


Abstract
Cryptogenic stroke might relate to paradoxical embolism stemming from right-to-left shunt caused by patent foramen ovale (PFO). We performed radionuclide venography using the Valsalva maneuver, followed by 99mTc-macroaggregated albumin (MAA) brain SPECT to investigate the fate of emboli originating from the lower extremities. Methods: Ten patients (9 men, 1 woman; mean age, 61 ± 17 y) with PFO underwent radionuclide venography with and without the Valsalva maneuver on the whole-body image, followed by brain SPECT with 99mTc-MAA to determine the cortical uptake that would detect right-to-left shunt. After counts in each region of interest (ROI) were normalized by comparison with the averaged count, the distribution of MAA was compared with that of 99mTc–hexamethyl-propyleneamine oxime (HMPAO) brain SPECT by drawing ROIs on frontal, temporoparietal (anterior circulation territory), occipital, and cerebellar areas (posterior circulation territory). Results: The thyroid on the whole-body scan was visualized after the Valsalva maneuver in 2 of the 10 patients. In 7 of 10 patients, 56 ROIs in the visualized cortical uptake showed that the distribution of MAA correlated well with that of HMPAO according to the equation: HMPAO = −71.21 + 1.71 × MAA, (r = 0.575, P < 0.01). The excess difference in the relative counts in the posterior over anterior circulation territory was 5.6% and 16.1% of the HMPAO and MAA values, respectively. Conclusion: Brain SPECT with 99mTc-MAA was more sensitive than thyroid visualization in detecting right-to-left shunt. The excess flow in the posterior cerebral circulation indicated an increased likelihood of cerebral emboli originating from the lower extremities and indicated that the flow difference between HMPAO and MAA probably resulted from poor linearization of HMPAO in the high-flow area.
- cerebral embolism
- patent foramen ovale
- radionuclide venography
- 99mTc-microaggregated albumin
- brain SPECT
About 40% of ischemic strokes are not identified according to conventional criteria (1). Most authors agree that this type of cryptogenic stroke probably occurs because of paradoxical embolism caused by right-to-left shunt, such as patent foramen ovale (PFO), especially in younger patients (age, <55 y) (2–4). If PFO is present, the relative risk of developing cerebral infarction becomes 7.2–10 times higher than with healthy patients (5,6). Transesophageal echocardiography (TEE) is superior to transthoracic echocardiography (TTE) in identifying PFO (7–9). The size of the foramen ovale correlates with the occurrence of brain infarction (10); the Valsalva maneuver is more sensitive in detecting PFO compared with the basal condition (4,11). Venography performed on patients with cerebral embolization to survey deep vein thrombosis diagnosed only 9.5% with cryptogenic stroke (12). However, deep vein thrombosis should be looked for carefully in patients with cryptogenic stroke, because understanding the etiology of ischemic stroke is useful for the treatment of such patients. A radioactive tracer exceeding 10 μm in diameter can be visualized in the brain after injection into veins of the lower extremities in patients with right-to-left shunt, because embolic distribution through patent foramen ovale is frequent during stroke affecting posterior circulation (13).
We compared the visualization of thyroid and cortical uptake with or without the Valsalva maneuver to detect right-to-left shunt. We also assessed the regional distribution of possible emboli from veins of lower extremities to the brain using 99mTc-macroaggregated albumin (MAA) brain SPECT after radionuclide venography in patients with PFO confirmed by TEE.
