


Abstract
The concept of sentinel lymph node biopsy in breast cancer surgery relates to the fact that the tumor drains in a logical way through the lymphatic system, from the first to upper levels. Therefore, the first lymph node met (the sentinel node) will most likely be the first to be affected by metastasis, and a negative sentinel node makes it highly unlikely that other nodes are affected. Because axillary node dissection does not improve prognosis of patients with breast cancer (being important only to stage the axilla), sentinel lymph node biopsy might replace complete axillary dissection to stage the axilla in clinically N0 patients. Sentinel lymph node biopsy would represent a significant advantage as a minimally invasive procedure, considering that, after surgery, about 70% of patients are found to be free from metastatic disease, yet axillary node dissection can lead to significant morbidity. Furthermore, histologic sampling errors can be reduced if a single (sentinel) node is assessed extensively rather than few histologic sections in a high number of lymph nodes per patient. Although the pattern of lymph drainage from breast cancer can be variable, the mammary gland and the overlying skin can be considered as a biologic unit in which lymphatics tend to follow the vasculature. Therefore, considering that tumor lymphatics are disorganized and relatively ineffective, subdermal and peritumoral injection of small aliquots of radiotracer is preferred to intratumoral administration. 99mTc-labeled colloids with most of the particles in the 100- to 200-nm size range would be ideal for radioguided sentinel node biopsy in breast cancer. Lymphoscintigraphy is an essential part of radioguided sentinel lymph node biopsy because images are used to direct the surgeon to the site of the node. The sentinel lymph node should have a significantly higher count than that of background (at least 10:1 intraoperatively). After removal of the sentinel node, the axilla must be reexamined to ensure that all radioactive sites are identified and removed for analysis. The sentinel lymph node should be processed for intraoperative frozen section examination in its entirety, based on conventional histopathology and, when needed, immune staining with anticytokeratin antibody. The success rate of radioguidance in localizing the sentinel lymph node in breast cancer surgery is about 94%–97% in institutions where a high number of procedures are performed and approaches 99% when combined with the vital blue dye technique. At present, there is no definite evidence that negative sentinel lymph node biopsy is invariably correlated with negative axillary status, except perhaps for T1a-b breast cancers, with a size of ≤1 cm. Randomized clinical trials should elucidate the impact of avoiding axillary node dissection on patients with a negative sentinel lymph node on the long-term clinical outcome of patients.
- sentinel lymph node
- breast cancer
- radiocolloid
- interstitial administration
- lymphoscintigraphy
- intraoperative γ-probe guidance
Questioning lymph nodes that drain areas of neoplasia is becoming standard practice in the staging of patients with cancer. The rationale for this practice was observed in 1907 when Jamieson and Dobson (1) described the significance of neoplastic cells initially spreading to the so-called primary gland. The term “sentinel node”—that is the first lymph node encountered by lymphatic vessels draining a tumor—was coined in 1960 by Gould et al. (2) for cancer of the parotid gland. The value of lymphatic mapping was highlighted in 1977 by Cabanas (3) with his studies of patients with penile cancer. Cabanas reported that the 5-y survival was 90% in patients in whom histology failed to show metastatic disease in the so-called sentinel lymph node (which he erroneously believed to be found always in a fixed anatomic location), whereas it was 70% when the sentinel node alone was metastatic, 50% when the sentinel node and other inguinal nodes were involved, and still lower (20% at 3 y) when iliac nodes were also involved. Therefore, he concluded that, when biopsy of the sentinel lymph node is negative for metastatic disease, no further surgical therapy is immediately indicated.
At approximately the same time, external lymphoscintigraphy was applied to lymphatic mapping in patients with truncal primary melanomas located in areas where lymphatic drainage was ambiguous (e.g., the midline of the back and the periumbilical region) (4). At that time, lymphatic mapping of the internal mammary chain was performed on patients with breast cancer to assist in the planning of external radiotherapy after surgery (5).
Thus, the extensive body of knowledge available today not only builds on experience of pioneers in the sentinel lymph node concept, such as Cabanas in penile cancer (3), but also can be traced back to much earlier observations on the lymphatic spread of some solid epithelial tumors, such as gastric cancer, parotid cancer, cutaneous melanoma, breast cancer, and vulvar cancer (6–14). Therefore, the concept of the sentinel node mapped by scintigraphy clearly fits well with the clinical experience of those working on many types of cancer.
Clinical practice, at present, uses lymphatic mapping with either vital dyes and direct vision at surgery or radiopharmaceuticals for scintigraphic mapping with a gamma camera and intraoperative identification of sentinel lymph nodes (using a specially built probe) on patients with tumors such as cutaneous melanoma (15–18) and breast cancer (19,20).
Although most human carcinomas are resectable when first diagnosed (thus being potentially curable by surgery alone), the long-term prognosis of patients is reduced if early metastatic spread to the regional lymph nodes is found. Unfortunately, recurrence in a lymph node is often the first sign that metastasis has occurred (21,22). Identification of lymphatic spread at the time of initial treatment planning now plays a pivotal role in staging the cancer because lymphatic metastases mean that treatment with local therapy alone is likely to fail. The patient must be offered either regional or systemic adjuvant therapy.
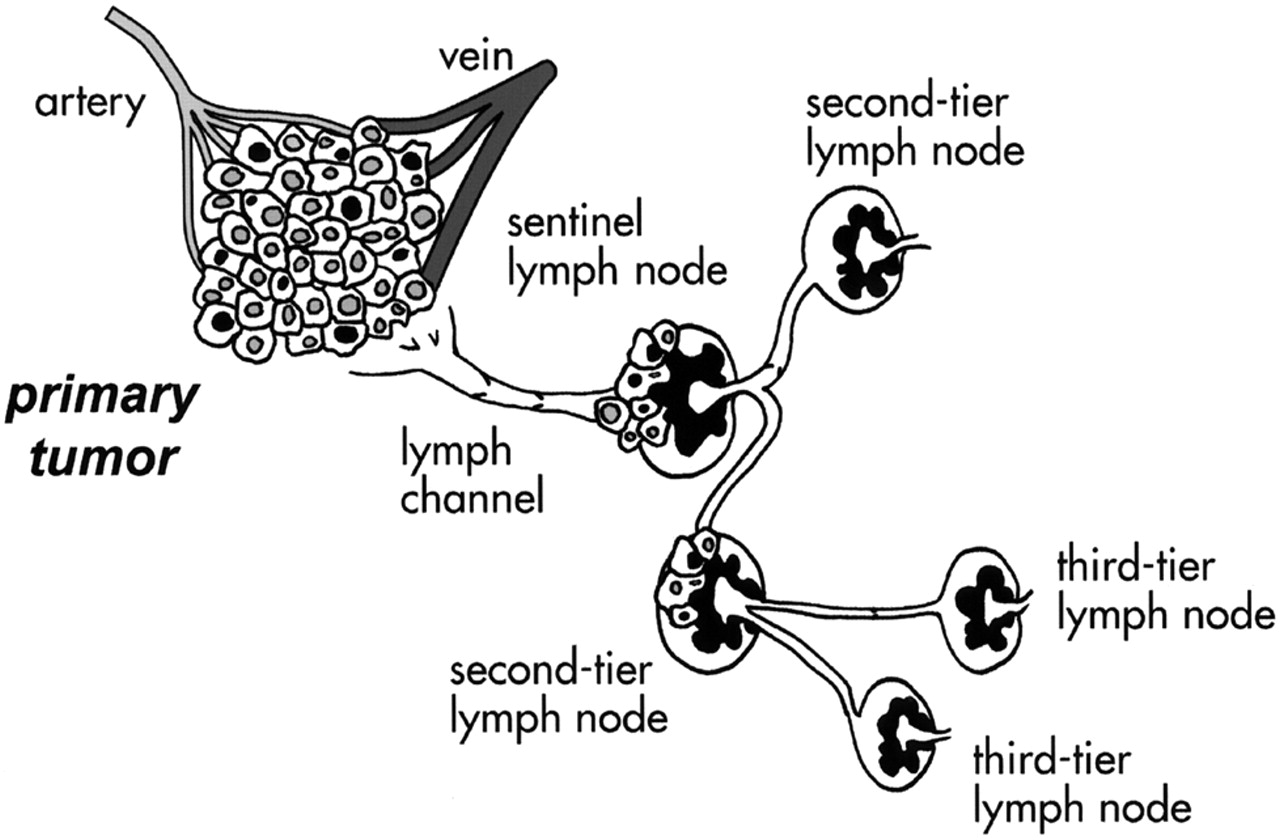
The concept of the sentinel lymph node is intimately embedded in the notion that, as a consequence of the orderly pattern of lymph flow, metastatic spread of solid tumors through the lymphatics follows a predictable pattern (23). On the basis of this assumption, performing a histologic evaluation of the sentinel lymph node (the first node on the direct lymphatic pathway draining from the primary tumor) increases the likelihood of detecting metastasizing tumor cells (Fig. 1). The tumor status of the sentinel node should accurately predict the histopathologic status of the regional lymphatic basin draining the tumor; in particular, a sentinel lymph node free from tumor metastasis would exclude tumor spread to the at-risk regional lymphatic basin. Although it is possible for there be a negative sentinel lymph node with metastatic involvement of a second-tier node, this occurrence is very rare, especially when the primary tumor is in an early stage of growth. Therefore, in most patients the sentinel node concept remains valid.

Schematic conceptualization of sentinel lymph node. Being first node encountered by lymph draining from primary tumor, sentinel lymph node should be site where clusters of tumor cells migrating through lymphatic channels are most likely to be entrapped and possibly proliferate before widespread tumor dissemination in body. Second-tier (or second-echelon) lymph nodes receive lymph (and possibly tumor cells) from sentinel lymph node and in turn drain lymph toward third-tier lymph nodes.
The following sections address the main issues concerning application of the sentinel lymph node concept to breast cancer. Whereas biopsy of the sentinel lymph node is already the standard of good clinical care for patients with melanoma, debate is still open as to whether the same should also apply to patients with early breast cancer (24).
