


Abstract
The objective of this study was to evaluate the role of quantitative perfusion lung scintigraphy (QPLS) in predicting the development of chronic rejection in patients who underwent single-lung transplantation. Methods: Eighteen patients (15 men, 3 women; age range, 41–60 y; mean age, 54.6 ± 6.0 y) who underwent single-lung transplantation for emphysema (n = 14) or pulmonary fibrosis (n = 4) were studied. Patients were evaluated using QPLS and pulmonary function tests before surgery and at 1–3 mo and 1–3 y after transplantation. Relative perfusion of the transplanted lung was calculated from standard perfusion lung scintigrams. Values for forced expiratory volume in the first second (FEV1) were obtained from lung function tests at the same time points. The maximal and minimal relative perfusion and FEV1 values in the early (1–3 mo) and late (1–3 y) follow-up periods were identified for each patient. Receiver operating curve (ROC) analysis was performed on all parameters. Results: In total, 82 lung scans were performed (mean, 4.8 ± 1.55 per patient) and 484 FEV1 test determinations were obtained (mean, 30.0 ± 15.6 per patient) during a follow-up period ranging from 8 to 84 mo (mean, 39.6 ± 19.3 mo). In 7 of the 18 patients, chronic rejection developed, whereas 11 patients had a favorable outcome. No significant difference was found in the number of complications (acute rejection and infection episodes) between patients with a favorable outcome and patients with chronic rejection, up to 1 y after transplantation. At 1–3 mo, minimal relative perfusion values were 67.1% ± 12.2% in the favorable outcome group and 50.8% ± 9.6% in the chronic rejection group (P = 0.02). Before surgery and at 1–3 y, minimal relative perfusion was not significantly different between the 2 groups. The difference in maximal relative perfusion at 1–3 y was marginally significant, with 76.5% ± 8.9% in the favorable group and 64.3% ± 15.0% in the chronic rejection group (P = 0.051). FEV1 values were not significantly different preoperatively and 1–3 mo after surgery between the chronic rejection and the favorable outcome groups. Late in the follow-up period (1–3 y), FEV1 values in the chronic rejection and favorable outcome groups were 35.6% ± 7.9% and 56.9% ± 13.6%, respectively (P = 0.002). ROC analysis of minimal relative perfusion at 1–3 mo identified a threshold of 57% under which the sensitivity and specificity for chronic rejection were 83% and 88%, respectively. Minimal FEV1 for the same period identified a threshold of 48% under which the sensitivity and the specificity were 80% and 67%, respectively. Conclusion: QPLS early after transplantation in our patients predicted the development of chronic rejection in patients with single-lung transplantation for emphysema and pulmonary fibrosis, whereas surgical complications, acute rejection, infection episodes, and lung function tests did not predict the outcome. This early prediction could not be obtained from lung function tests performed at the same time.
Single-lung transplantation has become an effective mode of therapy for patients with end-stage chronic obstructive lung disease and pulmonary fibrosis. Advances in lung preservation and surgical technique as well as immunosuppressive therapy have markedly improved the survival rate. Common complications that occur in the first 6 mo after transplantation are infection and acute rejection, the latter being effectively treated with immunosuppression. After this initial period, patients are monitored for the effects of immunosuppressive therapy and for early detection of chronic rejection. The histologic manifestation of chronic rejection is bronchiolitis obliterans (1,2), a rapidly progressive inflammatory disorder of the small airways of the transplanted lung causing severe obstructive lung disease, mostly irreversible and unresponsive to therapy (1). The inflammatory airway changes induce perfusion abnormalities, which can be visualized on perfusion lung scintigraphy. This technique is therefore an effective tool for monitoring this disease process (3). The goal of this study was to evaluate the role of quantitative perfusion lung scintigraphy (QPLS) and lung function tests in the early prediction of chronic rejection.
MATERIALS AND METHODS
Patients
Eighteen patients (15 men, 3 women; age range, 41–60 y; mean age, 54.6 ± 6.0 y) who underwent single-lung transplantation in Rabin Medical Center and Hadassah University Hospital were studied between 1993 and 1998. Patients who survived the operation for more than 6 mo were included in the study. Transplantation was performed on 14 patients for emphysema and on 4 patients for pulmonary fibrosis.
All patients received standard immunosuppression, which included cyclosporin A, prednisone, and azathioprine. No induction therapy was given. Gancyclovir for cytomegalovirus prophylaxis (4 wk), itraconazole (6 mo), and trimethoprim-sulfamethoxazole (3 times per week) were also administered. In cases of acute rejection, methylprednisolone (1 g/day) was administered for 3 consecutive days.
Patients were classified as having a favorable outcome or chronic rejection. The criteria for chronic rejection were based on the working formulation for the determination of chronic dysfunction in lung allografts associated with the histologic pattern of bronchiolitis obliterans (2,3). Bronchiolitis obliterans was classified as mild, moderate, or severe when values for forced expiratory volume in the first second (FEV1) decreased to 66%–80%, 51%–65%, or 50% or less, respectively, from the baseline values. The presence or absence of pathologic evidence of bronchiolitis obliterans also characterized each stage.