MATERIALS AND METHODS
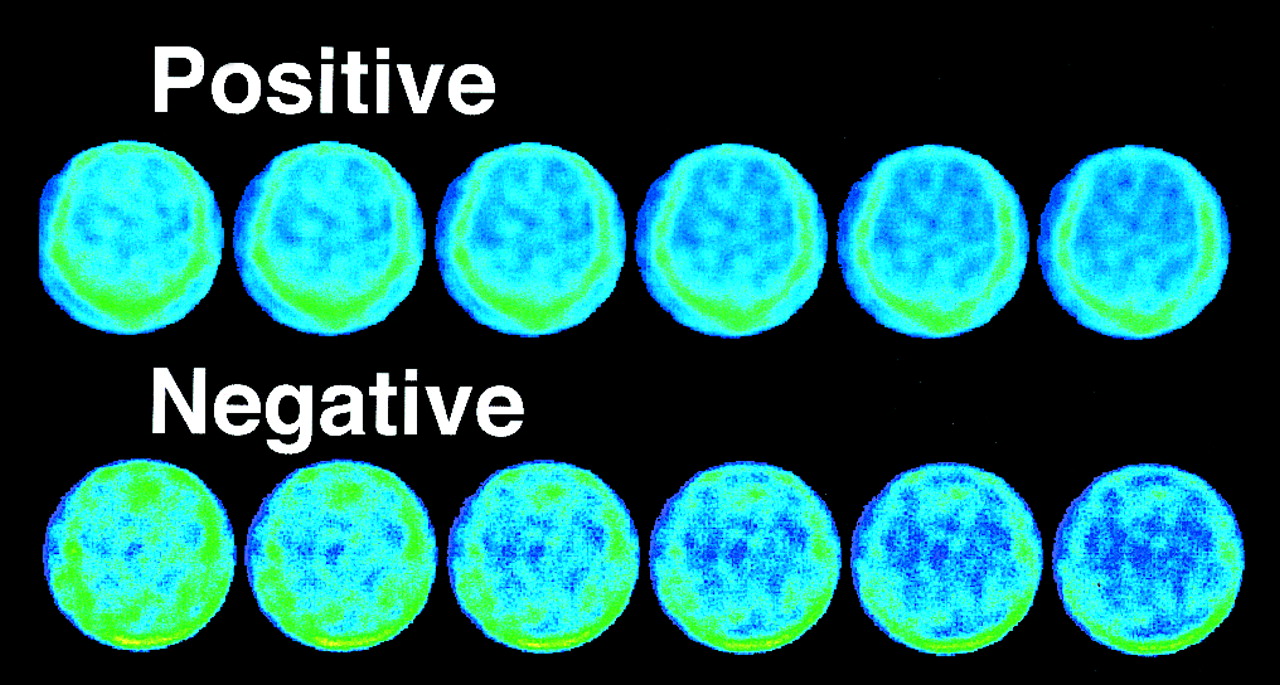
The severity of shunt was assessed by TEE using Lethen’s criteria, namely +, ++, and +++, representing < 10, 10–50, and > 50 microbubbles/3 s, respectively, with contrast echo (12). Radionuclide venography was performed twice to survey deep vein thrombosis—once under basal conditions and once after the repeated Valsalva maneuver. In other words, “with Valsalva” for 45 s and “without Valsalva” for 15 s was repeated during an injection of 185 MBq 99mTc-MAA (Nihon Mediphysics Co. Ltd., Nishinomiya, Japan) into both dorsal veins. One tourniquet was placed above the malleoli and one each was placed above and below the knee. Whole-body images of radionuclide venography were obtained from the injection site to the brain at a sweep speed of 80 cm/min. We assessed visualization of the thyroid with or without the Valsalva maneuver, of the cortical uptake (Fig. 1), and of perfusion defects in lung scans. Radionuclide venography and lung scans performed using a dual-head gamma camera (VERTEX; ADAC Laboratories, Milpitas, CA) with a 7-mm full width at half maximum (FWHM) were followed by brain SPECT with 99mTc-MAA. 99mTc-MAA brain SPECT was performed using a ring type gamma camera (Headtome SET 070; Shimadzu Co., Kyoto, Japan) with a 12-mm FWHM. SPECT image data were acquired over 30 min into a 128 × 128 matrix, using a general all-purpose collimator. All data were corrected for attenuation of 0.11 cm−1 and tomographic data were reconstructed using a filtered backprojection algorithm. Hence, transaxial 5-mm-thick slices were obtained. 99mTc-hexamethylpropyleneamine oxime (HMPAO) brain SPECT proceeded in the same manner as 99mTc-MAA brain SPECT except that the collimator was high resolution (8-mm FWHM) instead of general all-purpose resolution.
