


Abstract
The double-well single-plastic scintillation counter (DW counter) has been developed to reduce the need for technical expertise in a plasma sample method after a single injection of radioactive marker. The DW counter serves the 2 functions of a standard well counter in well A and a dose calibrator in well B. The aim of this study was to assess the clinical feasibility of the counter for the estimation of glomerular filtration rate (GFR) with 99mTc-diethylenetriaminepentaacetic acid (DTPA). Methods: The study was performed on 25 patients with varying degrees of renal dysfunction. The GFR was estimated by a single-sample method after a single injection of 99mTc-DTPA. Total injected dose and plasma radioactivity were calculated following 2 methods: standard dilution with a single well (dilution method) and no dilution with 2 wells (direct method). Results: The GFR directly estimated by the DW counter correlated excellently with the GFR estimated by the dilution method (r = 0.998; root mean square error = 2.01 mL/min/1.73 m2). The 95% of differences (−0.3124 to 0.0423 percentage injected dose [%ID]/L/1.73 m2) in plasma concentration between the 2 comparative methods was <2 SDs. The direct method tended to give slightly higher readings of plasma concentration than did the dilution method (95% confidence interval = −0.0364 to −0.0904 %ID/L/1.73 m2). Conclusion: The DW counter can circumvent laborious dilution techniques and expertise required for quantifying the GFR in a single-sample method after a single injection of 99mTc-DTPA in clinical practice. It is proposed as an alternative to the standard dilution method.
- plastic scintillation counter
- plasma sample method
- glomerular filtration rate
- 99mTc-diethylenetriaminepentaacetic acid
The glomerular filtration rate (GFR) is considered to be a representative parameter for evaluating the functional state of the kidney (1,2). Simple and accurate determination of the GFR is still a challenge in clinical practice (3). A plasma sample method, after a single injection of radioactive marker, has proven to be more accurate than the other methods for quantification of renal function (4–7). However, this method requires laborious and cumbersome procedures involved in diluting the injected radioactive marker. To simplify the procedures, we have developed a double-well single-plastic scintillation counter (DW counter) that has a very wide dynamic range (approximately 106) for radioactivity measurement.
In this article, the GFR determined by the DW counter without dilution of the injected dose was compared with that measured in a single-plasma method after a single injection of 99mTc-diethylenetriaminepentaacetic acid (DTPA) with standard dilution.
Materials and Methods
DW Counter
The DW counter consists of 2 wells and a single-plastic scintillator (cylindrical; external diameter, 60 mm; internal diameter, 40 mm; width, 10 mm; height, 100 mm). The single scintillator is common to the 2 wells (Fig. 1). Well A is arranged to simulate a regular single-well scintillation counter for plasma samples with low radioactivity. The capacity of the measured volume in a tube is limited to a maximum of 4 mL. In contrast, well B was designed specifically for counting radioactivity in a straight-needle injection syringe before the injection and an injected syringe with an attached 3-way cock and straight needle after the injection. The 2 wells are geometrically separated with a lead collimator for regulating sensitivity to radioactivity between them. The instrument has 2 photomultipliers with a coincidence circuit and cannot discriminate γ-ray energy emitted from radionuclides.

Illustration of mechanical constituents of DW counter.
In the prototype that we used in this study, the sensitivity for 140 keV of 99mTc in wells A and B was estimated to be 6.721% and 0.006882%, respectively. Thus, the difference in relative sensitivity between the 2 wells is approximately 980 times. In addition, the sensitivity for the empty syringe with 3-way cock and needle was calculated to be 0.00628%. The difference in sensitivity between the pre- and postinjection syringes was considered to rise from geometric problems.
The measured counting rates (count per s [cps]) in the 2 wells were converted to the standard radioactivity unit (becquerel) by correction of the different counter sensitivities of each well. The conversion factor of cps to standard becquerels in each well was 14.8787 for well A, 14,534.88 for the preinjection syringe, and 15,901.30 for the postinjection syringe with 3-way cock. These conversion factors remained constant for 99mTc, used injection volume, and measured sample volume.
