


Abstract
The adenomatous polyp of the colon is clinically important as a precursor of colonic cancer. The aim of this preliminary study was to evaluate the potential usefulness of 18F-FDG PET for detecting adenomatous polyps of the colon. Methods: We performed a retrospective study of 110 subjects who underwent both PET study and total colonoscopy. On nonattenuation-corrected PET images, focal distinct FDG accumulation along the large intestine was considered a positive finding, and the PET results were compared with colonoscopic findings. Histology and adenoma size were determined by polypectomy. Results: Fifty-nine adenomatous polyps, 5–30 mm in size, were found in 30 subjects by total colonoscopy. PET findings were positive for 14 of the 59 adenomas (24%). The positivity rate for PET images rose with the increase in size of the adenomas; it was 90% in adenomas (9/10) that were ≥13 mm. The overall false-positive rate was 5.5% (6/110 subjects). Conclusion: Increased glucose metabolism is observed in colonic adenomas, and detectability with PET increases with the increase in adenoma size. Adenomas are premalignant lesions, and it is important to realize that colonic adenomas may be found incidentally during an FDG PET study.
Because increased glucose uptake is one of the biochemical characteristics of cancer cells, whole-body 18F-FDG PET has been used successfully in depicting various malignant tumors, including colorectal cancers (1–4). In addition, we have had patients with adenomatous polyps of the colon that were detected incidentally with PET (5). The adenomatous polyp is benign, but it is thought to be a precursor of colon cancer (6). It is an accepted medical practice to remove colonic adenomas when they are found. Detection of an adenoma contributes to the prevention of colorectal cancer (7). Barium enema study and colonoscopy are the gold standards for detecting colonic adenomas, although a recent study showed the limitation of barium enema in detecting small adenomas (8). One disadvantage of both examinations is that preparatory bowel cleansing is required.
To our knowledge, the PET literature has not referred to the colonic polyp in detail. Thus, we reviewed PET images obtained in our institution and investigated the potential usefulness of FDG PET in the detection of adenomatous polyp of the colon.
MATERIALS AND METHODS
Our institution is a membership-based medical club offering periodic health checkups. Subjects of this study were 110 asymptomatic club members (71 men, 39 women; age range, 36–84 y; mean age ± SD, 56.5 ± 9.3 y) who had undergone both PET study and total colonoscopy as part of our cancer-screening program (9). All PET studies were performed at our institution as routine examinations. Informed consent was obtained from all subjects before the PET study. All subjects fasted at least 4 h before the PET study and, 45–60 min after the administration of 260 MBq FDG, emission scanning was performed with a whole-body PET scanner (ECAT EXACT 47; CTI/Siemens, Knoxville, TN). Transmission scanning for attenuation correction was not performed. Transaxial and coronal PET images were evaluated visually by the same physician, who had experience in PET oncology for >5 y. On the PET images, distinct focal FDG accumulation along the large intestine was interpreted as a positive finding. Total colonoscopy was performed at each subject’s local hospital. Intervals between the PET study and colonoscopy were <3 mo. All colonoscopic results were obtained directly from the hospitals in which the studies were performed. The colonoscopic findings were reported in terms of the site and size of polyps. Polyp sizes were determined by polypectomy. During interpretation of the PET images, the colonoscopic findings were available, and the PET images were compared with the colonoscopic findings. Because PET is clearly limited in detecting small lesions and because high-grade dysplasia is uncommon in small adenomas (6), adenomatous polyps that were <5 mm were excluded from this study.
