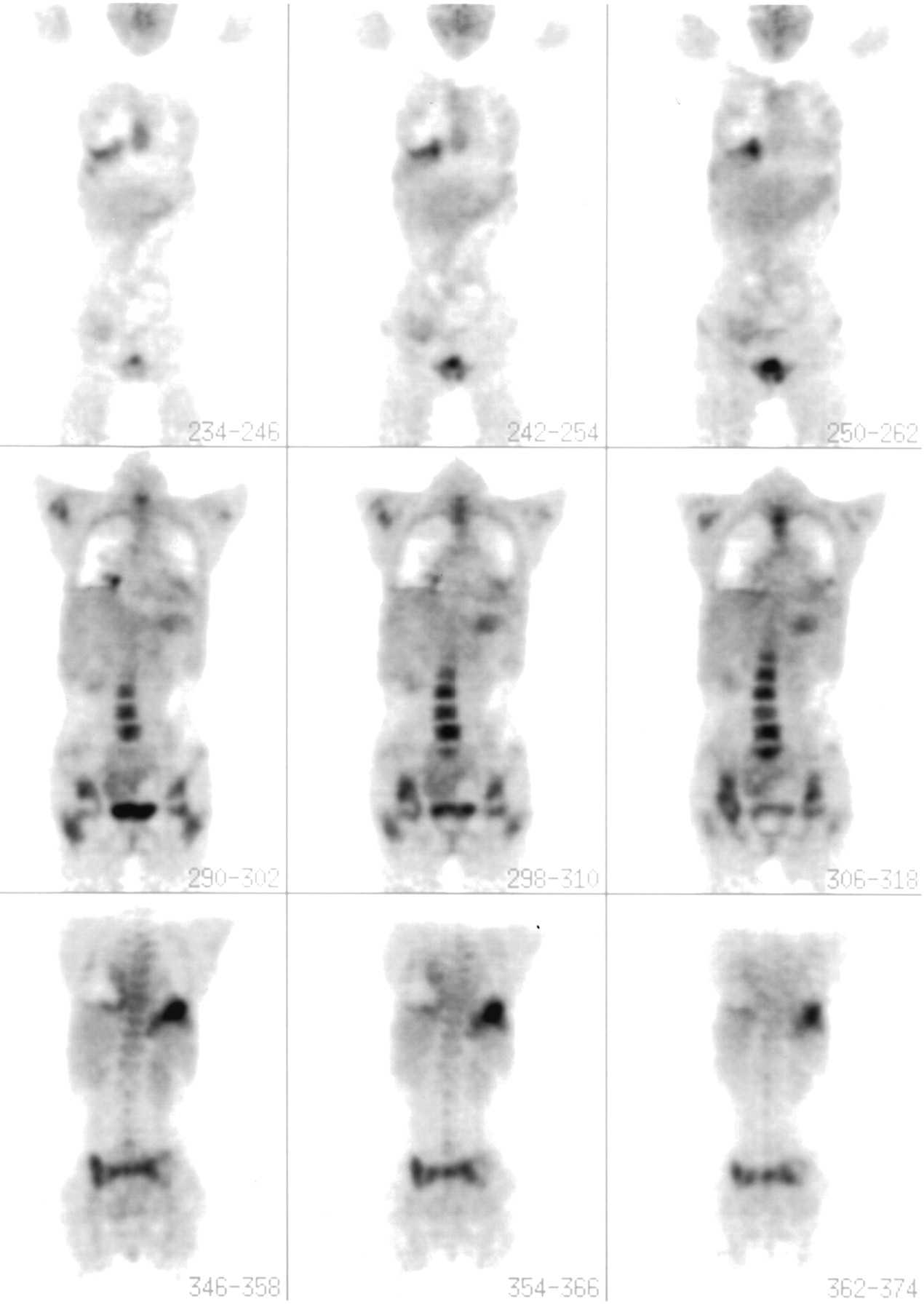
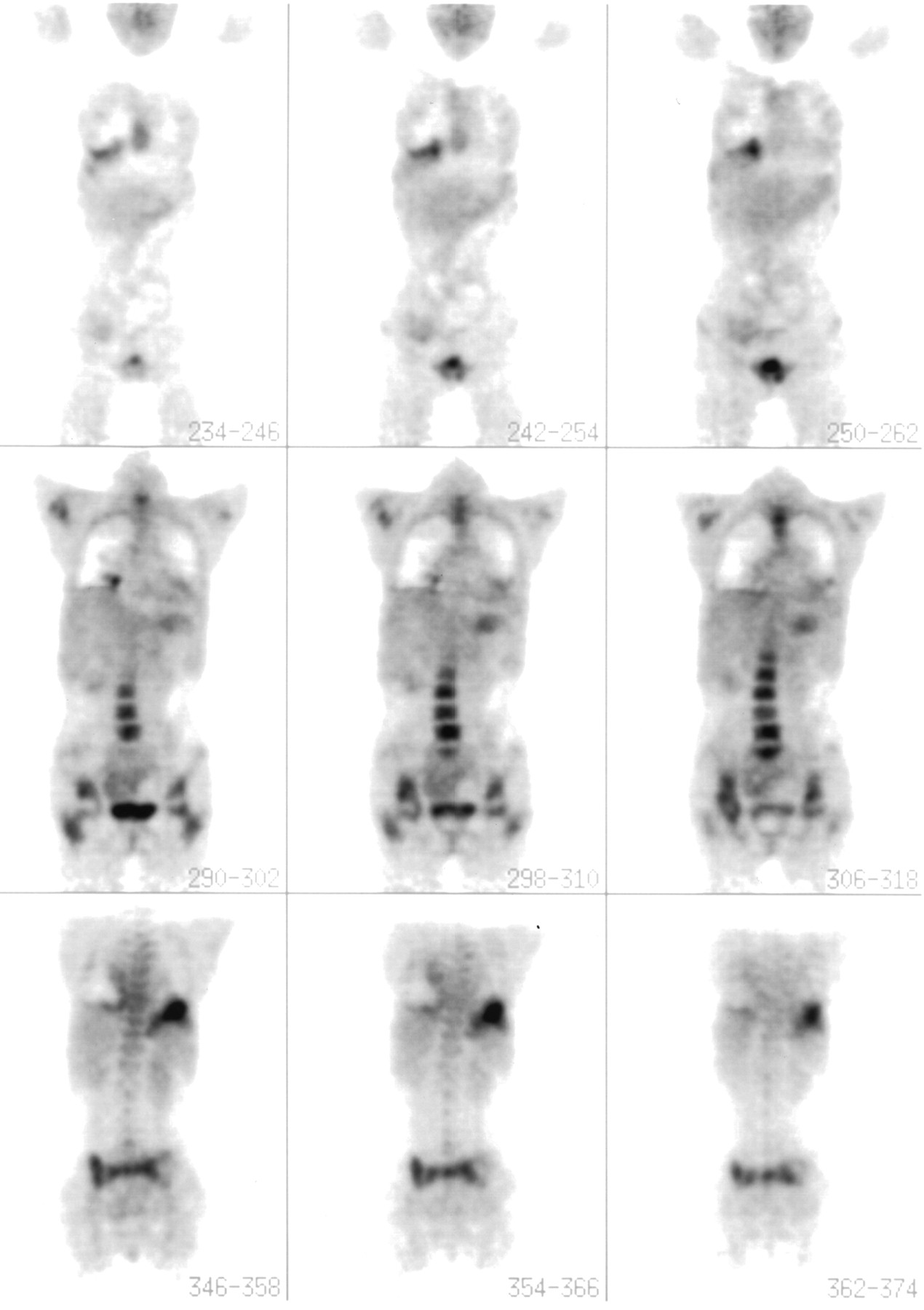
Patient with Bence Jones protein λ-chain myeloma. Extensive disease is seen in spine, and plasmacytomas are seen in right lower lung and left upper abdomen.
Of particular interest, 4 (25%) of 16 patients had no evidence of multiple myeloma on a routine skeletal bone survey but had positive whole-body 18F-FDG PET findings. One patient previously considered to have stage IA disease was reconsidered to have a single (solitary) plasmacytoma. Dedicated PET showed the patient to have multiple lesions, which were subsequently confirmed by MRI and CT. The disease of this patient was restaged as IIIA. The 3 additional patients had stage III disease by other criteria but had no documented sites of discrete or focal bone disease. Again, the new sites of disease were confirmed by MRI or CT.