CLINICAL PROBLEM
The so-called TNM system, which considers the size of the primary tumor (T), the tumor status of regional lymph nodes (N), and the presence of distant metastases (M) to characterize cancer patients, represents today the fundamental triad for prognostic staging in patients presenting with breast cancer (25,26).
Although current imaging techniques can define parameter T and parameter M in patients with newly diagnosed breast cancer, their diagnostic yield is unacceptably low (or not cost-effective) for predicting parameter N in patients with a negative clinical examination. The low negative predictive value of various instrumentation or tumor targeting agents (magnetic resonance, γ-scintigraphy, and PET) is particularly worrisome when staging cancer patients.
Mammographic screening procedures result in early detection of breast cancer, when the tumor is around 1 cm in diameter (27,28) and the probability of axillary metastasis is relatively low (20%–30%) (29–35). A negative axilla at clinical examination has a poor predictive value concerning cancer involvement of lymph nodes; therefore, histologic examination of any nodes is important in identifying metastatic involvement. Unfortunately, this implies the risk of some significant side effects, resulting, for example, from axillary node dissection. These considerations explain the ongoing debate about whether to routinely perform axillary dissection in breast cancer (36–41), which still represents the standard surgical treatment for breast cancer irrespective of tumor size.
The 20%–30% likelihood of axillary nodal metastases in early breast cancer (T1a-b, tumor size, ≤1 cm), which rises to 30%–40% when including also patients with T1c cancer (size, 1–2 cm), has maintained axillary node dissection as part of the staging procedure in patients with a clinically negative axilla (42). Regrettably, axillary dissection is associated with a relatively high incidence of immediate and late postsurgical complications, especially lymphedema and sensory-motor disturbances. Because these occur in many patients who are found to have no nodal disease after surgery, these distressing outcomes fuel the debate on routine axillary node dissection in all patients with breast cancer (43–45).
Furthermore, thorough histologic evaluation of 15–20 lymph nodes is impossible in standard clinical care. A limited number of histopathologic sections (3 per lymph node at most) is usually examined; thus, it is possible to miss small areas of cancer and to misclassify patients as tumor free versus those having metastatic disease (46,47).
Moreover, the benefit of adjuvant chemohormonal therapy in breast cancer appears to be independent of the axillary lymph node status (48–51). Thus, adjuvant therapy is used in patients with metastatic disease as well as in patients with nonmetastatic axillary nodes if the latter have at least 1 risk factor (tumor size, >2 cm; histologic grade, G2–3; negative receptors for steroid hormones). In this regard, new biologic markers are being explored as prognostic indicators in breast cancer (52,53).
Although the presence of nodal disease makes an important difference, the number of metastatic axillary lymph nodes is virtually of no value in the choice of the routine therapeutic regimens (50,54). Thus, the choice of adjuvant therapy in early breast cancer is not significantly affected by the number of axillary nodes involved but, rather, by whether there is involvement. The therapeutic value of axillary node (or internal mammary node) dissection is questionable in patients whose disease is clinically N0 at the time of primary surgery for breast cancer (30,55–63). In fact, prophylactic axillary dissection does not achieve significant advantages as to incidence of first recurrence and of distant metastases versus axillary dissection performed when lymph node involvement becomes clinically apparent. Furthermore, there is only a marginal benefit in terms of overall survival (4.7%, with 95% confidence intervals = 1.9%–7.5%; P < 0.01) (64,65).
Focusing on just 1 or a few sentinel lymph node(s) for extensive histologic evaluation increases the accuracy of histopathologic staging of the axilla in patients with breast cancer (47,66,67). Thus, the availability of a minimally invasive procedure for defining axillary node status in patients with early breast cancer whose disease is clinically N0 is particularly attractive to surgeons and to patients. Randomized clinical trials should provide the definitive answer as to whether avoiding axillary dissection in breast cancer patients with a negative sentinel node will maintain today’s parameters concerning locoregional control of the disease, tumor recurrence, and overall survival. In such condition, radioguided surgical biopsy of the sentinel lymph node might actually become the new acknowledged standard of clinical care for patients with early breast cancer.
ANATOMY AND PHYSIOLOGY OF LYMPHATIC SYSTEM AS IT RELATES TO BREAST CANCER
The lymphatic system drains water, low-molecular-weight solutes, protein macromolecules, cell fragments, and inflammatory cells from the interstitial space, ultimately returning the fluid components to the vascular space (68–70). The lymphatic system originates embryologically in the cervical region near the outflow from the heart, in the form of separate puddles of lymph devoid of red blood cells. These lymph puddles coalesce and follow the progressive growth of arteries toward the periphery (71,72). Lymphatic channels form as buds from venous structures, a common embryologic origin that creates the potential for lymphovenous anastomoses under conditions of increased lymph pressure and flow (73,74).
Lymphatic vessels of the breast tend to accompany the routes of blood supply, represented mainly by the axillary and internal mammary vessels, with a minor contribution from the lateral perforating branches of the intercostal branches. Thus, distribution of lymphatic drainage from the breast is approximately proportional to the 3 routes of blood supply: Most of the lymph drains to the axillary lymph nodes. About 3% drains to the parasternal, internal mammary chain nodes, whereas under normal circumstances the posterior intercostal lymph nodes receive a very small proportion of lymph flow from the breast (75).
Because of its embryologic origin in the ectoderm, the mammary gland is, in a sense, an organ of the skin; therefore, its lymphatic drainage mostly parallels lymph flow from the overlying skin. In fact, the breast is situated between the lymphatics of the overlying dermis and the deep lymphatic collectors of the underlying fascial plane, being intimately connected with both sets of lymphatic structures (76) (Fig. 2). Lymph from the skin covering the mammary gland drains to a tenuous, diffuse subcutaneous plexus located between the skin and the superficial fascia. An extensive lymphatic plexus around each lobule of the mammary gland follows the path of the galactophore ducts (periductal plexus), converging to the areola to form Sappey’s subareolar plexus, which is part of the general subcutaneous plexus. The subcutaneous plexus and the deep fascial plexus communicate efficiently along fibrous strands transversing the breast, through a system of lymphatic vessels equivalent to those that connect the subcutaneous plexus and the deep fascial plexus elsewhere (77). In the skin, communicating lymphatic vessels between the superficial plexus and the subcutaneous plexus follow fibrous strands about 1 mm apart from each other; in the breast, they are located in the perilobular space, being spaced up to 8 mm from each other in the nonlactating breast (78).

(A) Schematic representation of structure of cutaneous blood and lymph vessels. For simplicity, blood and lymph vessel networks (which are intimately embedded in each other) are represented separately on left (red and blue) and on right (yellow). Embryologic origin in ectoderm places mammary gland in ideal space between subcutaneous plexus and deep lymphatic collectors (emphasized in figure). Each branch of periductal plexus drains lymph mostly toward skin surface (through subareolar plexus), whereas minor component drains toward deep collectors (draining in turn toward internal mammary chain). Radiocolloids injected intradermally over mammary gland drain to subcutaneous plexus, which is also terminal pathway of predominant lymph drainage from mammary gland. (B) Schematic representation of pathways of lymphatic drainage from mammary gland (modified from (150)). Most lymph produced in mammary gland surfaces at subareolar plexus, then merges with subcutaneous plexus of overlying skin, and flows with centrifugal pattern mostly toward axilla. Lymph from deeper portion of gland drains either through same pathway or through deep lymphatics to reach parasternal, internal mammary chain (and even contralateral side). abdom. = abdominal.
Under physiologic conditions of lymph flow and pressure, unidirectional valves in the communicating vessels drive lymph from the deep fascial plexus toward the subcutaneous plexus (75). Most of the lymphatic drainage from the mammary gland surfaces at Sappey’s subareolar plexus, merging with the subcutaneous plexus of the overlying skin, which in turn drains to the anterior or to the pectoral group of axillary lymph nodes. A minor component of lymph drainage (almost exclusively for the deeper portion of the mammary) occurs through the deep fascial plexus located within the fascia overlying the pectoral muscles. This lymph can drain either through the periductal plexus as described or directly to lymph nodes of the internal mammary chain (or both) through the deep lymphatic collectors (79).
Complex architecture deriving from common embryologic origin explains why most of the mammary gland and of overlying skin can be considered as a single biologic unit sharing a common centrifugal lymphatic pathway to the same axillary nodes (80) (Fig. 2). However, certain lymphatic vessels from the lateral portion of the gland drain to lymph nodes of the pectoral group, whereas part of the medial portion of the breast drains to nodes of the internal mammary chain (and to lymphatics of the opposite gland), part of the lower portion of the breast drains to the lymphatic system of the abdominal wall, and, finally, part of the upper portion of the gland drains to the apical axillary lymph nodes and to the deep cervical nodes. These patterns of lymphatic drainage are very variable and it is impossible to predict the route of drainage of any particular tumor on the basis of the location of the tumor within the breast.
In general, epithelial cancers do not have an efficient lymphatic system of their own. Tumor lymphangiogenesis is grossly dysplastic, exhibiting some or all of the following patterns: Prelymphatics do not link with lymphatics, basal lamina and flattened endothelium are inconsistent and often incongruous, and interconnection of stroma with blood vessels and lymphatic structures is often abnormal (72). This makes the use of intratumoral injections less logical than that of peritumoral or subdermal injections.
Although tumor-produced angiogenic factors have definitely been linked to tumor growth (81–83), to our knowledge, no similar growth factors have been identified for the lymphatic system. Debate is still open on some lymphangiogenic activity of the vascular endothelial growth factor in tumors (84–86).
The origin and drainage of lymphatics in the breast are relevant to the technique of injection of the radiopharmaceutical for lymphoscintigraphy and for radioguided biopsy of the sentinel lymph node. Experimental evidence emphasizes either the absence or inefficiency of structured lymphatic drainage from most solid tumors, including breast cancer. The interstitial fluid leaving the tumor bed has to follow the lymphatic spaces and pathways of the normal tissues surrounding the tumor. In particular, radiolabeled colloids injected intratumorally will drain through lymphatic channels encountered after percolating out from the tumor space to the surrounding parenchyma; obviously, such percolation is facilitated when the volume of the injectate is relatively large with respect to the tumor volume.
