


Abstract
The aim of the study was to determine whether the sentinel lymph node (SLN) can be accurately detected in cutaneous melanoma patients when the injection distance from the tumor site is expanded. Methods: In 100 patients with cutaneous melanoma, lymphoscintigraphy was performed twice. First, we injected 37 MBq 99mTc nanocolloid intracutaneously at a 2- to 5-mm distance from either the melanoma or the biopsy scar. The injection was followed by dynamic imaging, which continued until the SLN became visible. On another day, we repeated the investigation, injecting the radiopharmaceutical intracutaneously exactly 10 mm from the previous injection site. The detected SLNs of both investigations were compared to determine the number and location of SLNs for each patient. Results: The SLN identification rate was 94% with close injection and 100% with 10-mm-distant injection. All SLNs detected with close injection were visible with distant injection. In 84 of 100 patients, the images of both investigations showed the same number and location of SLNs. In the remaining 16 patients, an additional SLN was detected with the distant injection. Conclusion: The reproducibility of lymphoscintigraphy using different injection distances was 84%. The discordance in the remaining 16% was caused by detection of a lymph node in addition to the original SLN with distant injection. Diagnostic excision of the primary tumor before lymphoscintigraphy was possible without preventing detection of the original SLN. However, in 16% of our patients, excision of an additional lymph node had to be considered when lymphoscintigraphy was performed after diagnostic excision.
The surgical management of cutaneous melanoma patients has changed considerably in recent years because of the increasing use of the sentinel lymph node (SLN) approach. Published data suggest that lymphatic mapping and sentinel node biopsy in early-stage melanoma may become standard practice in lieu of elective lymph node dissection (1–5). Regional lymph node status is one of the most important predictors of disease progression (6,7). Therefore, accurate detection and precise excision of the SLN is necessary to evaluate the SLN status. Most patients with cutaneous melanoma undergo lymphoscintigraphy after diagnostic biopsy. This is necessary in deciding whether an SLN approach is appropriate. The criterion for lymphoscintigraphy and SLN excision is an invasion depth of more than 1 mm Breslow thickness (8). According to recent recommendations, a thin melanoma with an invasion depth of less than 1 mm is sufficiently treated by diagnostic excision with a 10-mm margin and does not need further treatment (5,6).
However, clarification is needed on whether a diagnostic excisional biopsy up to 10 mm from the primary tumor can alter the lymphatic flow such that the original SLN, which is associated with the primary tumor, is missed. Therefore, we chose a study design in which the radiotracer was injected at different distances. We examined whether different SLNs were detected by circularly expanding the injection distance by 1 cm.
MATERIALS AND METHODS
We consecutively investigated 100 patients with cutaneous melanoma (42 women, 58 men; age range, 24–78 y) after they had consented to participate. Eighty-one patients had undergone diagnostic biopsy (<1.0 cm margins) at least 1 wk before the lymphoscintigraphy, and in 19 patients the melanoma was still present. The invasion depth was less than 1.5 mm in 63 patients and greater than 1.5 mm in 37 patients. All patients were scheduled for wide excision of the primary site. Ten melanomas were on the head and neck, 49 were on the trunk, and 41 were on the extremities. The main patient characteristics are shown in Table 1. Patients with clinically known metastases were excluded from the study. In all patients, lymphoscintigraphy was performed twice. First, on the day before surgery, we injected approximately 30 MBq 99mTc-nanocolloid at four different sites (the 3-, 6-, 9-, and 12-o’clock positions; 0.1 mL per depot) intracutaneously between 2 and 5 mm from the intact primary melanoma or biopsy scar. Planar images were obtained until up to 1 h, and a delayed control image was obtained on the next day. Immediately after obtaining the control image, we injected the same amount of 99mTc-nanocolloid intracutaneously exactly 10 mm from the previous injection site, maintaining the same patient position. Figure 1 schematically presents the injection sites. The total injected volume of the radiotracer was 0.3–0.5 mL. All tracer preparations were made according to the same procedure by mixing 5 mL NaCl with 0.5 mg nanocolloid and 800 MBq 99mTc-pertechnetate. Therefore, the particle concentration was constant in each patient and for each investigation. We paid particular attention to avoiding subcutaneous injection. Immediately after intracutaneous injection, a dynamic acquisition was performed at one frame per 10 s using a 64 × 64 matrix, until the SLN became visible. Subsequently, frontal (256 × 256 matrix) and, if necessary, lateral and oblique static views were obtained at 30 min and 1 h after injection. The SLN was exactly localized using a handheld γ probe (C-Trak; Care Wise, Morgan Hill, CA). The SLN was marked on the skin with a water-resistant dye for the surgeon.