The relationship between the converted and standard radioactivity was linear (range, 103–109 Bq; r = 0.99999). The error of the predicted radioactive value to the standard radioactivity was <1% in our preliminary test. No geometric problem in sensitivity was observed for a solution volume of 1–3 mL in a tube for well A and of 1–5 mL in a 5-mL injection syringe for well B.
Clinical Study
The study was performed on 25 patients (11 males, 14 females; age range, 12–89 y; mean age, 59.2 ± 19 y; mean height, 157.7 ± 9.7 cm; mean weight, 54.4 ± 12.2 kg; mean body surface area, 1.54 ± 0.20 m2) with varying degrees of renal dysfunction. Mean serum level of creatinine was 1.04 ± 0.49 mg/dL (range, 0.47–2.1 mg/dL); mean level of blood urea nitrogen was 16.8 ± 6.8 mg/dL (range, 6.2–31.2 mg/dL).
DTPA was labeled with 99mTc in-house using a commercially available freeze-dried kit (Daiichi Radioisotope Co., Tokyo, Japan). Labeling yield of the kit was confirmed to be >95%. A 2.5-mL plastic injection syringe (Terumo, Tokyo, Japan) containing 37–185 MBq (1–5 mCi) in 2 mL was prepared for each patient. The radioactivity (Cpre) in the preinjection straight-needle syringe was counted by the DW counter in the dedicated well (well B). Just before intravenous injection, the straight needle of the injection syringe was replaced by a 3-way cock with butterfly needle that was filled with normal saline solution. The straight needle was kept for subsequent counting after the injection. 99mTc-DTPA was administered intravenously as a bolus injection followed by a rinse with 20 mL normal saline. The renal scintigraphy entailed a standard method for 20 min. In the injected syringe (Cpost) with 3-way cock and straight needle attached, radioactivity was again counted by the DW counter in the same way as it was in the preinjection dose. No significant interstitial leakage was determined by gamma camera imaging of the injection site after scintigraphy.
A blood sample was taken at 180 min after the injection, except in 2 patients (1 was taken at 134 min and the other was taken at 220 min), and plasma radioactivity per milliliter was counted by the same DW counter in the well dedicated for a sample tube (well A; maximum volume, 4.0 mL; Shionogi, Tokyo, Japan). Percentage plasma concentration per injected dose and apparent volume of the distribution were determined by the following 2 ways.
Standard Dilution Method
A 0.1-mL aliquot of the injected stock solution was diluted with 500 mL normal saline and the radioactivity (cps) in 1 mL diluted solution was counted by the DW counter in well A. The 1-mL plasma sample was also counted by the DW counter in well A. The measured net counting rate (cps) was used for calculation of total injected dose (IDdil), which was determined by correction of the dilution rate. The plasma concentration (Pdil) and apparent volume of distribution (Vdil) were calculated by the following equations: IDdil (cps) = radioactivity in diluted solution (cps/mL) × ratio of injected volume to volume of stock solution included in aliquot (2 mL/0.1 mL) × 500; Pdil (percentage injected dose [%ID]/L) = (counting rate in plasma [cps/mL]) × 1,000)/IDdil (cps) × 100; Vdil (L) = IDdil (hertz)/(counting rate in plasma [cps/mL] × 1,000).
Direct Method Without Dilution of Injected Dose
The measured net counting rate (cps) with background count subtraction of the pre- and postinjection syringe was converted to standard radioactivity (becquerels) by multiplying by the conversion factors. The radioactivity of the postinjection syringe was corrected with the radioactive decay constant of 99mTc (half-life, 6.01 h) from the initial measurement of the preinjection syringe. The measured net counting rate (cps) with background count subtraction of the plasma in well A was also converted to standard radioactivity (becqerels) by multiplying by the conversion factor for well A. It was also corrected with the decay constant from the initial measurement of the preinjection dose (Cdir, becquerels). The correction of physical decay was calculated automatically by the computer in the instrument. Plasma concentration (Pdir) and apparent volume of distribution (Vdir) were calculated directly from converted radioactivity (becquerels) without dilution procedures as follows: IDdir = Cpre (Bq) − Cpost (Bq); Pdir (%ID/L) = (Cdir [Bq/mL] × 1,000)/IDdir (Bq) × 100; Vdir (L) = IDdir (Bq)/(Cdir [Bq/mL] × 1,000).