RADIOPHARMACEUTICALS
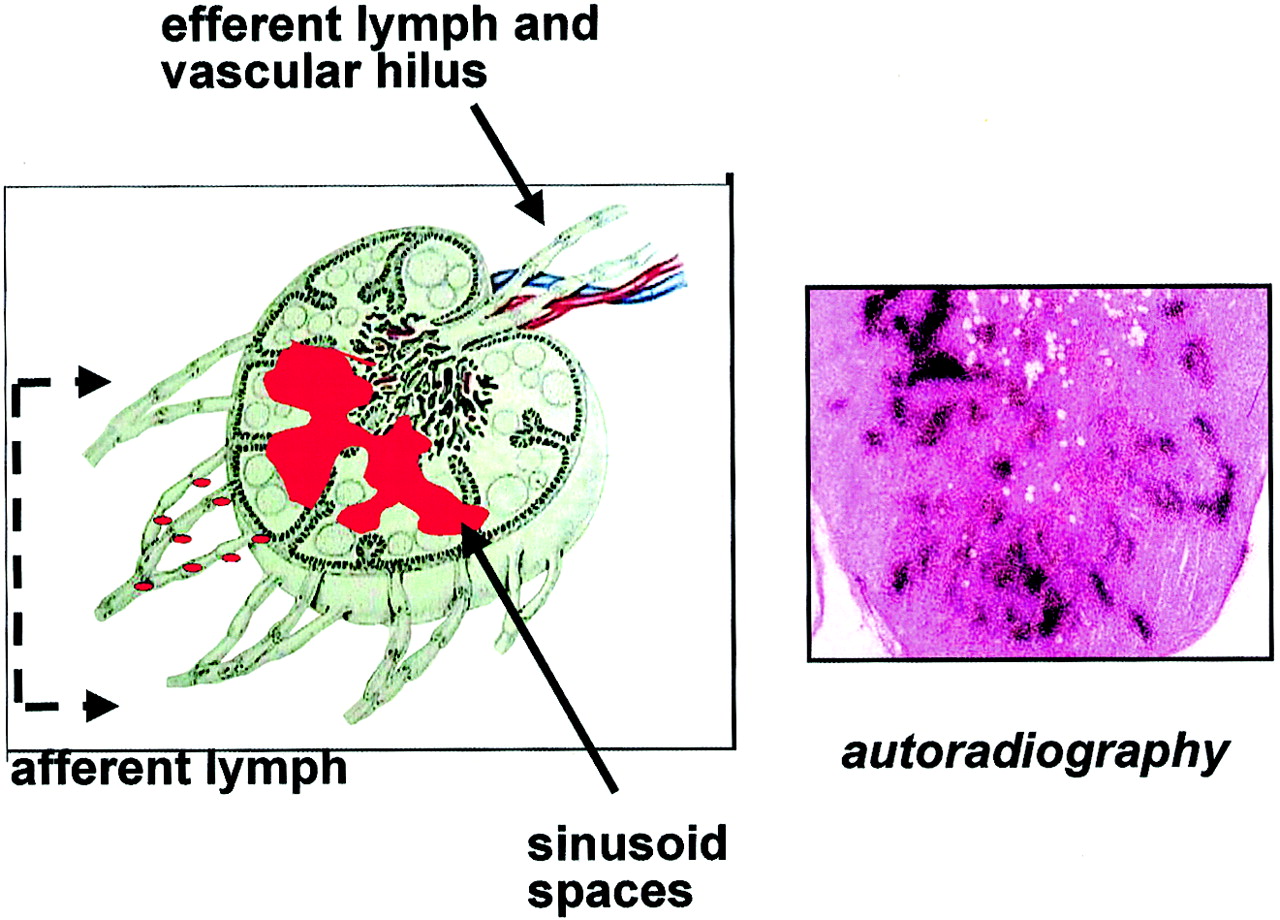
In radioguided surgery for sentinel lymph node biopsy, the radiopharmaceutical should fulfill at least the following criteria: visualize the lymphatic channels leading from the site of interstitial administration to the corresponding lymph node and be preferentially retained in the first lymph node(s) encountered. Intranodal retention is associated with the macrophages lining the sinusoid spaces of lymph nodes, whose main function is to clear the affluent lymph of particulate matter, based on active, saturable phagocytosis (87) (Fig. 3).

(Left) Red dots symbolize radiocolloids migrating with afferent lymph from site of interstitial injection to lymph node, where they are entrapped by macrophages lining sinusoid spaces (red area). (Right) Low-magnification histoautoradiograph of sentinel node removed about 20 h after injection of 99mTc-HSA nanocolloid. Black dots (silver grains) show retention of radioactive agent in sinusoid spaces. (Hematoxylin–eosin, about ×8)
When there is massive nodal metastatic involvement, few normal cells remain in the node, the biologic clearing mechanism is lost, and the node is not visualized during lymphoscintigraphy. Interstitial injections of specific tumor-seeking radioactive tracers to overcome this problem have shown disappointing results (88).
For colloidal particles ranging in size from 2.5 to 1,000 nm, the general prerequisites for uptake by macrophages are a net negative surface charge and preliminary opsonization of such micellar compounds by a class of compounds that includes complement components C3, C4B, and C5 and some α- and β-globulins (89,90). These properties are shared by several formulations, either inorganic (198Au-colloid, 99mTc-antimony sulfide, 99mTc-sulfur colloid, 99mTc-stannous fluoride, 99mTc-rhenium sulfide) or derived from biologic substances (nano- or microcolloid of human serum albumin [HSA]).
Opsonization may occur in plasma or in the lymph, as is the case when the tracer is injected interstitially. The opsonized material activates a membrane-bound receptor on macrophages, leading to phagocytosis. Efficiency of this clearing process varies with several factors besides the net surface charge and degree of opsonization, such as antigenic properties, size and number of the particles, specific anatomic region, and so forth. (87,91–95).
After interstitial injection, radioactive colloids are cleared by lymphatic drainage with a speed that is inversely proportional to the particle size. Distribution of the particle size within each radioactive colloid preparation is in general rather disperse (not always with a gaussian-type curve (92,96)) around the mean values indicated by the manufacturers (Table 1).
Approximate Ranges of Particle Size Estimated for Various Radiocolloids
Inconsistencies observed in the reported ranges of particle sizes (11,92,96–98) are associated with several factors, including the method used for the measurement, determination performed before or after radiolabeling, poor stability of the agent after labeling, incubation with serum, and use of regularly eluted (high concentration of 99mTc as a fraction of the total technetium in the eluate) versus technetium eluted after a long interval of ingrowth (low concentration of 99mTc as a fraction of the total technetium in the eluate) for labeling. Other factors can include the pore size of any filters used (as in the case of 99mTc-sulfur colloid), in-house modifications of the reconstitution procedures versus those recommended by the manufacturers, and so forth. (11,95).
Lymphatic drainage of radiocolloids injected interstitially proceeds over several hours, as small particles are drained first, followed by intermediate-size particles, whereas large particles may be retained virtually indefinitely at the injection site (Fig. 4). Thus, distribution of the particle size within each radiocolloid preparation is a major determinant of the kinetics of tracer clearance through lymphatic drainage for the different agents. Detailed information on the exact distribution in relation to the particle size range is scanty or not available at all, except perhaps for 99mTc-HSA nanocolloid and 99mTc-sulfur colloid (Table 1) because these 2 tracers (including various in-house modifications of sulfur colloid) are currently the most widely used radiocolloids for sentinel node biopsy.

(A) Time–radioactivity curves from region-of-interest (ROI) analysis after dynamic recording of lymphoscintigraphy performed by intradermal injection of 6 MBq (150 μCi) 99mTc-HSA nanocolloid; y-scale is arbitrary to plot all 3 curves within same order of magnitude. Injection site shows minimal reduction over 60 min, barely discernible from physical decay. Tracer appears in sentinel node starting few minutes after injection, with quasiplateau maintained over 60 min. Lymphatic channel shows early passage of radioactivity, continuing with quasipulsatile pattern. Direct supply of radiocolloid draining from injection site (continuing over several hours) keeps radioactivity content of sentinel node at relatively higher level than that of second- or third-tier nodes, even if active retention of tracer by macrophages is saturated. (B) Definition of 3 ROIs on representative frame set from dynamic recording: ROI 1 = injection site; ROI 2 = lymphatic channel; ROI 3 = sentinel node.
The amount of radioactivity retained in the sentinel lymph node(s) 15–18 h after interstitial injection of radiocolloid of intermediate particle size (colloidal albumin) is in general quite low. About 1% of the injected dose is retained per node when the tracer is injected subdermally in patients with breast cancer, with much smaller amounts being retained (0.1% of injected dose per node) when the tracer is injected in the peritumoral parenchyma (99). These figures compare well with data obtained similarly after intradermal administration in patients with cutaneous melanoma (0.36% of injected dose per node) (100). Earlier studies performed in an experimental rabbit model with radiocolloids with smaller particle size (198Au-colloid and 99mTc-antimony sulfur colloid) showed much higher uptake (5%–9% of injected dose per node) (101).
When radioactive agents for lymphoscintigraphic imaging were originally developed, emphasis was on fast visualization of lymphatic vessels rather than lymph nodes. Therefore, the range of particle size was generally skewed toward the lower end of the useful range for colloids—that is, >5 nm (particles <4–5 nm are quickly cleared from the injection site through the blood capillaries) (102) but <30–50 nm to ensure fast lymphatic drainage.
