


Abstract
The aim of this study was to evaluate the prognostic value of SPECT imaging using the amino acid analog 3-[123I]iodo-l-α-methyltyrosine (IMT) in patients with gliomas. Methods: One hundred fourteen consecutive patients with newly diagnosed gliomas were examined by IMT SPECT (low-grade glioma, n = 12; anaplastic astrocytoma or oligodendroglioma, n = 46; glioblastoma, n = 56). Seventy-one of these patients had undergone tumor resection 4–6 wk before SPECT imaging (group A). Forty-three patients with unresectable tumors were examined after stereotactic biopsy (group B). IMT uptake at the site of the tumor was assessed visually and quantified relative to a contralateral reference region (IMT uptake ratio). After IMT SPECT, all patients were treated with conformal radiotherapy. The median follow-up time was 27 mo. Results: In group A, focal IMT uptake at the resection site was visible in 52 of 71 patients (73%). Median survival was only 13 mo in these patients, whereas median survival was reached in patients without focal IMT uptake (P = 0.02). Furthermore, the intensity of IMT uptake significantly correlated with survival: patients with an IMT uptake ratio > 1.7 were at a 4.6 times higher risk of death than were patients with a lower IMT uptake (P < 0.001). The IMT uptake ratio remained a significant prognostic factor when age and grading were included in a multivariate model. In contrast, IMT uptake did not correlate with survival in group B (P = 0.95). Conclusion: In patients with unresectable high-grade gliomas, IMT uptake appears not to correlate with the biologic aggressiveness of tumor cells. Nevertheless, the clear association between focal IMT uptake after tumor resection and poor survival suggests that IMT is a specific marker for residual tumor tissue. Therefore, IMT SPECT is expected to become a valuable tool for the planning and monitoring of local therapeutic modalities.
Glial neoplasms have a well-established propensity for local invasiveness and recur in most patients at or near the site of origin. In contrast to most extracranial tumors, distant metastases are uncommon even in advanced tumor stages. Nevertheless, the prognosis of patients with malignant gliomas remains poor. Furthermore, histopathologically benign, low-grade tumors have a high incidence of recurrence and often show progressive dedifferentiation in the course of disease. The development of systemic chemotherapy for gliomas has been challenging because the blood–brain barrier is impermeable for many potentially active chemotherapeutic drugs (1).
Because of these biologic characteristics of glial tumors and the limitations of systemic therapy, local therapeutic modalities such as conformal (2) or stereotactic radiotherapy (3), endoradiotherapy (4,5), local application of chemotherapeutic drugs (6), and gene therapy (7) are being studied intensively. All these therapeutic approaches require that the extension of the tumor tissue be defined accurately. Brain tumors are most commonly delineated using CT and MRI. In CT studies, glial tumors generally appear as ill-defined masses of low density. In MRI studies, tumor tissue is usually hypointense on T1-weighted images and hyperintense on T2-weighted images. However, the tumor borders defined by these abnormalities on CT and MR images often cannot be differentiated from surrounding vasogenic edema (8). Additionally, most high-grade gliomas show a disruption of the blood–brain barrier resulting in contrast enhancement on CT and MR images. In untreated tumors, contrast enhancement generally corresponds to highly cellular and vascularized areas of the tumor. However, contrast enhancement clearly does not represent the outer tumor border, because infiltrating glioma cells can easily be detected within, and occasionally beyond, a 2-cm margin around the area of contrast enhancement (9,10). Furthermore, disruption of the blood–brain barrier is an unspecific finding and may be caused by several factors other than tumor cell infiltration. Specifically, in patients previously treated by surgery or radiotherapy, recurrent or persistent tumor is often indistinguishable from reparative changes (8). Thus, CT and MRI have well-recognized limitations in the delineation of gliomas, and the true extension of glial neoplasms may be under- or overestimated by these imaging modalities.
Tracer techniques targeting special aspects of tumor metabolism, proliferation rate, and surface receptors may overcome these limitations when used in combination with morphologic imaging modalities. For delineating gliomas, imaging of the increased amino acid transport rate of tumor cells has been particularly encouraging (11). Several studies have shown that brain tumors can be visualized by the radiolabeled amino acid analog 3-[123I]iodo-l-α-methyltyrosine (IMT) and SPECT (12–14). Furthermore, IMT SPECT has shown promising results for differentiating between recurrent brain tumors and therapy-induced reactive changes such as radionecrosis (15,16). We have shown, in a previous study, that glioma volumes defined by IMT SPECT are considerably different from volumes defined by MRI (17). However, it is not known whether the findings of IMT SPECT are specific for tumor tissue after surgery and whether the intensity of IMT uptake is correlated with patient survival. This study addressed these 2 issues by analyzing the prognostic value of residual IMT uptake after resection of cerebral gliomas. For comparison, the correlation between IMT uptake and patient survival was also determined for a group of patients with previously untreated tumors.