The GFR for 23 adults was determined by the formula of Christensen and Groth, which was rewritten by Watson (9). The GFR for 2 children (ages, 12 and 16 y) was determined by the formula of Ham and Piepsz (10). The GFR and plasma concentration were normalized for a body surface area of 1.73 m2 (11).
Statistical Analysis
The linear regression and correlation analysis was used to evaluate the relationship between the dilution and direct methods. Difference in GFR and plasma concentration (%ID/L) between the dilution and direct methods were estimated and 95% of difference and 95% confidence interval were assessed (12).
Results
The directly determined GFR correlated excellently with that determined by the dilution method in the single-sample approach (r = 0.998; P < 0.001; root mean square error [RSME] = 2.01 mL/min/1.73 m2) (Fig. 2). The 95% of difference (limits of agreement) of GFR between the dilution and direct estimates was −0.009 to 7.881 mL/min/1.73 m2 (Table 1). The 95% confidence interval of difference in GFR between the 2 comparative methods was −0.623 to 2.198 mL/min/1.73 m2. The dilution method tended to give slightly higher readings of GFR than did the direct method (Table 1).

Scatter plot of GFR estimated by dilution method vs. GFR estimated by direct method (• = adult; × = children).
Results of Differences in GFR and Plasma Concentration Between Dilution and Direct Methods
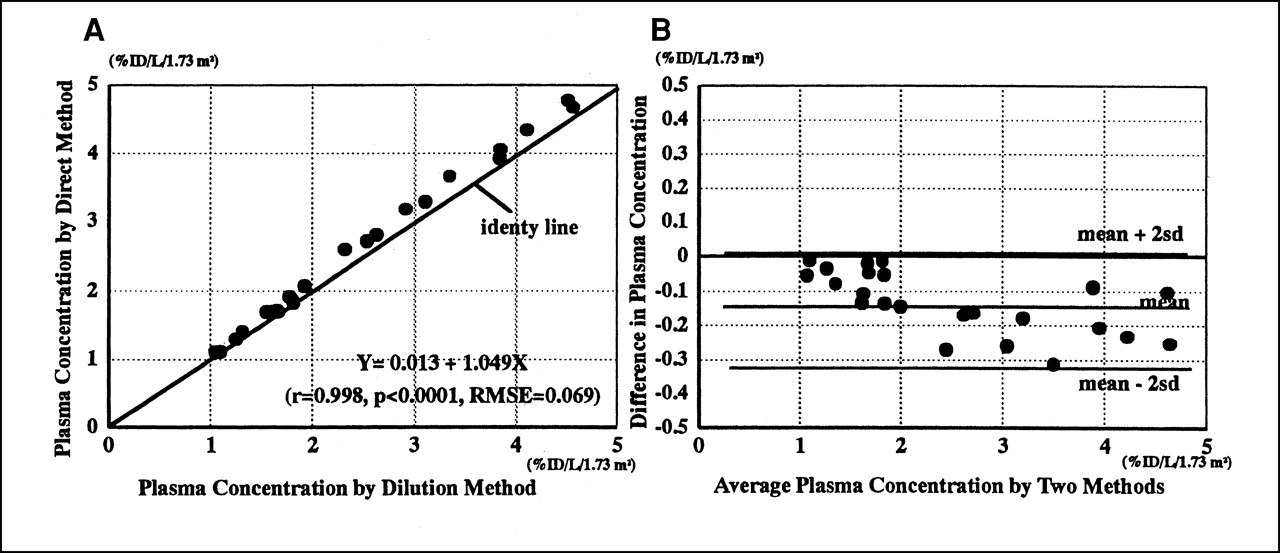
The plasma concentration determined by the direct method also correlated excellently with that determined by the dilution method (r = 0.998; P < 0.001; RMSE = 0.069 mL/min/1.73 m2) (Fig. 3A). The 95% of difference of plasma concentration between the dilution and direct estimates was −0.3124 to 0.0423 %ID/L/1.73 m2 (Table 1). The 95% confidence interval of difference in GFR between the 2 comparative methods was −0.0364 to −0.0904 %ID/L/1.73 m2. The direct method tended to give slightly higher readings of plasma concentration than did the dilution method, and the difference in plasma concentration seemed to be related to the level of plasma concentration (Fig. 3B). But the 95% of differences in plasma concentration between the 2 comparative methods is <2 SDs. The results indicate that the direct method can be used in place of the dilution method for clinical purposes.
