


Abstract
Postsurgically elevated or increasing serum calcitonin levels strongly suggest the presence of residual or recurrent medullary thyroid carcinoma (MTC). Several imaging modalities (sonography, MRI, CT, scintigraphy with different types of radiolabeled ligands, etc.) are routinely used in an attempt to localize tumorous tissue, but such efforts often fail. In the search for a more reliable method, 18F-FDG PET was applied to detect tumor tissue of residual or recurrent MTC. Methods: Forty patients with a postoperatively elevated plasma calcitonin level were included. These patients underwent routine diagnostic imaging procedures (CT, MRI, and 131I-metaiodobenzylguanidine [MIBG] whole-body planar scintigraphy or SPECT) and 18F-FDG PET examinations. Two independent experts visually analyzed the images provided by each method to detect pathologic lesions. Lymph nodes of ≥1 cm in short diameter that were detected by radiologic methods were considered to be pathologic. 18F-FDG accumulation with a sharp contour reported by both independent observers was similarly regarded as pathologic. Results: PET detected 270 foci with a high tracer accumulation, whereas only 116 lesions were detected by MRI and 141 by CT. The numbers of such foci determined by PET, MRI, and CT were 98, 34, and 34, respectively, in the neck; 25, 5, and 6, respectively, in the supraclavicular regions; and 117, 35, and 39, respectively, in the mediastinum. 131I-MIBG scintigraphy findings were positive for only 3 patients. Conclusion: For MTC patients with a postoperatively elevated plasma tumor marker level, PET was more sensitive and superior in localizing tumorous lymph node involvement than were the other imaging modalities, especially in the cervical, supraclavicular, and mediastinal lymphatic regions.
Medullary thyroid carcinoma (MTC) originating from the calcitonin-secreting parafollicular cells (C cells) is a relatively rare disease, composing 3%–10% of all malignant thyroid tumors (1). The familial forms, which account for 25% of all MTCs, include 3 well-defined syndromes: familial MTC and multiple endocrine neoplasia types 2A and 2B. The remainder (75%) of MTCs are sporadic. Among the metastases, lymph node involvement is the most common throughout the clinical course. During initial staging, the incidence of pathologically proven cervical lymph node metastases has been reported to be 71%–80% (2–4); the corresponding value for mediastinal involvement is 36% (2,4), whereas distant metastases have been reported in 20% of MTC patients (5).
Postsurgically elevated basal serum calcitonin and carcinoembryonic antigen (CEA) levels suggest persisting tumorous tissue (6), and testing of the levels of these plasma markers is therefore the most frequently applied method in long-term follow-up. Selective venous catheterization (7,8), with a correct localization rate of 89%, is the gold standard for identification of residual or recurrent lymph nodes; however, its invasiveness restricts its general use. Morphologic imaging methods can confirm the involvement of lymph nodes on the basis of their size, but these investigations are often insufficient because of the smallness of the tumorous lesions (9,10). Sonography has shown a lymph node detection rate of 28%–78% (11,12), compared with 38%–70% for CT (11,12) and 44%–74% for MRI (13,14). Various tumor-avid radiotracers, such as 201Tl-chloride, 123I- or 131I-metaiodobenzylguanidine (MIBG), radiolabeled anti-CEA antibodies, pentavalent 99mTc-dimercaptosuccinic acid, and 111In-pentetreotide, have been used for tumor imaging with limited efficacy (15–22).
The accumulation of 18F-FDG in malignant tissue is well known; it is influenced by the grade of malignancy, related to glycolysis (23). 18F-FDG has been successfully used in the follow-up of patients with differentiated thyroid cancer (24–30). There are similar reports on 18F-FDG PET investigations in MTC; however, the number of patients involved in these studies was generally <10 (31–34), with the exception of a single study (35) in which 20 patients were investigated.
We report data on the application of 18F-FDG PET in several MTC cases and compare the results of this method with those of conventional imaging procedures for the diagnosis of residual or recurrent MTC.
MATERIALS AND METHODS
Patients
Forty nondiabetic patients (18 men, 22 women; age range, 23–69 y; mean age ± SD, 48 ± 11 y) with a history of MTC (15 hereditary, 19 sporadic, and 6 undetermined) were included in this investigation. The initial histologic result, including the immunophenotyping of each case, was revised by an independent pathologist. All but 1 patient had undergone total, near-total, or subtotal thyroidectomy, and 28 had undergone lymph node dissection, node picking, or both. The only exception was a patient who had a sternotomy because of the atypical localization of the primary tumor in the mediastinum.
