


Abstract
Although mammography is well established as a first-line tool for breast cancer screening and detection, efforts to develop complementary procedures continue. Observation of 99mTc-sestamibi tumor uptake provided the impetus for its evaluation as an adjunctive technique. This trial's objectives were to determine in a multicenter trial the diagnostic accuracy of 99mTc-sestamibi in women with suspected breast cancer and to investigate factors influencing diagnostic accuracy. Methods: Our multicenter trial enrolled 673 women (387 with nonpalpable abnormalities; 286 with palpable abnormalities) scheduled for excisional biopsy or mastectomy. Blinded and unblinded interpretations of scintigraphic images were compared with core laboratory established histopathologic diagnoses to define the diagnostic accuracy of 99mTc-sestamibi breast imaging. Results: Blinded readers' diagnostic accuracy was 78%–81%. Inter-reader agreement was excellent, ranging from 95% to 100% (κ = 0.82–0.99). Overall institutional sensitivity and specificity for 99mTc-sestamibi breast imaging were 75.4% and 82.7%, respectively. In this population with a 40.1% disease prevalence, the positive predictive value was 74.5% and the negative predictive value was 83.4%. The negative predictive value was 94% in patients with a 40% or lower mammographic likelihood of breast cancer. Sensitivity was higher for palpable abnormalities; specificity was higher for nonpalpable abnormalities. Sensitivity was decreased for tumors <1 cm in largest dimension but appeared not to be affected by patient's age. Conclusion: As an adjunct to current procedures, 99mTc-sestamibi breast imaging may contribute to patient management decisions in selected populations, including women with dense breasts, mammographically indeterminate lesions >1 cm, and palpable abnormalities.
Breast cancer is the most common malignancy of American women after skin cancer and the leading cause of nonpreventable cancer death (1). Breast self examination, clinical breast examination, and screening mammography are the recommended procedures for early breast cancer detection. Screening mammography has been shown to reduce breast cancer mortality in women 40–69 y old (2,3), although the benefit reported in women 40–49 y old (3) is somewhat less than that reported in the older population (2). Still greater reduction in mortality is sought, and there is a clear need to extend the full benefit to women of all ages. Thus, intensive efforts in early diagnosis have focused on improvements in patient outcomes by developing procedures that improve the sensitivity and positive predictive value of the procedures used to evaluate patients with suspected breast cancer.
99mTc-sestamibi is a radiopharmaceutical that was originally developed as a myocardial perfusion imaging agent. However, results from in vitro (4–6) and in vivo (7–10) preclinical studies have suggested that it may have potential as a tumor imaging agent. Several investigators have reported results of breast imaging with 99mTc-sestamibi that have generally supported this potential (11–20). The objectives of our study were to extend these earlier results by determining in a multicenter trial the diagnostic accuracy of 99mTc-sestamibi in women with suspected breast cancer and to investigate factors influencing diagnostic accuracy.
MATERIALS AND METHODS
Subjects
Six hundred seventy-three women were enrolled at 42 institutions in the United States and Canada. Enrollment occurred from April 1994 through May 1995. For enrollment in the trial, the subjects were to be already scheduled for an excisional biopsy (or mastectomy) on the basis of the presence of a nonpalpable mammographically detected breast abnormality or a palpable breast abnormality; 387 women with nonpalpable abnormalities and 286 women with palpable abnormalities were enrolled. As in clinical practice, women with palpable abnormalities did not necessarily have mammographic abnormalities. Because preliminary pilot work had suggested that trauma could lead to false-positive 99mTc-sestamibi images, subjects could not have undergone fine-needle aspiration or core needle biopsy within 1 wk before the 99mTc-sestamibi imaging study. To be evaluable, subjects had to have an abnormality identified by palpation or mammography (or both), 99mTc-sestamibi scintigraphy, and excisional biopsy (or mastectomy) in that sequence; 563 women met evaluability criteria (315 with nonpalpable abnormalities and 248 with palpable abnormalities). The investigational protocol was approved by the institutional review board at each participating center, and each subject provided written informed consent.
