


Abstract
Occipital lobe perfusion defects have been identified on regional cerebral blood flow (rCBF) SPECT scans of adolescent children and young adults with major depressive disorder (MDD). We reinvestigated a series of rCBF SPECT scans obtained several years ago on drug-naive children with a clinical diagnosis of MDD and on healthy children. Methods: To test whether visually apparent abnormalities in rCBF constitute statistically significant differences between patients, given the relatively small sample sizes, we applied the technique of statistical parametric mapping (SPM). Results: Two groups of patients were identified: 8 with significant posterior flow deficits in the occipital cortex (Brodmann’s areas 18 and 19), usually symmetric, and best visualized on paramedian sagittal sections, and 13 without obvious occipital perfusion deficits but with anterior rCBF deficits in a pattern often described in the literature, attaining statistical significance in the right frontal region. Other localizations in the left frontal and bilateral prefrontal regions did not attain significance, but each localization contained statistically significant maxima (z scores). The scan findings of all 18 healthy children were normal. Conclusion: With the aid of SPM, 2 groups of children with significantly different rCBF behavior were identified. The reason for this difference is not known but should be investigated to determine its possible significance to patients with MDD.
Occipital lobe (Brodmann’s areas 18 and 19) perfusion defects have been identified on 99mTc-hexamethylpropyleneamine oxime regional cerebral blood flow (rCBF) SPECT scans of adolescent children and young adults with major depressive disorder (MDD) diagnosed by the criteria of the Diagnostic and Statistical Manual of Mental Disorders, third edition (1,2). By applying the technique of statistical parametric mapping (SPM), we reinvestigated a series of rCBF SPECT scans obtained several years ago from a group of children (for the purposes of this study, defined as individuals ≤ 18 y old) who were drug naive and had clinically diagnosed MDD and from a group of healthy children (3). In SPM, the statistical significance of differences in voxel intensity between patient groups is tested with an appropriate test statistic, such as a t statistic, for each voxel. Contiguous groups of voxels (clusters) with a greater than expected extent or degree of difference from control subjects, based on gaussian field theory, are interpreted as regionally specific effects (3). The resulting test statistics are assembled into a whole-brain map, the statistical parametric map, which shows regions where the difference from control subjects in the spatial extent of voxel clusters or the value of a single maximum voxel exceeds chance. For studies with no prestated hypothesis supported by prior data, the statistical tests are corrected for the number of potential hypothesis tests performed, but for studies, like ours, in which a specific regional effect is supported by prior research, such corrections are not made for statistical tests in the region of interest.
MATERIALS AND METHODS
rCBF SPECT scans were obtained with a PRISM 3000 triple-head camera (Marconi Medical Systems, Cleveland, OH) equipped with fanbeam collimators (6.0-cm full width at half maximum). The dose of 99mTc-hexamethylpropyleneamine oxime (Ceretec; Nycomed Amersham, Chicago, IL) was 5.18 MBq/kg. At the time of imaging, a group of 8 patients (3 boys, 5 girls; age range, 11–18 y) was found to have occipital perfusion defects on interpretation of scans. A second group of 13 patients (8 boys, 5 girls; age range, 11–16 y) was found not to have posterior defects, but some patients showed evidence of the type of frontal perfusion defects that the literature has described. The group of 18 healthy volunteers (9 boys, 9 girls; age range, 11–18 y) who were studied at the same time had normal SPECT findings. Informed consent was obtained from each subject and his or her parents or guardians, in accord with the rules of the campus institutional review board. Further, the study was approved by the National Institutes of Health. The radiotracer was injected intravenously in a room with subdued lighting and low ambient noise while the subjects kept their eyes and ears open.
rCBF SPECT data were obtained and processed as previously described (4). The resulting images comprised complete, contiguous sets of transaxial views parallel to the canthomeatal plane, with orthogonal sagittal and coronal sets of sections. Data in these 3 projections were then reregistered in space as defined by Talairach and Tournoux (5) (Talairach space), with transaxial slices parallel to a plane through the anterior and posterior commissures, using MEDx 3.2 software (Sensor Systems, Sterling, VA) and an Ultra 60 9.1-GB computer (Sun Microsystems, Palo Alto, CA). With the SPM program, data were processed for the identification of significant clusters of voxels and were smoothed at 10 × 10 × 10 mm. Global cerebral blood flow was controlled for by proportional scanning, and a gray matter threshold of 0.8 was used. The images were scaled to a mean global cerebral blood flow of 50 mL/min/dL.
