


Abstract
In this prospective study, somatostatin receptor (SS-R) scintigraphy was compared with conventional staging procedures for the initial staging of patients with low-grade non-Hodgkin’s lymphoma (NHL). Methods: Fifty consecutive untreated patients with low-grade NHL underwent SS-R scintigraphy as part of their initial staging. Planar images were obtained 24 and 48 h after intravenous injection of 220 MBq 111In-pentetreotide. SPECT images of the upper abdomen were obtained from all patients. SS-R scans were evaluated blindly without knowledge of the results of the conventional staging methods. SS-R scintigraphy findings were compared with the results of physical and radiologic examinations. Results: SS-R scintigraphy findings were positive in 42 of 50 patients (84%). In 10 patients (20%), the SS-R scan revealed new lesions that had not been revealed by conventional staging procedures. These 10 patients were all upgraded to a higher stage. Consequently, the treatment plan would have been altered in 5 patients (10%). However, in 19 patients (38%), lesions apparent after conventional staging methods were missed by SS-R scintigraphy. The sensitivity of SS-R scintigraphy varied from 62% for supradiaphragmatic lesions to 44% for infradiaphragmatic lesions. The specificity of SS-R scintigraphy was high (98%–100%). In comparison with CT scanning and sonography, SS-R scintigraphy is inferior for the visualization of NHL lesions in the thorax and abdomen. Conclusion: Although SS-R scintigraphy findings are positive in a large proportion of patients with low-grade NHL, in most patients only part of the lesions can be visualized. Because of the limited sensitivity, we recommend SS-R scintigraphy for initial staging of patients with low-grade NHL only in selected conditions and not for the general work-up.
Low-grade non-Hodgkin’s lymphomas (NHLs) often present as disseminated disease. Bone marrow involvement is frequently seen. The survival curves reveal a progressive decline with no indication of a plateau, providing no evidence of a cure. The median survival is ∼8 y (1). Local irradiation can result in prolonged freedom from progression and possibly a cure in approximately half of patients with stage I and small-volume stage II low-grade NHL (2,3). Therefore, for low-grade NHLs, staging is important to identify patients with truly localized disease who may be cured by radiotherapy.
Somatostatin receptors (SS-Rs) are present in a wide variety of human tumors (4). The radiolabeled SS analog [111In-diethylenetriaminepentaacetic acid-d-phenylalanine]-octreotide has been used successfully for in vivo visualization of SS-R positive tumors (4). With in vitro autoradiography, SS-R presence was shown in lymph nodes with NHLs. Of 11 low-grade B-cell NHLs, 10 were SS-R positive, and a high receptor density was restricted to the neoplastic follicles (5).
Studies evaluating the clinical impact of SS-R scintigraphy for the staging of NHLs are rare, and they are all based on relatively small numbers of patients and heterogeneous patient groups (6–13).
We report the results of a prospective study of 50 patients newly diagnosed with low-grade NHL in which the value of SS-R scintigraphy was assessed.
MATERIALS AND METHODS
Patients
Fifty consecutive, newly diagnosed and previously untreated patients with low-grade NHL were enrolled in a prospective study. The diagnosis of low-grade NHL was substantiated by histologic and immunohistologic methods and was classified according to the Working Formulation (14). The stage of the disease according to the Ann Arbor classification (15) was established by conventional methods that always included a physical examination; inspection of the Waldeyer’s ring by an ear, nose, and throat specialist; chest radiography; CT scanning of the chest, abdomen, and pelvis; and sometimes sonography of the neck or abdomen. The diagnosis of bone marrow involvement was always verified after cytologic, immunologic, and histopathologic examination of marrow aspiration and biopsy. CT scanning was performed with contiguous 10-mm axial sections after oral and intravenous administration of contrast material. All patients gave informed consent to the study, which was approved by the ethics committee of the University Hospital Rotterdam.