RESULTS
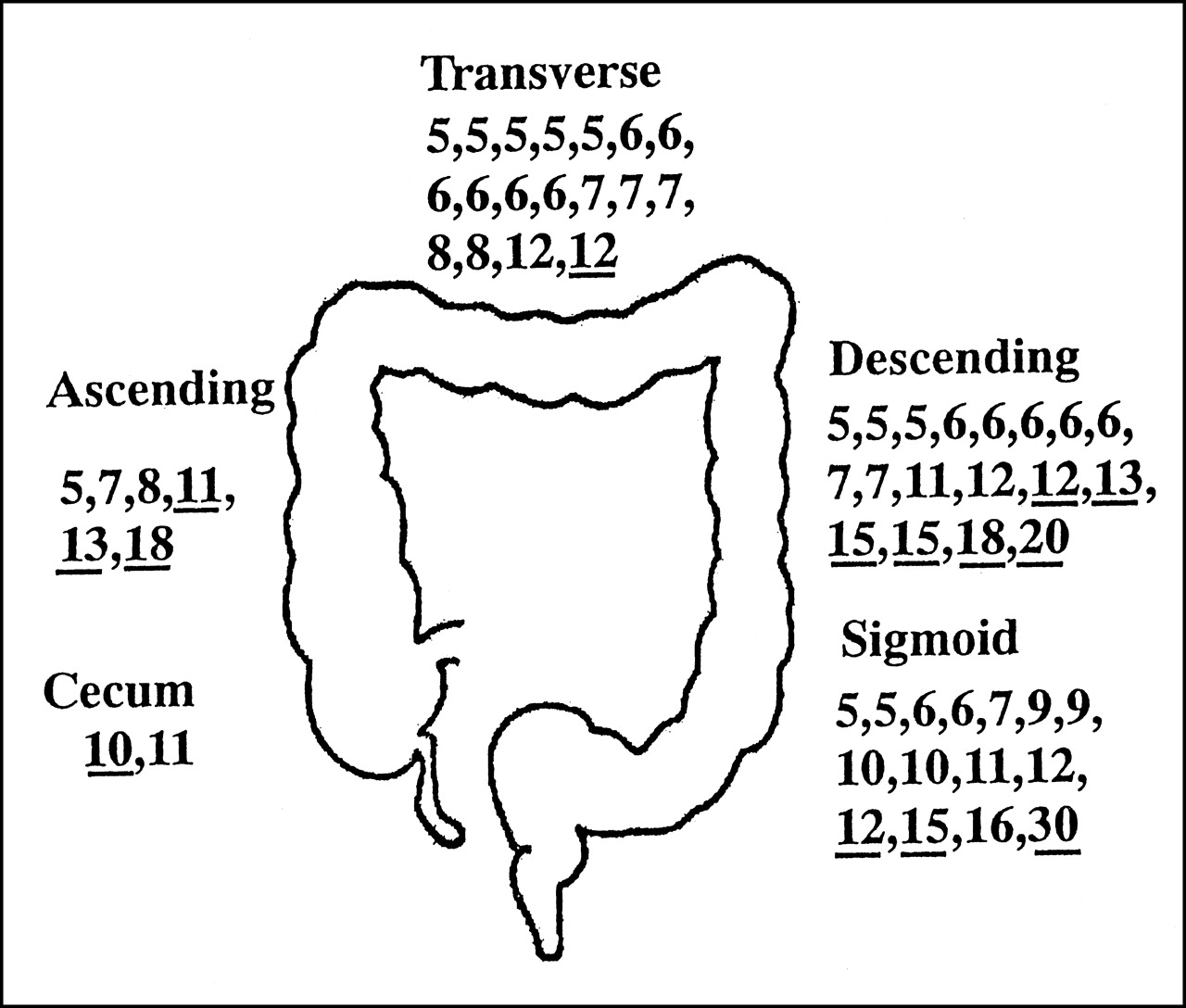
Fifty-nine adenomas (size range, 5–30 mm) were found in 30 subjects on total colonoscopy. PET findings were positive in 14 of these adenomas (size range, 10–30 mm) in 13 subjects. PET findings were negative in the other 45 adenomas (size range, 5–16 mm) (Fig. 1).