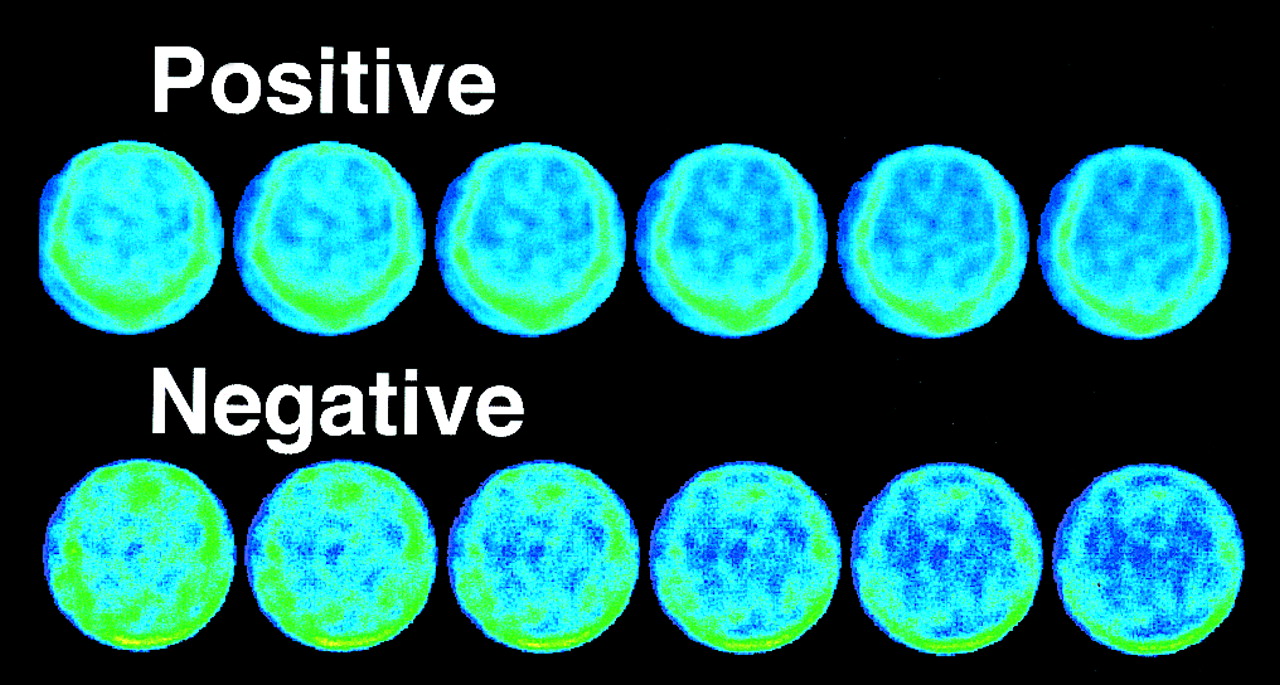
Criteria for cortical uptake visualization
To semiquantify the brain distribution, normalized mean counts in each region of interest (ROI) were obtained by standardization with the averaged count in all ROIs for each patient, using the following formula:
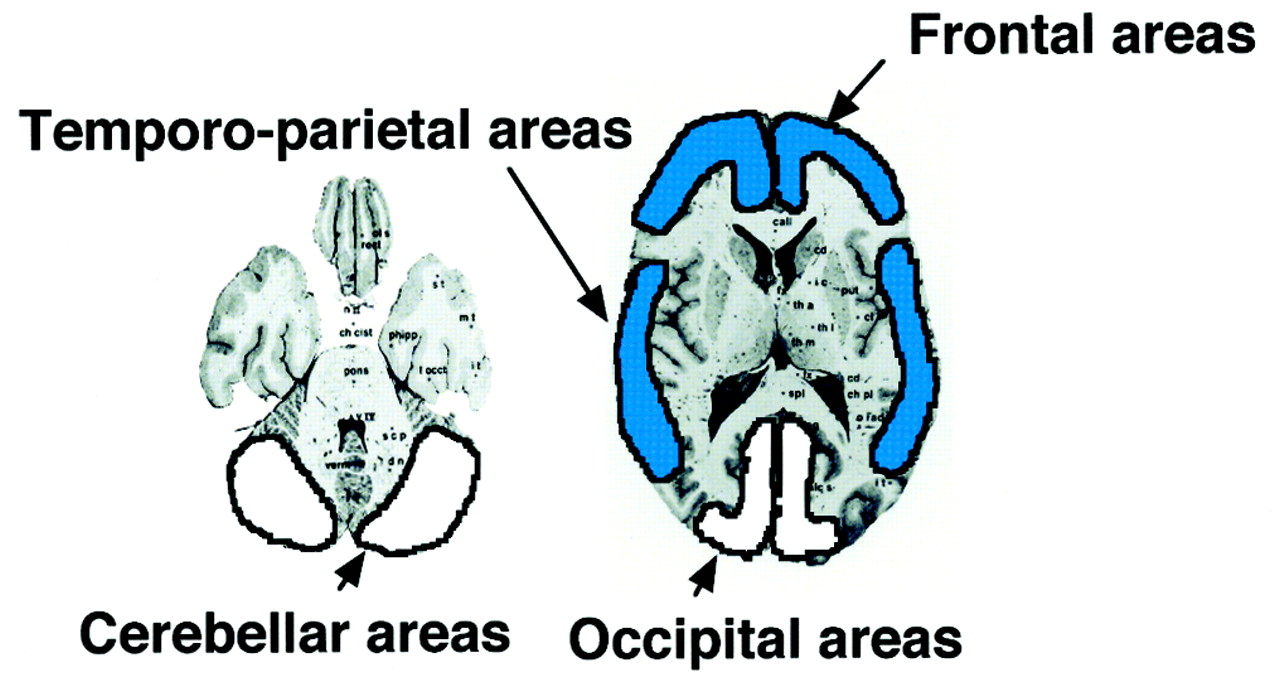
 By drawing ROIs on the frontal and temporoparietal areas (anterior circulation territory) and the occipital and cerebellar areas (posterior circulation territory) (Fig. 2), the distribution of 99mTc-MAA was compared with that of 99mTc-HMPAO taken 3–7 d after radionuclide venography. The profiles of the 10 patients (9 men, 1 woman; mean age, 61 ± 17 y) are described in Table 1. All results are expressed as mean ± SD. The significance of differences was calculated using the paired t test for comparison between anterior and posterior circulation territories with 99mTc-MAA and 99mTc-HMPAO brain SPECT. The significance of differences in thyroid visualization was calculated by χ2 test. A probability value of <0.05 was considered to be significant.