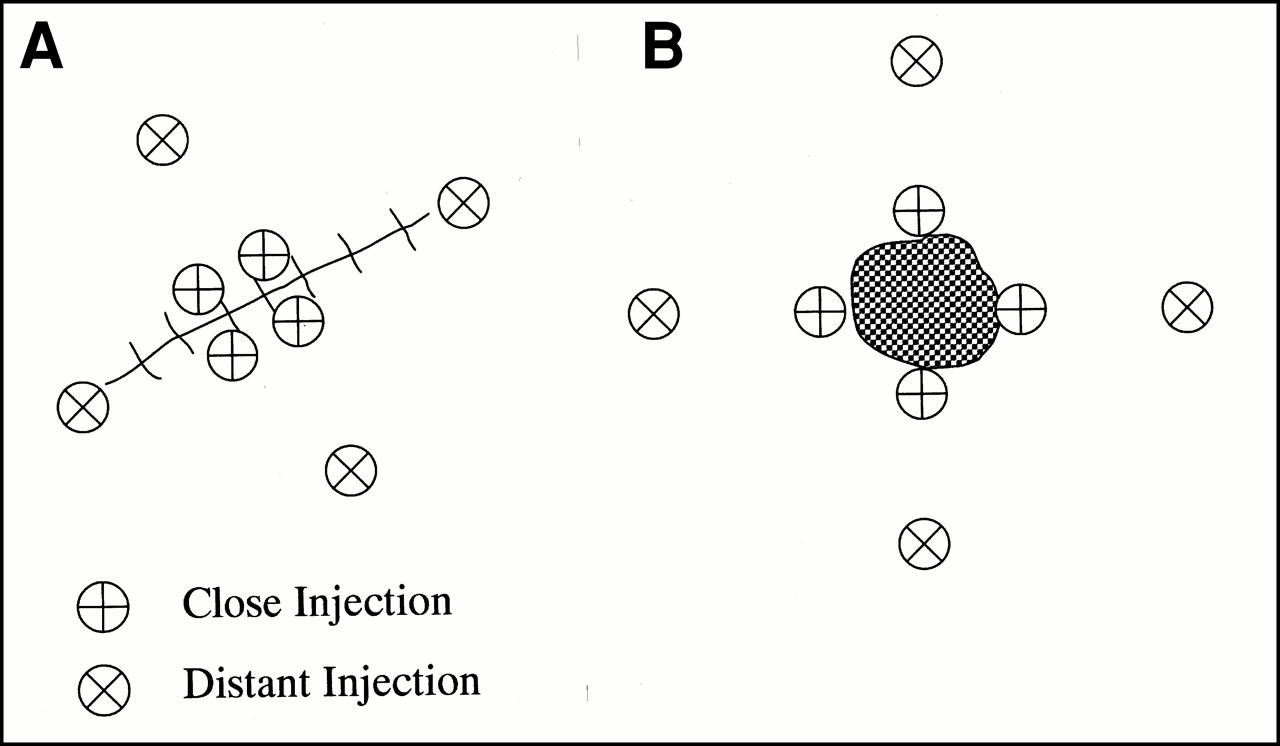
Schematic presentation of injection sites shows biopsy scar (A) and primary tumor (B), with four close injection sites ⊕ and four distant injection sites ⊗ 10 mm from close injection sites.
Patient Characteristics
Histologic Evaluation
The specimens were examined with hematoxylin–eosin staining. SLNs were further evaluated with immunohistochemical markers for S100 and HMB45.
Data Interpretation
The detected SLNs of the two investigations were compared to determine the number and location of SLNs. If one radioactive lymph node was visible, it was defined as the SLN. If more than one radioactive lymph node were in a basin, we defined any lymph node having a direct connection with the injection site as an SLN, independent of the intensity of radiotracer uptake and the time of appearance.
Recovery was defined as follows: If an SLN was localized through a close injection and detected through a distant injection, this SLN was recovered independently of the detection of an additional SLN. The Wilcoxon signed rank test was used to compare both injection sites according to the identification rate, number, and location of the SLNs in each patient. P < 0.05 was considered significant.