There were also 4 (25%) of 16 patients, already documented to have stage III disease, who were found to have additional foci of extramedullary disease. The nature of the focal uptake was confirmed both by other imaging and by direct biopsy in 2 instances (pulmonary [Fig. 1] and periorbital). The predilection for extramedullary spread was also confirmed by the subsequent development of additional extramedullary disease, including subcutaneous lesions. One patient died with fulminant disease at 4 mo after the study, and another with aggressive relapse after stem cell transplantation died at 23 mo. The other 2 patients with extramedullary disease are still alive and undergoing therapy at 6 and 18 mo, although the disease of 1 has already relapsed after transplantation.
MGUS
Fourteen patients had a working diagnosis of MGUS (13) and negative scan findings, showing neither diffuse marrow uptake nor areas of focal disease in marrow sites. Current follow-up is between 3 and 43+ mo from the time of the first 18F-FDG PET scan. All but 2 patients had a new diagnosis of MGUS. The 2 prior diagnoses were of 3 and 9 y duration. Both patients have negative scan findings and still have MGUS 23 and 31 mo later. In 1 (7%) of 14 patients, multiple myeloma has since developed after 8 mo and was associated with the development of multifocal positive scan findings. Of interest, 4 patients have been documented to have primary systemic amyloidosis in association with the MGUS in the absence of myeloma. At the time of the first study, all sites of amyloid were also negative on scans. However, in 1 patient, treated with stem cell transplantation for amyloidosis, focal uptake at the site of a plasmacytoma subsequently developed, with amyloid located in the distal esophagus (Fig. 3). This solitary relapse site has been treated with local irradiation. One other patient with IgA κ-chain MGUS had an 18F-FDG PET scan that was negative at bone marrow sites but revealed a renal mass. This proved to be a renal carcinoma (previously unsuspected), which was resected and has not recurred at more than 2 y later. The whole-body 18F-FDG PET scan remains negative in bone marrow sites, and the IgA κ-chain MGUS is persistent but stable.

Patient with relapse after stem cell transplantation. Dysphagia developed and was associated with positive finding in distal esophagus. Direct biopsy showed plasma cells with local amyloid deposition. This responded well to local irradiation.
Remission Monitoring
Ten patients have been monitored with baseline and follow-up 18F-FDG PET scans for 6–42+ mo. New focal sites of disease have developed in 6 (60%) of the 10 patients. Because patients with nonsecretory disease were preferentially enrolled for monitoring in this initial study of whole-body 18F-FDG PET, the establishment of specific sites of focal relapse was especially helpful for this subset of patients. In all 6 instances of focal relapse, local irradiation was feasible and used as a first step in management. Four (67%) of 6 had nonsecretory disease and no other methodology available to adequately screen the whole skeleton for early relapse.
Relapsing Disease
Twenty-six patients were evaluated at the time of suspected relapse. Twenty-one (81%) of the 26 patients had new, previously unsuspected sites of disease documented by whole-body scanning. This was extremely helpful in assessing the extent and exact anatomic distribution of the disease. Six (23%) of the 26 patients showed evidence of new extramedullary disease, which was subsequently documented by other imaging and biopsy plus further follow-up. Extramedullary sites included skin, bladder, retroperitoneum (with ureteral obstruction), liver, lung (Fig. 2), and mediastinum. As noted for the previously untreated patients, the onset of extramedullary disease indicated a poor prognosis. Currently, subsequent survival has been 3, 4, 6+, 8, 11, and 13+ months: that is, a median of 7 mo.
For the patients showing relapse in bone, the new sites of disease were widely scattered and typical for myeloma; including the spine, scapulae, ribs, clavicle, base of the skull, pelvis, and femora. The whole-body 18F-FDG PET scans showed new sites of active disease. Again, in patients with nonsecretory disease, studied for the first time at relapse, focal disease was amenable to radiation in 2 additional instances. When necessary, sites of disease were confirmed by bone marrow or tissue biopsy, MRI, or CT, especially around joints such as the shoulder to exclude inflammatory disease.
Impact of Dedicated 18F-FDG PET
The dedicated 18F-FDG PET system has been in use at Cedars-Sinai Medical Center since September 1999. Approximately one third of the scans performed as part of this study used this system and involved 50% of the patients. The dedicated system significantly improved the quality of the images. However, serial studies involving earlier coincidence or collimated studies did not affect the serial follow-up conclusions (Table 2) or the algorithm for further evaluation (Table 3). For example, the patient in whom myeloma developed at 8 mo (Table 2) underwent initial scanning with the coincidence technique. The findings were negative, and the patient was clinically stable. At the time of follow-up with the dedicated system, new changes reflective of myeloma were seen and showed a correlation with other changes in the laboratory results and clinical status. It is obvious that the dedicated system has superior resolution and should be used whenever possible to maximize the data.