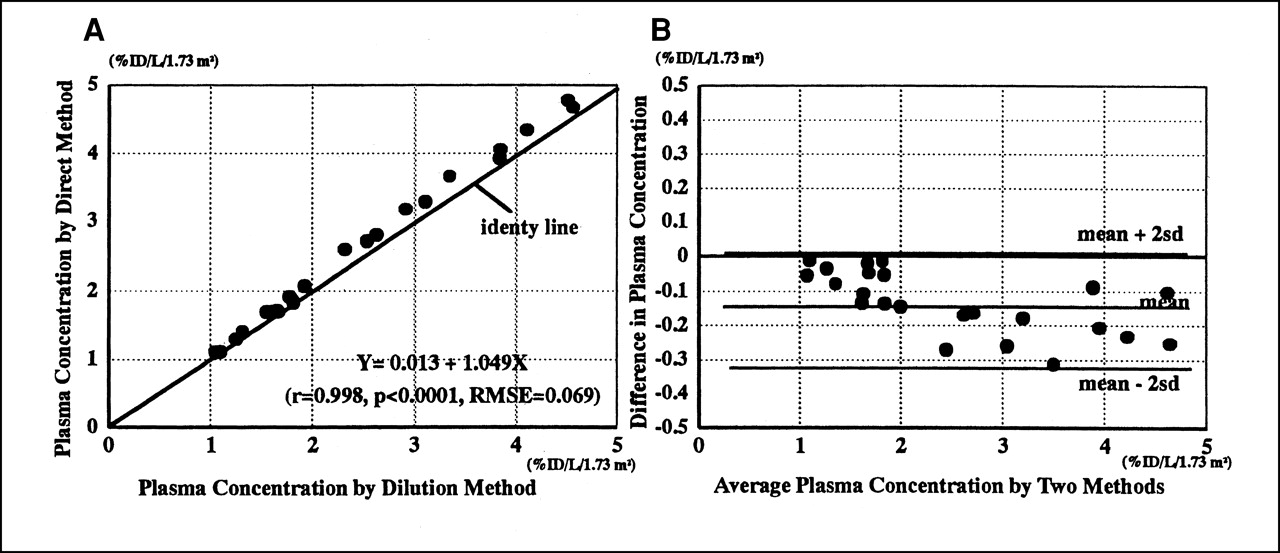
Relationship of plasma concentration calculated by dilution and direct methods. (A) Scatter plot of plasma concentration determined by direct method vs. that determined by dilution method. (B) Scatter plot of differences in plasma concentration (Pdil − Pdir) vs. mean plasma concentration by 2 methods.
Discussion
The single-sample method after a single injection of radioactive marker has been shown to be accurate (5–7). The basic concept of a plasma sample method for determining renal function after a single injection of radioactive marker was established 20–30 y ago (13–17). These algorithms have been widely adopted to quantify the GFR with even a nonradioactive contrast marker such as iohexol (18–20). 51Cr-ethylenediaminetetraacetic acid has been used as a radioactive marker in European countries (5,6); 25I-iothalamate has been used in the United States (1,2,4,21). These radioactive markers cannot be used in scintigraphy. 99mTc-DTPA is the most popular radioactive marker anywhere for renal scintigraphy as well as for evaluation of the glomerular function (22–24). However, a plasma sample method for calculating GFR with 99mTc-DTPA at the time of scintigraphy has not been common in clinical practice, because the preparation of a diluted standard solution is indispensable for calculation of total administered dose. The dilution procedures are technically cumbersome and laborious. As a matter of practice, it is not easy to prepare the standard solution for scintigraphy on each patient studied. Therefore, a plasma sample method has been performed as a test designed specifically for determining renal function using a radioactive marker found in routine practice and clinical research study.