RESULTS
The SLN identification rate was 94% (94 of 100 patients) with close injection and 100% with 10-mm-distant injection and was statistically significantly higher for the distant injection (P < 0.05). With close injection, a single sentinel node was found in 53 patients; two nodes, in 25; three nodes, in 19; four nodes, in 1; and five nodes, in 2. The mean number of nodes per patient was 1.5. Comparing the location and quantity of radiolabeled lymph nodes for the two different examinations, we found that 84% (84 of 100 patients) had the same SLNs (Fig. 2). In 16 patients, an additional SLN was apparent on lymphoscintigraphy with 10-mm-distant injection, resulting in a mean of 1.7 nodes per patient. This discordance was found in 3 of 19 patients without excisional biopsy and in 13 of 75 patients with small excisional biopsy. In 3 patients with biopsy, an SLN could be found only with the distant injection.
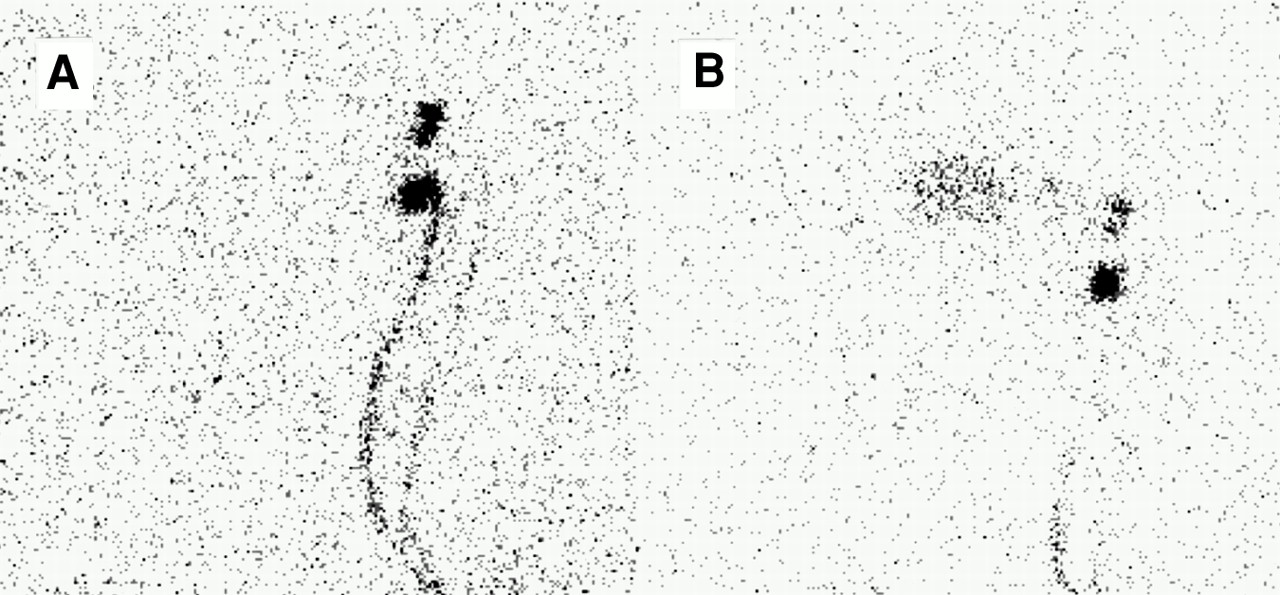
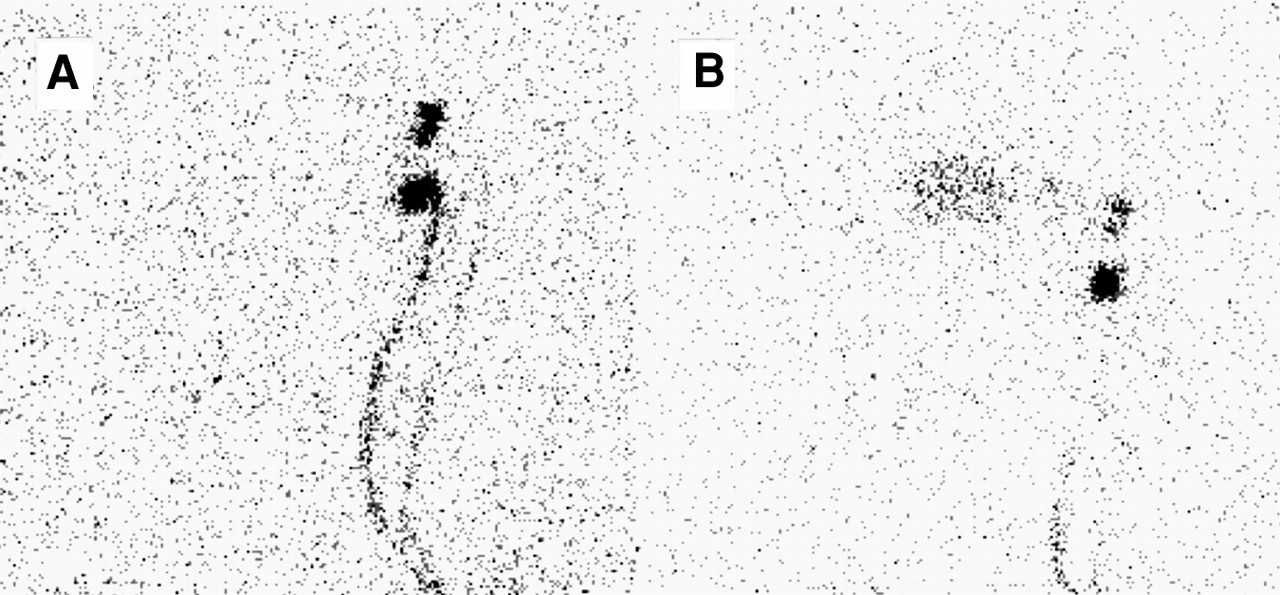
Comparison of lymphoscintigraphic images in patient with melanoma on lower leg. (A) Early close-injection image shows three sentinel nodes in left groin with different radiotracer uptake. Two afferent lymph channels are clearly visible, and one is discreetly visible. (B) Distant-injection image shows same sentinel nodes.