SPM analysis was performed to test the 2 prestated hypotheses, namely, that the group of patients with apparent occipital rCBF deficits will have statistically significant differences from control subjects in the occipital region and that the group with no apparent occipital deficits will have statistically significant differences from control subjects in the frontal regions. The height threshold of the SPM program was set at P = 0.01, thus allowing into analysis only voxels differing between groups at this significance level. Based on their adjacency, voxels surviving the height threshold were then grouped into clusters of size k voxels, with the most statistically significant voxel in each cluster having a z score of z. The anatomic location of each significant cluster was determined in the x-, y-, and z-dimensions (in millimeters) of Talairach space (Tables 1 and 2). The statistical significance of each cluster was assessed by calculating the probability of observing a cluster of extent size k and the probability of observing a z score of magnitude z, both uncorrected for the number of tests performed. Both tests were considered statistically significant at P ≤ 0.05.
Results of SPM Analysis on 8 Patients with MDD and Occipital Deficits vs. 18 Control Subjects
Results of SPM Analysis on 13 Patients with MDD and Frontal Deficits vs. 18 Control Subjects
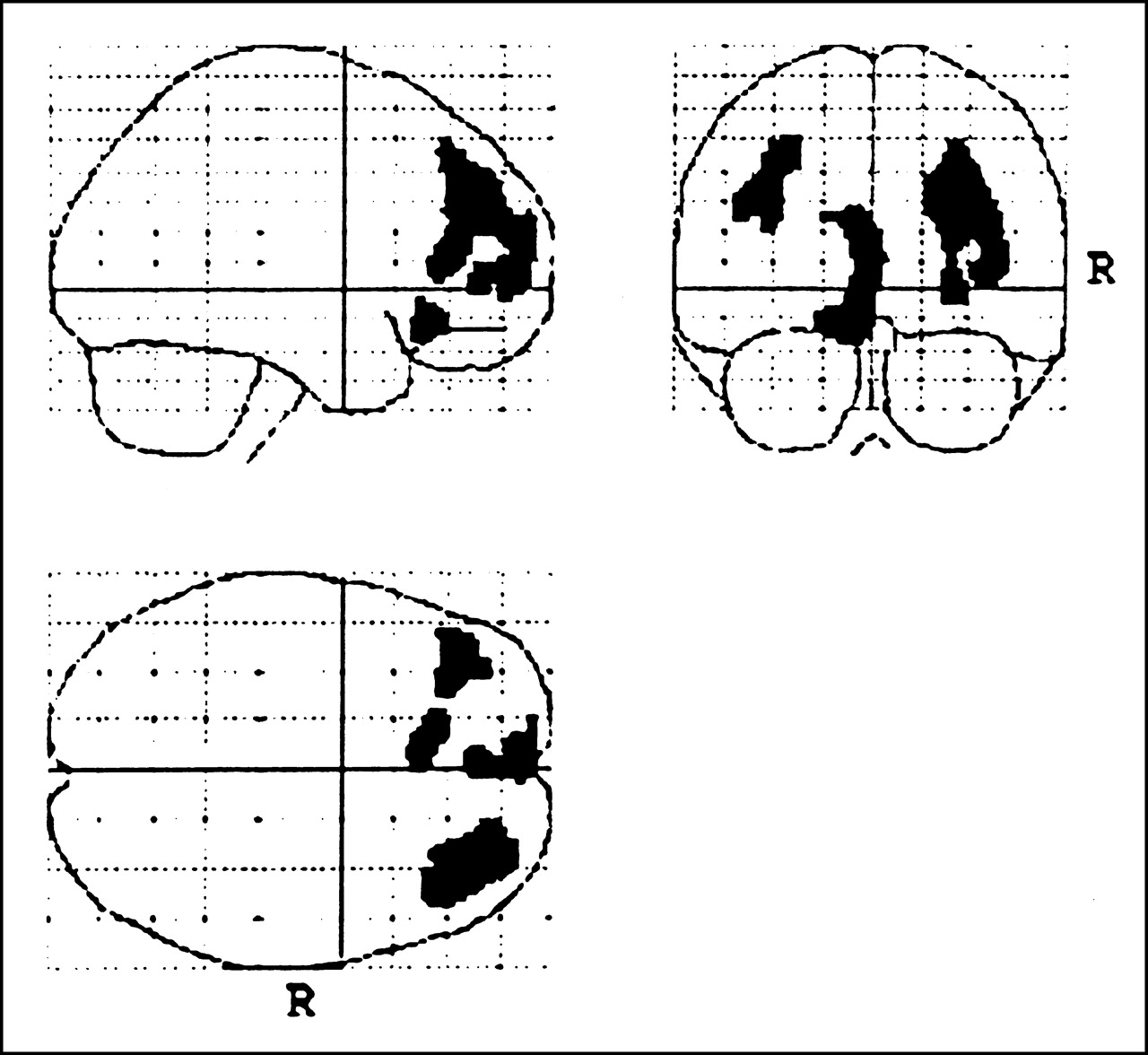
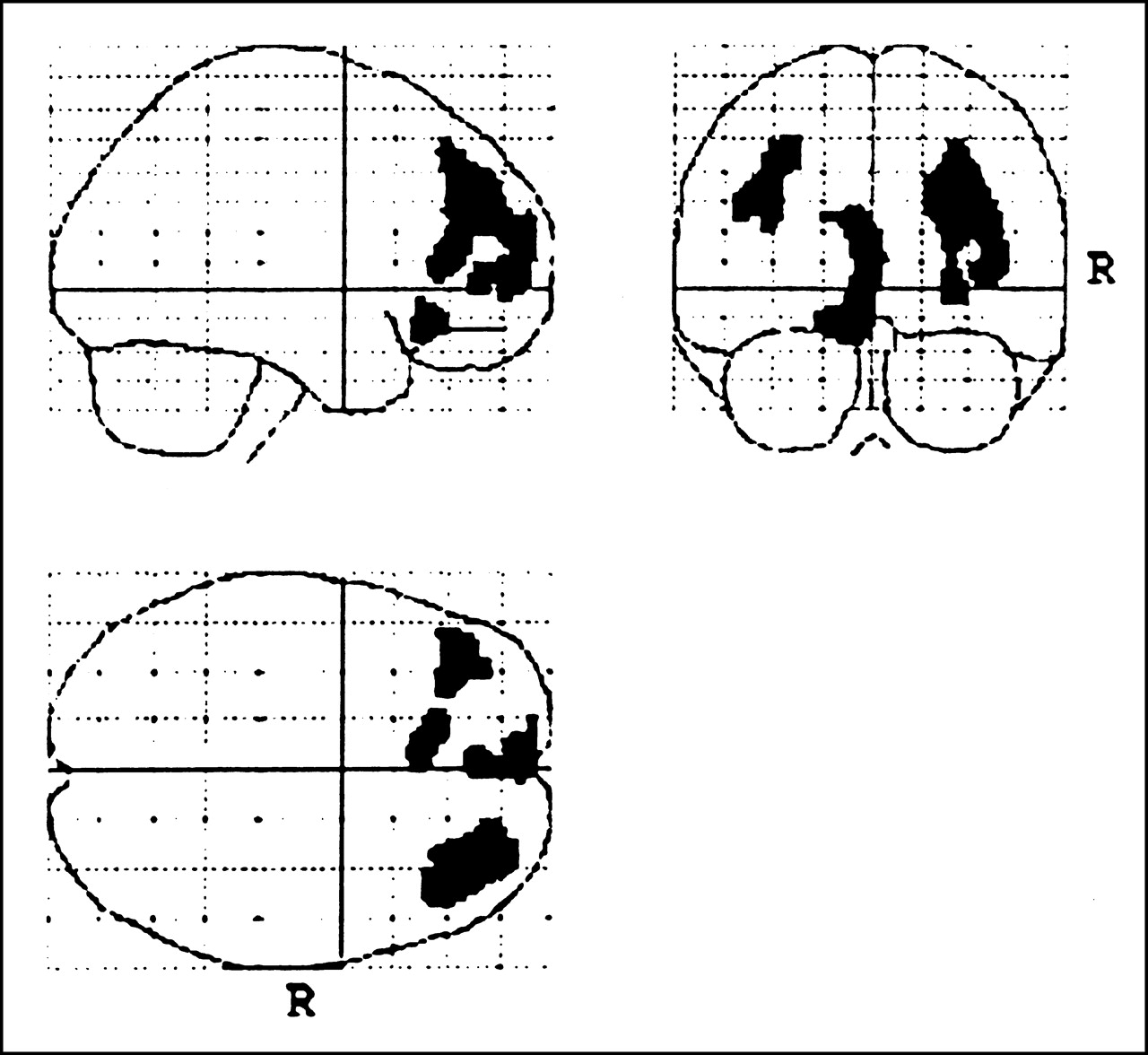
Transaxial slices of each statistical parametric map were constructed contiguously and were fused with a standard MR image of the brain to help localize the significant clusters. The final figures for presentation were prepared by consolidating all views in midplane images in the x-, y-, and z-projections, thus superimposing all significant data on each projection (Figs. 1 and 2).

SPM maps of SPECT data from 8 patients with MDD and occipital defects and from 18 control subjects. Statistically significant data are projected onto midplane sections in each projection. Right frontal localizations are not statistically significant.
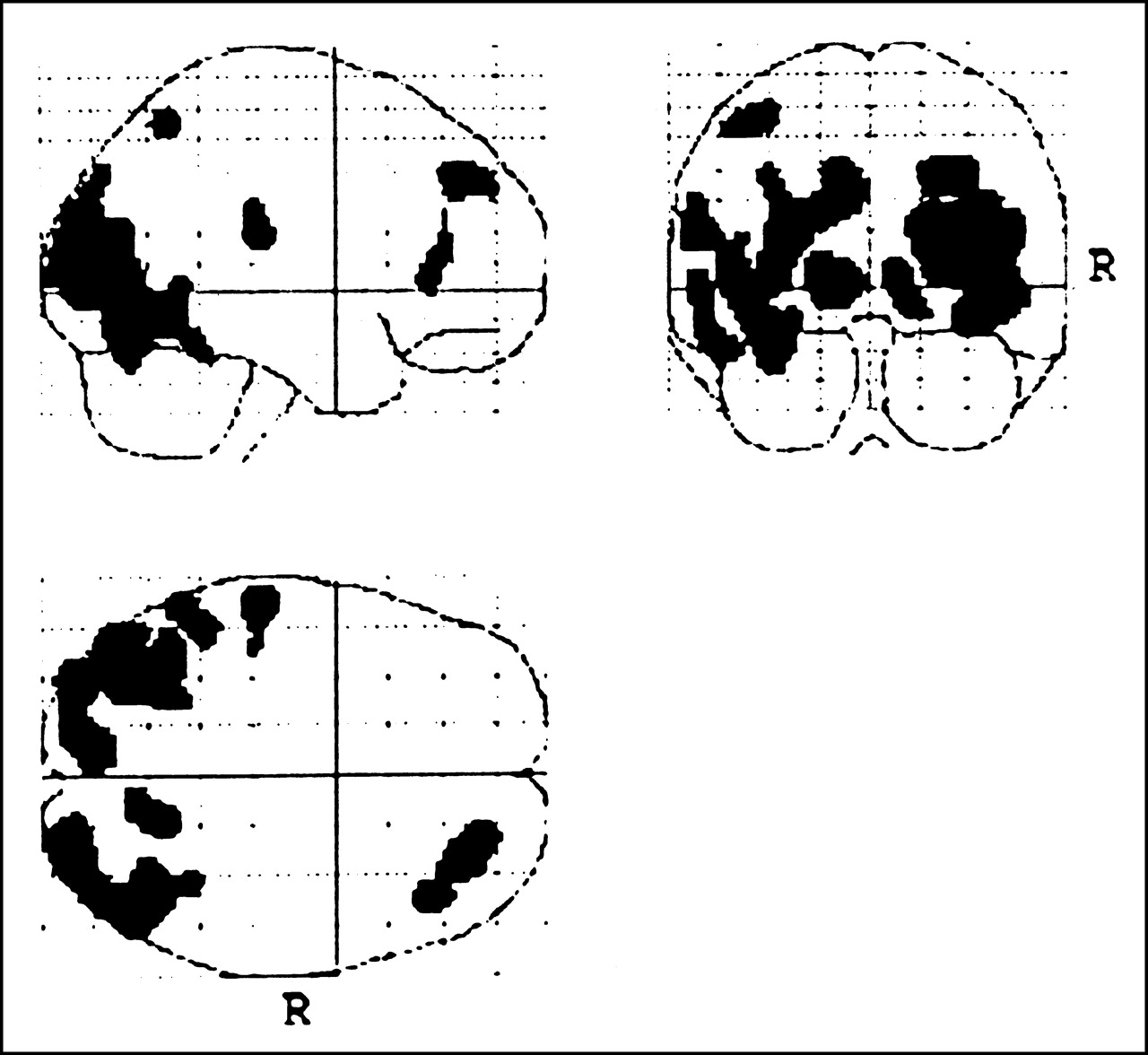
SPM maps of SPECT data from 13 patients with MDD but no occipital defects and from 18 control subjects. Only data in right frontal region achieved statistical significance (Table 2).
RESULTS
Figure 1 shows statistical parametric maps in 3 projections of SPECT data from the 8 patients with occipital rCBF deficits and from the control subjects. The SPM statistical analysis identified 2 statistically