SS-R Scintigraphy
The maximum interval between conventional staging procedures and SS-R scintigraphy was 3 wk. All examinations were completed before initiation of therapy. Patients were injected intravenously with 220 MBq 111In-pentetreotide (OctreoScan; Mallinckrodt, Inc. BV, Petten, The Netherlands). Planar total body scintigraphy was performed 24 h after injection with a large-field-of-view gamma camera (Counterbalance 3700 and ROTA II; Siemens Gammasonics, Erlangen, Germany) equipped with a medium-energy collimator. Repeated scintigrams were obtained 48 h after injection, when accumulation of radioactivity in the abdomen was observed on 24-h scintigrams. Laxatives were given to reduce intestinal radioactivity caused by some hepatobiliary clearance of 111In-pentetreotide. Head and neck images were obtained anteriorly and laterally from both sides. The remainder of the body was imaged with separate anterior and posterior images of the thorax, upper abdomen (including liver/spleen and kidneys), lower abdomen, and extremities. The thorax was imaged with arms elevated. Preset counts were 300,000 for the head and neck and 500,000 for the thorax and abdomen, or a maximum of 15 min. In all patients, SPECT images of the upper abdomen were made 24 h after injection using a triple-head camera (3000XP; Picker, Cleveland, OH). SPECT data were reconstructed by filtered backprojection. A detailed description of the scanning protocol is given in several reviews (16–18). In healthy individuals, a physiologic accumulation of radioactivity may be seen 24 h after injection of 111In-pentetreotide in the pituitary gland, thyroid gland, liver, spleen, kidneys, intestines, urinary bladder, and, frequently, the gallbladder. Accumulation of radioactivity at other sites is considered to be abnormal and indicates the presence of pathologic SS-R positive tissue. In organs with physiologic uptake of 111In-pentetreotide (e.g., liver and spleen), inhomogeneous or focal uptake patterns were considered to be indicative of lymphoma. Independent, blinded evaluation of SS-R scans was performed by two experienced nuclear medicine physicians at the same time. If the initial interpretations were different (occurring in <5% of patients), a blind discussion was held until consensus was reached. The intensity of pathologic uptake of 111In-pentetreotide in the lesions observed on the planar images was graded semiquantitively as follows: grade 0 = negative, no abnormal activity; grade 1 = equivocally positive, small amount of accumulation of radioactivity; grade 2 = clear accumulation of radioactivity, intensity less than that of the liver; and grade 3 = clear accumulation of radioactivity, intensity equal to or greater than that of the liver. The SS-R scan was considered positive in any given patient if at least one of the identified lymphoma lesions was positive on the scan (grade 1, 2, or 3).
Assessment of True State of Lesion or Region
CT scans and other radiologic tests were evaluated by experienced radiologists without knowledge of the SS-R scintigraphy data. Lymph nodes >15 mm in diameter were considered unequivocally abnormal on CT scanning or sonography and were interpreted to represent NHL. Lymph nodes < 10 mm were considered benign. Lymph nodes with a diameter of 10–15 mm were considered equivocal. CT and sonography criteria for involvement in a normal-sized spleen or liver included unexplained infiltrates or focal abnormalities of decreased attenuation. The spleen was considered enlarged on CT, sonogram, or SS-R scan if the longitudinal diameter was >130 mm (19,20).
Findings of SS-R scintigraphy were compared with the sum of the results of conventional staging procedures. The following lymph node regions were evaluated: occipital left/right, upper cervical left/right, medial cervical left/right, preauricular left/right, submandibular left/right, supraclavicular left/right, infraclavicular left/right, axillary left/right, brachial left/right, mediastinal, lung-hilar left/right, paraaortic (including celiac nodes and nodes from the hepatic and splenic hili), iliac left/right, inguinal left/right, femoral left/right, popliteal left/right, mesenteric, and the Waldeyer’s ring. In addition, all extranodal sites of potential involvement were also evaluated. This process resulted in a total of 70 possibly involved lymph node regions and extranodal sites. In cases of disagreement between findings in SS-R scintigraphy and conventional staging procedures, we attempted to determine the status of the lesion. Status was verified if possible by biopsy or using noninvasive methods, including sonography, MRI, CT, or bone scintigraphy. All patients were followed during and after therapy. For any documented lesion, a final assessment was made of its true state as benign, malignant, or indeterminate. This assessment was based on the result of the pathologic examination (histology or cytology if done) supplemented by the clinical course. A lesion was considered benign because of pathologic evidence, or if the long-axis measurement was <10 mm and the lesion did not increase in size. A lesion was considered malignant because of pathologic evidence, or if the largest diameter was >15 mm, or in retrospect on the basis of the clinical course (disappearance or change in size of a lesion of >10 mm after therapy). The status of the lesion was considered indeterminate if the nature of the lesion could not be assessed from the data. Regions without lesions on any test were considered to have a true state of absence of disease. The spleen was considered positive for NHL if there was unequivocal palpable splenomegaly alone or equivocal palpable splenomegaly with radiologic confirmation of either enlargement or multiple focal defects that were neither cystic nor vascular. Liver involvement was diagnosed if there were multiple focal defects that were neither cystic nor vascular, noted with at least two imaging techniques.
Assessment of Sensitivity and Specificity of a Test
The sensitivity and specificity of the different tests were calculated separately for each of the regions for which each test was performed. For the calculation of sensitivity, the lesions with a true state of malignancy were used, whereas for the calculation of specificity, the regions with no lesions or only lesions with a final assessment of benign were used. The sensitivity of a test for a lymph node region or extranodal site was defined as the number of lesions with a positive test result for that region divided by the total number of lesions with a final assessment of malignant in that region. The specificity of a test for a lymph node region or extranodal site was defined as the number of patients with a negative test result divided by the total number of patients tested with a true state of benign/absent in that region.
RESULTS
Patients
The clinical characteristics of the 50 patients with low-grade NHL enrolled in the study are listed in Table 1. Follicular lymphoma constituted 64% of the histologies. There were 9 patients (18%) with a lymphoma of mucosal-associated lymphoid tissue (MALT). Immunophenotypically, all NHLs were of B-cell origin. Localized disease (i.e., stages I or II) was more common (60%) than advanced disease (40%). Details of the anatomic distribution of the malignant lesions are given in Table 2. Lymph nodes in the neck were involved in 56% of the patients. Approximately half of the patients (52%) presented with infradiaphragmatic disease. Below the diaphragm, the para-aortic region and the mesenteric and inguinal lymph nodes were most frequently involved. The most common sites of extranodal involvement were the stomach and orbita/eye. Bone marrow infiltration with NHL was apparent in 22% of patients.