Whole-Body 18F-FDG PET Scan Results
Potential Role for 18F-FDG PET Scan Evaluation Based on Current Data
DISCUSSION
Our study indicates an important complementary role for whole-body 18F-FDG PET in the evaluation of patients with multiple myeloma and related disorders. There were no false-negative results in the discrimination of MGUS from active myeloma. Additional clinically useful information was obtained from positive scan findings in patients with active myeloma. Although myeloma subsequently developed in 1 MGUS patient, and plasmacytoma in another, both occurred more than 6 mo after the initial scan. In patients with active myeloma, symptomatic or new active sites of disease were routinely detected, although not every lesion detectable using traditional structural imaging (e.g., CT or MRI) was seen using metabolic 18F-FDG PET imaging. The utility of metabolic imaging to detect sites of active disease was particularly evident in patients with relapsing disease, 81% of whom had new sites identified. Twenty-three percent of relapsing patients demonstrated extramedullary disease, which had a particularly poor prognosis, conferring a median survival of 7 mo in this patient group.
These findings in myeloma reflect both the overall experience with 18F-FDG PET in clinical oncology (14–19) and the specific utility in several other malignancies (10–26). The recent findings in the evaluation of patients with non-Hodgkin’s lymphoma and Hodgkin’s disease are particularly notable (22, 23) Prior clinical experience with myeloma patients is limited (27, 28).
The gold standard for imaging in myeloma patients is a radiologic full skeletal survey. Using this technique, one can evaluate all high-risk disease sites for the presence of focal or diffuse bone destruction or loss. Unfortunately, early evidence of bone damage is missed. In our study, 4 patients (25%) with negative radiologic surveys had multiple focal lesions on 18F-FDG PET, with the disease of 1 patient being upstaged from stage I to stage III. The scan results drew attention to sites of potential clinical problems. In 4 additional patients (again, 25%), the presence of extramedullary sites of disease indicated a poor prognosis (Table 2).
Although high-resolution CT and MRI have allowed the identification of myeloma sites in patients with negative radiography findings, 18F-FDG PET has the advantage of allowing whole-body screening as well as distinguishing between new active disease and old disease, scar tissue, necrotic tissue, radiation changes, and separate benign disease (e.g., fibromas or lipomas). For example, in a patient being monitored after radiation therapy and stem cell transplantation, MRI showed several lesions of uncertain significance that were negative on 18F-FDG PET. Biopsies showed scar tissue and a lipoma. Conversely, biopsy routinely confirmed myeloma at sites positive for 18F-FDG uptake on PET. The only false-positive finding was a hemangioma evident on MRI but not examined by biopsy.
On the basis of this initial experience, an algorithm can be established for the further delineation of the role of whole-body 18F-FDG PET (Table 3). In each of the disease settings—MGUS, active myeloma, remission, and relapse—it is possible to identify areas of clinical utility that deserve detailed analysis and a cost-benefit review. For example, in patients with MGUS, detailed and expensive testing is frequently used to rule out active myeloma and to try to definitely diagnose MGUS. Studies such as bone marrow cytogenetics, kinetics, and immunophenotyping are often used and are expensive (29). If further testing confirms the utility of whole-body 18F-FDG PET, it can prove to be quite convenient and cost-effective. Likewise, in patients either with active myeloma at baseline or undergoing serial monitoring during remission or relapse, clinically meaningful information can be gathered to assess prognosis and treatment options. Again, further studies are required to evaluate this type of algorithm incorporating systematic alternate imaging and a formal cost-benefit analysis. If comparisons with other diseases such as lymphomas are any guide, several areas of utility can be reasonably anticipated (18,19).
In the evaluation of myeloma, it is hard to imagine the abandonment of radiography as a standard technique. In the foreseeable future, radiographs will remain the yardstick for comparison. In addition, MRI and CT have an established role in the identification and anatomic definition of myeloma lesions, especially in the spine and brain. Nonetheless, as indicated in the algorithm, it is likely that whole-body 18F-FDG PET can usefully complement these technologies in the clinical settings described. Does a patient have MGUS? Does a patient have residual disease after transplantation? Is relapse focal or diffuse, and is poor-risk extramedullary disease present? These are the kinds of questions that are usefully and conveniently answerable with whole-body 18F-FDG PET.