In our opinion, radiocolloids with most of the particle size ranging from 100 to 200 nm would represent the best compromise between the need for an efficient and fast lymphatic drainage (compatible with conveniently fast visualization of lymphatic pathways) and the need for satisfactory retention in the sentinel lymph node (compatible with subsequent delayed intrasurgical γ-probe use). As shown earlier (103), relatively small radiocolloids (<50 nm) visualize lymphatic vessels within a few minutes after interstitial injection and quickly progress to visualize second-tier or third-tier nodes as well (Fig. 5). Whereas larger radiocolloids (>300 nm) are preferentially retained in the sentinel lymph node, their slow migration from the injection site makes it more difficult to perform lymphoscintigraphy before the patient’s appointment in surgery. In a series of 240 patients evaluated with different injection techniques and tracers, the average number of lymph nodes visualized by radiocolloids with particle size reported between 15 and 50 nm was 2.1 ± 1.1, whereas the average number was 1.6 ± 0.8 for particles 5–100 nm in size and 1.3 ± 0.5 for particles 200–2,000 nm in size (99). Although radiocolloids with particle size in the “ideal” 100- to 200-nm range are not commercially available, experience acquired with current commercial preparations allows each group of investigators to gain reasonable confidence in the procedure with the agents available.

Scintigraphs obtained in right anterior oblique view 15 min after subdermal injection of radiocolloids with different particle size: 99mTc-sulfide (left), 99mTc-HSA nanocolloid (center), and special formulation of 99mTc-HSA microcolloid, not available commercially (151) (right). Even on early imaging, radiocolloids with small and intermediate particle size visualize several nodes in addition to sentinel node, whereas only sentinel node is visualized by radiocolloid with relatively large particles.
Three types of radiocolloid preparations are commonly used for lymphoscintigraphy combined with intraoperative γ-probe sentinel node identification. 99mTc-sulfur colloid is the most commonly used agent in the United States, either unfiltered (particle size, about 15–5,000 nm) or filtered. Different pore sizes (100 or 220 nm) have been proposed, with the goal of obtaining particles in the range of about 50–100 or 50–200 nm. Although some authors still claim the superiority of the unfiltered versus the filtered preparation (104,105), the prevailing trend now favors the routine use of filtered 99mTc-sulfur colloid for sentinel lymph node studies.
Most European investigators use 99mTc-HSA nanocolloid with particles between 4 and about 100 nm (95% of the particles < 80 nm). At present, this radiopharmaceutical offers the best range of particle size, approaching the ideal range, and offers the additional benefits of instant labeling at room temperature and stability in vitro and in vivo.
99mTc-antimony trisulfide (3–30 nm) is commercially available in Australia and Canada, where it is widely used for sentinel lymph node procedures. Finally, although the average particle size of 99mTc-rhenium sulfide is reported by the manufacturer to be about 100 nm, this agent actually has a trimodal distribution in particle size: about 40 nm (8% of the particles), 440 nm (61%), and between 650 and 2,200 nm (31%) (96).
The number of particles injected is another important parameter in radioguided sentinel node procedures. Only a small fraction of the colloidal particles is actually radiolabeled in the tracers prepared by current standard methods. For instance, in 99mTc-HSA nanocolloid, only about 5% of the particles are tagged with 99mTc (R. Franceschini, Nycomed-Amersham-Sorin, Saluggia, Italy; personal communication, March 1999): Refining the radiolabeling technique to increase considerably this fraction should be a priority of radiochemistry in this field. In fact, the clearing function of lymph nodes is not based on mere mechanical filtration depending on size of the particles; rather, it is a biologic trap mechanism based on active phagocytosis by macrophages. Because it can be assumed that the clearing capacity of each node is saturated rather quickly, the higher is the number of particles arriving to the draining lymph node, the sooner macrophages are saturated and particles progress to serially visualize subsequent echelon nodes. In this regard, radioguided identification of the sentinel node requires administration of a radioactive dose high enough to allow detection based on counting rates, for external imaging and intraoperative localization. The specific activity of the preparation is important to administer a preparation with the fewest particles. Therefore, methods of high specific activity labeling should be sought.
TECHNIQUES
Tracer Injection
At least 3 main parameters define the optimal technique(s) of administering the radiopharmaceutical for lymphatic mapping and sentinel node biopsy in breast cancer surgery: site of injection, volume of the injectate, and dose injected. An additional parameter is timing of injection relative to surgery, though with lesser importance in the overall procedure. Criteria for defining the optimal combination of these parameters partly overlap each other; site of injection is the most crucial parameter, which heavily affects the final choice of the other 2 main parameters, volume and dose.
Advocates of intratumoral injection (an extension of the technique developed earlier for intraoperative lymphatic mapping with vital blue dye) argue that this is the best site to inject to visualize lymph drainage from the tumor. Common corollaries of the intratumoral route are a relatively large volume of the injectate (at least 4 mL, which easily percolates out of the tumor mass especially for T1 breast cancers) and a relatively high injected dose of radiocolloid (about 37–370 MBq [1–10 mCi]). The purpose of injecting a large volume is to increase intratumoral pressure (which is higher than in the surrounding normal tissues because of the abnormal lymphatic system in the tumor) to force lymph flow from the tumor, thereby enhancing the likelihood of visualizing the lymphatic pathways and draining node(s). A high dose is required because the fraction of radiocolloid injected intratumorally that leaves the tumor through this paraphysiologic lymphatic drainage is minimal (because of the virtual absence of a lymphatic system within the tumor). The introduction of a large volume can lead to distortion of tissues and lymphatics and, therefore, have an unpredictable effect on radiocolloid clearance.
Drawbacks of direct intratumoral injection include the following: (a) The tumor is intrinsically devoid of an organized lymphatic system of its own. (b) Large volumes of the injectate may alter the physiology of lymph drainage from the tumor, thus increasing the risk of visualizing nonsentinel nodes. (c) Even 18–24 h after intratumoral injection, the large fraction of the injected dose retained virtually indefinitely within the tumor may interfere with imaging, either by scatter or shine-through. Scatter is a major problem with intraoperative γ-probe identification of a sentinel node located close to the tumor, an occurrence observed in >25% of all patients with breast cancer (8). (d) Scintigraphic visualization of the draining lymphatics and lymph nodes is usually very slow (requiring several hours for a thorough scintigraphic study). (e) Possible spreading of tumor cells along the needle track (however low the likelihood of such an occurrence might be) is a concern to patients and to investigators, though often this area is removed at surgery, at least for superficial cancers.
Most investigators currently favor interstitial administration of radiocolloids through the extratumoral route for sentinel node biopsy. At this time, 2 approaches to extratumoral radiocolloid administration are used: the peritumoral, intraparenchymal injection technique and the intradermal–subdermal injection technique.
With intraparenchymal administration, the tracer is injected in a site immediately adjacent to the tumor, in the space with a supposedly normal lymphatic system that is the only possible drainage pathway for fluids, particles, and cells leaving the tumor through the extravascular route. In this approach, the radiocolloid is given in 4–6 deposits around the tumor circumference. Each aliquot is about 0.5–1 mL and contains 7–18 MBq (0.2–0.5 mCi) 99mTc-labeled colloid. Although injections are directed simply by palpation in most centers, it is advisable to inject the tracer under sonographic guidance (or stereotactic devices) within about 2 mm from the tumor periphery. As with the other 2 approaches (intratumoral and subdermal–intradermal), 25-gauge or even 27-gauge needles are commonly used for injection, the only difference being the length of the needle bore according to depth of the injection.
Radiocolloids injected in the mammary parenchyma tend to visualize the lymphatic drainage pathway and nodes faster than radiocolloids injected intratumorally. Nonetheless, although this is not the norm, completing a lymphoscintigraphic study can still require up to 3–4 h, especially on patients with large breasts or on postmenopausal women; slow lymphatic clearance in the latter condition possibly reflects the physiologically reduced lymph flow in the aging mammary parenchyma. The use of gentle massage for 2–3 min after injection may aid clearance of radiocolloids, possibly by breaking up the injected bolus.
Irrespective of the quadrant where the primary tumor is located, the peritumoral, intraparenchymal route of radiocolloid injection results in a high rate of visualization of internal mammary sentinel nodes, which is described in an average 20% of the patients, with a maximum of about 30% reported by Alazraki et al. (11). Although the long-term clinical impact of identifying pathways of lymphatic drainage to the internal mammary chain in patients with early breast cancer is still unclear, this finding is a definite plus of the peritumoral administration route when one compares its merits with those of the subdermal–intradermal injection technique. Some sentinel nodes can also be detected within the breast parenchyma, in between the pectoralis muscles, and in the supraclavicular fossa.
The likelihood of visualizing a lymphatic duct and a draining node increases when the radiocolloid is injected in the skin overlying the mammary gland; as a matter of fact, vast experience acquired with hundreds of lymphoscintigraphic studies (G. Paganelli, unpublished data, December 2000) clearly indicates that lymphatic drainage of radiocolloids from the skin is richer and faster than drainage from the resting breast parenchyma (106). Therefore, axillary sentinel lymph nodes can be efficiently visualized as early as 20–30 min after intradermal injection of radiocolloid, thus making the entire lymphoscintigraphic procedure highly practicable.
Nevertheless, convenient timing is not the only factor that makes the intradermal administration route such an attractive option for sentinel lymph node biopsy in early breast cancer. Reliability of this approach for sentinel node identification has a sound anatomic and physiologic basis. Because of the common embryologic origin in the ectoderm, the mammary gland and the overlying skin can be regarded as a single biologic unit whose pathways of lymphatic drainage are intimately embedded in each other (Fig. 2). In particular, the subcutaneous plexus is the common draining system for lymph produced in the dermis (which is the site where radiocolloid is injected) and for most of the lymph produced in the mammary gland. Lymph collected by the periductal plexus converges in the subareolar plexus, which in turn merges in a centrifugal manner with the subcutaneous plexus. Clearly, a radiocolloid injected intradermally or subdermally will less likely drain toward the deep fascial lymphatic collectors to visualize the internal mammary chain, unless the regional pattern of lymph flow is disrupted by some paraphysiologic mechanism(s), such as change of flow direction associated with, for instance, metastatic involvement of the more superficial pathways of lymphatic drainage or prior surgery that may have altered the pathways of lymph flow.