MATERIALS AND METHODS
Patient Population
This study is a retrospective analysis of 114 consecutive patients with newly diagnosed gliomas who were imaged by IMT SPECT before conformal radiotherapy. All tumors were histopathologically proven by open surgery or stereotactic biopsy. Tumor grading was evaluated according to the classification of the World Health Organization (18). None of the patients had undergone previous radio- or chemotherapy for an intracranial tumor.
In 71 patients (35 women, 36 men; mean age ± SD, 50 ± 13 y), a tumor had been resected within 4–6 wk before SPECT imaging (group A). The histopathologic diagnosis was low-grade (grade II) astrocytoma in 6 of these patients, anaplastic (grade III) astrocytoma in 19, anaplastic (grade III) oligodendroglioma in 8, and glioblastoma (grade IV) in 38.
In 43 patients (20 women, 23 men; mean age, 58 ± 12 y), tumor resection had not been feasible because of the location of the tumors or the poor general condition of the patient (group B). In these patients, a histopathologic diagnosis had been obtained by stereotactic biopsy. IMT SPECT was performed within 2–3 wk after biopsy. Six of these patients had low-grade astrocytomas, 19 had anaplastic astrocytomas, and 18 had glioblastomas.
SPECT Imaging
Patients fasted for at least 4 h before IMT SPECT imaging to ensure standardized metabolic conditions. IMT was labeled by direct electrophilic iodination using Iodogen (Pierce, Rockford, IL) as an oxidant (19). Radiochemical yields were approximately 80%, and a specific activity of approximately 160 TBq/mmol was achieved. Data acquisition started 30 min after intravenous injection of 250–370 MBq IMT. One hundred 40-s projections were acquired with a triple-head camera (MULTISPECT 3; Siemens Medical Systems, Inc., Hoffman Estates, IL) equipped with dedicated 123I collimators (20). Transaxial tomograms were reconstructed by filtered backprojection (Butterworth filter; order, 10; cutoff frequency, 0.4 Nyquist). Attenuation was corrected by applying the method of Chang (21) as implemented in the standard software of the camera system (attenuation coefficient, 0.11/cm). The spatial resolution of the reconstructed images was 10 mm at full width at half maximum, and slice thickness was 4 mm. The study protocol was approved by the ethics committee at our institution, and written informed consent was obtained from all patients.
Analysis of IMT SPECT Studies
All IMT SPECT studies were evaluated by a single observer who was unaware of the clinical patient data and the results of other imaging studies. Images were displayed in axial, sagittal, and coronal slices on the computer screen of the gamma camera console using a linear gray scale. The SPECT studies were first visually assessed for focal IMT uptake of higher intensity than normal cortex. For quantitative analysis, circular regions of interest 1.5 cm in diameter were placed in the area with the highest IMT uptake in 3 consecutive axial slices. In the case of multiple sites of focal IMT uptake, the lesion with the highest IMT uptake was used for further analysis. Mirror regions of the same size were placed as a reference in contralateral normal tissue. An IMT uptake ratio was calculated by dividing mean lesion by mean reference activity. In addition, the ratio between maximum tumor IMT uptake and mean activity in the reference region was calculated.
Radiotherapy and Patient Follow-Up
After SPECT imaging, all patients underwent conformal radiotherapy using a 6-MeV linear accelerator (Mevatron; Siemens). The target dose was 60 Gy, delivered in daily fractions of 1.8–2.0 Gy. Details of the applied 3-dimensional conformal irradiation treatment have been published (22). After radiotherapy, 31 patients received cyclophosphamide–carmustine (1,3-bis-(2-chloroethyl)-1-nitrosourea) chemotherapy. Follow-up information was provided by clinic records, correspondence from referring and referral physicians, and telephone calls to physicians and patients’ families. Survival was measured from the time of SPECT imaging.
Statistical Methods
Quantitative parameters were expressed as the mean value ± 1 SD. Differences in quantitative parameters for groups of patients were analyzed by the Mann–Whitney and Kruskal–Wallis tests. The correlation between quantitative parameters was assessed by Spearman rank correlation. Differences in proportions of patients were evaluated using χ2 statistics. Survival curves and median survival times were determined by the Kaplan–Meier nonparametric method. Tests for differences in survival in different groups of patients were performed using log-rank statistics. For all estimated parameters, 95% confidence intervals (CI) were determined. A stepwise Cox proportional hazards model was used to test for the significance of the following factors: age (age ≥ 50 y vs. age < 50 y), histopathology (glioblastoma vs. no glioblastoma), and IMT uptake (high vs. low). High IMT uptake was defined as a higher uptake ratio than the median of all analyzed patients. Variables were retained in the model if the associated 2-tailed probability values were ≤0.05. All statistical computations were performed using the StatView software package (SAS Institute, Cary, NC), version 5.0 for Windows (Microsoft, Redmond, WA).