significant clusters of voxels with lower rCBF in patients than in control subjects (k, Table 1). One cluster was in the left occipital region, and the other in the right. Each had 3 noncontiguous but highly statistically significant maxima (z, Table 1). Although these highly significant localizations were in Brodmann’s areas 18 and 19—the occipital region occupied by the visual association cortex—the visual cortex proper did not show reduced rCBF. Figure 2 shows the statistical parametric map from the 13 patients whose scans did not show occipital flow deficits and from the control subjects. In this group, only 1 set of voxel clusters was large enough to be statistically significant (k, Table 2). Located in the right frontal gyri, this set had noncontiguous but highly statistically significant maxima (z, Table 2). The spatial extents of 3 additional clusters in the left frontal region and the left and right prefrontal regions (Fig. 2) were not significant (P = 0.12, 0.17, and 0.24, respectively), possibly because of a type II error from the small sample size. All 3 left frontal clusters and both the left and the right prefrontal clusters had statistically significant maxima, with z scores of 0.001–0.007.
DISCUSSION
SPM assessment of the rCBF SPECT data derived from 21 children with MDD and 18 healthy children seemed to show a significant difference between 2 groups of patients whose scans showed rCBF deficits. One of these groups included 8 patients who, when compared with all control subjects, appeared to show significant rCBF deficits in the occipital regions, with possible frontal flow abnormalities as a lesser finding. The other group included 13 patients who showed several significant frontal clusters. This group had a tendency toward bilateral frontal and prefrontal abnormalities, if not in terms of entire clusters, at least in terms of statistically significant maxima (z scores). The basis for this difference in rCBF behavior in children with MDD is not known, but the difference has been observed in adults as well (2).
CONCLUSION
We believe that these findings should be explored further to learn their significance to the clinical status of patients and possible implications for diagnosis and treatment.
Footnotes
Received Nov. 6, 2000; revision accepted Mar. 9, 2001.
For correspondence or reprints contact: Frederick J. Bonte, MD, University of Texas Southwestern Medical Center, 5323 Harry Hines Blvd., Dallas, TX 75390-9061.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.