Using this administration approach, a small volume of tracer (0.15–0.3 mL containing 10–20 MBq [0.3–0.6 mCi] 99mTc-colloid) is injected as a single aliquot in the skin directly overlying the tumor. On the basis of how deep injection is performed, tracer administration is defined as intradermal when the needle is almost tangent to the skin surface and a classical urticarial pomphus develops; when, instead, injection is a little deeper (this occurrence is signaled by reduced resistance to penetration of the needle), the pomphus is less obvious and administration is defined as subdermal. Some overlap occurs between these 2 modalities and the 2 terms are often used interchangeably, also because of wide variations in thickness of the skin overlying the breast.
Some investigators perform periareolar tracer injection (usually 4 aliquots) as a modification of the subdermal route; however sound its pathophysiologic basis may be (because of rich connections of the subareolar plexus with the general subcutaneous plexus), we do not favor this technique, also because it causes some discomfort to patients. This approach may also reveal sites of drainage of the breast per se against specific drainage of the tumor.
Advantages of the intradermal–subdermal injection technique are represented by its high practicability with minimum training, small volume administered as a single injection, fast visualization of lymphatic drainage pathways, and low dose administered.
Some studies have compared the lymphoscintigraphic pattern and performance of sentinel node identification by adopting the intradermal approach and the peritumoral, intraparenchymal approach in the same patients (11,107–110). Although the 2 techniques are reported to yield virtually equivalent results in the vast majority of patients (107,108,110), some authors report a sizable proportion of discordant results concerning sentinel nodes either in the axilla or in the internal mammary chain (or both) (11,109). Perfect equivalence between the 2 approaches (111) requires further comparative studies and better understanding of the role of tumor status of the internal mammary chain nodes on therapy planning and on long-term outcome of patients. Although the incidence of metastatic involvement of internal mammary lymph nodes in patients with T1 breast cancer (up to 2 cm in diameter, possibly the optimal target for sentinel node biopsy) had been reported earlier to be about 15% (112), a much lower value has been reported more recently (about 2.7%) (113).
It is reasonable to assume that the 2 injection techniques, intradermal and peritumoral, are complementary (11) (Fig. 6). Another reasonable approach might be to inject the radiocolloid intradermally when a T1a-b tumor (≤1 cm in diameter) is located rather superficially in the breast and peritumorally in the case of larger tumors or tumors located deep within the mammary gland.
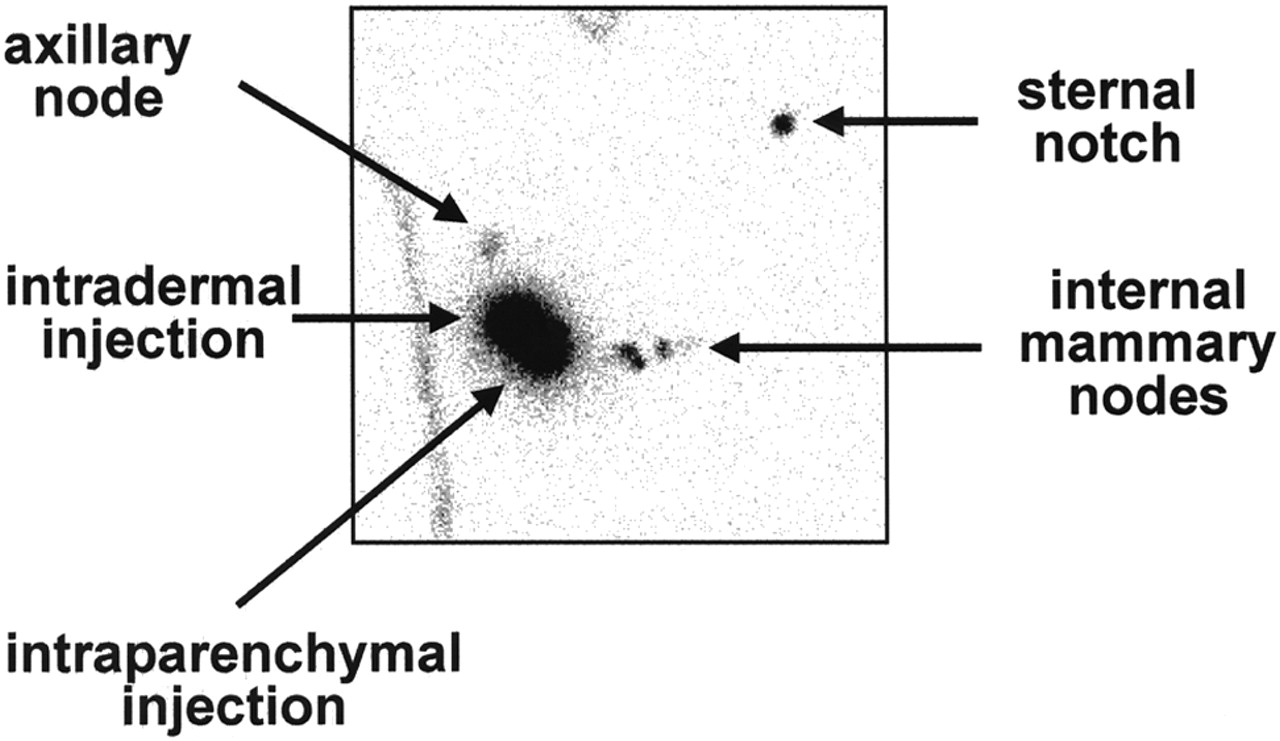
Scintigraph obtained in anterior view about 45–60 min after injecting 2 separate aliquots of 99mTc-HSA nanocolloid (about 7 MBq [200 μCi] each) intradermally and, 15 min later, intraparenchymally in right breast; contour of body in area under evaluation is identified with aid of radioactive point source. Intradermal injection ensures visualization of single sentinel lymph node between breast and axilla, whereas intraparenchymal injection visualizes lymphatic drainage toward internal mammary chain (at least 3 sequential lymph nodes).
Imaging and External γ-Probe Counting
Lymphoscintigraphy is an integral component of any procedure of sentinel lymph node biopsy in breast cancer surgery because it provides important information not available otherwise, such as possible lymphatic drainage toward the internal mammary chain, a pattern that would be undetected if relying only on intraoperative γ-probe counting (114). It is particularly helpful when visualizing more than a single sentinel node in the axilla to distinguish true additional sentinel nodes on different lymphatic pathways from second- and third-tier nodes (Fig. 7). Moreover, by providing accurate topographic coordinates preoperatively, lymphoscintigraphy enables the surgeon to focus attention on the correct spot in the axilla, thus shortening the surgical procedure and increasing the overall accuracy of sentinel node biopsy. This feature is especially appreciated when γ-probe guidance is complemented with the vital blue dye technique.
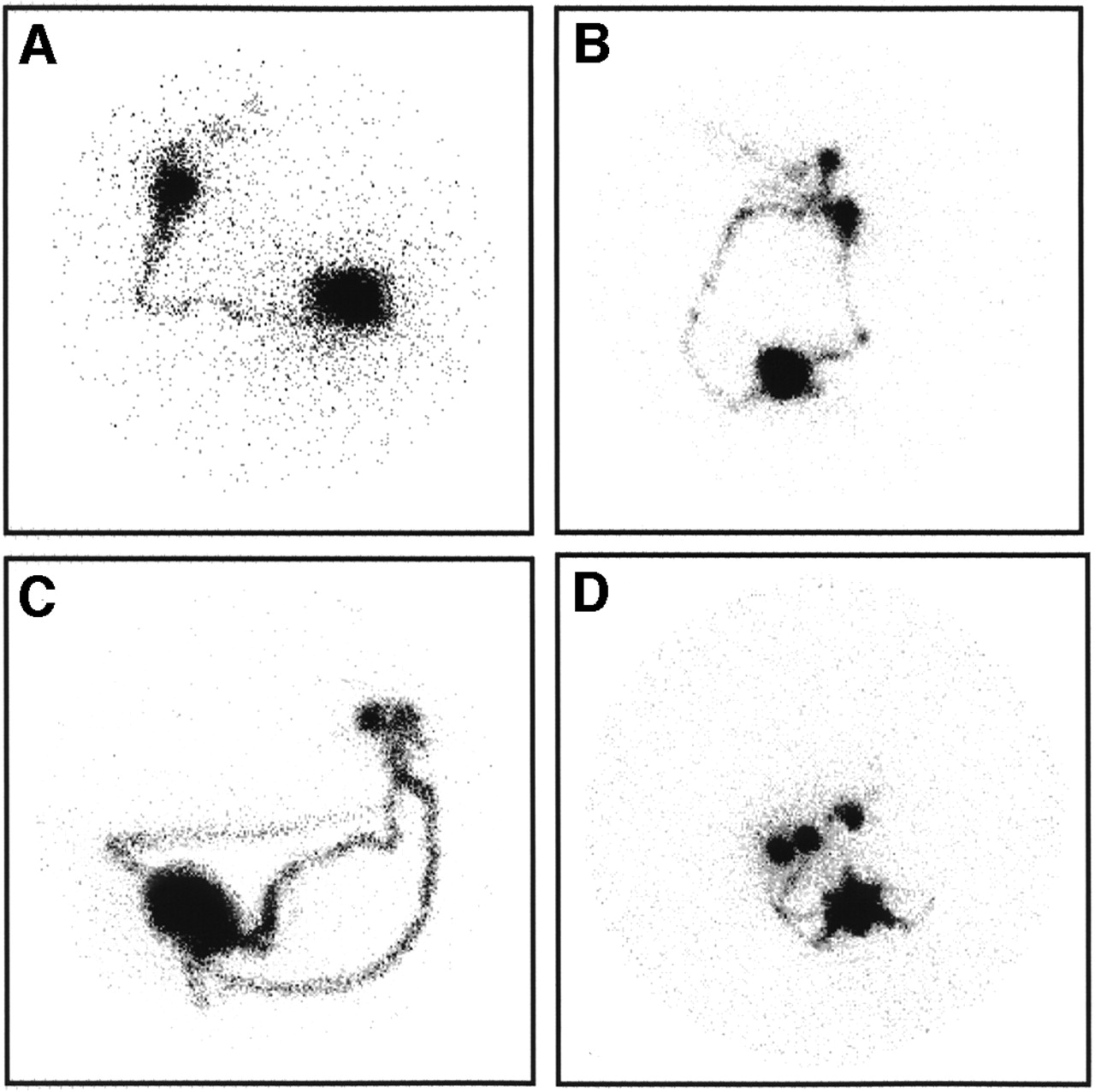
Representative scans illustrate variable patterns of lymphatic drainage that would not be discerned only by intraoperative γ-probe counting. Imaging times were between 30 and 60 min after intradermal injection of 99mTc-HSA nanocolloid. (A) Right anterior oblique (RAO) view shows single lymphatic vessel leading to single sentinel lymph node, with serial visualization of subsequent-tier nodes. (B) Left anterior oblique (LAO) view shows 2 separate lymphatics leading, through widely diverging pathways, to 2 separate but adjacent sentinel nodes (with serial visualization of subsequent-tier nodes). (C) LAO view shows 3 separate lymphatics leading, through widely diverging pathways, to 2 separate but very close sentinel nodes (2 of vessels, originating at opposite poles of injection site, merge in single channel before crossing path of third vessel). (D) RAO view shows multiple lymphatics leading from site of injection in outer upper quadrant to at least 3 separate sentinel nodes (with serial visualization of subsequent-tier nodes).