RESULTS
Group A
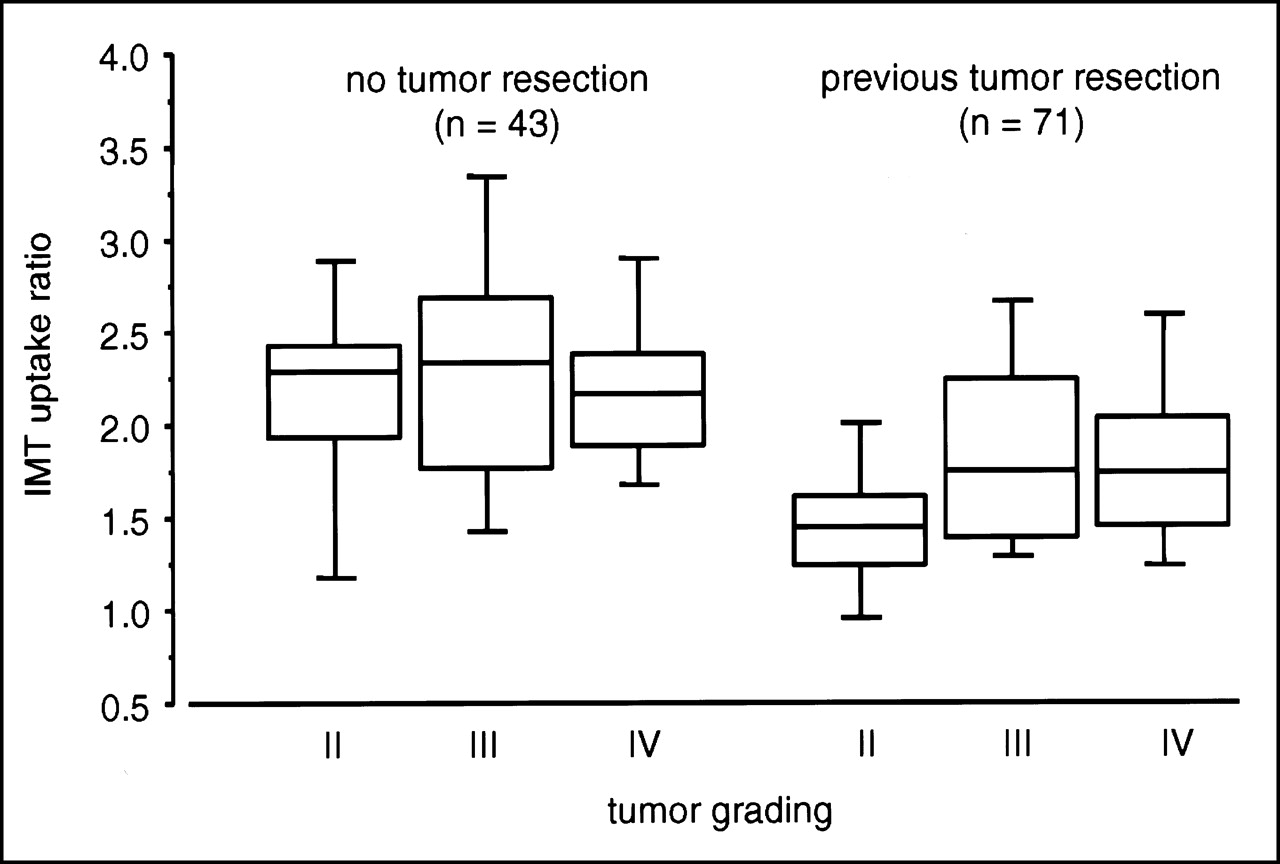
Among the 71 patients of group A, focal IMT uptake at the site of the resection margin was visible in 52 (73%). Figure 1 shows typical SPECT studies with and without focal IMT uptake. The IMT uptake ratio of all 71 patients was 1.8 ± 0.5 (median, 1.7). No significant correlation was seen between IMT uptake ratio and tumor grading (P = 0.16; Fig. 2). Similar results were obtained when maximum tumor IMT uptake was analyzed instead of mean tumor IMT uptake. The maximum IMT uptake ratio in grade II, grade III, and grade IV tumors was 1.7 ± 0.4, 2.2 ± 0.7, and 2.1 ± 0.6, respectively (P = 0.23). There was also no significant correlation between IMT uptake and patient age (P = 0.34).

In patients with anaplastic astrocytoma, examples of IMT SPECT studies with (A) and without (B) focal IMT uptake at resection site. (A) On left, MR image (T1-weighted after administration of gadolinium-DTPA) shows resection cavity (white arrow) and rim of contrast enhancement (black arrow). Resection cavity contains blood and is, therefore, hyperintense in T1-weighted image. On right, IMT SPECT image shows intense uptake of IMT at resection margin. This patient died 6 mo after SPECT study. (B) On left, MR image shows resection cavity (white arrow) and surrounding contrast enhancement (black arrow). However, on right, IMT SPECT image shows no clear focal IMT uptake. This patient was still alive after 38 mo of follow-up.