Mammography
Mammography was performed using standard craniocaudal and mediolateral oblique views with additional views obtained as clinically indicated. Each participating site in the United States was accredited by the American College of Radiology Mammography Accreditation Program. The Canadian site had full accreditation in medical imaging by the Diagnostic Accreditation Program in British Columbia. Additionally, phantom images and representative mammograms from each site were evaluated by the mammography core center. Deficiencies noted by the core center were corrected before enrolling patients. Collection of mammography results was based on the American College of Radiology Breast Imaging Reporting and Data System (21). Although it is not a common practice, for this trial the mammographer at each site assigned a mammographic probability of malignancy to each lesion (palpable or nonpalpable) that was to be biopsied. The parenchymal patterns “heterogeneously dense” and “extremely dense” were defined to represent dense breasts, whereas “almost entirely fat” and “numerous vague densities” were defined to represent fatty breasts.
Scintigraphy
Planar imaging with high-resolution collimation was performed using the gamma cameras available in the investigators' departments. Subjects received a 740- to 1110-MBq (20–30 mCi) bolus intravenous injection of 99mTc-sestamibi in the arm contralateral to the suspicious breast abnormality; subjects with bilateral abnormalities were injected in a dorsalis pedis vein. Five minutes after injection, a 10-min lateral view of the breast scheduled for biopsy was obtained with the subject positioned prone on an imaging table overlay (Bodfish Research and Design, Inc., Bodfish, CA) so that the breast being imaged was pendent (11). The subject was then repositioned to obtain a lateral view of the contralateral breast followed by a supine anterior view. Lateral views were repeated 1 h after injection.
Scintigraphic images were read at the sites by the investigators (institutional results). Because most investigators in the trial had minimal experience interpreting 99mTc-sestamibi breast images, a set of 18 images, scored on a 5-point scale (0 = normal; 1 = equivocal; 2 = focal uptake, low intensity; 3 = focal uptake, medium intensity; and 4 = focal uptake, high intensity) but without histopathologic correlation, was provided for image scoring training.
For the calculation of diagnostic statistics, scores of 2–4 were considered positive, scores of 0 were considered negative, and scores of 1 were considered uninterpretable and were not analyzed. Overall, institutional readers scored 6.4% of biopsied scintigraphic abnormalities as 1. In addition to the image interpretation by the investigators, two groups of three independent nuclear medicine physicians who had no knowledge of the subjects' clinical history, institutional scintigraphic results, or other test results (blinded readers) interpreted the images. Thus, the blinded readers were not told whether they were reading images from subjects with nonpalpable abnormalities or with palpable abnormalities. One group of blinded readers read the images from subjects with nonpalpable abnormalities, and the other group read the images from subjects with palpable abnormalities. For the blinded reading, digital data were converted to a common image display format, and images were randomized and read from the computer display.
Lesion Correlation
Because breast tissue is highly mobile and because mammographic and scintigraphic imaging used different views and techniques (compressed versus noncompressed), it was necessary to review the scintigraphic findings to establish lesion correlation. Thus, a radiologist not associated with the trial reviewed the scintigraphic images and mammograms in conjunction with the blinded readers' image interpretations and the investigational sites' mammographic data reporting to determine whether the scintigraphic abnormality corresponded to the same tissue as the mammographic finding. Similarly, a breast surgeon not associated with the trial reviewed the scintigraphic images, blinded readers' image interpretation, and the investigational sites' physical finding reporting to determine whether the scintigraphic abnormality corresponded to the same tissue as the palpable abnormality. All calculations of diagnostic statistics were based on histopathologically determined malignancy or benignity of biopsied tissue. Because a scintigraphic abnormality that did not correspond to a mammographic abnormality or physical finding was not biopsied, such abnormalities could not be assigned as malignant or benign and thus were excluded from analysis. Characterization of these scintigraphic abnormalities as either false-positive or true-positive findings is the objective of a follow-up study.
Biopsy and Histopathology
Biopsy decisions were based on clinical presentation independent of scintigraphic findings. After needle localization, excision of nonpalpable mammographically detected abnormalities was confirmed by specimen radiography. The institutional histopathologists determined tumor size from excised tissue specimens. Histopathologic diagnosis by the core laboratory was based solely on excisional biopsy or mastectomy specimens. Evaluation was performed on original slides or recuts of the tissue blocks if originals were unavailable. Ductal carcinoma in situ (DCIS), infiltrating ductal carcinoma, and infiltrating lobular carcinoma were classified as malignant. Cases of lobular carcinoma in situ were classified as nonmalignant.