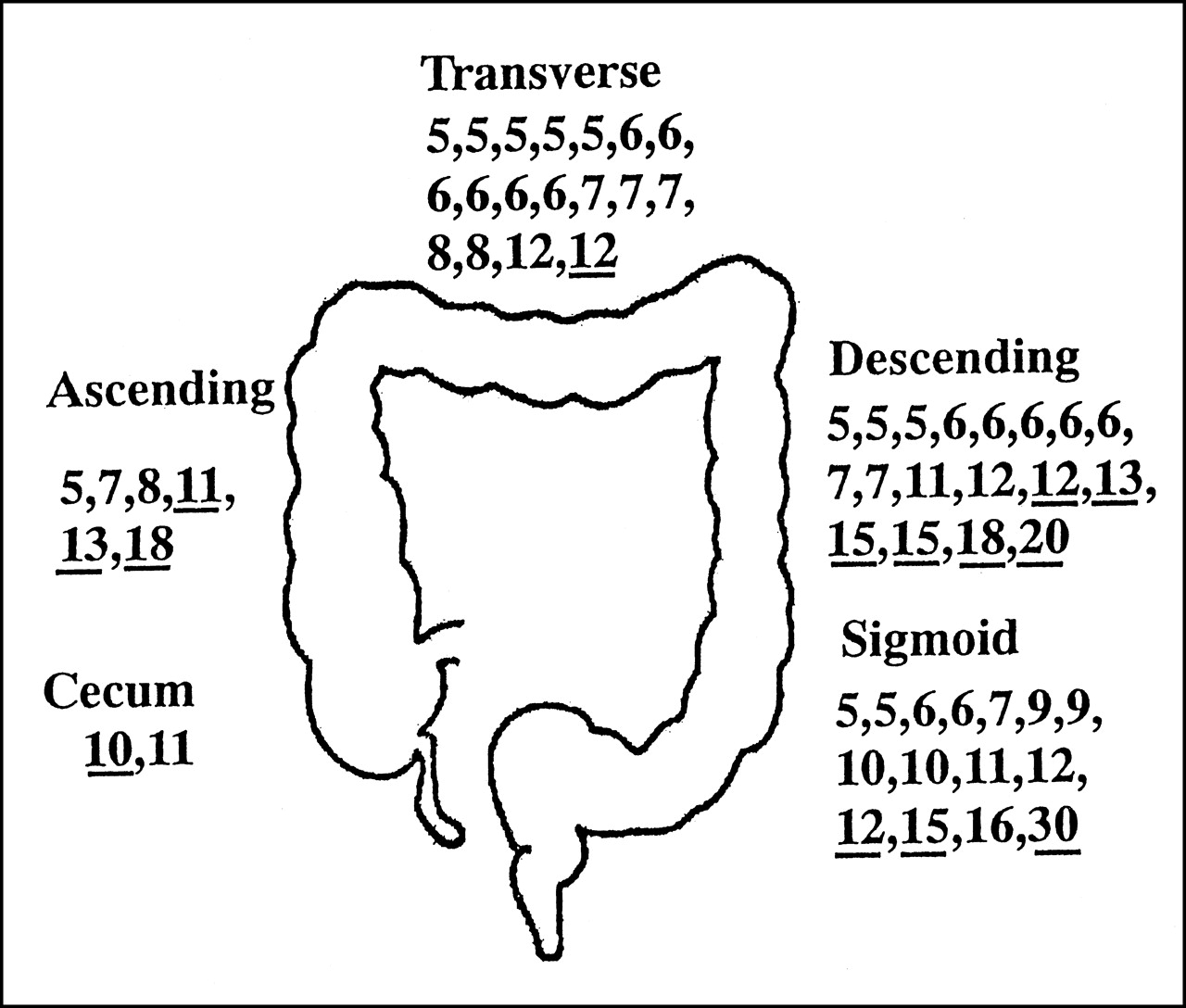
Sites and sizes of 59 adenomas diagnosed by colonoscopic polypectomy. Numbers indicate adenoma sizes (mm) and underlines indicate PET-positive adenomas.