IMT uptake and tumor grading. On left, no significant correlation (P = 0.71) is seen between IMT uptake and tumor grading in the 43 patients who were imaged after stereotactic biopsy. On right, no significant correlation (P = 0.16) is seen between IMT uptake and tumor grading in the 71 patients who were imaged after tumor resection.
The median follow-up time after SPECT imaging was 25 mo, and the range was 7–56 mo. Overall median survival was 21 mo (2-y survival rate, 44%; CI, 30%–59%). In patients without focal IMT uptake at the site of the resection, median survival was not reached during the follow-up period (2-y survival rate, 76%; CI, 55%–97%). In contrast, median survival was only 13 mo (2-y survival rate, 34%; CI, 17%–50%) in patients with focal IMT uptake (P = 0.02; relative risk, 3.2; CI, 1.1–9.1).
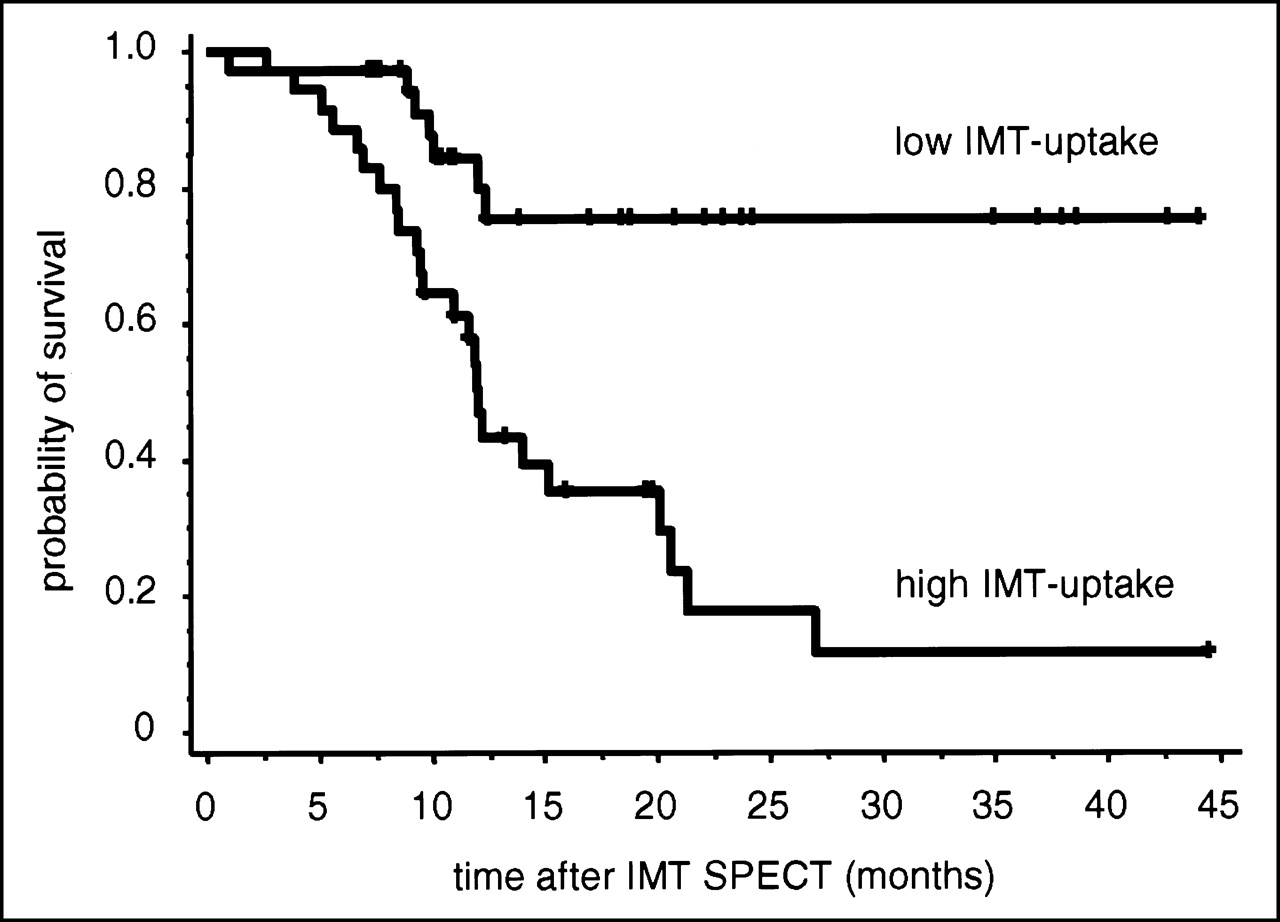
In the quantitative image analysis, median survival was not reached in patients with low IMT uptake (uptake ratio ≤ 1.7). In contrast, median survival was only 12 mo in patients with high IMT uptake (P < 0.001; relative risk, 4.6; CI, 2.0–10.6; Fig. 3). The corresponding 2-y survival rates were 76% (CI, 59%–91%) and 18% (CI, 1%–34%), respectively. Similar results were obtained when only patients with high-grade tumors (grades III and IV) were analyzed. In these 65 patients, overall median survival was 20 mo (2-y survival rate, 39%; CI, 23%–56%). Survival was significantly shorter in patients with high IMT uptake (median survival, 12 mo) than in patients with low IMT uptake (median survival not reached; P = 0.001). No significant differences were found between the groups of patients with low and high IMT uptake with respect to tumor grading, age, or use of chemotherapy (P > 0.1; Table 1).