Lung Function Evaluation and Radionuclide Perfusion Studies
Lung function tests included the FEV1 obtained from spirometry. FEV1 tests were performed before surgery, every week during the first 3 mo, every 2 wk up to 1 y after transplantation, and every 3 mo thereafter. Studies were performed more frequently if clinically indicated. Bronchoscopy was performed on days 7, 14, and 30 after transplantation; 3 mo after transplantation; and when clinically indicated, as when lung function dropped or infection and rejection were suspected. FEV1 values were determined for the same times at which perfusion lung scintigraphy was performed and were expressed as a percentage of the predicted FEV1.
QPLS was performed before transplantation, several times in the first 3 mo after transplantation, and every 6 mo thereafter. Scintigraphy was performed after intravenous administration of 111 MBq (3 mCi) 99mTc-macroaggregated albumin (Pulmolite; DuPont, Billerica, MA) with the patient supine. A single-head gamma camera (SPX-4; Elscint Ltd., Haifa, Israel) equipped with a parallel-hole collimator was used. Anterior, posterior, and left and right posterior oblique views were obtained, collecting 500,000–700,000 counts per view. The posterior view was used for calculation of the relative perfusion. Right and left lung counts were separately obtained from rectangular regions of interest. The percentage of the transplanted lung counts from the total lung counts was called relative perfusion.
Data Analysis
Follow-up was divided into 2 intervals: an early phase 1–3 mo after transplantation and a late phase 1–3 y after transplantation. The lowest (minimal) and the highest (maximal) relative perfusion and FEV1 values were identified for each patient in each interval. A 2-tailed Student t test was used for comparison of these variables in the favorable outcome and chronic rejection groups. A probability value of 0.05 or less was considered statistically significant. Receiver operating curve (ROC) analysis was used to identify the threshold under which the chronic rejection group would be best identified.
RESULTS
Eighteen patients were followed up for 8–84 mo after transplantation (mean, 39.6 ± 19.3 mo). Eleven patients had a favorable outcome, and chronic rejection of the transplanted lung developed in 7 patients. The diagnosis of chronic rejection was established during follow-up and was based on FEV1 values and biopsy results.
Eighty-two perfusion lung scans were obtained, with a mean of 4.80 ± 1.55 per patient (range, 3–8). FEV1 values were obtained 484 times, with a mean of 30.0 ± 15.6 determinations per patient (range, 13–74). Table 1 describes the surgical complications, acute rejection episodes, and infection episodes in the early (≤3 mo) and 4- to 12-mo periods after transplantation in 17 of the 18 patients. Information about 1 patient was not available.
Clinical Data and Outcome in Patients After Single-Lung Transplantation
The number of acute rejection episodes was similar in the favorable outcome group and in the chronic rejection group during the first 3 mo after transplantation (1.30 ± 0.95 versus 1.28 ± 0.95, P = 0.97). For the same period, 1.20 ± 1.22 and 0.57 ± 0.97 episodes of infection occurred in the favorable and chronic rejection groups, respectively (P = 0.28). The number of episodes of acute rejection and infection recorded at this early period was 2.50 ± 1.27 and 1.80 ± 0.34, respectively, for the 2 groups of patients (P = 0.22).
Four to 12 mo after transplantation, no difference was observed in acute rejection episodes (0.30 ± 0.67 versus 0.43 ± 0.79, P = 0.72), acute infection episodes (0.40 ± 0.70 versus 0.43 ± 0.53, P = 0.92), and all episodes (0.7 ± 1.06 versus 0.86 ± 0.90, P = 0.75) in the 2 groups of patients. The total number of episodes in the first year (acute rejection and infection) were not significantly different between patients with a favorable outcome and patients with chronic rejection (2.90 ± 2.33 versus 2.71 ± 1, P = 0.84). Four surgical complications occurred in the study group: bronchial stenosis and infection of the bronchial anastomosis in the favorable outcome group and bronchial stenosis in 2 patients of the chronic rejection group.
The results of relative perfusion lung scintigraphy and FEV1 values in the favorable outcome and chronic rejection groups are shown in Table 2 and in Figures 1 and 2. No significant difference was observed between the 2 patient groups before transplantation.