Performing lymphoscintigraphy in the afternoon before surgery (15–18 h preoperatively) is logistically convenient for the routine in the nuclear medicine department and consistent with the pathophysiology of lymphatic drainage for radiocolloids (115). When using the smaller radiocolloids, it may be best to image the patients and use γ-probe guidance on the same day because these smaller colloids may have passed to second- or third-echelon nodes before surgery at 15 h. In this case, tracer injection in the early morning with surgery at 4–6 h may be more ideal.
Whichever technical approach is followed in the choice of tracer and modality of injection, there is more general consensus on how to perform lymphoscintigraphic acquisitions for sentinel lymph node identification. The energy setting of the gamma camera should be centered on the 140-keV emission peak of 99mTc, with a ±10% window. The use of a high-resolution collimator and an acquisition matrix of 256 × 256 pixels (preferably in byte mode) is highly recommended. In this regard, doses injected intratumorally are usually at least 10-fold higher than those injected intradermally, thus resulting in scatter artifacts that are particularly inconvenient when they affect visualization of a sentinel node that is located a few centimeters away from the injection site. Intermediate effects are observed with intraparenchymal injection, which involves doses about 5-fold higher than those of intradermal injection.
Large-field-of-view gamma cameras are useful to obtain the lymphoscintigraphic pattern of the entire lymphatic basin in a single picture. However, in some cases, small-field-of-view gamma cameras are especially helpful for accurate topographic localization because they can be placed closer to the axilla.
Positioning of the patient on the imaging table and choice of the best scintigraphic projection are important factors for a satisfactory lymphoscintigraphic study before γ-probe–aided biopsy of the sentinel node. The patient should be positioned supine, with the arm abducted completely to allow the head of the gamma camera to be placed as close as possible to the axilla. In patients with large breasts, it is sometimes useful to move the breast to clear the axillary and parasternal regions, thus reducing the attenuation effect of soft breast tissue on the radioactive focus corresponding to the sentinel node, which accumulates <1% of the injected dose.
An anterior scintigraphic view is frequently used initially, but it is usually changed to oblique anterior views, with some craniocaudal tilting, during visualization of radiocolloid drainage. The angles are modified as needed to distinguish between the injection site and focal accumulations corresponding to the draining nodes.
Timing of the sequential spot views reflects the variable combination of tracer used and modality of injection: Radiocolloids with small particle size migrate faster than large radiocolloids and, conversely, radiocolloids injected intradermally migrate faster than those injected intratumorally or intraparenchymally. In a typical lymphoscintigraphic study with 99mTc-HSA nanocolloid (95% of particles < 80 nm) injected intradermally as a single 10- to 20-MBq dose, images are acquired every 10 min for about 3–5 min (recording 400,000–500,000 counts if the injection site is included in the view). The entire procedure is usually completed with good visualization of the sentinel node(s) within about 50–60 min after tracer injection. After intratumoral or intraparenchymal injection of the same tracer, images can be acquired every 30 min or so because the lymphoscintigraphic study can take as long as 2 or 3 h to complete. Finally, completion of lymphoscintigraphy can take even longer (15–18 h) when radiocolloids with larger particle size are injected intratumorally or intraparenchymally.
Continuous dynamic recording for lymphoscintigraphy is feasible when smaller particle radiocolloids are injected intradermally, for instance, at 1 frame per minute for 60 min with a 64 × 64 matrix (as done in the case analyzed in Fig. 4), although it is not used routinely because of the frequent need to change the angles of view with progression of lymphatic drainage. Nonetheless, recording dynamic lymphoscintigraphy can be useful in the learning phase of the procedure, to gain confidence, and to become acquainted with the technique.
It is helpful to define the outline of the body in the area under the head of the gamma camera to localize the sites of tracer accumulation. The body silhouette is easily represented either through a transmission scan obtained with a 57Co flood source or simply by moving a radioactive point source along the contour of the body while recording the scan.
A final, integral phase of lymphoscintigraphy is to mark the exact position of the sentinel node in the axilla using indelible ink, either with the aid of a radioactive point source or preferably using the γ-probe (or both) for counting the axilla externally focusing on the spot(s) visualized by lymphoscintigraphy. With external counting, target-to-background ratios >2 (typically in the 3–10 range) identify the sentinel node(s). In this topographic localization phase, the arm should be abducted at about 90°, approximately in the same position as on the operating table during surgery, to identify accurate topographic coordinates the surgeon can use during the surgical procedure. Marking the skin projection of the sentinel node and having the images available may assist the surgeon in reducing the operating time to find the sentinel node and in keeping the surgical incision to a minimum.
Intraoperative γ-Probe Counting
After positioning the patient on the operating table before starting the surgical procedure, localization of the sentinel node should be confirmed further by external counting with the γ-probe. Minor variations in the sequence of operating procedures exist: Some surgeons remove the primary tumor first and then proceed to perform the biopsy of the sentinel node, whereas other surgeons perform the sentinel node biopsy first and then proceed to remove the tumor while waiting for the results of intraoperative frozen section histopathology. Occasionally, a single surgical incision is extended to expose the tumor and the location of the sentinel node in the axilla when the tumor is located in the outer upper quadrant.
In most recent reports, the overall success rate of lymphoscintigraphy in sentinel node identification is very high, around 97%. The vital blue dye technique has a much lower success rate when used alone (mostly around 75%–80%), and it marginally improves radioguided identification of the sentinel node. Nevertheless, the vital blue dye technique can usefully complement the radioguided procedure to reach a combined success rate of 98%–99%, especially when the sentinel lymph node is diffusely metastatic (therefore, its capacity to retain the radiocolloid is impaired). Many surgeons combine the 2 techniques using the blue dye in the lymphatics as a road map to help find the radioactive sentinel node. This can be important because a noninvolved lymph node may be only few millimeters in diameter and very soft to palpation.
A γ-probe–guided search of the sentinel lymph node is based on detecting a focal spot of radioactivity accumulation in the area of interest (open surgical field). The probe is now in direct contact with the hot spot and is adequately shielded from radiation scattered from the injection site. Thus, counting rates change almost instantly from tens or hundreds of counts per second to nearly zero (as the patient’s background virtually corresponds to room background) when moving the detector—for instance, simply changing the angle—from the hot spot (lymph node) to nearby tissues. Therefore, the concept of target-to-background ratio as commonly used for in vivo nuclear medicine procedures takes on a new meaning; typically, the ratio of counts in the hot spot relative to background is in the 10 to 100 range, though with wide variations depending on the dose injected, type of tracer injected, time elapsed between tracer injection and surgery, and type of γ-probe used. Reexamination of the operative site should then be performed to ensure that the area of radioactivity has been removed and that a second node is not also active; if it is, it should be removed and the axilla should be reexamined until no areas of increased counts are found. Complete removal of the sentinel node(s) is confirmed by reduction of the counting rate in the axilla to background levels. Intraoperative frozen section histopathology is performed on the node with the highest counting rate as well as on any additional lymph nodes with counting rates at least 20% of the counting rate in the hottest node.
Histopathologic Examination of Axillary Sentinel Lymph Nodes
To have real impact in the management of breast cancer patients, histologic examination of the sentinel lymph node(s) must be extremely careful and extensive. The nodes must be entirely and serially sectioned at reduced intervals. Computer simulations and the current practice have shown that, to identify small micrometastatic foci (size, ≤2 mm), the nodes must be sectioned at 50- to 200-μm intervals, thus evaluating up to 60 or more sections per node (116,117). Most macrometastases in a sentinel node are detected in few sections starting from the hilus: about 77% in the first section, 84% within the first 3 sections, and 93% within the first 5 sections. Distribution of micrometastases in a sentinel node is much more dispersed, with only about 53% detected within the first 5 sections and 91% within the first 10 sections; a nonnegligible 9% will be found in sections 11–20 (G. Viale, unpublished data, December 2000); after all, tumor cell clusters giving rise to metastases nest initially in the most peripheral sinusoid spaces of the lymph node. On the other hand, detecting micrometastases is crucial because their presence in the sentinel lymph node is associated with additional metastatic disease of the axilla in about 25% of the patients (117).
Histologic examination of axillary sentinel nodes can be performed either on permanent sections of formalin-fixed, paraffin-embedded tissue or intraoperatively on frozen sections. This latter procedure enables surgical treatment of the primary tumor and, when indicated, axillary node dissection in a single session. Even in the case of intraoperative examination, the sentinel nodes must be entirely and serially sectioned because examination of a few frozen sections from only one half of the node (as routinely done for other purposes) will lead to an unacceptably high number of false-negative results.