The positivity rate for PET images rose with the increase in lesion size; it was 90% in adenomas (9/10) that were ≥13 mm (Table 1). The positivity rate was significantly higher in the cecum, ascending colon, and descending colon (10/26, 38%), where the colon is fixed to the retroperitoneum, than it was in the transverse and sigmoid colon (4/33, 12%) (Fisher’s exact test, P = 0.0199) (Table 2).
Sizes of Adenomas with Corresponding PET-Positive Rates
Sites and PET-Positive Rates
Of 13 subjects with PET-positive adenomas, 4 had undergone PET studies 11–15 mo earlier. Abnormal FDG accumulation was identified retrospectively on earlier PET images of 2 of these subjects (Table 3). An example case is presented in Figure 2.
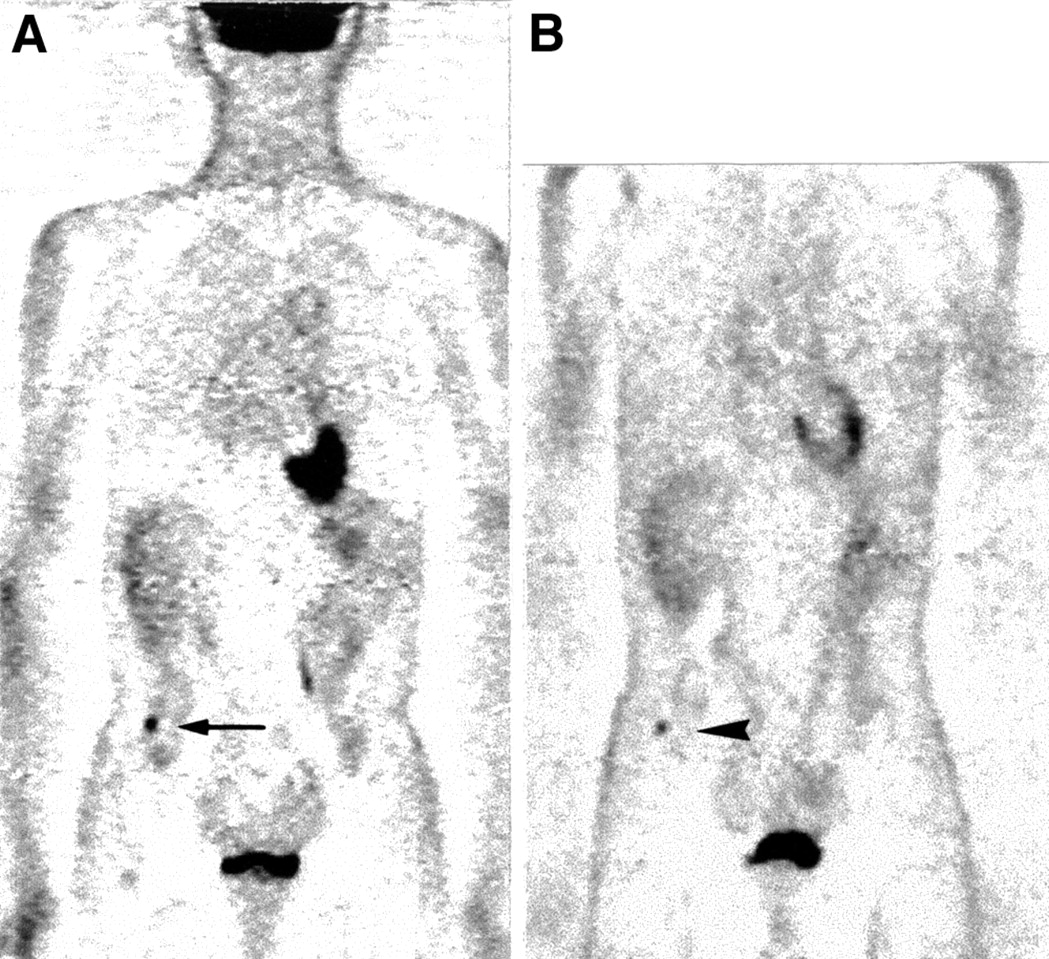
(A) A 50-y-old asymptomatic man with focal FDG uptake in ascending colon (arrow). After PET study, he underwent colonoscopy, which revealed sessile polyp in ascending colon. Polypectomy was performed, and histopathologic study showed 11-mm villotubular adenoma with high-grade dysplasia. (B) On retrospective evaluation of PET images obtained 15 mo earlier, focal FDG uptake was identified at same site (arrowhead).