No SLNs were detected with close injection that were not detected with distant injection. All SLNs detected with close injection were recovered with distant injection. Comparing the patients with and without excisional biopsy, we found no statistically significant differences in identification rate and recovery (Table 2).
Lymphoscintigraphy Results in a Comparison of Close and Distant Injection for Cutaneous Melanoma
In 8 patients, the melanoma was at the midline of the trunk. A comparison of both investigations showed that SLN detection was concordant in 6 patients and partly discordant in 2 patients, with one additional SLN in one axillary basin with distant injection. A representative example is shown in Figure 3. No statistically significant differences from the other melanoma sites were seen.
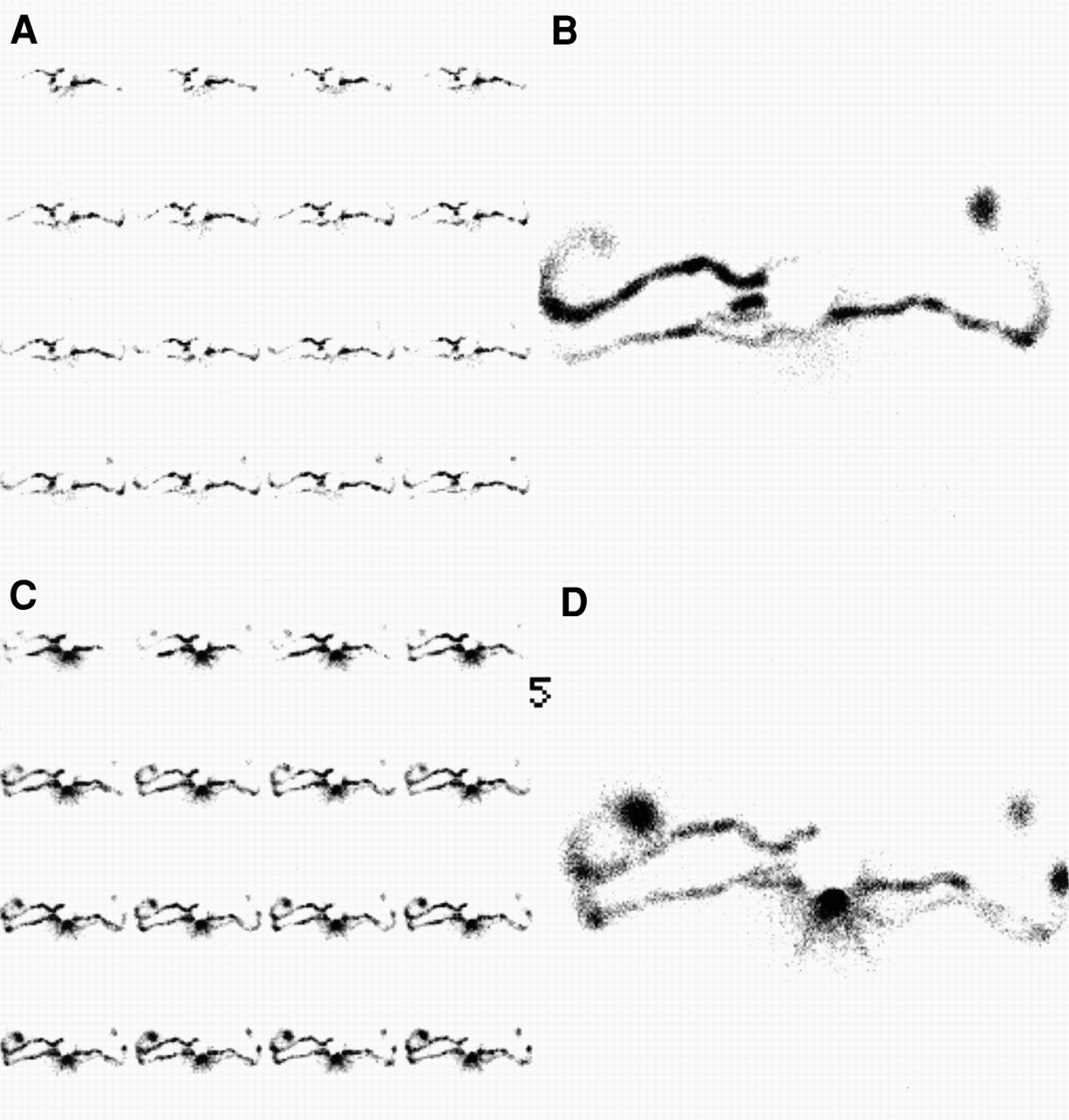
Comparison of lymphoscintigraphic images in patient with melanoma at midline of back. Injection sites are covered by lead sheet. Close-injection images (A and B) show convergence of several lymph channels toward single node in left axillary basin and one lymph channel to one SLN in right axilla. Distant-injection images (C and D) show additional lymph channel draining to additional SLN in right axilla. Dynamic image (C) shows delayed appearance of additional SLN.
The discordant or additional radioactive nodes were in the same draining basin in 13 patients and in an additional basin in 3 patients. In 2 of these 3 patients, the additional radioactive node was in the contralateral basin. In the third patient, in addition to the axillary basin, the ipsilateral inguinal basin contained one lymph node. Distant injection did not reveal any additional tumor-positive SLNs.
Comparison of Lymph Channels and Intensity of Tracer Accumulation in SLNs
In 90 patients, the lymph channels were visible at both investigations. In 76 patients, the lymph channels were identical; in 14 patients, the lymph channels were partly discordant, but they drained to the same SLNs in 8 patients. In 12 patients, an additional lymph channel draining to an additional lymph node was visible with distant injection (Fig. 3). In 10 (10%) of the 100 patients in whom more than one SLN was detectable in a lymphatic basin, the most intense node was not the same in both studies (Fig. 4). In 25 patients (25%) with more than one radioactive lymph node in a basin, the afferent lymph channel could be visualized to define a lymph node as an SLN.