Clinical Characteristics of 50 Patients with Low-Grade NHL
Anatomic Distribution of 162 Malignant Lesions in 50 Patients with Low-Grade NHL
Patient-Related Sensitivity of SS-R Scintigraphy
The SS-R scan was positive in 42 of 50 patients (84%). An entirely negative scan was seen in 8 of 50 patients (16%). In 4 of 9 patients (44%) with a MALT lymphoma, the SS-R scan was negative; 2 had gastric lymphoma and 2 had ocular lymphoma. The SS-R scans in the other 5 patients with MALT lymphoma were positive; 2 had lymphoma of the stomach, 1 had lymphoma of the parotid gland, 1 had lymphoma of the orbit, and 1 had lymphoma of the orbit, stomach, intestine, spleen, and abdominal lymph nodes.
Comparison of SS-R Scintigraphy with Conventional Staging Procedures
Table 3 compares the results of SS-R scintigraphy with those of conventional staging (exclusive bone marrow examination) in the 50 patients. In 10 patients (20%), the SS-R scan revealed new lesions suggestive of NHL that were not revealed by conventional staging procedures. We were unable to verify the discrepant findings in these 10 patients because of ethical considerations, lack of patient consent, or lack of therapeutic consequences. In 19 patients (38%), lesions apparent after conventional staging were missed on SS-R scintigraphy. Furthermore, in 3 patients (6%), the results of the comparison were mixed; that is, in the same patient, new lesions were disclosed by SS-R scintigraphy and other lesions were missed. Finally, the results of SS-R scintigraphy and conventional staging procedures were concordant in 36% of the patients.
Comparison of Results of SS-R Scintigraphy with Those of Conventional Staging in 50 Patients with Low-Grade NHL
Table 4 shows the clinical stage based on conventional staging procedures (excluding the bone marrow evaluation) in comparison with the clinical stage based on conventional staging procedures complemented with SS-R scintigraphy. Because of the different SS-R scintigraphy findings, the clinical stage was upgraded in 10 patients (20%). As a result, the treatment plan would have been altered in 5 patients (10%). On the other hand, in 12 patients (24%), in whom SS-R scintigraphy missed certain apparent localizations of NHL, the clinical stage would have been underestimated when based only on the results of SS-R scintigraphy.
Clinical Stage Based on Conventional Staging Procedures Complemented with SS-R Scintigraphy Compared with Clinical Stage Based on Conventional Staging Only
Lesion-Related Sensitivity and Specificity of SS-R Scintigraphy
In the 50 patients, a total of 162 malignant lesions were distinguished from the physical examination in combination with SS-R scintigraphy, other imaging techniques, histopathology, and the outcome of subsequent follow-up. Of these, 95 lesions were localized above the diaphragm, 64 lesions were below the diaphragm, and 3 were elsewhere. A minority of the lesions were extranodal (n = 20). Table 5 gives the sensitivity of SS-R scintigraphy for detecting lymphoma in each of the lymph node regions and extranodal sites. For supradiaphragmatic nodal lesions, the sensitivity varied from 59% to 78% (Fig. 1). The sensitivity was best for lesions in the mediastinum (78%). The smallest NHL lesion above the diaphragm that was correctly visualized by SS-R scintigraphy was located in the upper cervical region and had a diameter of 1.2 cm. The largest supradiaphragmatic lesion that was missed by SS-R scintigraphy had a diameter of 4.0 cm and was located in the axilla. The scintigraphic sensitivity for lymph nodes in the abdominal and inguinal regions varied from 30% to 54% (Figs. 2 and 3). Only 38% of the gastrointestinal lymphomas were visualized by SS-R scintigraphy. In the para-aortic and iliac regions, small lymph nodes of 1.5 cm in diameter were detected by SS-R scintigraphy. However, 1 mesenteric lymph node mass of 7.0 cm in diameter was entirely missed by SS-R scintigraphy. In 1 patient, lymphoma localization in the stomach was detected by SPECT only, whereas it had not been visualized on the planar images. In the other patients, SPECT provided no added value. In only 1 of the patients (9%) with bone marrow infiltration, the SS-R scan revealed marrow positivity. The sensitivity of SS-R scintigraphy for all lesions combined was 55%, varying from 62% for supradiaphragmatic lesions to 44% for lesions below the diaphragm. For nodal lesions, the sensitivity was 56%, and for extranodal sites, it was 45%. The estimated overall sensitivity of SS-R scintigraphy in the 42 patients with a positive scan was 60%. The specificity of SS-R scintigraphy was high (98%–100%). The intensity of uptake of 111In-pentetreotide in the malignant lesions was negative in 45%, grade 1 in 31%, grade 2 in 23%, and grade 3 in 1%. The maximum uptake of 111In-pentetreotide in the malignant lesions per patient was negative in 16%, grade 1 in 28%, grade 2 in 54%, and grade 3 in 2%. The mean uptake per patient was grade 1.07.