By drawing ROIs on the frontal and temporoparietal areas (anterior circulation territory) and the occipital and cerebellar areas (posterior circulation territory) (Fig. 2), the distribution of 99mTc-MAA was compared with that of 99mTc-HMPAO taken 3–7 d after radionuclide venography. The profiles of the 10 patients (9 men, 1 woman; mean age, 61 ± 17 y) are described in Table 1. All results are expressed as mean ± SD. The significance of differences was calculated using the paired t test for comparison between anterior and posterior circulation territories with 99mTc-MAA and 99mTc-HMPAO brain SPECT. The significance of differences in thyroid visualization was calculated by χ2 test. A probability value of <0.05 was considered to be significant.
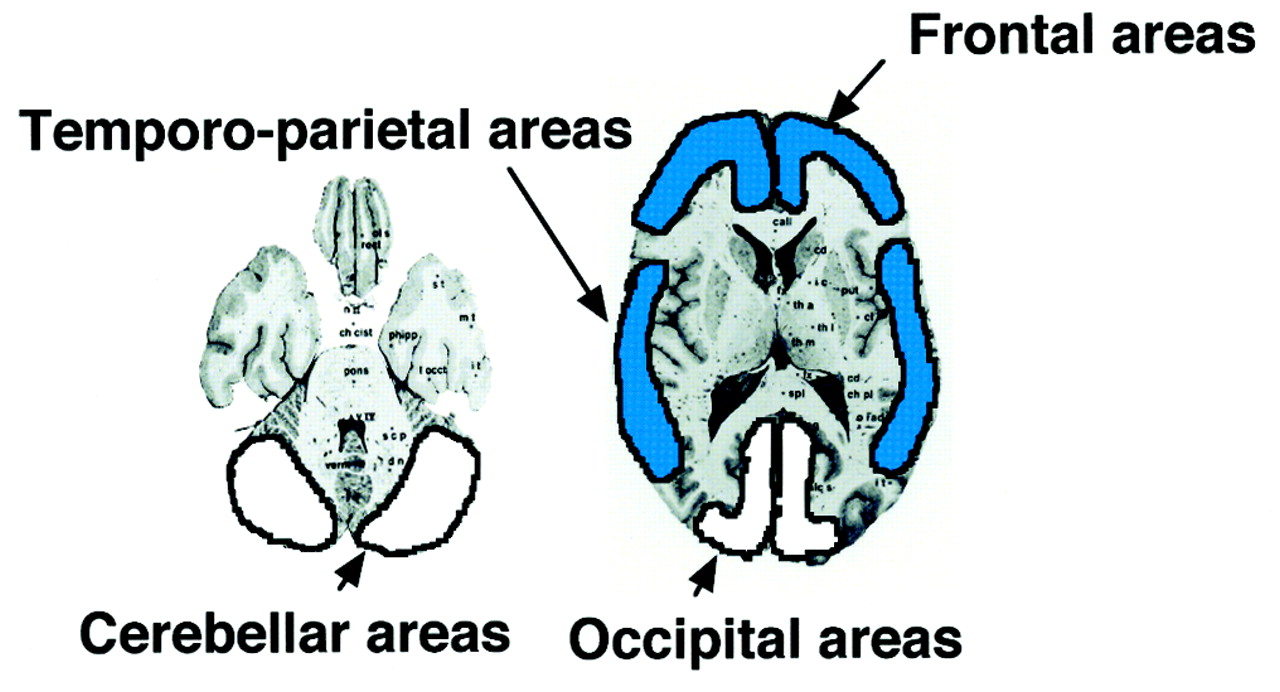
Placement of ROIs in middle cerebral arterial territory (shaded) and posterior cerebral arterial territory (white).