Previous PET Findings in 4 Subjects with PET-Positive Adenomas
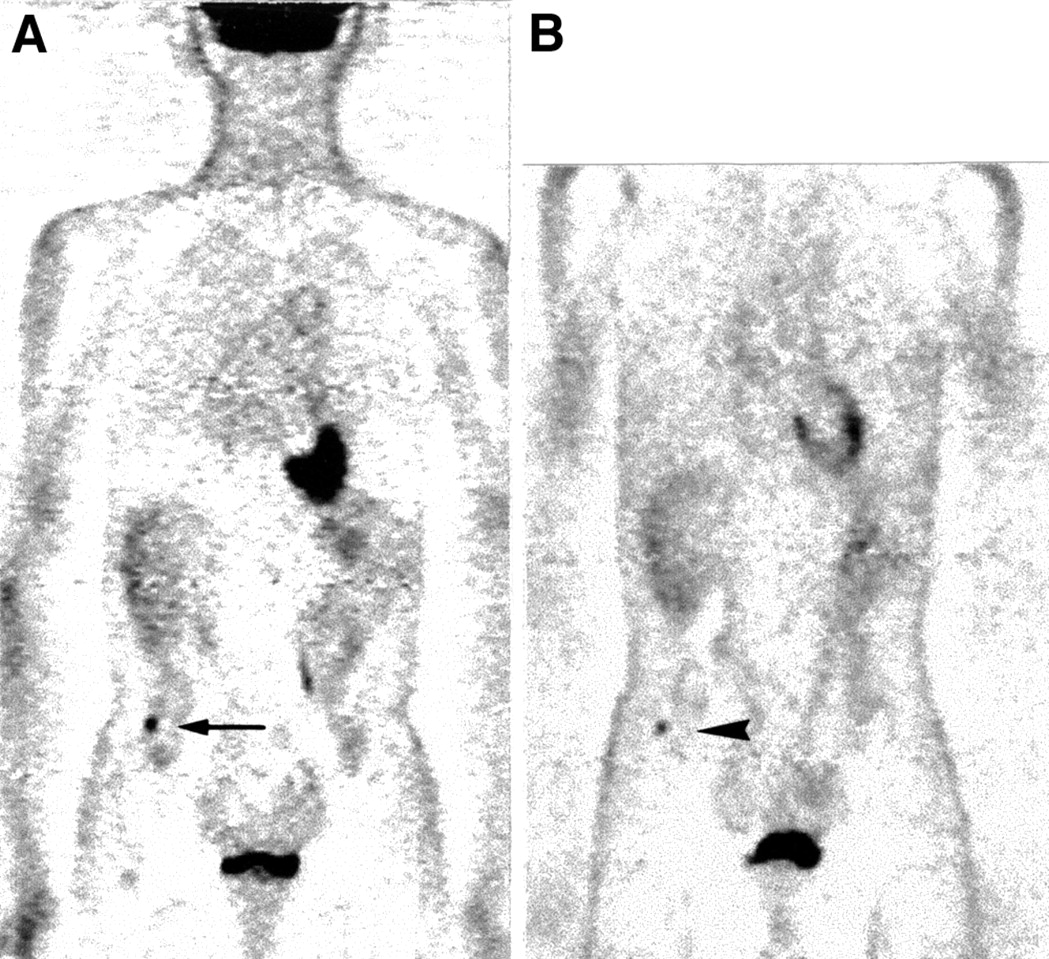
There were 6 subjects in whom focal FDG accumulation was observed on PET images, though the colonoscopic result was negative. This finding accounted for a false-positive rate of 5.5% (6/110 subjects) in our study. An example of false-positive images is shown in Figure 3.