Visualization of submandibular lymph node in 42-y-old woman with stage IA NHL of low-grade malignancy by SS-R scintigraphy. Right lateral image of head and neck shows grade 2 pathologic uptake (arrow) within submandibular lesion. Normal uptake of radioactivity is seen in thyroid. On physical examination, lymph node of 3 cm in diameter was palpated.
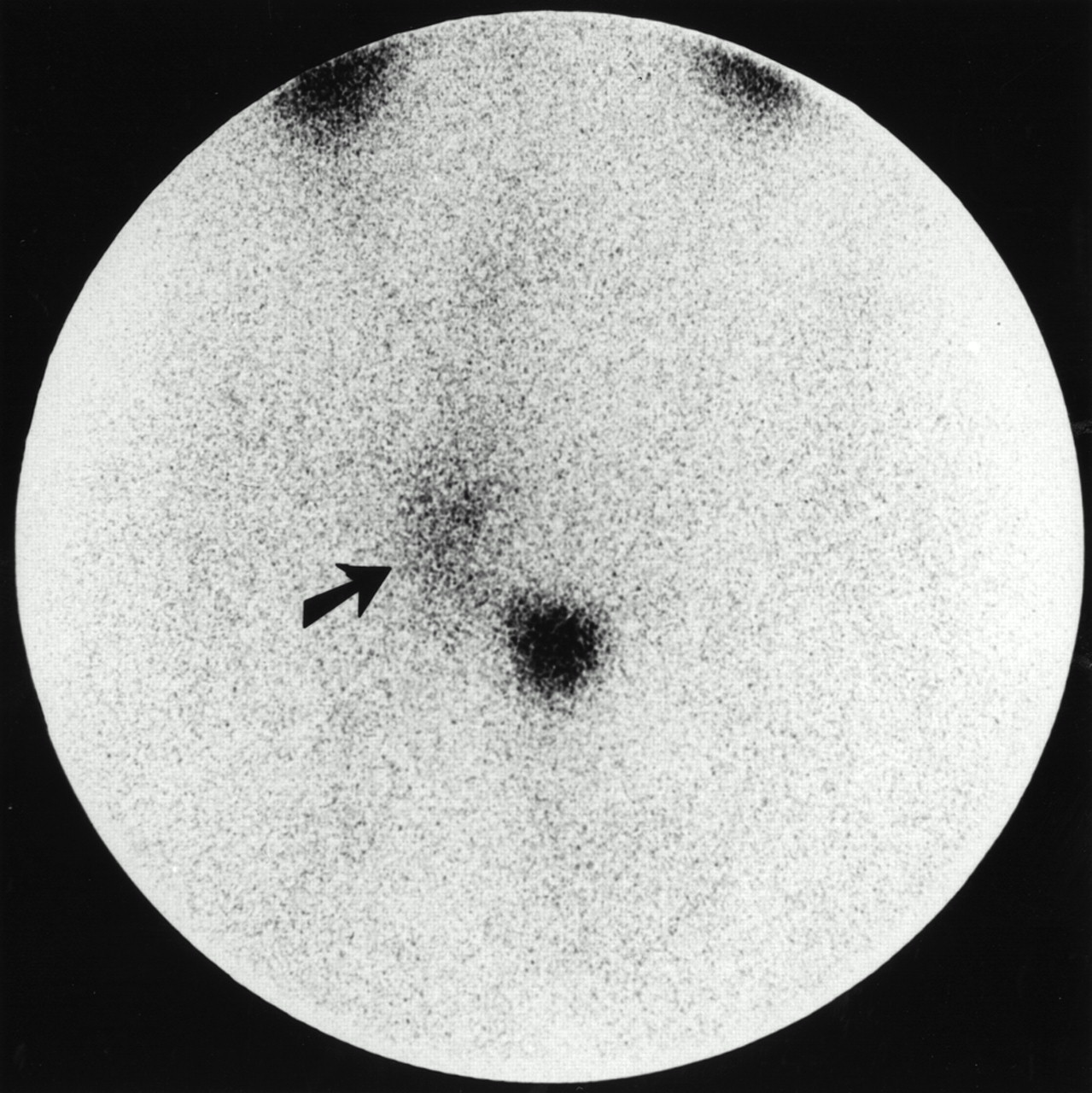
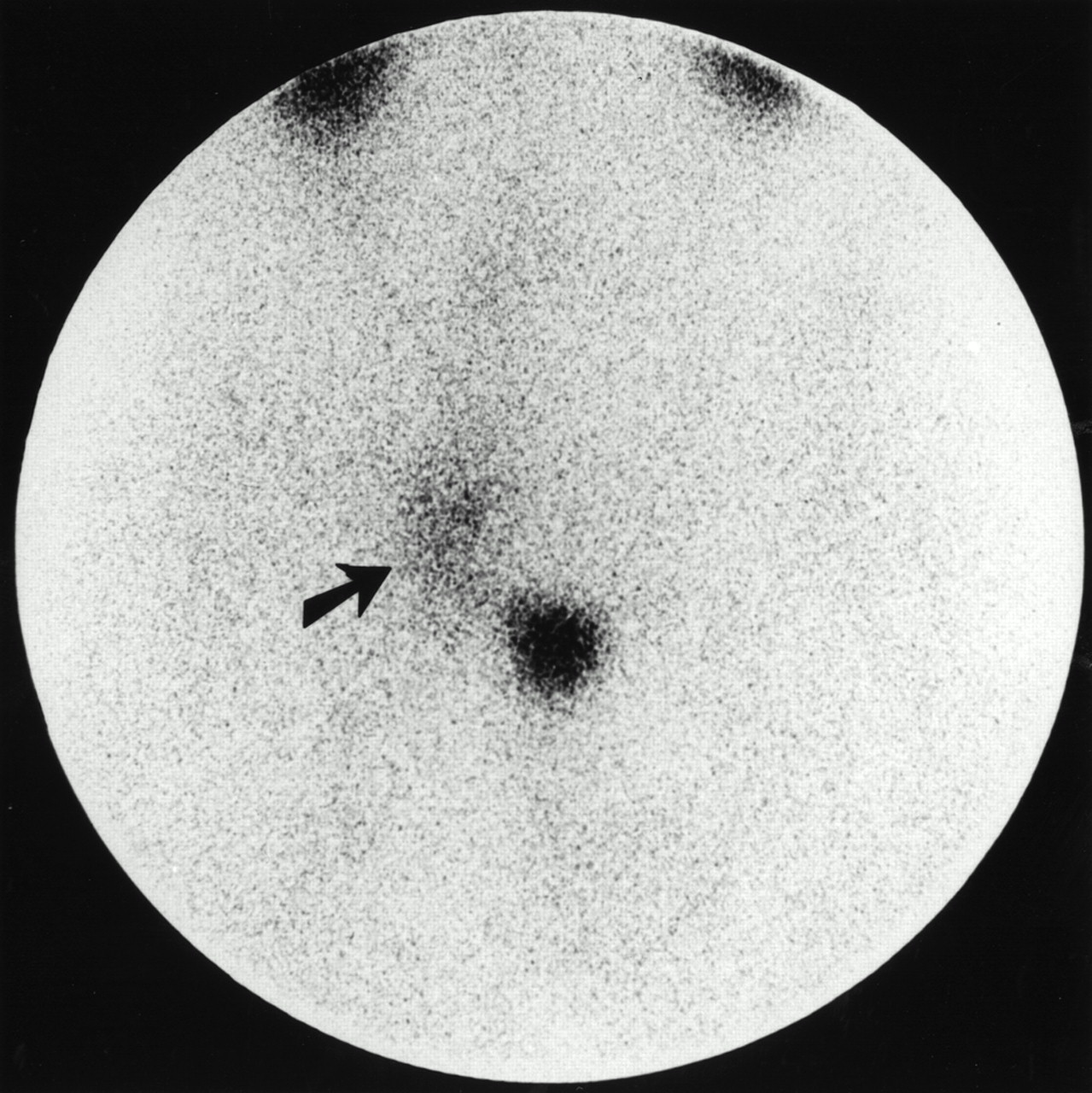
SS-R scintigraphy in 36-y-old man with low-grade NHL shows multiple enlarged lymph nodes of 2–3 cm in diameter in right inguinal and iliac regions. Pathologic lymph nodes are clearly seen (grade 2 uptake, arrow). Normal accumulation of radioactivity is seen in bladder and kidneys.