Patient Profiles
RESULTS
We performed 99mTc-MAA brain SPECT after radionuclide venography using the Valsalva maneuver to investigate the fate of emboli that originated in the lower extremities. All patients were confirmed as having PFO by TEE. After the Valsalva maneuver, the thyroid was visualized in 2 patients and the cortical uptake was visualized in 7 patients. No perfusion defects were detected in the lungs. The cortical uptake was visualized in all patients with atrial septal aneurysm (Table 1). Analysis of 56 ROIs from these 7 patients showed that the distribution of MAA correlated well with that of HMPAO according to the following equation: HMPAO = −71.21 + 1.712 × MAA (r = 0.576, P < 0.01) (Fig. 3). The standardized counts for HMPAO were 97.2 ± 4.2 in the anterior circulation territory and 103.0 ± 3.9 in the posterior circulation territory; for MAA the standardized counts were 91.4 ± 8.0 in the anterior circulation territory and 109.0 ± 14.5 in the posterior circulation territory (Fig. 4). Therefore, the mean count difference between the anterior and posterior circulation territories was 5.6% and 16.1% of the excess HMPAO and MAA, respectively, in the posterior circulation territory.
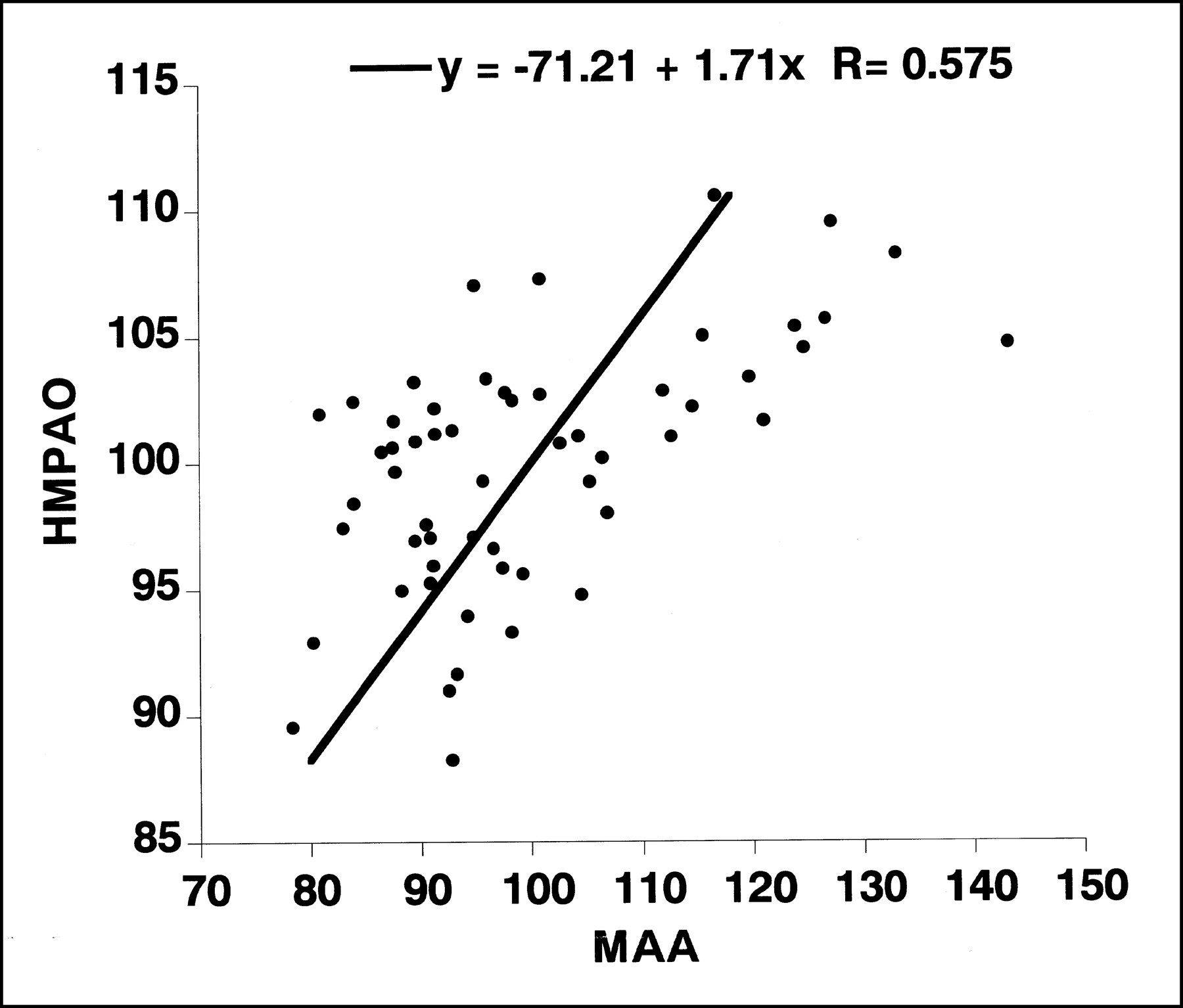
Correlation between HMPAO- and MAA-corrected counts in brain. *P < 0.01 vs. HMPAO.
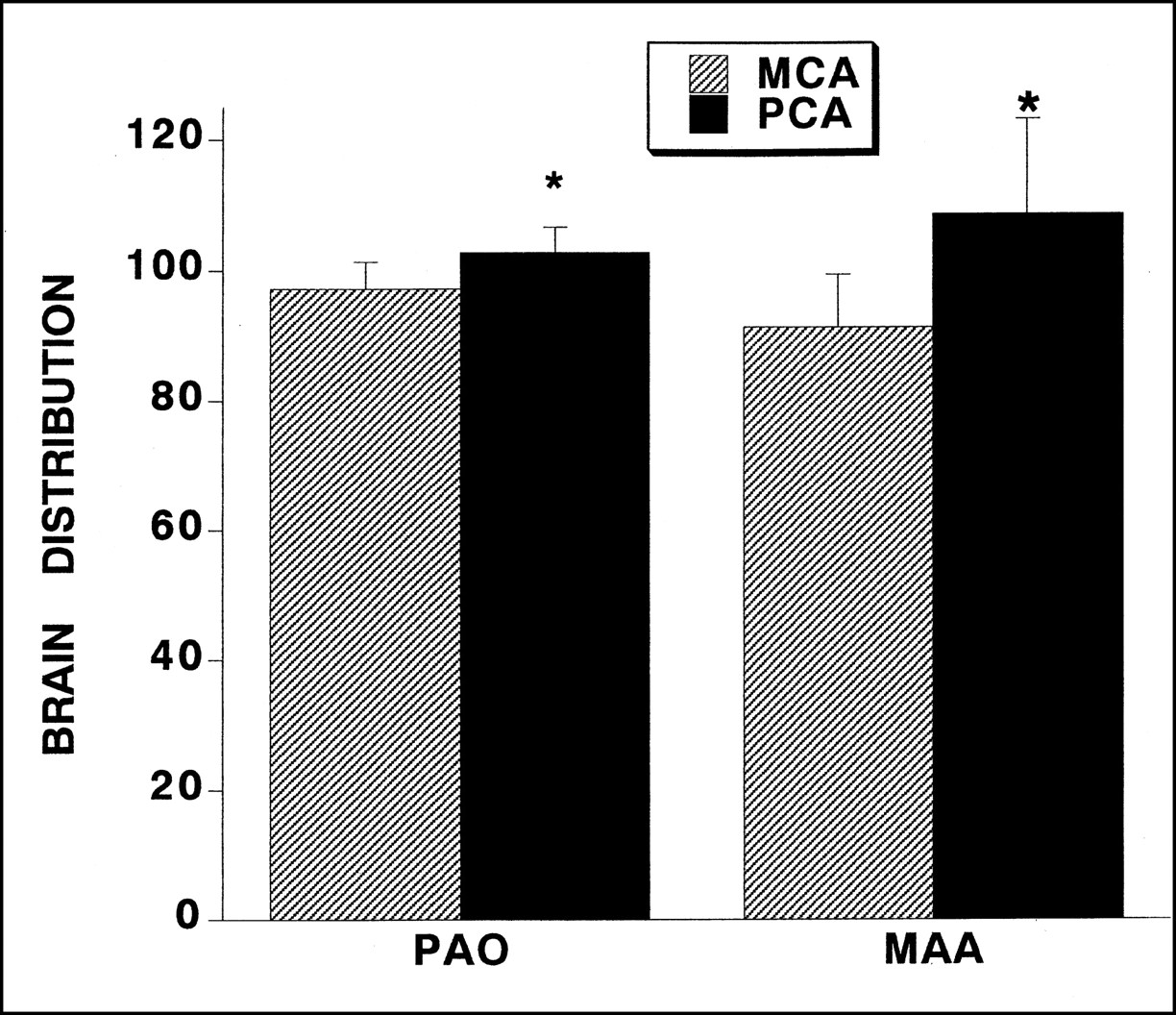
Distribution difference depending on anterior and posterior circulations of HMPAO- and MAA-corrected counts in brain (MCA, middle cerebral arterial territory; PCA, posterior cerebral arterial territory).