A 49-y-old asymptomatic woman with focal FDG uptake in lower abdomen (arrow). Adenoma in sigmoid colon was suspected, but colonoscopic examination showed no abnormality. Arrowhead indicates FDG in left ureter.
DISCUSSION
Increased glucose metabolism has been reported in colorectal cancer. In 1962, Macbeth and Bekesi (10) showed increased anaerobic glycolysis in vitro in surgically resected colon cancers. Later FDG PET studies, which were based on in vivo measurement of glucose metabolism, showed high FDG uptake in both primary (3,11–13) and recurrent colorectal cancers (1,2,4,14). Primary colorectal cancers as small as 1.4 cm (3) and 1.8 cm (13) were detected with PET.
To our knowledge, this study is the first to describe in detail high FDG uptake in adenomatous polyps of the colon. Histologically, there are several types of benign colonic polyps—for example, adenoma, hyperplastic polyp, juvenile polyp, and inflammatory polyp. Adenomas and hyperplastic polyps are the most prevalent, and only adenomas have the potential for malignant transformation (6). In a previous study, 35 hyperplastic polyps (size range, 3–38 mm) were all negative on FDG PET (3). It is noteworthy that adenomatous polyps, which have the potential for cancer, accumulate FDG, whereas hyperplastic polyps, which do not have the potential for cancer, do not accumulate FDG.
In our study, the larger adenomas could be detected by FDG PET, whereas the smaller ones could not. The spatial resolution (full width at half maximum) of our PET machine is 6.0 mm in the axial plane, and for lesions less than twice this length (i.e., <12 mm), FDG uptake is underestimated because of the partial-volume effect. We believe that this partial-volume effect affected the detectability of the small adenomatous polyps in our study.
It is accepted medical practice to remove colonic adenomas when they are detected, although there is no consensus regarding the minimum size of the adenoma that should be resected. The likelihood of malignant transformation increases with the increase in adenoma size (6). Our study revealed that adenomatous polyps ≥13 mm could be detected incidentally during FDG PET study; adenomatous polyps ≥13 mm are large enough and should be resected.
In our study, adenomas in the cecum, ascending colon, or descending colon were more likely to be visualized by PET than were adenomas in other parts of the large intestine. This finding can be explained by the fact that the cecum, ascending colon, and descending colon are fixed at the retroperitoneum; mobility is restricted. It is possible that mobility, including peristaltic movement of the colon, affects the visualization of adenomas with PET. Because the study was retrospective, we could not give anticholinergic drugs. Our result could also be explained by the fact that the larger adenomas in our study subjects were seen in the cecum, ascending colon, and descending colon than elsewhere. For example, 12 of 26 adenomas ≥11 mm (46%) were seen in 1 of these 3 sites, whereas only 8 of 33 adenomas of this size (24%) were seen in the transverse and sigmoid colon. Although the difference was not statistically significant (Fisher’s exact test, P = 0.068), the tendency was toward the presence of larger adenomas in these 3 sites.
As is shown in Table 3, 2 PET-positive and polypectomized adenomas, 11 and 18 mm, were identifiable on PET images 15 and 12 mo earlier, respectively. This finding raises the possibility that colonic adenomas can be detected with PET at a stage that is treatable by endoscopic polypectomy.