External irradiation was used as supplementary therapy in 30 patients, 7 received 131I-MIBG radionuclide therapy, and 3 had chemotherapy. As tumor markers, the basal plasma calcitonin level (reference level, <10 ng/mL) was measured by human calcitonin enzyme-linked immunosorbent assay (CIS Bio International, Gif sur Yvette, France) with 2 monoclonal antibodies, and CEA (reference level, <6 ng/mL) was determined by luminometry. The marker levels were assessed postsurgically after 2 mo and at 6-mo intervals thereafter. Details of the individual patients are displayed in Table 1.
Patient Characteristics
Imaging
All diagnostic imaging examinations of the same patient were performed at least 2 mo after any therapy and were completed within a 3-mo interval. Written consent was obtained from all patients before the start of the procedures. 18F-FDG PET studies were performed with a 4096 Plus scanner (General Electric, Uppsala, Sweden) providing fifteen 2-dimensional sections over an axial field of view of 10 cm. The in-plane resolution was 5.5 mm (full width at half maximum), and the axial resolution was 6 mm. To suppress myocardial uptake, patients had to fast for at least 4 h before receiving 5.55 MBq/kg (0.15 mCi/kg) 18F-FDG by intravenous injection. The patients were also requested to abstain from physical activity before injection and until scanning. Whole-body examinations were begun from the base of the pelvis 40 min after the administration of 18F-FDG (7–9 bed positions, 10 min acquisition time per position). The acquired data were reconstructed using filtered backprojection with a Hanning filter (cutoff, 0.5 pixels−1). To avoid the extra inconvenience to the patients of a lengthy transmission scan, which would have been required because of the lack of an iterative reconstruction and segmentation algorithm in the software bundled with the camera, we did not correct for tissue attenuation.
Native and contrast-enhanced helical CT scanning was performed with a Somatom HR (Siemens, Erlangen, Germany) scanner, with a slice thickness of 5 mm from the base of the skull to the apex of the lung and a slice thickness of 10 mm for the rest of the body. Axial and coronal unenhanced T1-, T2-, and proton-weighted images of the neck, chest, and abdomen were obtained with a 1.5-T MRI unit (Magnetom; Siemens) for all patients, excluding 5 individuals with claustrophobia. The T1 axial sequences were repeated after the administration of contrast material.
Overlapping multiple planar images of the whole body were obtained for all patients with a Starcam 600XR/T (General Electric Medical Systems, Milwaukee, WI) or GCA-7100DI (Toshiba Corp., Tokyo, Japan) gamma camera, 48–72 h after the injection of 40 MBq 131I-MIBG. Additional SPECT scans of the neck and thorax were obtained for some patients with a high-energy parallel-hole collimator.
Interpretation
The number of pathologic foci was determined by visual assessment of the reconstructed images of the individual imaging modalities by 2 experts. 18F-FDG accumulation with a sharp contour reported by both independent observers was regarded as pathologic. Lymph nodes of ≥1 cm in short diameter that were detected by radiologic methods were likewise considered to be pathologic.
RESULTS
Elevated calcitonin levels (range, 14.5–5,827 ng/mL; mean ± SD, 1,246.44 ± 1,505.43 ng/mL) were detected in all 40 patients, 25 of whom had a CEA level (range, 6.5–694.5 ng/mL; mean ± SD, 120.13 ± 176.02 ng/mL) above the reference range.
Various numbers of involved lymph nodes and other metastases were visualized through the different imaging modalities for all patients studied (Tables 2 and 3). PET scans were conclusive for 38 patients, showing 98 cervical, 25 supraclavicular, 4 axillary, 117 mediastinal, 3 abdominal, 14 hepatic, 6 osseous, and 2 pulmonary lesions with a high 18F-FDG uptake, whereas CT revealed 34, 6, 3, 39, 3, 24, 0, and 31 such lesions, respectively, and MRI revealed 34, 5, 1, 35, 0, 16, 2, and 22, respectively. In addition, a breast metastasis was found in 1 patient; it was detected by CT, MRI, and PET (Fig. 1) and was confirmed by histology. Thyroid remnants were confirmed by CT, MRI, sonography, or thyroid scintigraphy for patients having a less radical thyroidectomy (near-total or subtotal). In these patients (8/31, 26%), a total of 12 lesions with 18F-FDG uptake were present in the central cervical region at the site of the thyroid bed. These accumulations associated with the physiologic uptake by the thyroid remnants were not included in the number of lesions found by PET. When PET was compared with anatomic tomographic imaging methods, the differences were clear: PET detected more foci in the neck (37 patients) and the mediastinum (33 patients) than the others did (Figs. 2 and 3), but PET failed to localize many lesions in the lung and the liver. 131I-MIBG planar scintigraphy findings were positive for only 3 patients. The results with this method (2 cervical, 1 mediastinal, and 1 bony lesion) did not add any information to that furnished by the other diagnostic examinations. For 2 patients, despite the elevated calcitonin level (patient 22, 40.2 ng/mL; patient 33, 21.5 ng/mL), all the examinations failed to localize any metastases. The results of PET, CT, and MRI were considered to be false-negative for both patients.