Statistical Analysis
The primary analysis in evaluating 99mTc-sestamibi for detecting the presence of malignancy compared the blinded reader's image interpretation with the histopathologic diagnosis. Sensitivity, specificity, positive and negative predictive values, and accuracy were calculated. Comparisons between two groups were performed using a two-sample test of proportions. Group differences were considered significant at P < 0.05. Inter-reader agreement was assessed using the κ statistic. κ < 0.40 indicates poor agreement, whereas κ = 0.40–0.75 and κ > 0.75 indicate fair-to-good and strong agreement, respectively (22).
To further investigate factors influencing diagnostic results, a multivariable regression analysis was performed. Variables entered into the model included patient age dichotomized as ≤50 or >50 y, mammographers' likelihood of malignancy, mammographic finding categorized as mass or calcification, lesion palpability, and tumor size dichotomized as <1 or ≥1 cm.
RESULTS
The prevalence of malignancy was 40.1% overall: 48.4% for palpable abnormalities and 32.9% for nonpalpable abnormalities. The mean age of the evaluable subjects was 52.2 y (range, 23–85 y); 31.6% were premenopausal and 49.5% had dense breasts. Women with nonpalpable abnormalities were older, less likely to be premenopausal, and less likely to have dense breasts than were women with palpable abnormalities (Table 1).
Subject Demographics
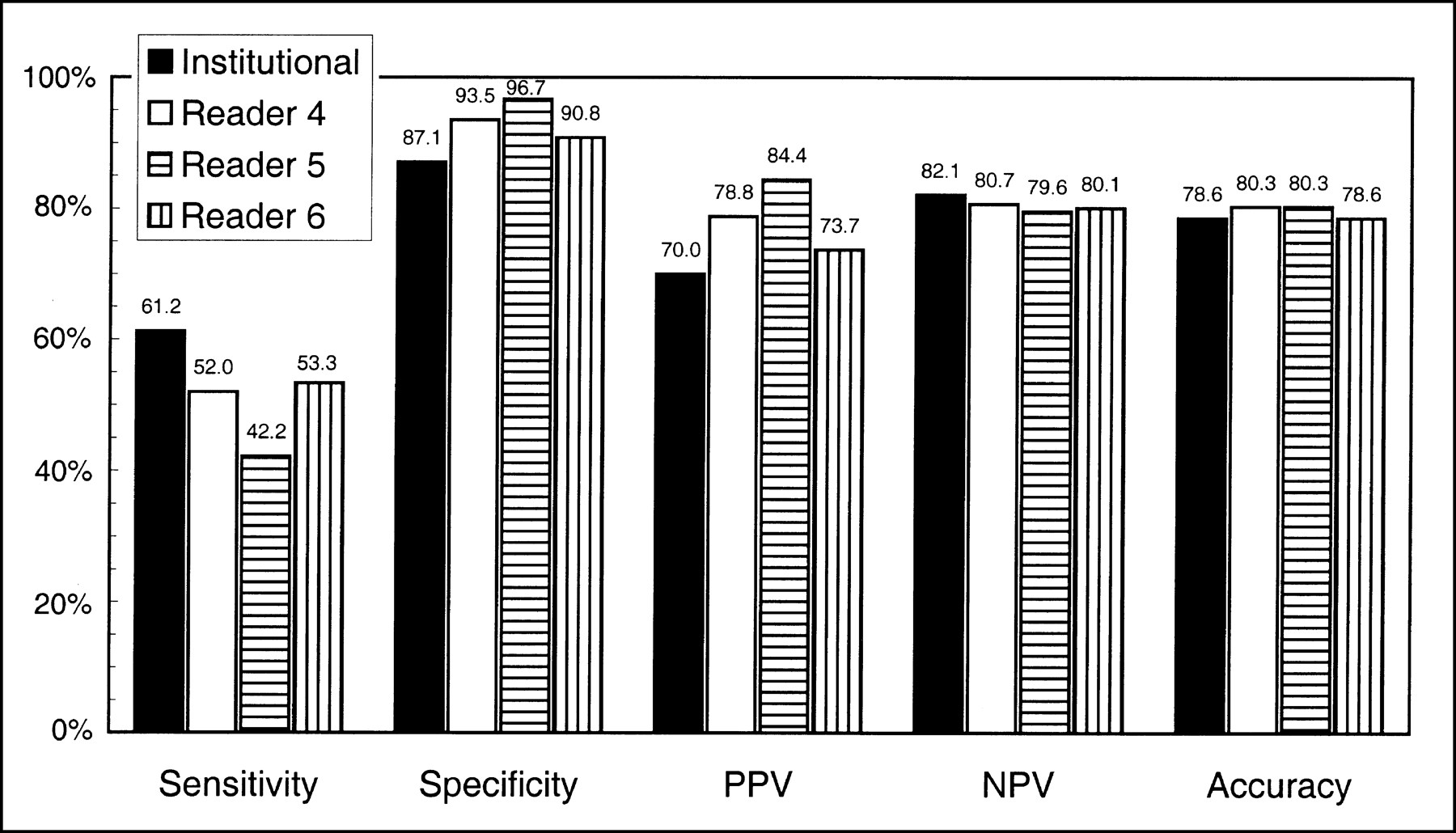
The overall institutional sensitivity and specificity for 99mTc-sestamibi breast imaging were 75.4% and 82.7%, respectively. Sensitivity was higher and specificity was lower for palpable abnormalities compared with nonpalpable abnormalities (P < 0.05). Specificity was higher and sensitivity was lower for the blinded readers compared with the institutional results. These differences in sensitivity and specificity tended to be balanced, because the diagnostic accuracy for the blinded readers and institutional readers for palpable and nonpalpable abnormalities were similar, ranging from 78% to 81% (Figs. 1 and 2).
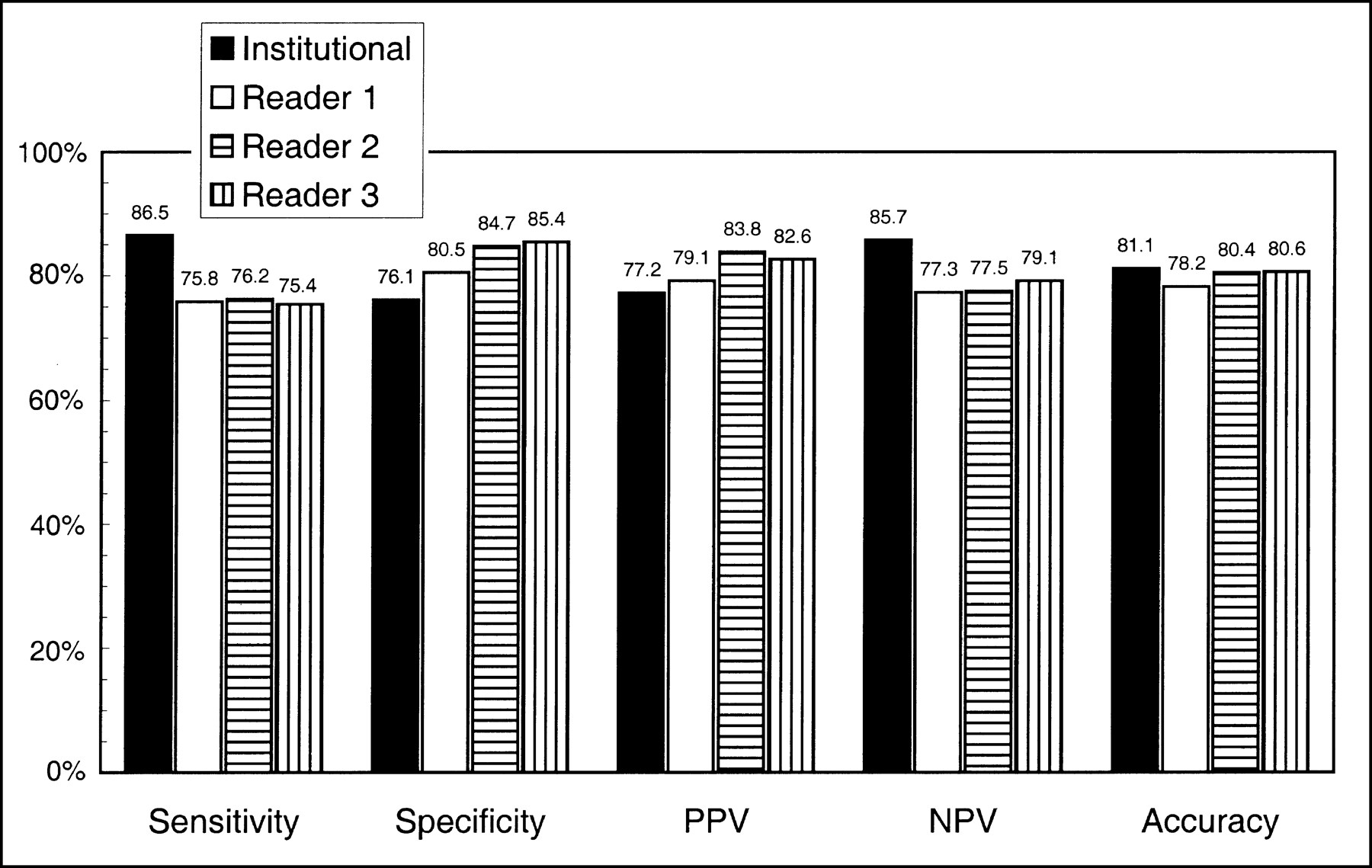
Diagnostic statistics for 99mTc-sestamibi breast imaging in patients with palpable abnormalities. PPV = positive predictive value; NPV = negative predictive value.