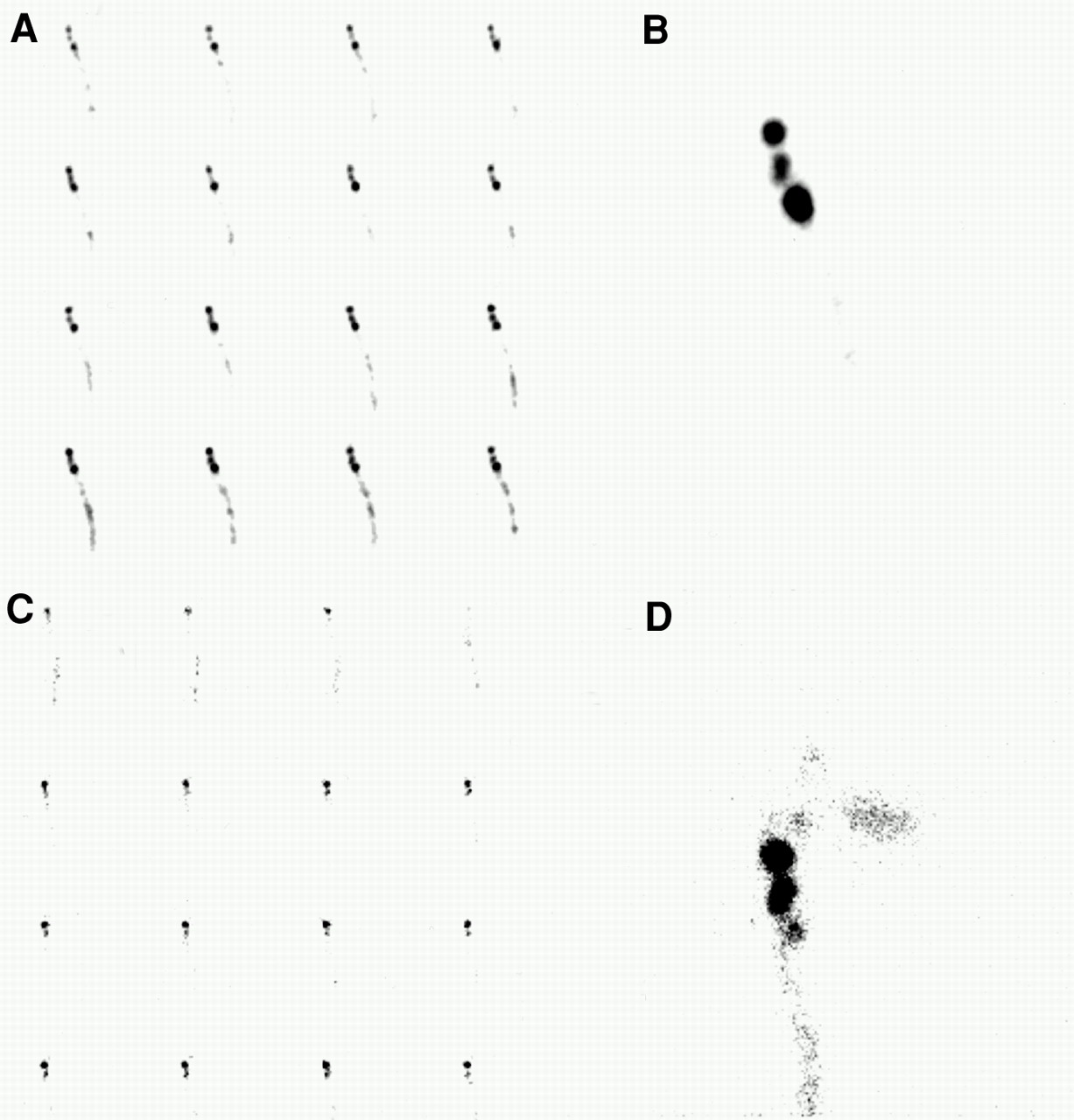
Comparison of lymphoscintigraphic images in patient with melanoma on lower leg. Close-injection images (A and B) show three sentinel nodes in left groin. Only one lymph channel is visible. Distant-injection images (C and D) show same sentinel nodes but with different uptake of radiotracer. Dynamic image (C) shows earlier appearance of lymph node lying more distant from injection site.
Incidence of Metastases
In 12 patients (12%), one SLN was tumor positive. Only 1 patient had a Breslow thickness less than 1.5 mm. In all these patients, SLN detection was the same for the two injection modalities.
DISCUSSION
Diagnostic excision of the primary tumor, with an excisional distance of up to 10 mm from the clinically visible margin of the melanoma, is normally performed before SLN excision. The reason for injecting the radiotracer up to 10 mm from the melanoma margin is the reduced area caused by melanoma removal. Whether diagnostic biopsy can prevent detection of the original SLN is unknown.
A literature review shows that repeated injection of a radiopharmaceutical at the same skin region reveals different numbers and locations of SLNs in 10% of patients (9,10). In our study, the distance between injection sites was 20 mm (10 mm in each direction). Therefore, we expected greater discordance in SLN detection than that reported in the literature for use of different injection sites. Our study showed that SLN identification was reproducible in 84% of patients. Discordance was evident in 3 of 19 patients without excisional biopsy and 13 of 75 patients with small excisional biopsy. However, decisive for identification of SLN status is not reproducibility but the ability of distant injection to detect all SLNs that were detected with close injection. We found this ability for 100% of the SLNs that were detected with close injection.