The general trend toward extensive intraoperative histologic examination of the sentinel lymph node has generated a recommended protocol that can be summarized as follows (117). The surgical specimen is checked for radioactive counting rates, using the γ-probe for ex vivo counting, to confirm correct identification of the sentinel node and of other nodes possibly draining lymph from the tumor site. The nodes are bisected starting at the hilus, and both halves are frozen in isopentane chilled by liquid nitrogen. Fifteen pairs of frozen sections are then cut at 50-μm intervals from each half. Whenever any tissue is left, additional pairs of sections are cut at 100-μm intervals, until examination of the node is complete. One section of each pair is routinely stained with hematoxylin–eosin; the other section is left unstained for possible immunocytochemistry with anticytokeratin antibodies to assess the nature of questionable cells detected in the corresponding stained sections.
In the experience of a well-trained, harmonized multidisciplinary team focused on breast cancer surgery, the time required for such an extensive examination of the sentinel nodes is approximately 40 min—that is, the time normally spent by the surgeon to complete removal of the tumor, having performed sentinel lymph node biopsy first.
Recent reports have emphasized the role of immunocytochemistry in the accurate identification of micrometastases in sentinel nodes, suggesting that immunoreactions for cytokeratins (epithelial markers) should be performed for all sentinel nodes (118–120). However, the use of immunocytochemistry does not overcome the need for extensive sectioning of the lymph node, which must be sampled entirely. To keep the time required and the costs of the examination of the sentinel nodes as low as possible, the use of immunocytochemistry should be limited to those cases for which diagnosis cannot be made confidently on purely morphologic grounds (hematoxylin–eosin staining). This is particularly true for single-cell metastases, commonly occurring in invasive lobular carcinomas. Thus, the proportion of cases to process with immunocytochemical examination depends on the training and expertise of the examining pathologist on the one hand and the quality of the tissue sections on the other hand.
The potential of amplification of specific messenger RNA molecules by the polymerase chain reaction to detect metastases in sentinel nodes has also been explored (121,122). In these procedures, RNA molecules are extracted from fresh or frozen nodes, and complementary DNA is synthesized by reverse transcription. Epithelial-specific markers (cytokeratin 19, carcinoembryonic antigen, mucine-1, maspin, mammaglobin, and so forth) are then amplified by the polymerase chain reaction.
In vitro experiments have shown that these techniques are effective in identifying a single metastatic cell among 1,000,000 normal lymphoid cells. However, results obtained in vivo have thus far been less impressive. In fact, the sensitivity of these techniques often does not reach the expected 100% of cases known to harbor metastases (most likely caused by problems with the sampling procedures). Even more important, however, is their low specificity (about 85%), with several false-positive results being observed when the procedure is applied to uninvolved nodes or to nodes from patients without any neoplastic disease (G. Viale, unpublished data, December 2000).
RESULTS, CLINICAL SIGNIFICANCE, INDICATIONS, AND CONTRAINDICATIONS FOR SENTINEL LYMPH NODE BIOPSY IN BREAST CANCER SURGERY
When one considers the high number of variables involved in the procedure of radioguided sentinel node biopsy, the success rate of the technique reported by different groups is amazingly consistent. The success rate is commonly considered as the occurrence of positive radioguided identification of the sentinel node based on the combined lymphoscintigraphic and γ-probe counting approach. In articles published in 1997–2000, the success rate of radioguided procedures in localizing the sentinel node during breast cancer surgery is reported to range between 94% and 97% for studies involving >100 patients. In some studies, the success rate in sentinel node localization approaches 99% when radioguidance is complemented with the vital blue dye technique.
Nevertheless, these figures refer only to the easiest, immediate parameter available for assessment—that is, success rate defined as the fraction of patients in whom the sentinel node is identified. This definition cannot automatically imply that the node identified is the true or the only sentinel node. It should be emphasized that >1 sentinel node is identified in a relevant fraction of patients, with average values being reported on the order of 1.5–1.8 per patient.
It also appears that injection of radiocolloid deeper in the breast parenchyma usually entails visualization of additional lymphatic drainage to nodes of the internal mammary chain, although the pathophysiologic and clinical significance of this finding is at present unclear and, therefore, remains to be explored further. Thus, the very high success rate reported for radioguided localization of the sentinel node in patients with breast cancer must be considered with a word of caution. Further careful investigations, which should also consider the long-term outcome of patients submitted to sentinel node biopsy, are necessary to confirm that the true sentinel node (or nodes) has been localized.
Another important parameter in sentinel node biopsy is classification of tumor status of the node by intraoperative frozen section histopathology. Clearly, the most dreadful occurrence to be avoided is misclassification of the patient’s disease by defining a sentinel node as tumor free, yet finding metastatic disease in lymph nodes of the subsequent echelons. The occurrence of such false-negative sentinel nodes has been documented in most studies that also involved complete axillary node dissection and extensive histopathologic evaluation of the axilla. The incidence of this finding, which in our experience (41,99,103,123,124) and in widely reported studies, ranges mostly between 4% and 8% of all patients undergoing sentinel lymph node biopsy, can be affected by technical factors in the identification step (is it the true sentinel node?) and by the accuracy of intraoperative histopathology.
The lowest values for the incidence of a false-negative sentinel node are reported when the technique outlined earlier is used for extensive histopathology. Furthermore, in our own experience, a false-negative sentinel lymph node was never observed in patients with breast cancer in the early stage of growth (T1a-b; tumor size, ≤1 cm) (123,124).
The final, crucial parameter concerning the accuracy of sentinel node biopsy in breast cancer surgery is the impact of this procedure on the long-term clinical outcome of patients. This issue is currently unresolved and hopefully will be clarified by ongoing long-term investigations, involving 2 arms, to which patients who are eligible for the study are randomly assigned. Axillary node dissection is routinely performed on 1 arm irrespective of the tumor status of the sentinel lymph node; it is performed on the other arm only if the sentinel node is metastatic on intraoperative frozen section histopathologic examination. In this regard, some preliminary considerations can be made on the basis of the experience of the European Institute of Oncology, in which >2,000 patients with breast cancer have so far undergone radioguided biopsy of the sentinel node, beginning in March 1996. In a 2- to 4-y follow-up encompassing at present about 1,000 patients who underwent surgery in the period 1996–1998, none of the patients with T1 breast cancer and a negative sentinel node has so far developed tumor recurrence (G. Paganelli, V. Galimberti, U. Veronesi, unpublished data). Although systematic analysis is still missing, this observation is in line with similar data derived from a prospective study performed on a small group of patients with a median follow-up of 39 mo (125).
Therefore, within any center performing sentinel node biopsy without subsequent axillary clearance, a strategy must be developed for adequate follow-up of these patients. Regular restaging should be considered probably for a minimum of 5 y. This should include not just palpation of the axilla by a trained surgeon but also imaging with sensitive techniques, possibly on an annual basis.
Radioguided sentinel lymph node studies are contraindicated in patients with the following findings: (a) patients with palpable axillary nodes or other evidence of axillary node metastatic disease; (b) patients with breast cancer above stage T2 (>4 cm in diameter); (c) patients with multifocal or multicentric cancer (99) or patients in whom breast cancer recurrence is expected within 10 y (126); and (d) patients who previously underwent any surgical procedures in the axilla that may have altered the regional pattern of lymphatic drainage. Conflicting results have been reported concerning the accuracy of sentinel lymph node biopsy in patients who previously underwent excisional biopsy of their breast cancer (127,128) or neoadjuvant chemotherapy (129–132). Therefore, under these conditions, the potential benefit deriving from sentinel lymph node biopsy should be carefully evaluated for each patient on the basis of a strict case-by-case approach.
Some surgeons now consider that enough experience has accumulated indicating that it is safe for the patients to omit axillary lymph node dissection when intraoperative histopathology shows that the sentinel node is free from metastases. In this case, we strongly recommend that the procedure be considered as safe with a high level of certainty only in patients with T1a-b tumors, while keeping in mind the validity of the other exclusion criteria indicated above.
LEARNING CURVE IN SENTINEL LYMPH NODE BIOPSY
Sentinel node biopsy is a combined effort involving at least 3 different specialties: nuclear medicine, surgical oncology, and pathology (possibly health physics). The learning curve depends on how quickly the different operators develop the attitude to work as a single team. Thus, the individual specialists must gain confidence with the various steps of the procedure and, at the same time, rely on each other’s contribution to the entire process.
A close correlation has been reported between the number of procedures performed and the positive predictive value of the technique (133), ranging from 71% after performing <40 procedures to 98% after performing hundreds of sentinel node biopsies (134). According to Orr et al. (135), the learning curve is complete after performing about 60–80 procedures. Cody et al. (136) reported an 86% success rate for the less experienced surgeons, rising to 94% for the more experienced surgeons, whereas Bass et al. (137) reported a success rate of 90% ± 4.5% after performing 23 procedures, rising to 95% ± 2.3% after 53 procedures. Obviously, full axillary lymph node dissection must be performed on all patients during the learning phase, irrespective of whether histology of the sentinel node shows metastatic disease.
Having instructed nuclear medicine and surgical oncology personnel at several institutions on how to perform radioguided sentinel node biopsy, we believe that the learning phase can be considered as complete after performing about 40–60 radioguided sentinel node biopsies. This range depends on how frequently the procedures are performed, an indirect parameter of the level of motivation of the entire team involved.
Two important performance parameters must be analyzed when certifying a multidisciplinary team for sentinel node biopsy in breast cancer surgery: (a) the fraction of successful procedures, considering the learning phase as complete when the sentinel lymph node is identified in at least 97% of the patients; and (b) the fraction of patients with metastasis in the sentinel node at intraoperative histology; this fraction should be about 20%–30% in patients with T1a-b breast cancer and about 35% in patients with T1a-c cancer (as observed in patients undergoing routine axillary node dissection).
EVALUATING γ-PROBES FOR SENTINEL LYMPH NODE BIOPSY
Several reports on evaluation of the physical performance parameters of handheld γ-probes can serve as references for the methodology to follow (138–143). About 20 different models of handheld γ-probes are available. Besides sentinel node biopsy, additional applications of radioguided surgery can involve radionuclides other than 99mTc, even including positron emitters. Thus, choosing the most appropriate radiation-sensitive component of the probe is crucial in relation to the type of the scintillation crystal (CdTe, CsI[Tl], CsI[Na], NaI[Tl], Bi4Ge3O12, CdZnTe, HgI2) and the thickness of the crystal. Candidate γ-probes should be evaluated by a team including primarily the health physicist, the nuclear physician, and the surgeon who will be using the instrument in the operating room (limited to the ergonomics of the probe).