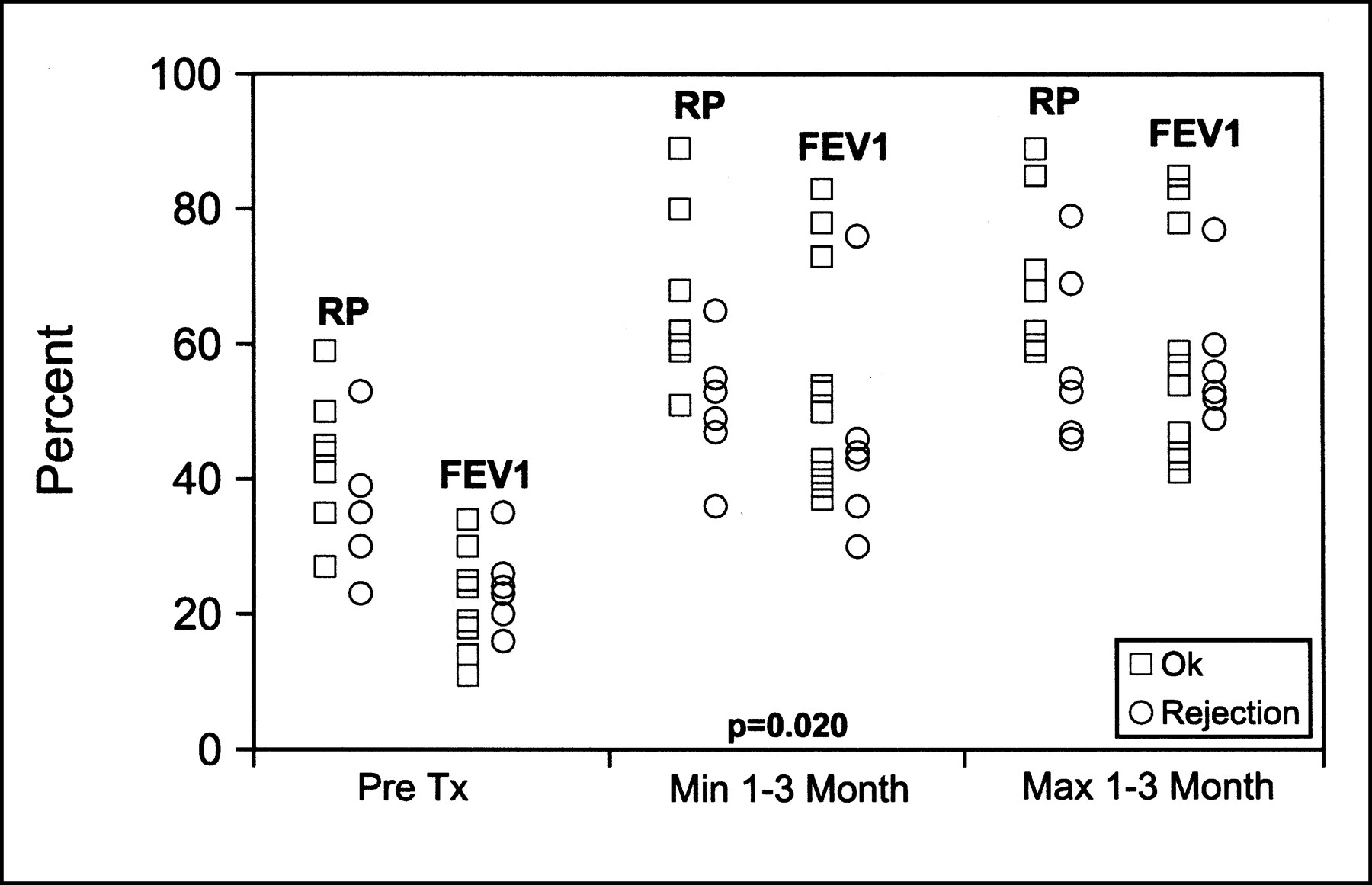
Relative perfusion (RP) of transplanted lung and FEV1 values before transplantation and early (1–3 mo) after transplantation. Max = maximal value; Min = minimal value; Pre Tx = before transplantation. Number of data points in each group represents available data for that group (Table 2).