Diagnostic statistics for 99mTc-sestamibi breast imaging in patients with nonpalpable abnormalities. PPV = positive predictive value; NPV = negative predictive value.
Age
The group of women who were ≤50 y old with nonpalpable abnormalities had a disease prevalence of 21.2%, whereas the group of younger women with palpable abnormalities had a prevalence of malignancy of 34.0%. The overall diagnostic sensitivity for 99mTc-sestamibi breast imaging was comparable in women ≤50 y old and women ≥50 y old (75.3% and 75.5%, respectively; P = not significant). When the results were considered separately for women with palpable abnormalities and for women with nonpalpable abnormalities, there was a trend for higher sensitivity in older women, although these differences were not statistically significant (Table 2). Imaging specificity was higher in the older population, although this difference was not statistically significant for institutional results for women with palpable abnormalities.
Diagnostic Performance of 99mTc-Sestamibi Breast Imaging as Function of Patients' Age
Tumor Size
Diagnostic sensitivity of any imaging procedure is affected by limitations inherent in the procedure (e.g., scintillation camera resolution). Consequently, we assessed sensitivity for the detection of nonpalpable abnormalities as a function of the largest tumor dimension measured on the excised specimen. Institutional sensitivity was significantly higher for tumors ≥1 cm than for tumors <1 cm (74.2% and 48.2%, respectively; P < 0.05). Similar results were observed for the blinded readers.
Likelihood of Malignancy
The prevalence of histopathologically determined disease was well tracked by the mammographers' estimate of a lesion's likelihood of being malignant (r = 0.98; P < 0.005). The institutional sensitivity and specificity of 99mTc-sestamibi imaging were similar in women with all likelihoods of disease, 64%–82% and 73%–87%, respectively (Table 3). Consequently, in women with ≤40% mammographic likelihood of malignancy, the negative predictive value for 99mTc-sestamibi imaging was 94%.
Diagnostic Performance of 99mTc-Sestamibi Breast Imaging as Function of Mammographic Likelihood of Breast Cancer
Invasive Cancer Versus DCIS
Although our primary analysis classified DCIS as malignant, cognizant of the controversy over whether all DCIS progresses to invasive cancer, we also analyzed the sensitivity for invasive cancer and for DCIS separately. Overall institutional sensitivity was 82.0% for invasive cancer and 45.9% for DCIS (P < 0.001). For women with palpable abnormalities, sensitivity was 90.5% for invasive cancer and 57.1% for DCIS (P = 0.002). For women with nonpalpable abnormalities, sensitivity was 69.2% for invasive cancer and 39.1% for DCIS (P = 0.02).
Time of Imaging
We were interested in evaluating the impact of time of imaging after 99mTc-sestamibi injection on diagnostic accuracy because 99mTc-sestamibi tumor efflux could lead to decreased diagnostic sensitivity for delayed imaging. Overall institutional results showed a modest decrease in sensitivity for delayed imaging and a corresponding increase in specificity. However, diagnostic accuracy (Table 4) and area under the receiver operating characteristic curve were comparable for early and delayed imaging. Consequently, to ensure highest sensitivity for the identification of malignant abnormalities, we recommend early scintigraphic imaging only.
Diagnostic Performance by Imaging Time
Inter-Reader Agreement
Reproducibility for the detection of malignancy among the blinded readers was very high. Inter-reader agreement among the three blinded readers who read scintigraphic images from subjects with palpable abnormalities ranged from 96% to 100% (κ = 0.93–0.99). Inter-reader agreement for evaluation of nonpalpable abnormalities ranged from 95% to 96% (κ = 0.82–0.89).