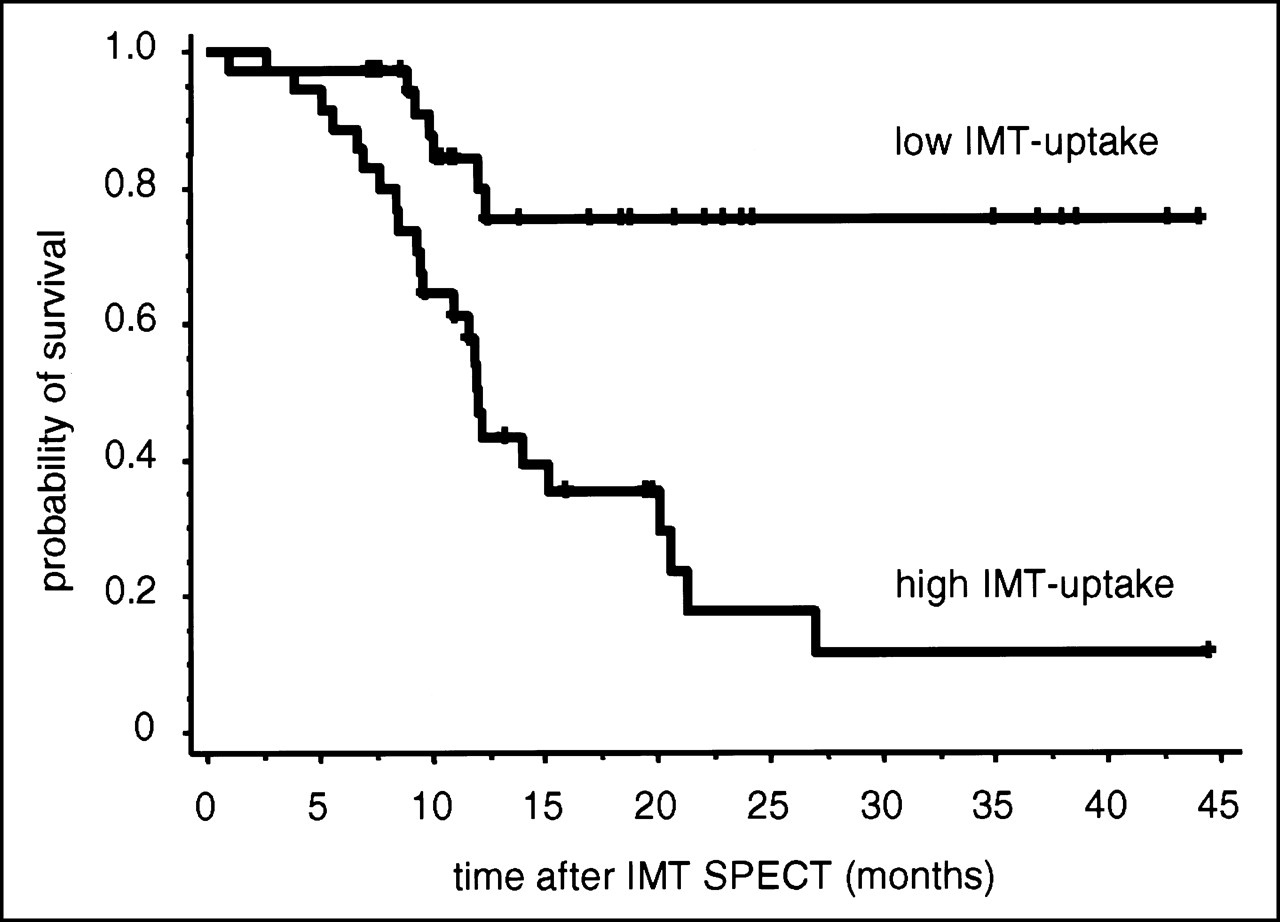
Kaplan–Meier estimates of overall survival among patients with low and high postoperative IMT uptake (n = 71). In patients with IMT uptake ratio > 1.7 (high IMT uptake, n = 35), survival is significantly shorter (P < 0.001 by log-rank test) than in patients with uptake ratio ≤ 1.7 (low IMT uptake, n = 36).