Double-contrast barium enema and colonoscopy are the gold standards for diagnosis of colonic adenomas. Both examinations are sensitive and relatively inexpensive, although the rate of detection with barium enema is related to adenoma size (8). Compared with these examinations, PET is insensitive and relatively expensive. Therefore, PET cannot substitute for barium enema or colonoscopy, and PET is not reliable as a screening tool for small adenomas. The advantage of PET imaging is that it can survey the entire body noninvasively, including the colon and rectum, without bowel preparation. PET can be an option for patients for whom bowel preparation, barium enema study, or colonoscopy poses a formidable barrier. It is most important to recognize that colonic adenomas can be detected incidentally during FDG PET study; the incidence of colonic adenomas is not low.
The degree of FDG uptake may relate to the degree of dysplasia in the adenoma. However, we were unable to investigate this relationship. The criteria for dysplasia differ among pathologists, and our pathologic diagnoses depended on reports from each hospital’s pathologist; 1 particular pathologist could not review all specimens. In addition, we did not perform transmission scanning for attenuation correction, and thus we were unable to quantitatively evaluate local FDG uptake. Further study should be done to determine how the degree of FDG uptake relates to the degree of dysplasia.
The large intestine is a well-known site of physiologic FDG uptake (15,16), and intestinal FDG uptake poses a practical problem in the evaluation of PET images. Intestinal uptake can hinder detection of FDG uptake in the adenoma. It can also be the source of a false-positive result. In our study, the rate at which false-positive findings resulted from intestinal FDG uptake was 5.5% (6/110 subjects). Scans interpreted as positive were interpreted incorrectly in as many as 32% subjects (6/19). Our posit is that, in addition to the suggestion of colonic carcinoma, distinct focal FDG uptake along the large intestine suggests the presence of colonic adenoma and this finding calls for prompt colonic examination by barium enema study or colonoscopy.
CONCLUSION
Increased glucose metabolism is observed in colonic adenoma. Therefore, colonic adenoma and carcinoma may not be differentiated by PET. Adenomas have the potential for malignant transformation, and most of them are curatively resected by colonoscopic polypectomy. Hence, it is important to recognize that adenomatous polyps can be found incidentally with PET. Further study encompassing a large number of patients with colonic adenoma is warranted to confirm our observation.
Footnotes
Received Aug. 18, 2000; revision accepted Mar. 9, 2001.
For correspondence or reprints contact: Seiei Yasuda, MD, Department of Surgery, Tokai University School of Medicine, Kanagawa, 259-1193, Japan.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Identifying targetable metabolic dependencies across colorectal cancer progression
- Total Abdominal 18F-FDG Uptake Reflects Intestinal Adenoma Burden in Apc Mutant Mice
- Nonlaxative PET/CT Colonography: Feasibility, Acceptability, and Pilot Performance in Patients at Higher Risk of Colonic Neoplasia
- [18F]FDG PET/CT imaging of colorectal cancer: a pictorial review
- Glucose Deprivation Contributes to the Development of KRAS Pathway Mutations in Tumor Cells
- The Potential Role of Systemic Buffers in Reducing Intratumoral Extracellular pH and Acid-Mediated Invasion
- Screening for Cancer with PET and PET/CT: Potential and Limitations
- Acid-Mediated Tumor Invasion: a Multidisciplinary Study
- Synchronous Primary Neoplasms Detected on 18F-FDG PET in Staging of Patients with Esophageal Cancer
- 2-(18F)-Fluoro-2-Deoxy-D-Glucose Positron Emission Tomography Detects Clinical Relevant Adenomas of the Colon: A Prospective Study
- PET/CT Detection of Unexpected Gastrointestinal Foci of 18F-FDG Uptake: Incidence, Localization Patterns, and Clinical Significance
- An Evolutionary Model Of Carcinogenesis
- Application of quantitative models from population biology and evolutionary game theory to tumor therapeutic strategies
- 18F-Fluoro-2-deoxyglucose positron emission tomography in the evaluation of gastrointestinal malignancies