A point of discussion is whether disruption of the cutaneous lymphatics by excisional biopsy alters lymphatic flow to the sentinel node. Our study showed that circular expansion of the injection distance by 1 cm did not impede the detection of SLNs. This finding is consistent with retrospective findings after wide local excision of primary melanoma (11). Those findings, and ours, imply that the area draining a melanoma site is larger than the area excised in small excisional biopsy. Because the draining areas of SLNs overlap considerably, wider injection results in detection of additional SLNs. This fact may explain our detecting additional lymph nodes when injecting the radiotracer at a distance of 10 mm rather than close. The result was that in 16% of our patients, excision of an additional lymph node was needed because of previous tumor excision. Kapteijn et al. (9) reported a 12% discordance (3/25 patients) when injecting the radiotracer in a manner identical to ours. Similar to us, the authors found not complete discordance but only one additional lymph node in 3 patients. These findings, and ours, imply that distant injection may detect SLNs more accurately. However, none of the additional detected lymph nodes were tumor positive in either study. We cannot conclude that distant injection is more accurate at detecting SLNs just because more lymph nodes can be detected. We suggest that diagnostic excision of the primary tumor can be performed without preventing the original SLN from being found.
The comparison of lymph channels using different injection sites revealed concordance in 76% of patients. In 14%, the lymph channels were partly discordant, that is, if more than one lymph channel into a lymph basin were visible, only part of the channels was different. Despite this discordance, the SLNs detected in the two studies were identical in 8 patients. This high correlation of lymph channels in both investigations supports the assumption that draining areas of SLNs have large, overlapping fields. The SLN may be difficult to determine when more than one lymph node is seen in the lymphatic basin. The visualization of lymph channels has great importance in the identification of an SLN. When a lymph vessel is found to be connected to a lymph node, that lymph node is an SLN. This determination is not dependent on the intensity of tracer uptake. The SLN is not necessarily the most intense node in the lymphatic basin (Fig. 4). It is necessary to detect the lymph vessels using sequence images, positioning the detector close to the patient’s skin and using a concentrated radiotracer (30 MBq in 0.2 mL). In 25 patients with more than one radioactive lymph node in a basin, we could define a lymph node as an SLN by visualization of the lymph channels using the dynamic and early images (Fig. 2). This ability is consistent with the finding of Glass et al. (12) that lymph channels were visualized clearly on early images and poorly on delayed images. We used 99mTc-nanocolloid having a particle size of 5–80 nm. The SLNs were visualized within 20 min after administration in 92% of patients. The fact that an average of 1.5 SLNs per patient were detected and the fact that lymph channels could be visualized in 90% of patients qualify 99mTc-nanocolloid as an ideal tracer. This statement is in agreement with reports comparing 99mTc-labeled human serum albumin and 99mTc-labeled sulfur colloid (12,13).
Like other investigators (9,10), we were not able to detect an SLN with close injection in all patients. The 6 patients in whom detection was not possible had undergone excisional biopsy, and in all, an SLN could be found with distant injection. In 4 of these patients, inflammation of the excision scar was present and could have caused the failure to detect an SLN. In the other 2 patients, the excision had been performed 4 wk previously, so granulation and fibrous tissues may have prevented lymphatic flow. These findings indicate that the radiotracer should be administered farther from the scar when it is inflamed or when granulation tissue is extensive.
CONCLUSION
Our study showed that lymphoscintigraphy was reproducible in 84% of patients when different injection distances were used. The discordance in the remaining 16% was caused only by the fact that distant injection detected a lymph node in addition to the original SLN. All SLNs detected with close injection were recovered with distant injection. Small excision of the primary tumor was possible without preventing detection of the original SLN. In 16% of patients with small excisional biopsy, excision of an additional SLN had to be considered.
Footnotes
Received Feb. 22, 2000; revision accepted Jun. 20, 2000.
For correspondence or reprints contact: Lukas Rettenbacher, MD, Landeskrankenhaus Salzburg, Müllnerhauptstrasse 48, A-5020 Salzburg, Austria.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Accuracy and Reproducibility of Lymphoscintigraphy for Sentinel Node Detection in Patients with Cutaneous Melanoma
- The Role of Interval Nodes in Sentinel Lymph Node Mapping and Dissection for Melanoma Patients
- Reproducibility of Cutaneous Lymphoscintigraphy: Same or Different Lymphatic Routes and Sentinel Nodes After Reinjection?