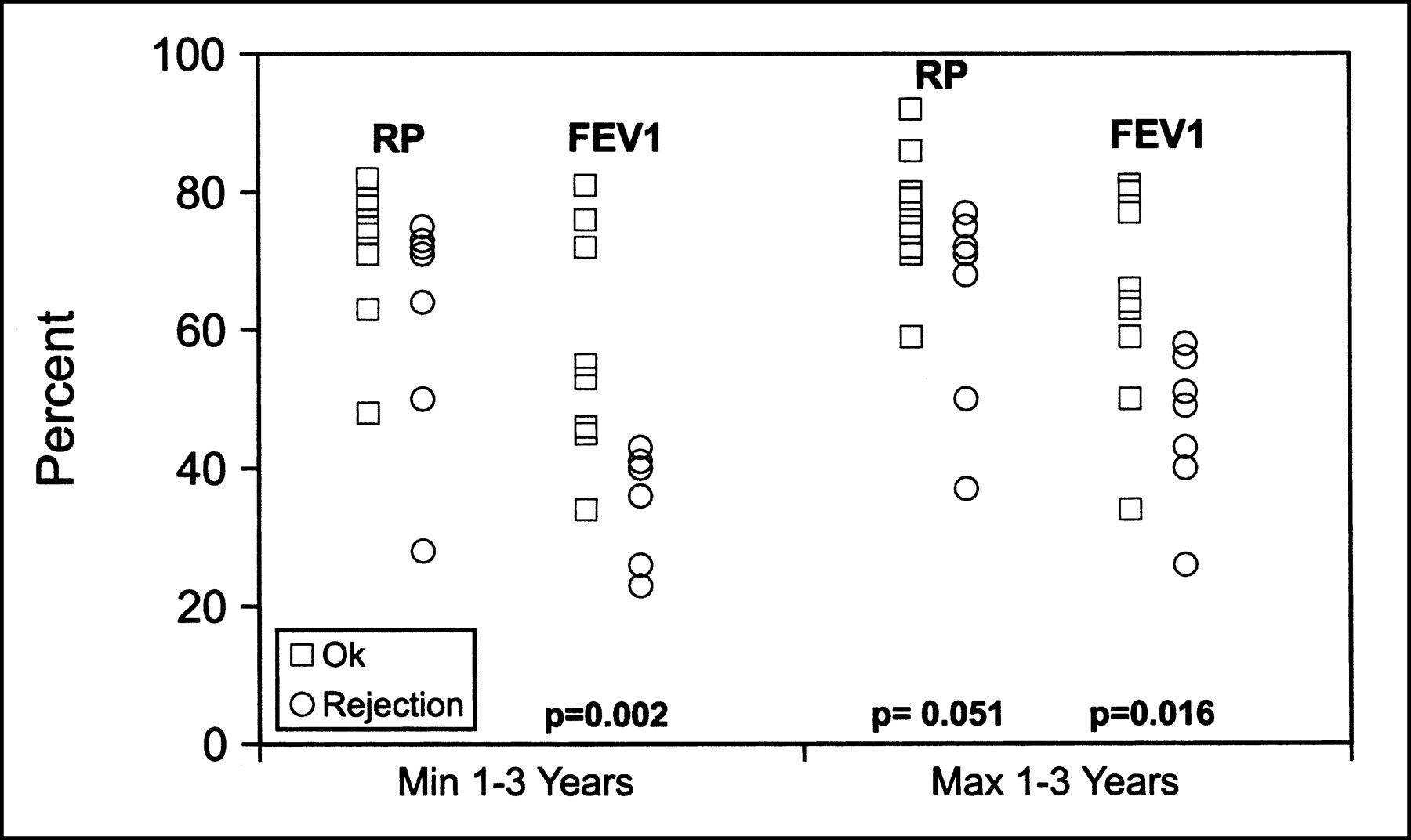
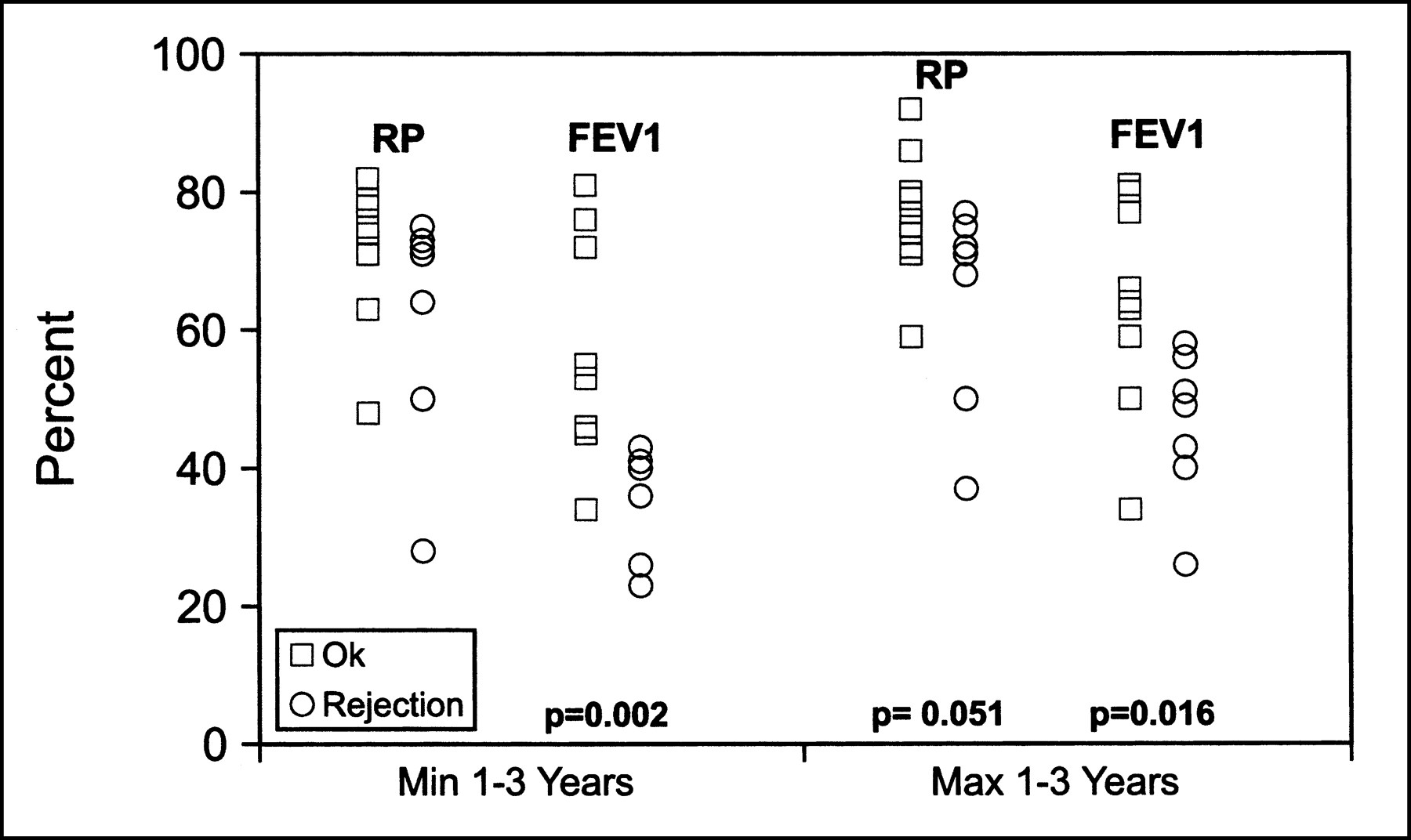
Relative perfusion (RP) of transplanted lung and FEV1 late (1–3 y) after transplantation. Max = maximal value; Min = minimal value. Number of data points in each group represents available data for that group (Table 2).