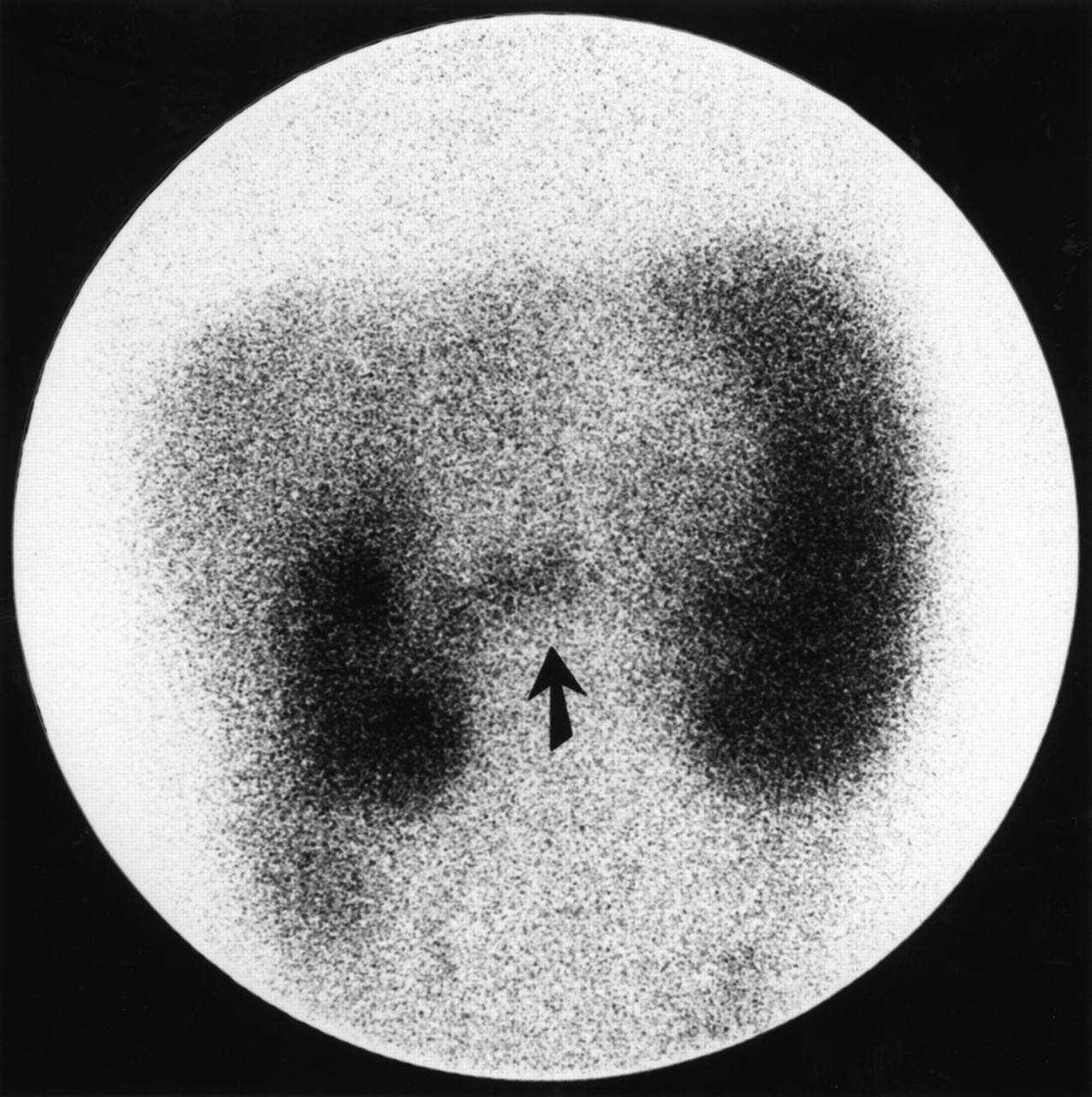
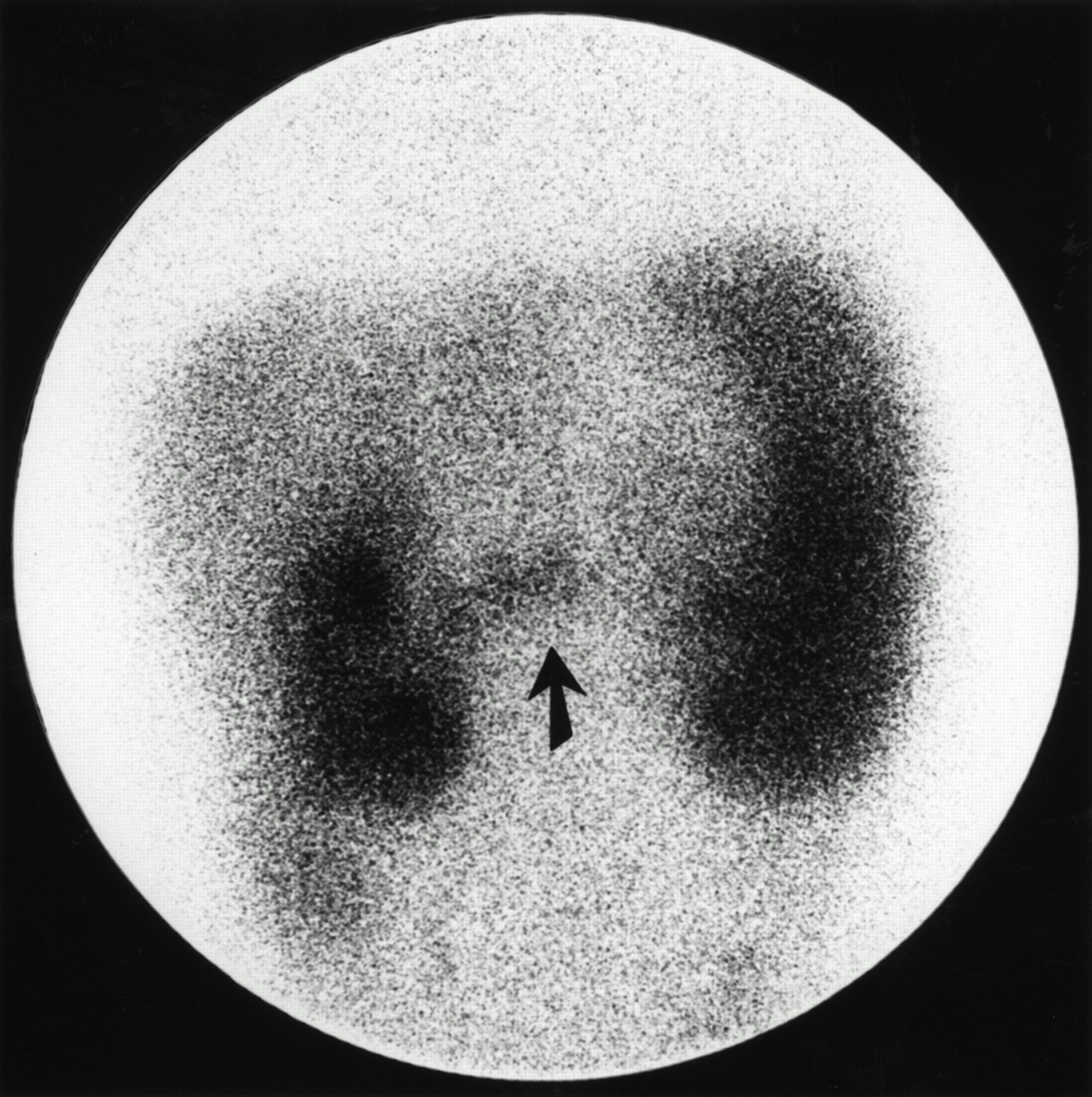
SS-R scintigraphy in 52-y-old woman with low-grade NHL shows pathologic uptake in abdominal region between kidneys (arrow). Normal uptake of radioactivity is seen in enlarged spleen. Normal uptake is also seen in liver and kidneys. CT scan of abdomen showed enlarged mesenteric lymph nodes.