Characteristics of the 71 Patients Imaged After Tumor Resection
In univariate analysis, age and histopathology were also found to be significant prognostic factors (P < 0.01). However, the IMT uptake ratio remained a significant prognostic factor when these known prognostic variables were included in a multivariate analysis. In the stepwise Cox proportional hazards model, only the variables IMT uptake (P < 0.001; relative risk, 4.2) and histopathology (P < 0.01; relative risk, 4.0) were found to be significant prognostic factors.
Group B
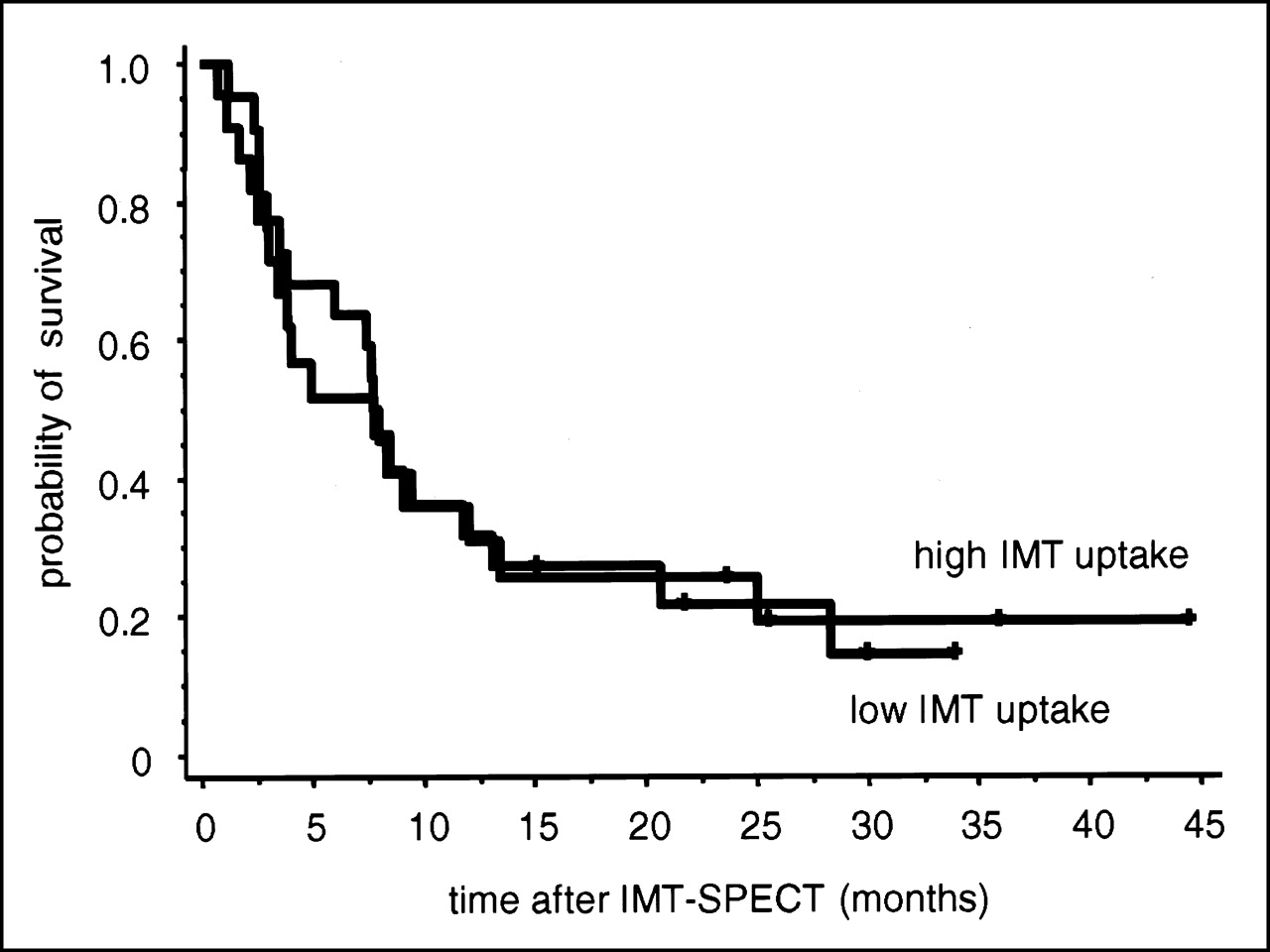
In the 43 patients of group B, 40 tumors (93%) showed focally increased IMT uptake. In 2 anaplastic astrocytomas and 1 low-grade astrocytoma, IMT uptake was similar to uptake in normal gray matter. For all 43 tumors, the IMT uptake ratio was 2.3 ± 0.6 (median, 2.2). Similarly to patients imaged after tumor resection, no significant correlation was found between IMT uptake ratio and tumor grading (P = 0.71; Fig. 2). The maximum IMT uptake ratio in tumors of grades II, III, and IV was 2.5 ± 0.7, 2.7 ± 0.8, and 2.6 ± 0.6 (P = 0.85), respectively. The median follow-up time was 32 mo, and the range was 4–56 mo. Overall median survival was 8 mo (2-y survival rate, 24%; CI, 11%–37%). Thus, survival was significantly shorter than in the 71 patients treated by surgical resection (P < 0.001). In contrast to the patients imaged after tumor resection, survival did not significantly differ between patients with high and low IMT uptake (P = 0.95; relative risk, 0.95; CI, 0.5–1.9; Fig. 4).