Relative Perfusion and FEV1 Values in Patient Population
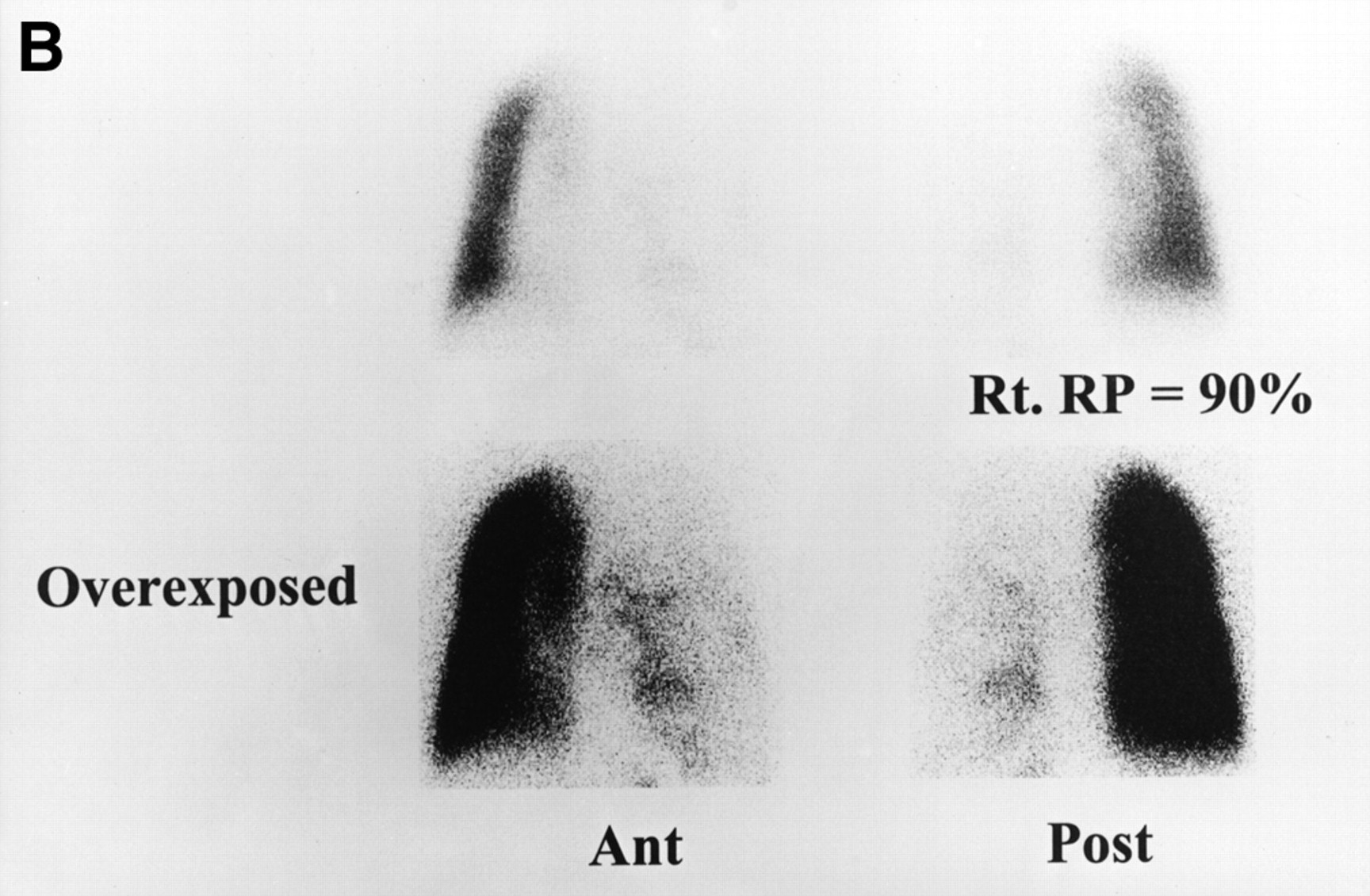
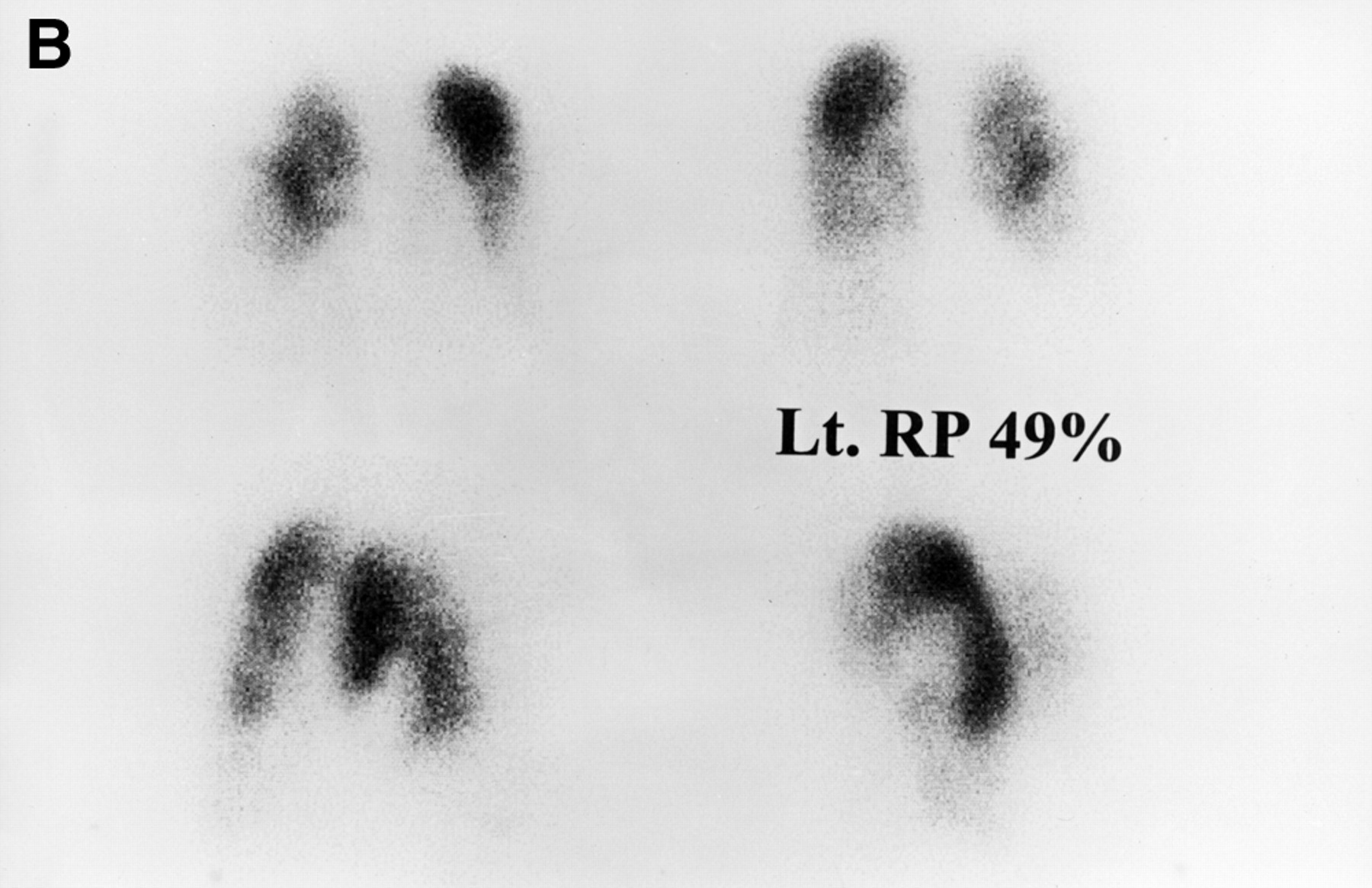
In the early period (1–3 mo) after transplantation, a significant difference was seen in the minimal values of relative perfusion between the 2 groups (P = 0.02), but no difference in maximal relative perfusion, minimal FEV1, or maximal FEV1 values were seen (Table 2; Fig. 1). Later in the follow-up of these patients (1–3 y after transplantation), minimal FEV1 deteriorated in the chronic rejection group (P = 0.002), as