CONCLUSION
Whole-body 18F-FDG PET reliably detects active multiple myeloma. Conversely, negative 18F-FDG PET findings strongly support the diagnosis of MGUS. Residual myeloma after stem cell transplantation, and extramedullary myeloma detected by 18F-FDG PET, are both findings indicative of high-risk myeloma and of a poor prognosis. 18F-FDG PET is a unique tool for the evaluation of nonsecretory myeloma. Whole-body 18F-FDG PET is a new, useful imaging tool for the evaluation of patients with plasma cell dyscrasias.
Footnotes
Received Apr. 2, 2002; revision accepted Jul. 9, 2002.
For correspondence or reprints contact: Brian G.M. Durie, MD, 8201 Beverly Blvd., Los Angeles, CA 90048.
E-mail: bdurie{at}salick.com
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Multiple myeloma with central nervous system relapse
- Multiple Myeloma, Version 3.2017, NCCN Clinical Practice Guidelines in Oncology
- Multiple Myeloma, Version 2.2016
- In Silico Modeling-based Identification of Glucose Transporter 4 (GLUT4)-selective Inhibitors for Cancer Therapy
- In vivo molecular imaging of chemokine receptor CXCR4 expression in patients with advanced multiple myeloma
- Impact of Initial FDG-PET/CT and Serum-Free Light Chain on Transformation of Conventionally Defined Solitary Plasmacytoma to Multiple Myeloma
- 11C-Acetate PET/CT for Metabolic Characterization of Multiple Myeloma: A Comparative Study with 18F-FDG PET/CT
- The role of positron emission tomography-computed tomography and magnetic resonance imaging in diagnosis and follow up of multiple myeloma
- Imaging in myeloma
- Multiple myeloma presenting as plasmacytoma of the jaws showing prominent bone formation during chemotherapy
- Imaging of Multiple Myeloma and Related Plasma Cell Dyscrasias
- Prognostic relevance of 18-F FDG PET/CT in newly diagnosed multiple myeloma patients treated with up-front autologous transplantation
- Multiple Myeloma
- Consensus recommendations for standard investigative workup: report of the International Myeloma Workshop Consensus Panel 3
- Prognostic Significance of Focal Lesions in Whole-Body Magnetic Resonance Imaging in Patients With Asymptomatic Multiple Myeloma
- Multiple Myeloma
- Targeting Glucose Consumption and Autophagy in Myeloma with the Novel Nucleoside Analogue 8-Aminoadenosine
- A new pet for myeloma
- NCCN Task Force: Clinical Utility of PET in a Variety of Tumor Types
- FDG-positron-emission tomography for staging and therapeutic assessment in patients with plasmacytoma
- Hyperattenuating bone marrow abnormalities in myeloma patients using whole-body non-enhanced low-dose MDCT: correlation with haematological parameters
- 18F-FDG PET/CT, 99mTc-MIBI, and MRI in Evaluation of Patients with Multiple Myeloma
- Multiple Myeloma Presenting With [18F]Fluorodeoxyglucose Avid Liver Lesions Diagnosed on Positron Emission Tomography Scan
- A prospective comparison of 18F-fluorodeoxyglucose positron emission tomography-computed tomography, magnetic resonance imaging and whole-body planar radiographs in the assessment of bone disease in newly diagnosed multiple myeloma
- Artifactual Spinal Metastases Imaged by PET/CT: A Case Report
- Imaging of Malignant Bone Involvement by Morphologic, Scintigraphic, and Hybrid Modalities
- Plasma Cell Problems: CASE 3. Plasmacytoma Mimicking a Paraganglioma of the Skull Base: Diagnostic Value of Somatostatin Receptor Scintigraphy
- Side Effects and Good Effects from New Chemotherapeutic Agents: CASE 3. Bortezomib in Primary Refractory Plasmacytoma
- Magnitude of Response With Myeloma Frontline Therapy Does Not Predict Outcome: Importance of Time to Progression in Southwest Oncology Group Chemotherapy Trials
- Unusual Presentations of Hematologic Malignancies: CASE 1. Solitary Bone Plasmacytoma: Role of Magnetic Resonance Imaging and Positron Emission Tomography
- Treatment of multiple myeloma