Kaplan–Meier estimates of overall survival among untreated patients with low and high IMT uptake (n = 43). There was no significant difference (P = 0.95 by log-rank test) in overall survival between patients with IMT uptake ratio > 2.2 (high IMT uptake, n = 21) and patients with uptake ratio ≤ 2.2 (low IMT uptake, n = 22).
DISCUSSION
The results of this study indicate that in patients with gliomas, residual focal IMT uptake is an important prognostic factor after tumor resection. In 71 consecutive patients, the intensity of IMT uptake significantly correlated with patient survival: an IMT uptake ratio > 1.7 was associated with a 4-fold higher risk of death. Furthermore, IMT uptake remained significantly correlated with survival when the important known prognostic factors age and tumor grading were included in a multivariate analysis. These findings strongly suggest that postoperative IMT uptake is a specific marker for residual tumor tissue and not an unspecific sign reflecting reparative changes.
Previous studies in a limited number of untreated patients have indicated that the intensity of IMT uptake correlates with tumor grading and tumor cell proliferation (23,24). Thus, the poor prognosis of patients with high IMT uptake can be related to the greater biologic aggressiveness of the residual tumor tissue. However, in our patient population, we did not observe a correlation between tumor grading and IMT uptake after tumor resection. Furthermore, IMT uptake remained an important prognostic factor when tumor grading was included in a multivariate analysis. Thus, in patients with a previous resection, IMT uptake measured by SPECT is more likely a marker for the presence of residual tumor tissue than for the biologic aggressiveness of the tumor cells. Several studies have shown that the amount of residual tumor tissue is an important prognostic factor after resection of gliomas (25–27). Therefore, the correlation between the IMT uptake ratio and survival may be explained by partial-volume effects: a smaller residual tumor will lead to a less intense signal in SPECT imaging than will a larger residual tumor, even when their amino acid uptake is identical.
The correlation between tumor grading and amino acid uptake has been discussed controversially in the literature. Several studies have reported that tumor uptake of 11C-methionine, which correlates closely with tumor uptake of IMT (28), is significantly different between low- and high-grade gliomas (29,30). Furthermore, Kaschten et al. (30) found a significant correlation between tumor uptake of 11C-methionine and survival. However, no significant differences in the amino acid uptake of low- and high-grade gliomas were observed in other studies using IMT and 11C-tyrosine (16,31). Furthermore, a considerable overlap in 11C-methionine uptake by low- and high-grade gliomas has also been noted (32).
In this study, we found no significant correlation between IMT uptake and tumor grading in patients with unresectable tumors. In addition, tumor IMT uptake did not correlate with survival in this group of patients. These discrepant findings are probably related to differences in the patient populations. Kaschten et al. (30) studied mainly grade II and IV tumors (n = 34) and included only a limited number of grade III tumors (n = 6). In this study, only 6 of the 43 patients with unresectable gliomas had grade II tumors. In addition, these patients were scheduled to undergo radiotherapy because of progressive tumor-associated symptoms. Therefore, they represented a subset of patients with advanced disease and were not representative of the whole group of patients with low-grade gliomas. Furthermore, sampling errors in the stereotactic biopsies used to grade tumors must be considered (33). Nevertheless, our study suggests that in patients with unresectable high-grade gliomas, IMT SPECT cannot be used to differentiate anaplastic astrocytomas and oligodendrogliomas (grade III tumors) from glioblastomas (grade IV tumors). This possibility is clinically important because patients with glioblastomas have a considerably poorer prognosis than do patients with grade III tumors. Furthermore, conventional imaging modalities cannot reliably differentiate between grade III and grade IV tumors, and stereotactic biopsies may be unreliable because of sampling errors (1).
In patients with high-grade tumors, the presence of residual tumor after surgical resection can be assessed by early postoperative MRI. A disruption of the blood barrier stemming from reparative changes has been shown to be uncommon within 72 h after tumor resection (25). Thus, contrast enhancement may be used as a relatively specific marker for tumor tissue during this period. Patients for whom contrast enhancement is seen on early postoperative MR images have been found to have a considerably poorer prognosis than patients without signs of residual tumor tissue (25). The prognostic relevance of residual IMT uptake after tumor resection is in accordance with these findings and underlines the importance of macroscopically complete resection for the treatment of gliomas. However, IMT SPECT has 2 obvious advantages over MRI for the assessment of residual tumor tissue.