expected, because the definition of chronic rejection is based on these values (4,5). Maximal FEV1 was also significantly different in the 2 groups at 1–3 y after transplantation (P = 0.016). During the same interval, minimal relative perfusion was not statistically different, and maximal relative perfusion was marginally significant (P = 0.051) between the 2 groups (Table 2; Fig. 2). Examples of patients with favorable outcome and chronic rejection are presented in Figures 3 and 4, respectively. After transplantation, the entire transplanted lung had homogeneous perfusion and remained homogeneous during follow-up (Fig. 3B). Patients who developed chronic rejection showed small perfusion defects and a heterogeneous perfusion pattern in the transplanted lung, similar to the pattern of the native lung (Fig. 4B).
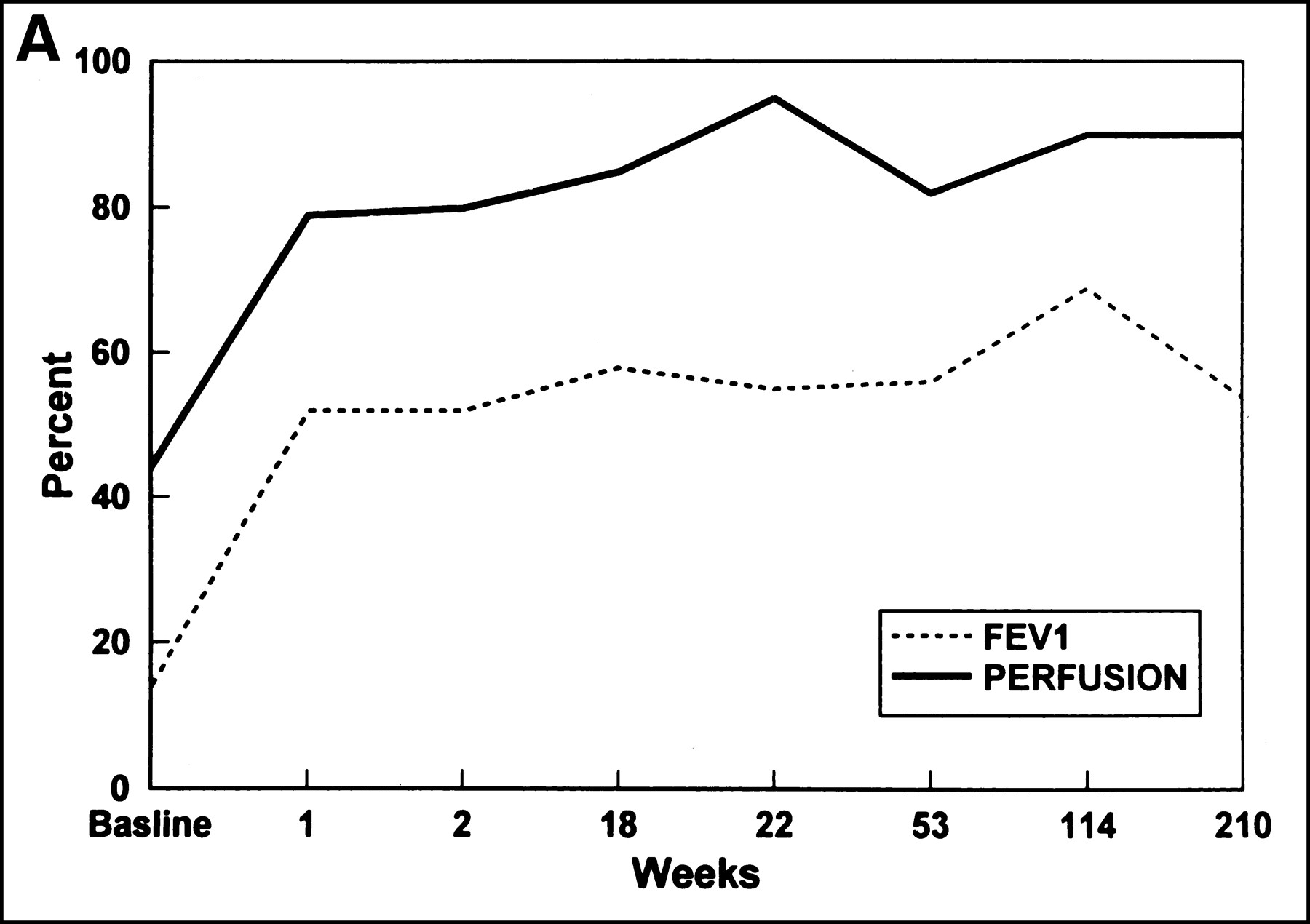

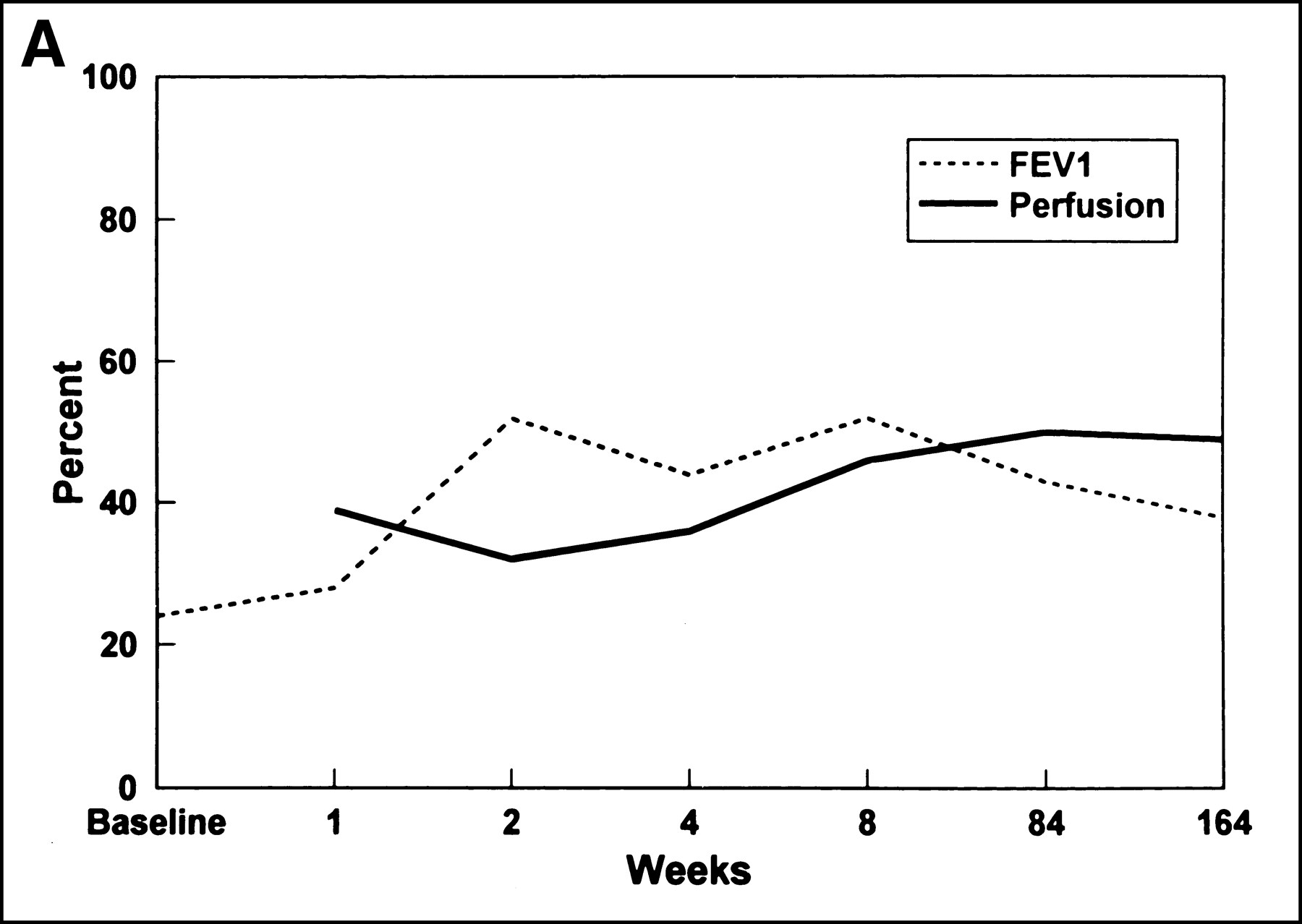
Relative perfusion (RP) of transplanted lung and FEV1 values during 210 wk of follow-up (A) and perfusion images at 210 wk (B) for patient with favorable outcome. Ant = anterior; Post = posterior; Rt. = right.