The DW counter was developed to simplify the laborious procedures involved in a sample method in routine practice. Although the study on the physical properties of the instrument was limited to only 1 radionuclide of 99mTc, it was confirmed that it possessed a good linearity between 103 and 109 Bq of radioactivity in preliminary experimental studies. Measuring radioactivity after converting cps to becquerels makes it possible to calculate plasma concentration without the dilution procedure. The instrument used in this study was a prototype that had been developed with coworkers of Aloka Co., Ltd. (Tokyo, Japan). After this study, the prototype became a commercial product with some mechanical improvements in the sensitivity of each well and in its operation. The precise data on its structural and physical properties will be reported elsewhere.
In this study, it was shown that direct GFR determination by the DW counter correlated excellently with the standard-dilution GFR determination. The precision of estimated GFR depends on the method that is used to determine it (5–7). However, the relationship of plasma concentration between the dilution and direct methods is not affected by age, sampling time, or GFR calculation formula. The directly determined plasma concentration also correlated excellently with that of the dilution method. Nonetheless, the direct method tended to give slightly higher readings of plasma concentration than did the dilution method. Furthermore, it appeared that the difference in the plasma concentration tended to increase in higher plasma concentrations. In the dilution study, the remaining radioactivity was not subtracted exactly for calculation of the injected dose. High plasma concentration corresponds to small apparent volume of distribution, which indicates slow plasma clearance and low GFR (7,8). In good renal function, it is thought that the difference in total injected dose between the dilution and the direct methods does not give the significant difference in plasma concentration, because of the relatively large distribution volume of the injected tracer. In contrast, the difference in plasma concentration seems to be apparent in decreased renal function state, because the distribution volume of the injected tracer is relatively small. Therefore, the bias may be explained by the residual radioactivity in the postinjection set. The exact correction of the residual radioactivity is considered to be important in the decreased renal function rather than the good renal function.
The dilution technique used in this study was simpler than was the technique recommended in the consensus report (7). In the context, the dilution method in this paper may not be approved as the standard. The precision of the direct method using the DW counter, which includes the dilution technique and mechanical stability, also needs further study. Nonetheless, it is emphasized that the DW counter can streamline the cumbersome and laborious procedures that are required for determining GFR in the standard dilution method.
Conclusion
This study reports on the clinical feasibility of the new measurement of GFR by the newly developed plastic scintillation counter in a single-sample method with 99mTc-DTPA. It is concluded that GFR can be determined more easily and more simply by a combination of the DW counter and a plasma sample method after a single injection of 99mTc-DTPA. The direct method using the DW counter can be used in place of the standard dilution method for clinical purposes.
Acknowledgments
The author thanks all collaborators who have been concerned with the development of the prototype DW counter, particularly Akinori Iwamoto, Keisuke Oshikiri, Jun Hachisuka, Shohei Matsubara, and Toshinori Oshima of Aloka Co., Ltd., for their technical support in handling the instrument. I also appreciate technologists Kouji Ihara, Tokihiro Oka, and Kimikazu Sasaki, of the nuclear medicine section of the JR Sapporo General Hospital, for their technical assistance in this clinical study.
Footnotes
Received Nov. 27, 2000; revision accepted Jun. 13, 2001.
For reprints or correspondence contact: Kazuo Itoh, MD, Department of Radiology, JR Sapporo General Hospital, Higashi-1, Kita-3, Chuo-ku, Sapporo, 060–0033, Japan.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.