First, it is well recognized that contrast enhancement underestimates the true extension of tumor tissue in patients with high-grade tumors. Furthermore, contrast enhancement may be faint in patients with anaplastic astrocytomas and is generally absent in patients with low-grade tumors. Thus, contrast enhancement obviously is an insensitive marker for tumor tissue, and use is limited to patients with high-grade tumors. Conversely, IMT uptake is frequently observed in tumors or tumor areas without contrast enhancement on MRI (17,20). Therefore, IMT SPECT appears to be a more sensitive test for the detection of tumor tissue postoperatively.
Second, IMT SPECT may be used to detect residual tumor tissue at the time of radiotherapy planning, approximately 4 wk after tumor resection. At that point, unspecific contrast enhancement is found on MRI in almost all patients and residual tumor cannot be delineated reliably (25). Early postoperative MRI often cannot be used for radiotherapy planning because the configuration of the resection cavity may have changed in the meantime.
What mechanisms can account for the postoperative specificity of IMT SPECT for tumor tissue? In vitro studies have shown that cellular uptake of IMT is predominantly mediated by the l-type amino acid transport system (34,35). In contrast to natural amino acids, IMT is not incorporated into proteins and is only minimally metabolized (13). Thus, tumor uptake of IMT assessed by SPECT imaging reflects the activity of the l-type transport system. Animal experiments and preliminary patient studies have indicated that amino acid uptake by inflammatory cells is relatively low compared with uptake by viable tumor tissue (36,37). Finally, there are apparently several subtypes of the l-type amino acid transport system. Several years ago, functional studies had already identified subtypes l1 and l2, which show marked differences in substrate affinity and expression pattern. Recently, the l type transport system was characterized at the molecular level, and several subtypes of the l-type transport system have been identified (38). One may therefore speculate that glial neoplasms overexpress a transporter subtype with a high affinity for IMT that shows only low expression in nonneoplastic cells. This possibility can explain why, in humans, no discernable uptake of IMT occurs in the bone marrow, pancreas, and small intestine although these show intense uptake of natural amino acids such as tyrosine and methionine, which are also substrates for the l-type transport system. The recent reports of human complementary DNA for different l transporter subtypes will allow testing of this hypothesis (38).
The limited spatial resolution of SPECT restricts use of IMT to the delineation of only relatively large tumors. However, 18F-labeled amino acid analogs with uptake mechanisms similar to that of IMT have recently been described (39,40). PET studies using these new tracers will enable visualization of l-type amino acid transport with considerably higher spatial resolution than is possible with IMT SPECT.
This study has 2 limitations that result mainly from the retrospective nature of the data analysis. First, early postoperative MRI was not routinely performed on all patients, and images were not always available at the time of data analysis. Therefore, the findings of IMT SPECT were not compared with the findings of early postoperative MRI in this study. Second, the importance of residual IMT uptake after tumor resection can be underlined by follow-up imaging that shows recurrent disease at the site of abnormality revealed by postoperative IMT SPECT. However, for most patients, follow-up imaging was performed at other institutions and the corresponding CT and MRI images were not available at the time of data analysis.
CONCLUSION
The correlation between postoperative IMT uptake and patient survival indicates that imaging of l-type amino acid transport represents a promising strategy to assess the presence and location of tumor tissue in patients with pretreated gliomas. Because of the known limitations of anatomic imaging, this functional approach to the delineation of tumor extension is expected to significantly improve planning of local therapies such as conformal radiotherapy, radiosurgery, or endoradiotherapy.
Acknowledgments
The authors appreciate the excellent technical support of the technologists at our institutions and the editorial help of Leishia Tyndale-Hines in the preparation of the manuscript. This study was supported in part by the Deutsche Krebshilfe.
Footnotes
Received Dec. 4, 2000; revision accepted Apr. 9, 2001.
For correspondence or reprints contact: Wolfgang A. Weber, MD, Nuklearmedizinische Klinik, Klinikum Rechts der Isar, Ismaningerstrasse 22, 81675 Muenchen, Germany.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cost-Effectiveness Analysis of Amino Acid PET-Guided Surgery for Supratentorial High-Grade Gliomas
- The Value of 99mTc-Tetrofosmin Brain SPECT in Predicting Survival in Patients with Glioblastoma Multiforme
- PET for response assessment in oncology: radiotherapy and chemotherapy
- Use of PET for Monitoring Cancer Therapy and for Predicting Outcome
- Comparison of O-(2-18F-Fluoroethyl)-L-Tyrosine PET and 3-123I-Iodo-{alpha}-Methyl-L-Tyrosine SPECT in Brain Tumors
- Comparative Biodistribution of Iodinated Amino Acids in Rats: Selection of the Optimal Analog for Oncologic Imaging Outside the Brain
- Increased Tumor Uptake of 3-123I-Iodo-L-{alpha}-Methyltyrosine After Preloading with Amino Acids: An In Vivo Animal Imaging Study