For example, a 22-y-old man developed an intractable headache in the occipital area during a rugby game. PFO with atrial septal aneurysm was detected by TEE, and radionuclide venography revealed the thyroid only after the Valsalva maneuver and patent deep veins accompanied by developed collaterals (Fig. 5A). MRI revealed a high intensity area in the left occipital territory and MR angiography indicated signal loss in the distal portion of the left posterior cerebral artery (Fig. 5B). 99mTc-MAA brain SPECT on day 12 showed the cortical uptake visualization in the cerebral cortex except for the left occipital area, where an increased accumulation on day 10 and hypoperfusion on day 23 were identified using 99mTc-HMPAO brain SPECT (Fig. 5C).

The example in this study, man (age, 22 y) with left occipital infarction. (A) Radionuclide venography demonstrated thyroid with Valsalva maneuver and patent deep veins accompanied by developed collaterals (L, left). (B) On day 17 MRI indicated high-intensity area in left occipital area and on day 19 MR angiography showed signal loss in distal portion of left posterior cerebral artery. (C) On day 12 99mTc-MAA showed defect in left occipital area (arrow), where 99mTc-HMPAO brain SPECT revealed hyperfixation on day 10 and hypoperfusion on day 23. MRA = MR angiography; PCA = posterior cerebral artery; T1 WI = T1-weighted image; T2 WI = T2-weighted image.
DISCUSSION
We performed 99mTc-MAA brain SPECT after radionuclide venography using the Valsalva maneuver to investigate the fate of emboli originating in the lower extremities. Ten patients with PFO underwent radionuclide venography with and without the Valsalva maneuver. In 2 of 10 patients the thyroid was visualized only after the Valsalva maneuver; in 7 of 10 patients the cortical uptake was visualized only after the Valsalva maneuver. In 56 ROIs of the 7 patients, the distribution of MAA correlated well with that of HMPAO. The count difference between the anterior and posterior circulation territories was 5.6% and 16.1% of the excess HMPAO and MAA, respectively, in the posterior circulation territory. The excess flow in the posterior cerebral circulation indicated an increased likelihood that cerebral embolism originated from the lower extremities, as the frequent stroke in that circulation was reported previously (13).
Without a right-to-left shunt, all injected tracers from the vein that exceed 10 μm are trapped in the lung capillaries. Once extrapulmonary accumulation such as in the thyroid and kidneys is visualized, the right-to-left shunt rate may exceed 18% (14). Because a PFO is found in 30% of patients at rest and in 50% during the Valsalva maneuver (4), the detectability of the right-to-left shunt must be enhanced under the latter conditions. The number of echogenic signals also increased in TEE during the Valsalva maneuver, correlating with the magnitude of right-to-left shunt better than under basal conditions (9). We combined the repeated Valsalva maneuver with radionuclide venography, because a transient right-to-left shunt might be boosted by elevating the pressure of the right atrium to exceed that of the left atrium because of the increased influx of venous return just after the cessation of the Valsalva maneuver (15). A large PFO may be more likely to cause paradoxical embolization and may explain the mechanism of stroke stemming from cryptogenic causes (10). However, our data indicated that thyroid visualization does not always correlate with the severity of PFO. We believed that even a small PFO might cause right-to-left shunting boosted by the Valsalva maneuver, the magnitude of which varied depending on the individual effort. TEE can differentiate the right-to-left shunt phenomenon but it cannot show how emboli are distributed in the brain. Our data showed that the distribution of MAA correlated with that of HMPAO, but the rate of blood flow in the posterior circulation was higher than that in the anterior circulation.