Sensitivity of Various Diagnostic Approaches for Detection of Low-Grade NHL Lesions in Different Lymph Node Regions and Extranodal Sites
In six lesions, a false-positive result was obtained. In three patients, nonspecific accumulation of radioactivity was caused by recent surgery. Extreme dental caries caused aspecific uptake in the jaws of the fourth patient. The fifth patient suffered from autoimmune hemolytic anemia and showed a high uptake of radioactivity in an enlarged spleen. After a splenectomy, the histopathologic examination did not provide indications of splenic infiltration of NHL. In the last patient, a multinodular goiter caused a high aspecific accumulation of radioactivity in the thyroid. Cytologic and immunologic analyses of a thyroid puncture were negative for NHL.
Sensitivity of Several Imaging Techniques
Table 5 gives the estimated sensitivities of each imaging technique applied, expressed per distinct lymph node region and extranodal site. For the detection of peripheral lymph nodes, the sensitivity of SS-R scintigraphy appears inferior to physical examination and CT scanning. CT scanning is also superior for the visualization of nodal lesions in the thorax and abdominal region. CT scanning and SS-R scintigraphy each have a low sensitivity for gastrointestinal and orbita/eye localizations.
DISCUSSION
SS-R scintigraphy has been shown to be a useful imaging tool in a wide variety of SS-R–bearing tumors, including neuroendocrine cancers, brain tumors, breast cancer, and Hodgkin’s disease (4,21,22). Although previous in vitro studies indicated the presence of SS-Rs in lymph nodes with NHLs (5), only a few NHL studies have used SS-R scintigraphy. These studies were all based on a small number of patients, varying from 4 to 28 patients with NHL (6–13). Therefore, the clinical value of SS-R scintigraphy in the staging of NHLs has not been properly established.
We report on the results of a prospective study that investigated the role of SS-R scintigraphy in the initial work-up of 50 patients with untreated low-grade NHL. Findings in SS-R scans were positive in 84% of the patients. There were 9 patients with a MALT lymphoma in whom SS-R sensitivity was comparatively low. A high proportion (44%) of SS-R scan findings were negative in patients with a MALT NHL. In our study, 3 of 5 patients with primary gastric MALT lymphomas had positive findings. Raderer et al. (23) reported negative SS-R findings in all 15 investigated patients with primary gastric MALT lymphomas. These investigators suggested that the expression of mRNA for SS-R subtypes 3 and 4, but not for SS-R subtype 2, in the gastric samples of their patients might explain the negative scanning results. The low sensitivity of SS-R scintigraphy in MALT lymphomas is similar to that of other imaging modalities, such as CT and FDG PET (24–27).
In 20% of the patients, the new lesions revealed by SS-R scintigraphy resulted in an upgrading of the clinical stage. As a result, these findings would have affected the treatment plan in 10% of the patients. These patients were restaged from stage I to stage III or stage IV and therefore were no longer eligible for curative radiotherapy. This discordance between SS-R scintigraphy and other techniques was not confirmed by biopsy. Although histologic confirmation would have been desirable, this process was not feasible in practice. On the other hand, in a substantial proportion (38%) of patients, lesions disclosed by conventional staging procedures were missed by SS-R scintigraphy.
We estimated the lesion-related sensitivity at 55%. The sensitivity varied from 62% for supradiaphragmatic lesions to 44% for lesions below the diaphragm. SPECT of the upper part of the abdomen was of little value. In one patient, only SPECT disclosed an NHL lesion that was not apparent on the planar images. CT was superior to SS-R scintigraphy for the detection of nodal lesions and also for most extranodal sites. However, SS-R scintigraphy was superior to CT for gastrointestinal lesions, although both imaging modalities have a low sensitivity.