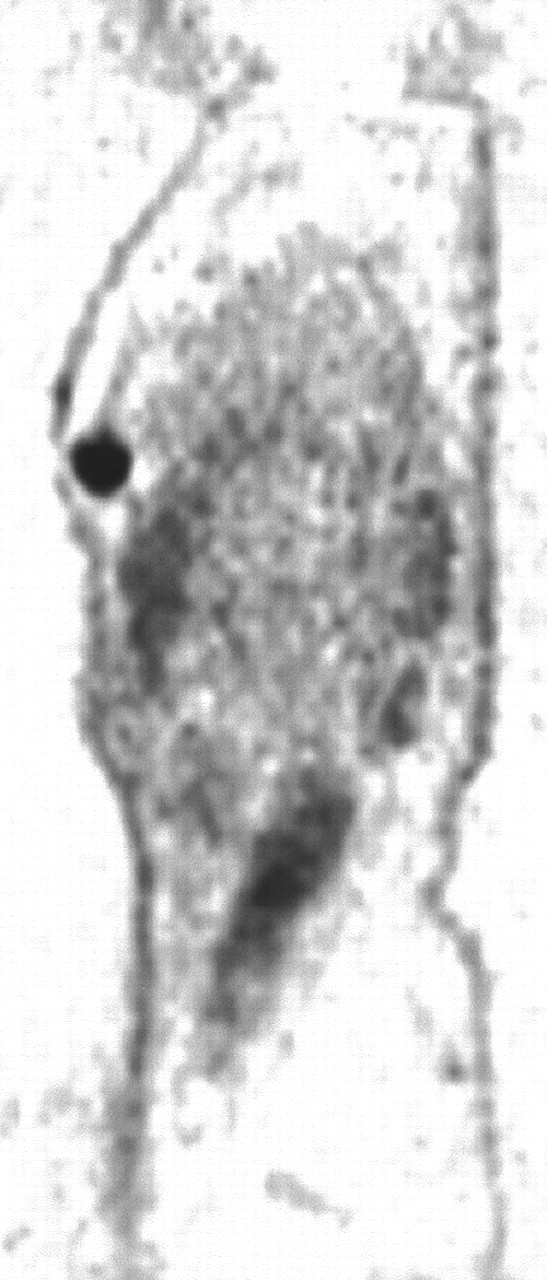
Sagittal slice shows high 18F-FDG accumulation in right breast of patient 17.

18F-FDG PET shows high tracer uptake in left lateral cervical compartment and in left supraclavicular region of patient 24. Radiologic methods detected lymph node only in left supraclavicular region. Histology confirmed metastases of MTC in both sites.

Coronal slices show multiple 18F-FDG accumulation in mediastinum and both pulmonary hila of patient 36.
Number of Patients with Detected Manifestations
Number of Affected Lymphatic Regions (Nodes) Detected
Aspiration cytology or surgical intervention assisted in the verification of localized cervical, supraclavicular, and mediastinal lymph node metastases in 10 patients. Although not all PET-detected lesions were proven pathologically, subsequent noninvasive radiologic examinations revealed pathologic lymph node enlargement or hepatic, pulmonary, or bone metastases in 15 patients. Small hepatic metastases were detected in 35 patients who underwent hepatic angiography. PET imaging revealed 2 cases of suspected bony metastases. In the case of the solitary metastasis, tumorous manifestation was supported by CT, MRI, and somatostatin receptor scintigraphy, but 2 completed biopsies (each reported by 2 independent pathologists) excluded the presence of metastatic disease. The other case also proved to be false-positive on the basis of the 3-y uneventful follow-up. Although the above methods supported the PET findings in a substantial proportion of our patients, the data on some patients still require validation. However, these patients have shown no clinical signs contradicting the PET findings.
The data obtained during the follow-up from the initial diagnosis (Table 1) clearly show the relatively benign clinical course of MTC: Only 1 patient has died during a mean follow-up of 81 mo (range, 17–379 mo) in the group with a definitive sign (hypercalcitoninemia) of metastatic disease.