Multivariable Regression Analysis
The only independent predictors of a true-positive 99mTc-sestamibi image in the multivariable regression analysis were lesion palpability and tumor size (global χ2 = 37.7). The analysis was also conducted excluding tumor size, as would occur for abnormalities detected solely as microcalcifications. Lesion palpability became the only predictive variable in that model.
DISCUSSION
Approximately 25 million mammographic examinations are performed annually in the United States for the screening and diagnosis of breast cancer. Despite widespread clinical acceptance and extensive refinement, 5%–15% of breast cancers are not visualized by this procedure. Some breast parenchymal patterns may compromise definitive mammographic interpretation and a large percentage of mammographically missed carcinomas have been ascribed to problems associated with imaging the dense breast (23). Highly nodular breasts, breasts with diffuse patterns of indistinct microcalcifications, and postsurgical parenchymal scarring and distortion of normal breast tissue associated with implants or radiation therapy pose additional challenges to the radiologist.
Improvements in mammography techniques and procedures can certainly overcome some of these interpretive challenges. However, an adjunctive technique such as 99mTc-sestamibi breast imaging, which relies on characteristics of tumor growth, has promise as a tool to assist in resolving difficult-to-interpret mammograms.
Earlier studies of 99mTc-sestamibi breast imaging reported diagnostic sensitivities ranging from 83% to 96% and specificities ranging from 83% to 94% in populations with disease prevalence ranging from 29% to 84% (11–20). Although some of these reports evaluated 99mTc-sestamibi breast imaging of both palpable and nonpalpable abnormalities, any attempt to estimate diagnostic sensitivity from these 10 earlier studies would be based on results from only 13 nonpalpable cancers. Thus, although these single center studies were limited by their focus on palpable abnormalities and their referral bias as evidenced by the high prevalence of disease, they did suggest the value of more systematically studying the diagnostic performance of 99mTc-sestamibi breast imaging. More recently, reports have appeared from multicenter studies conducted in Europe. The European multicenter trial reported an overall blinded sensitivity of 71% in a population with 65% disease prevalence, a sensitivity for palpable malignancy of 83%, and a sensitivity for nonpalpable malignancy of 30% (24). The Spanish multicenter study reported an overall blinded sensitivity of 90% in a population with 59% disease prevalence, a sensitivity for palpable malignancy of 94%, and a sensitivity for nonpalpable malignancy of 75% (25). Similar to many of the single center reports, a high prevalence of disease represented a limitation to these studies. Additionally, the results for nonpalpable abnormalities are difficult to evaluate because only 38 nonpalpable malignancies were included in the European trial and, although 126 nonpalpable lesions were represented in the Spanish study, the number of nonpalpable malignancies is not reported.
We examined the diagnostic accuracy of 99mTc-sestamibi breast imaging in women suspected of having breast cancer and scheduled for excisional biopsy or mastectomy. Diagnostic accuracy was also evaluated as a function of patient age, tumor size, and mammographers' estimate of likelihood of malignancy. The overall institutional sensitivity and specificity were 75.4% and 82.7% with a 79.8% diagnostic accuracy. In this population with a 40.1% disease prevalence, the positive predictive value was 74.5% and the negative predictive value was 83.4%. The sensitivity was lowest for nonpalpable tumors <1 cm in their largest dimension.
Screening mammography shows decreased sensitivity for invasive cancer in younger women compared with that of older women. Initially attributed to a higher prevalence of radiographically dense breasts in younger women, recent studies suggest that more rapid tumor growth and the greater prevalence of interval cancer in younger women may be the main cause of lower sensitivity (26,27). Multivariable regression analysis in this study showed that patient age was not predictive of a true-positive 99mTc-sestamibi image. Additionally, previous reports have shown that the sensitivity of 99mTc-sestamibi breast imaging is comparable in patients with dense and fatty breasts (28,29). This suggests an adjunctive usefulness for 99mTc-sestamibi breast imaging in younger patients, particularly in those with radiographically dense breasts.