The main parameters of physical performance of γ-probes are sensitivity, energy resolution, and spatial resolution. Sensitivity is the detected counting rate per unit activity, usually expressed as counts per second (cps)/kBq. This parameter basically reflects efficiency of the probe in converting incident radiation into an electric signal but also depends on the diameter of the crystal, which defines the solid angle by which the probe “sees” the source. Sensitivity can be measured by moving radioactive point sources at various distances along the central axis of the probe, in air or in water (or both). Rather than being considered an absolute parameter per se, this parameter should be considered in terms of target-to-background ratios, the main factor affecting surgical strategy in the operating room. This specific property is also called contrast and is jointly correlated with the detector sensitivity, energy resolution, and spatial resolution.
Energy resolution is related to the statistical uncertainty intrinsic in the radioactive detection process and is inversely related to the number of electrons produced by a radiation in the detector. Energy resolution is particularly important for rejection of scatter radiation, so that probes with higher energy resolution will eliminate more counts corresponding to scatter radiation while discarding fewer counts corresponding to the primary radiation.
Spatial resolution is critical for accurately localizing the radioactive source within the volume being explored and is evaluated by determining the detected counting rates as a function of the lateral distance from the central axis of the detector. The major determinant of spatial resolution is lateral shielding of the detector provided by the collimator, which limits the probe’s field of view. Heavier shielding provides better spatial resolution but also reduces sensitivity and increases the weight of the probe. Adequate shielding on the back and the sides enables the probe to be used for directional counting in the surgical field. Spatial resolution is especially important for sentinel node biopsy in breast cancer surgery because the spot of interest has a counting rate at least 2 logarithms lower than that of the injection site, which can be very close to the sentinel lymph node.
Linearity of the counting rate with increasing amounts of radioactivity is also important. High-quality probes exhibit a linear response up to about 4,000–5,000 cps, well over the maximum counting rates commonly found in sentinel lymph nodes in vivo and ex vivo.
Because most of the cost of γ-probe systems for radioguided surgery is associated with the detector, flexibility of the system to use with different radionuclides and with different intrasurgical uses should also be evaluated. The possibility of changing the collimation angle without changing the probe is a definite advantage versus more rigid systems that require additional devices for different uses.
RADIATION PROTECTION ISSUES
Interstitial injection of 99mTc-labeled colloids for lymphoscintigraphy and radioguided surgery does not entail any relevant radiation burden to patients (98,144). The real issue about radiation protection in radioguided surgery concerns the personnel involved in the procedure besides the nuclear medicine personnel.
Two main factors keep the radiation burden to such personnel at virtually negligible levels in radioguided procedures that are performed according to the protocol described above: Very low doses are injected into patients and 2 or 3 physical half-lives elapse between tracer injection and the surgical procedure. These 2 factors explain the results obtained in a carefully controlled study based on 50 sentinel node biopsy procedures and 50 radioguided procedures involving intratumoral injection of 99mTc-albumin macroaggregates (which are permanently retained at the injection site) (144) (about 11 MBq [300 μCi] in both cases).
The cumulative doses to personnel involved in the procedure (surgeons, nurses, pathologists) for 100 operations corresponded at most to about 1% (mean absorbed dose) or about 10% (mean effective dose) of the annual dose limits for the general population. The radioactivity counted in operating room materials possibly contaminated during surgery was also minimal and did not require any special handling procedure. The simple precaution of letting radioactivity decay for some hours was sufficient for tissue specimens in the pathology department, with the hottest material being the injection site.
The above data are consistent with those obtained by other groups after normalization to radioactivity unit and timing of surgery relative to tracer administration (145–149). Protocols implying the injection of radioactive doses that are higher than those described above (up to 20:1) and shorter time elapsed between tracer injection and surgery result in radiation exposure per procedure correspondingly higher than the above figures.
CONCLUSION
Identification of the sentinel lymph node draining a small tumor without palpable metastases is becoming the standard of practice in patients with breast cancer. To optimize sentinel node detection, 99mTc-sulfur colloid (or antimony sulfide or albumin nanocolloid) should be injected several hours before surgery. Radiocolloid has been administered directly into the tumor, in 4 quadrants adjacent to the tumor, intradermally, subcutaneously, or subareolar; in our opinion, either intradermal or peritumoral injection (or both) is preferred. Different volumes of injectate have been advocated, ranging from 0.1 to 4 mL per site; a volume of about 0.3 mL provides adequate images with a low incidence of failure to visualize the sentinel node. Images should be recorded after radiocolloid administration to determine if lymph drains to the sentinel node located medially rather than in the axilla. At the time of sentinel lymph node surgery, blue dye should be administered around the tumor. The combination of blue dye and radiocolloid administration allows the surgeon to identify the sentinel node on the basis of intraoperative γ-counting or blue staining. Once identified, the sentinel node is removed and evaluated by detailed histologic evaluation, including immune staining, for the presence of neoplastic cells. The remaining lymph nodes in the axilla are untouched, thereby reducing the morbidity associated with axillary node dissection.
Although sentinel lymph node identification is valuable in patients with small tumors, it is not recommended in all breast cancer patients. If axillary nodes are palpable, the primary tumor is >4 cm in diameter, the tumor is multicentric, or the patient has had prior axillary dissection or injury that alters the pattern of lymphatic drainage, sentinel node imaging should not be performed. Indication for sentinel lymph node biopsy should also be evaluated carefully for patients who have had prior neoadjuvant chemotherapy or excisional biopsy (or both).
Finally, sentinel node detection and biopsy require some experience on the part of the surgeon. Typical localization success rates of >95% can be achieved after 50 patients are studied. Patients are beginning to read about this procedure and to perceive the advantages of a technique that can avoid the potential morbidity of axillary dissection; thus, they may put pressure on surgical teams to opt for sentinel node localization. Like nothing else in nuclear medicine, sentinel lymph node localization has great potential for benefiting patients, but care must be taken to ensure that fair and accurate information is available to all.
Acknowledgments
The authors are indebted to and thank all coworkers and colleagues who, at various institutions, have contributed greatly to develop the programs of radioguided sentinel lymph node biopsy and to accumulate the expertise that constitutes the basis for this work. In particular, thanks are due to Drs. Ferdinando Buffoni, Paola Erba, Pietro Bianchi, and Giuseppe Agnese of the Nuclear Medicine Service, University of Genoa, Genoa; Drs. Marco Gipponi, Carlo Vecchio, Daniela Tomei, Franca Carli, and Guido Nicolò of the National Cancer Institute, Genoa; Drs. Concetta De Cicco, Marco Chinol, and Mirco Bartolomei of the Nuclear Medicine Service, European Institute of Oncology, Milan; and Drs. Alberto Luini, Viviana Galimberti, and Umberto Veronesi of the Division of Senology, European Institute of Oncology, Milan. This work was supported in part by grants from the Italian Ministry of University and of Scientific and Technological Research, the Italian Ministry of Health (Rome), and the Italian Association for Cancer Research (Milan).
Footnotes
Received Jan. 18, 2001; revision accepted Apr. 12, 2001.
For correspondence contact: Giuliano Mariani, MD, Regional Center of Nuclear Medicine, University of Pisa Medical School, Via Roma 67, I-56126 Pisa, Italy.
*NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/education/ce_online.html) UNTIL AUGUST 2002.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- CLINICAL PROBLEM
- ANATOMY AND PHYSIOLOGY OF LYMPHATIC SYSTEM AS IT RELATES TO BREAST CANCER
- RADIOPHARMACEUTICALS
- TECHNIQUES
- RESULTS, CLINICAL SIGNIFICANCE, INDICATIONS, AND CONTRAINDICATIONS FOR SENTINEL LYMPH NODE BIOPSY IN BREAST CANCER SURGERY
- LEARNING CURVE IN SENTINEL LYMPH NODE BIOPSY
- EVALUATING γ-PROBES FOR SENTINEL LYMPH NODE BIOPSY
- RADIATION PROTECTION ISSUES
- CONCLUSION
- Acknowledgments
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Radioguided Surgery
- Clinical Evaluation of 99mTc-Rituximab for Sentinel Lymph Node Mapping in Breast Cancer Patients
- Results of a Prospective Multicenter International Atomic Energy Agency Sentinel Node Trial on the Value of SPECT/CT Over Planar Imaging in Various Malignancies
- In vivo albumin labeling and lymphatic imaging
- Particle-Size and Radiochemical Purity Evaluations of Filtered 99mTc-Sulfur Colloid Prepared with Different Heating Times
- Does the Preparation and Utilization of 99mTc-Sulfur Colloid Affect the Outcomes of Breast Lymphoscintigraphy?
- The Sentinel Node Procedure in Breast Cancer: Nuclear Medicine as the Starting Point
- Evaluation of the Efficacy of a Small CdTe {gamma}-Camera for Sentinel Lymph Node Biopsy
- Sentinel Lymph Node Mapping of the Breast
- Usefulness of Medium-Energy Collimator for Sentinel Node Lymphoscintigraphy Imaging in Breast Cancer Patients.
- Is the "Ideal" {gamma}-Probe for Intraoperative Radioguided Surgery Conceivable?
- Sentinel Lymph Node Detection in Patients with Early-Stage Breast Cancer: Comparison of Periareolar and Subdermal/Peritumoral Injection Techniques
- Patient effective dose from sentinel lymph node lymphoscintigraphy in breast cancer: a study using a female humanoid phantom and thermoluminescent dosemeters
- Lymphoscintigraphy for Sentinel Node Mapping Using a Hybrid SPECT/CT System
- Factors Affecting Visualization Rates of Internal Mammary Sentinel Nodes During Lymphoscintigraphy
- Radioguided Sentinel Lymph Node Biopsy in Malignant Cutaneous Melanoma*