The patient- and lesion-related sensitivity of SS-R scintigraphy in this study is higher than that reported by other groups (8,10,12,13), who found lesion-related sensitivities varying from 29% to 35% in patients with low-grade NHL. The number and selection of patients may explain part of this difference in sensitivity. In other published studies, the number of patients investigated with low-grade NHL ranges from 3 to 12 (6–13). In the study reported here, 50 newly diagnosed patients were enrolled, and a relatively high proportion of these patients had stage I or stage II disease. Furthermore, differences in imaging protocol and dosage of 111In or pentetreotide may also play a role. The majority of the lesions showed a relatively small accumulation of radioactivity (i.e., grade 1 in 31% of lesions). Therefore, it is our opinion that the counting time should be long enough (at least 15 min) and the applied doses of the radionuclide should be sufficiently high (at least 200 MBq) to enhance the visibility of these lesions with relatively low uptake. Interestingly, Lipp et al. (13) were able to improve their previous reported results by doubling the doses of octreotide and 111In and using extended SPECT.
The reported low sensitivity for low-grade NHLs is quite different from that for Hodgkin’s disease. We, as well as other groups, have found a distinctly higher sensitivity (94%) in patients with Hodgkin’s disease (8,12,21,22,28). This result may be partly explained by the fact that ∼80% of the lesions in Hodgkin’s disease show a high uptake of radioactivity (grade 2 or grade 3) (29). We also found a higher sensitivity (71%) in patients with intermediate- and high-grade NHL (Lugtenburg, data not shown). In patients with low-grade NHL, the intensity of the uptake of radioactivity in the lesions is probably too low for the radiotherapeutic use of high doses of 111In-pentetreotide.
Six false-positive SS-R scintigraphy findings were obtained, and three of these are notable. In the first patient, inflammatory reactions caused by extreme dental caries resulted in aspecific uptake in the jaw. Clinically, this patient suffered from gingivitis and paradontitis. The second patient had autoimmune hemolytic anemia and splenomegaly for several years. A high uptake of radioactivity occurred in the spleen, which histologically was not infiltrated with NHL. The third patient had an enlarged thyroid caused by a multinodular goiter. Cytopathologic examination of the thyroid did not reveal NHL. False-positive uptake in thyroid diseases has been described previously (30). In the last three patients, radioactivity accumulated at sites of recent operations, a known pitfall (4). We agree with Gibril et al. (30), who state that by thoroughly understanding the circumstances that can result in false-positive localization and comparing the SS-R scintigraphy result with the clinical context, a correct diagnosis can be made in almost every case. We found a high specificity for SS-R scintigraphy (98%–100%).
The role of gallium scintigraphy in the staging of patients with NHL is still a subject of controversy. Available data in the literature indicate a low sensitivity of gallium scintigraphy in low-grade NHL. Even in studies using high-dose gallium and modern equipment, low sensitivities are reported, ranging from 56% to 79% per patient and 32% to 69% per lesion (31–33). Therefore, gallium scintigraphy currently has no standard place in disease staging of malignant lymphoma. Whole-body FDG PET has been shown to detect both nodal and extranodal sites of disease in patients with Hodgkin’s disease and NHL (34,35). Several studies have shown that FDG PET is at least comparable with other imaging modalities such as CT (36,37). Sensitivities of 86%–89% have been reported (38). However, limited data have been published concerning the value of PET in the initial staging of low-grade NHL (38,39).
A shortcoming of our study is that no gold standard was obtained. This is a major problem in tumor staging for tumors that are widespread and cannot be subject to complete histologic evaluation. Sensitivities and specificities are difficult to assess in these types of studies. We defined criteria for assessment of lesions as benign, malignant, or indeterminate as a second-best alternative. The assessment was based on the results of pathologic examination supplemented by the clinical course. Despite these shortcomings, we believe that the data are sufficiently solid to assess the value of SS-R scintigraphy in the initial staging of low-grade NHL.
CONCLUSION
Optimal staging of low-grade NHL is important for identifying those patients who present with truly localized disease and may be cured by radiotherapy. Although SS-R scintigraphy findings are positive in 84% of patients with low-grade NHL, our data indicate that SS-R scintigraphy is insufficiently sensitive. In most patients, not all of the lesions can be detected. This lack of sensitivity makes SS-R scintigraphy not generally useful in the initial staging of patients with low-grade NHL. However, its use may be considered in selected patients with stage I or II disease to identify more extended disease. This use, of course, must be weighed against the high costs and patient burden.
Acknowledgments
The authors thank Janneke J. Sluys-Dallinga and Petra Blom, research nurses, for their excellent data management. This study was supported by a grant from the Dutch National Health Care Council.
Footnotes
Received May 30, 2000; revision accepted Aug. 28, 2000.
For correspondence or reprints contact: Pieternella J. Lugtenburg, MD, Department of Hematology, University Hospital Rotterdam, Dr Molewaterplein 40, 3015 GD Rotterdam, The Netherlands.




{kind=link}
{kind=link}
{kind=link}