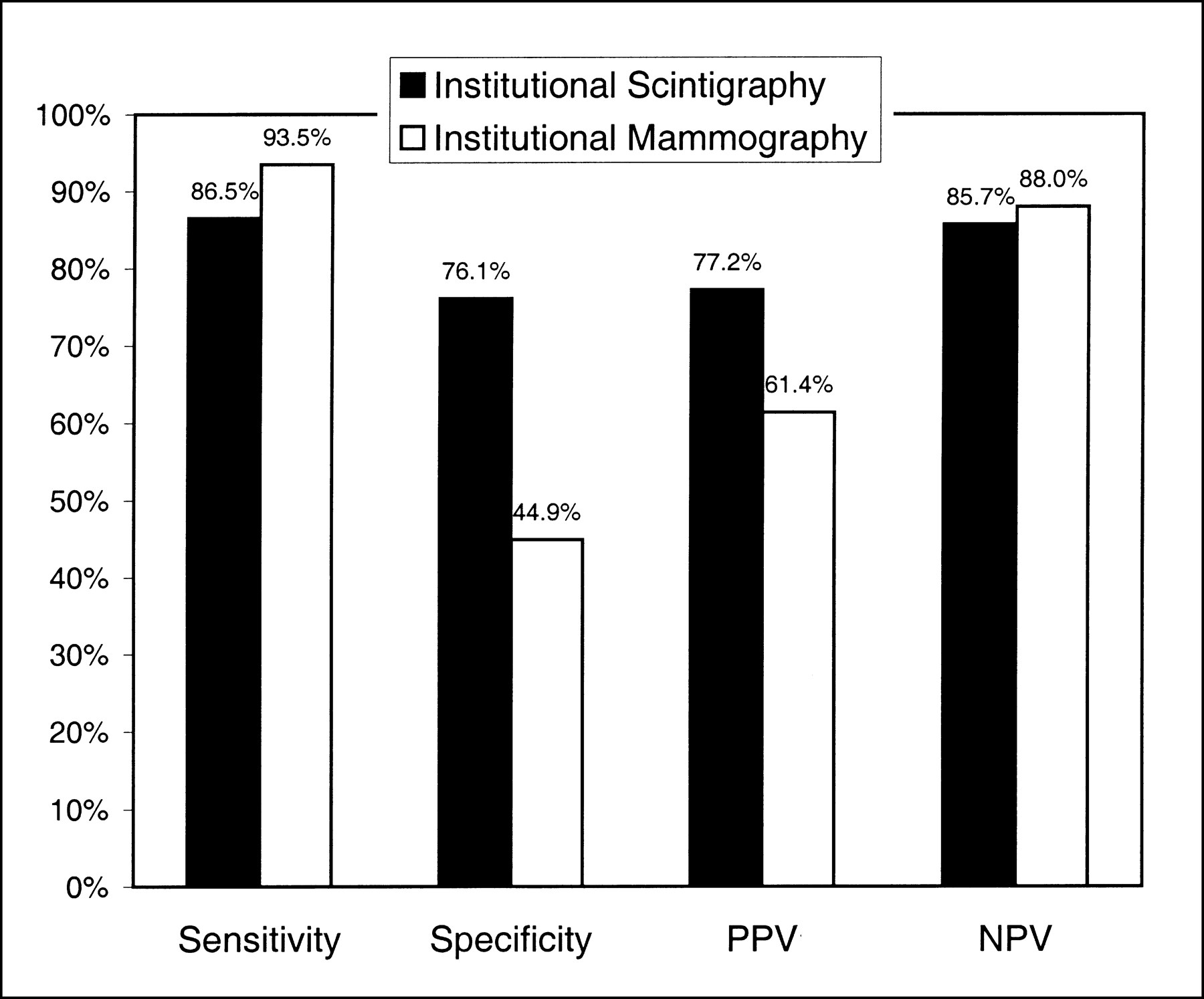
We also compared the performance of mammography and 99mTc-sestamibi scintimammography in the same population. The institutional 99mTc-sestamibi scintimammography sensitivity and negative predictive value for patients with palpable abnormalities were comparable with mammography; however, the specificity and positive predictive value were higher (Fig. 3).

Diagnostic statistics for 99mTc-sestamibi breast imaging and for mammography in patients with palpable abnormalities. PPV = positive predictive value; NPV = negative predictive value.