This may explain the frequency of stroke in the posterior circulation. The difference in brain distribution was 5.6% and 16.1%, HMPAO and MAA, respectively. The calculated difference between the anterior and posterior circulation was a 4.4% excess in the posterior circulation in a healthy patient (mean age, 40 y) (16), which is a relatively low difference. The age group from which these data were derived was younger than ours, which possibly suggests that aging reduced cerebral blood flow in the frontal areas.
The brain accumulates MAA in a different way than it does HMPAO. The former is an ideal tracer for blood flow measured by embolization of the cerebral arteries and the latter collects in the brain parenchyma by crossing the blood brain barrier because it is lipid soluble. Because a high flow range of HMPAO may be underestimated by the poor extraction fraction (17), the distribution of MAA and HMPAO in the brain should be different. When cerebral blood flow increases by more than 30% over the basal value in the visual cortex under conditions of daylight (18), the flow excess of the posterior circulation increases up to 50% higher than it does in the anterior circulation, which might explain the frequency of stroke in the posterior territory among patients with atrial septal aneurysm (19). When cryptogenic brain stroke is suspected, venography is used to explain paradoxical embolism from venous sources through a right-to-left shunt. But direct evidence for paradoxical embolism is usually absent, and systematic screening for deep vein thrombosis in the lower limbs or pelvis have generated extremely variable estimates (12). However, a report indicated that venous thrombosis does not correlate with cryptogenic stroke (20). Therefore a normal bilateral venogram does not rule out paradoxical embolism, because venous thrombosis may be localized in nonvisualized deep veins of the legs or the pelvis and the thrombosis may have undergone spontaneous lysis, complete embolization, or recanalization (21). In the present case, deep veins in the lower extremities were patent, but well-developed collateral veins may indicate previous deep vein thrombosis. We have stated that, in the case we describe, the ischemic stroke was probably elicited by the venous thrombosis in the lower extremities. The venous thrombosis likely traveled through PFO and reached the brain during a scrum in the rugby game and was conveyed by the blood flow to the left occipital area. The venous thrombosis was too large to lyse, resulting in the reperfusion injury that was revealed by HMPAO brain SPECT and that was referred to as hyperfixation in the subacute phase (22). Follow-up HMPAO brain SPECT was performed when the hyperfixed area subsided (13 d after venography) to avoid misinterpreting the area as increased cerebral blood flow.
CONCLUSION
We concluded that visualization of the cortical uptake using brain SPECT with MAA is more sensitive than that of the thyroid in detecting right-to-left shunt. The excess flow in posterior cerebral circulation indicated an increased likelihood of cerebral emboli originated from the lower extremities. Valsalva radionuclide venography and subsequent brain SPECT with 99mTc-MAA should be applied to identify a right-to-left shunt. These procedures can identify paradoxical embolism with visualization of brain embolism and can quantify embolic occurrence in the brain.
Acknowledgments
This work was supported by a Research Grant for Cardiovascular Disease (10C–8) from the Ministry of Health and Welfare.
Footnotes
Received Oct. 23, 2000; revision accepted Feb. 15, 2001.
For correspondence or reprints contact: Kohei Hayashida, MD, Department of Radiology, National Cardiovascular Center, 5-7-1 Fujishirodai, Suita, Osaka, 565-8565 Japan.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- An Approach to Working Up Cases of Embolic Stroke of Undetermined Source
- Provoked Right-to-Left Shunt in Patent Foramen Ovale Associates With Ischemic Stroke in Posterior Circulation
- Imaging Characteristics of Ischemic Strokes Related to Patent Foramen Ovale
- Paradoxical embolus to the brain from embolization of a carotid body tumor
- Right-to-left shunt does not increase white matter lesion load in migraine with aura patients
- Embolic Lesion Pattern in Stroke Patients With Patent Foramen Ovale Compared With Patients Lacking an Embolic Source
- First Clinical Experience with {alpha}-Emitting Radium-223 in the Treatment of Skeletal Metastases