DISCUSSION
Postoperative elevated or rising calcitonin and CEA levels often prompt the search for residual or recurrent MTC tissue. Conventional imaging methods (CT, MRI, and 131I-MIBG scintigraphy) frequently fail to reveal these tumorous lesions, because each modality has its own limitations.
In this study, we compared the findings of conventional diagnostic imaging with those of 18F-FDG PET in the investigation and restaging of MTC. Although CT and MRI detected a higher percentage of pulmonary and hepatic metastases than did 18F-FDG PET, 18F-FDG PET was superior in detecting lymph node involvement. We succeeded in identifying metastatic lymph nodes in all but 2 investigated MTC patients with elevated plasma tumor marker levels, and the number of detected lesions was higher than that found with any of the other conventional methods. In addition, the lack of attenuation correction probably decreased the tumor detection rate of PET, especially for the smaller tumors.
Lymph nodes in the cervical and mediastinal regions represent the first lymphatic levels of thyroid cancer. The lower number of involved cervical lymph nodes is explained by the fact that cervical dissections had been performed previously in many cases. Nevertheless, the number of involved cervical lymph nodes identified postsurgically seems surprisingly high, indicating the predominantly incomplete nature of the cervical dissections in the investigated group. This strategy is far from optimal. Prevalently systematic (cervical and mediastinal) lymph node dissection would help to avoid the early serious consequences (e.g., compression symptoms) of centrally located lymph node metastases. Our results indicate that MTC patients with an elevated calcitonin level during the follow-up display foci with a high tracer accumulation in at least one of the lymphatic regions (38/40 [95%]). This finding is in keeping with a reported lymph node metastasis incidence of 94% in hypercalcitoninemic patients after primary therapy (36).
In our study, small pulmonary metastases (<1 cm) detected by CT (and MRI) were not visualized by 18F-FDG PET. Data in the literature indicate a low sensitivity of 18F-FDG PET for small pulmonary metastases (27,29). A helical CT scan of the lung is therefore recommended if pulmonary metastasis is suspected.
Although this study detected metastases in all but 2 patients, a mismatch between the serum calcitonin level and the detected mass was found in many cases. The probable explanation for this mismatch was addressed by Ésik et al. (37), who reported a near-total prevalence of small hypervascular hepatic metastases in these cases. Our follow-up data (35 patients with angiographically proven hepatic metastases, of whom only 7 had positive PET findings for the liver) support this observation.
With 131I-MIBG scintigraphy, only 3 of the 40 patients investigated had positive scan findings. The limited uptake of this tracer indicates the poor and questionable diagnostic value of this method for the detection of recurrent MTC.
The results of this study lead us to recommend 18F-FDG PET examinations of MTC patients with postoperative elevated plasma tumor marker levels to select patients for secondary surgical intervention. If many lymph nodes are involved, a conservative approach (e.g., external irradiation) may be chosen as the appropriate treatment (38). Meticulous dissection is recommended in cases of limited dissemination or if some of the lymph node localizations are unfavorable (39). These centrally located metastatic lymph nodes in the neck and upper mediastinum represent metastases that may seriously affect the quality of life (39,40).
CONCLUSION
Our results indicate that 18F-FDG PET investigation is a highly sensitive method for the detection of metastases in MTC patients with elevated tumor marker levels. Its sensitivity surpasses that of other imaging procedures, especially in the localization of cervical and mediastinal lymph node involvement.
Acknowledgments
This study was supported in part by grant 219/2000 from the Scientific Health Care Council and grant T-29809 from the National Scientific Research Fund.
Footnotes
Received Feb. 16, 2001; revision accepted Aug. 20, 2001.
For correspondence or reprints contact: Szabolcs Szakáll, MD, PET Center, University of Debrecen, Nagyerdei körút 98, H-4012 Debrecen, Hungary.
E-mail: szakall{at}pet.dote.hu
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Secretive and proliferative tumor profile helps to select the best imaging technique to identify postoperative persistent or relapsing medullary thyroid cancer
- The impact of 18F-FDG PET/CT on assessment of nasopharyngeal carcinoma at diagnosis
- Diagnostic Accuracy of 18F-FDG PET in Restaging Patients with Medullary Thyroid Carcinoma and Elevated Calcitonin Levels
- Clinical Role of 18F-FDG PET/CT in the Management of Squamous Cell Carcinoma of the Head and Neck and Thyroid Carcinoma