Evaluation of diagnostic imaging procedures often focuses on the global presence of disease (e.g., in a breast) without consideration of whether the specific imaged abnormality represents disease. Thus, although other reports have been limited by their lack of attention to this issue, one limitation of our study is the possibility of errors in the correlation of the location of scintigraphic abnormalities with the exact location of the palpable or mammographic abnormalities and with the excised tissue. The lesion correlation process also served to identify scintigraphic abnormalities that did not correspond to mammographic or palpable abnormalities, which could hence represent false-positive findings were biopsy information available on such abnormalities. Preliminary studies of a scintigraphic needle localization technique (30) have shown the presence of malignancy in two of three patients with such scintigraphic abnormalities. Further development of this localization technique is essential to facilitate trials to better address issues of lesion correlation and the significance of scintigraphic abnormalities that correspond to neither palpable nor mammographic abnormalities.
Finally, our study is limited by subject enrollment criteria. Because each subject enrolled in this study was already scheduled for biopsy, our results should not be generalized to a screening population. However, the high negative predictive value in subjects with a low-to-intermediate likelihood of malignancy (Table 3) does suggest an adjunctive value for 99mTc-sestamibi breast imaging.
CONCLUSION
As an adjunct to current diagnostic procedures, 99mTc-sestamibi breast imaging may make a unique contribution to patient management decisions in selected patient populations. These groups include women with dense breasts, women with nonpalpable mammographically indeterminate lesions >1 cm, and women with palpable abnormalities.
This multicenter study on 563 subjects with biopsy confirmation defined the diagnostic characteristics of planar 99mTc-sestamibi breast imaging. The institutional sensitivity and specificity for breast cancer detection in palpable lesions were 87% and 76% and were 61% and 87% for nonpalpable lesions. The negative predictive value was 94% in patients with a 40% or lower mammographic likelihood of breast cancer. Sensitivity is independent of patient age, breast density, and mammographically established likelihood of malignancy but is decreased for small nonpalpable tumors.
Acknowledgments
The authors thank the patients and study coordinators who contributed to this study; the DuPont Pharmaceuticals Medical Research Staff, in particular Lori Bernard, MS, Edward Hogan, MS, Bernadette Emond, Rosemary Kerwin, RPh, Rommel Hidalgo, BS, and Tsushung A. Hua, PhD; and the blinded readers, core laboratory staffs, and principal investigators. The authors also express their appreciation to Mary Atkinson and Nancy Bush for their assistance in preparation of this manuscript. This study was supported by grants from DuPont Pharmaceuticals Company. This work was presented in part at the 43rd Annual Meeting of the Society of Nuclear Medicine, Denver, CO, June 3–5, 1996.
Footnotes
Received Nov. 29, 1999; revision accepted May 16, 2000.
For correspondence or reprints contact: Stephen B. Haber, PhD, DuPont Pharmaceuticals Company, 331 Treble Cove Rd., 500-2, North Billerica, MA 01862.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Bridge Not Too Far: Linking Disciplines Through Molecular Imaging Probes
- Nuclear Breast Imaging: Clinical Results and Future Directions
- A Bridge Not Too Far: Linking Disciplines Through Molecular Imaging Probes
- Comparison between 99mTc-Sestamibi Scintimammography and X-ray Mammography in the Characterization of Clusters of Microcalcifications: A Prospective Long-term Study
- Integrin Receptor Imaging of Breast Cancer: A Proof-of-Concept Study to Evaluate 99mTc-NC100692
- Inconclusive Triple Diagnosis in Breast Cancer Imaging: Is There a Place for Scintimammography?
- Tissue-Specific Effects on Uptake of 99mTc-Sestamibi by Breast Lesions: A Targeted Analysis of False Scintigraphic Diagnoses
- Are We Ready for Dedicated Breast Imaging Approaches?
- Evaluation of a Small Cadmium Zinc Telluride Detector for Scintimammography
- Diagnostic Value of 99mTc-Methylene Diphosphonate and 99mTc-Pentavalent DMSA Compared with 99mTc-Sestamibi for Palpable Breast Lesions
- Invited Commentary: One Step Forward
- Prognostic Value of 99mTc-Sestamibi Washout in Predicting Response of Locally Advanced Breast Cancer to Neoadjuvant Chemotherapy
- What Can We Expect from MDR Breast Cancer Imaging with Sestamibi?
- Sestamibi Scanning of Breast Cancer
- Is 99mTc-Sestamibi Scintimammography Complementary to Conventional Mammography for Detecting Breast Cancer in Patients with Palpable Masses?
- Scintimammography