Relative perfusion (RP) of transplanted lung and FEV1 values during 164 wk of follow-up (A) and perfusion images at 164 wk (B) for patient with chronic rejection. Lt. = left.
The ROC analysis of the data is presented in Table 3. ROC analysis of early relative perfusion values identified a threshold of 57% under which sensitivity and specificity for the detection of chronic rejection were 83% and 88%, respectively (Fig. 5). For the same period, an FEV1 threshold of 46% had a sensitivity of 83% but a specificity of only 60%. Because of very low specificity, ROC analysis of relative perfusion during the late follow-up period revealed no threshold values that could be used to distinguish between the 2 groups, whereas minimal and maximal FEV1 values showed a sensitivity of 100% and a specificity of 78% for an FEV1 threshold of 75% and 79%, respectively.

ROC curve of relative perfusion of transplanted lung.
ROC Analysis of Relative Perfusion and FEV1 Values in Patient Population
DISCUSSION
The cause of bronchiolitis obliterans in transplanted lungs is uncertain. It is characterized by the accumulation of lymphocytes in the submucosa of the inflamed airways and is affected by HLA mismatch (6). This pathologic process, because it responds to immunosuppression, is probably caused by rejection.
Infection may also be a possible cause of the inflammatory reaction and may precede the deterioration of lung function. Lung denervation and the loss of bronchial circulation in the transplant may also play a role in damage of the small airways (6). Early rejection and cytomegalovirus infection were found in some reports as a possible cause of bronchiolitis obliterans. In our group of patients, we could find no association between increased numbers of infection episodes, acute rejection episodes, or surgical complications in the early or late period after transplantation and the development of chronic rejection.
A working formulation for chronic dysfunction of lung allografts has been developed by a group of experts (4,5). The formulation is based on FEV1 by spirometry in conjunction with histologic findings on transbronchial biopsy specimens (5). The group claimed that the term “bronchiolitis obliterans” describes the manifestation of chronic rejection if there is no other cause for progressive airway disease. FEV1 values were, therefore, used in this study as lung function test criteria for identification of patients with and without chronic rejection.
After transplantation, perfusion shifts to the transplanted lung because of the relatively lower vascular resistance and intact vascular morphology of the graft. Several studies investigated lung perfusion and ventilation after transplantation in patients with emphysema (7,8), pulmonary hypertension (7,9), and pulmonary fibrosis (10). These studies found a marked shift of perfusion to the transplanted lung, more accentuated in patients with pulmonary hypertension than in patients with emphysema and pulmonary fibrosis. In cases of chronic rejection, the decrease in graft perfusion and the shift of perfusion toward the native lung may be caused by the inflammatory process of bronchiolitis obliterans or may reflect graft ischemia or graft vasculopathy. (4). Perfusion has been shown to deteriorate during early episodes of acute rejection (7). Some investigators have suggested that areas of decreased perfusion as documented by SPECT perfusion scintigraphy may be useful in directing lung biopsy, thus improving its yield in the diagnosis of bronchiolitis obliterans (3).
Ventilation scans of transplanted lungs with favorable outcome generally show relatively reduced ventilation compared with perfusion to the lung allograft (11,12). We therefore decided to base the scintigraphic evaluation on the more informative perfusion studies, using QPLS, at various times before and after transplantation. Our results indicated that patients in whom chronic rejection subsequently developed had low relative perfusion values in the transplanted lung during the early period after transplantation. A relative perfusion threshold of 57% was found to have a sensitivity of 83% and a specificity of 88% for chronic rejection. The diminished relative perfusion values were not associated with an increase in early episodes of acute rejection or infection or an increase in surgical complications. However, subclinical rejection episodes may not have been detected. Their corresponding FEV1 values at that early stage after transplantation did not differ significantly from those of patients with an uneventful outcome. These findings suggest that in patients in whom chronic rejection subsequently develops, a decrease in perfusion of the transplanted lung precedes changes in airway compliance.
During the late period after transplantation, when severe obstruction develops, FEV1 values clearly differentiated between patients with chronic rejection and patients with a favorable outcome. This observation was expected, because these values serve as criteria for chronic rejection. At this stage, QPLS showed lower values in patients with chronic rejection than in patients with a favorable outcome. The difference, however, was only marginally significant in our patients, possibly because of the small number of patients in the groups.
Our retrospective study, although of few patients, found that low relative perfusion in the early follow-up period (1–3 mo) after transplantation could predict later development of chronic rejection. Low early relative perfusion may be regarded as an early warning sign of chronic rejection, suggesting the need for biopsy and, perhaps, more intensive antirejection therapy. We believe that serial QPLS studies early after transplantation may enhance early detection of chronic rejection and affect therapeutic measures. Additional studies in a larger group of patients may be required to substantiate our observations.
CONCLUSION
In our study of patients who underwent single-lung transplantation for emphysema and pulmonary fibrosis, diminished perfusion in the transplanted lung early after transplantation predicted future development of chronic rejection. Deterioration was found earlier by scintigraphy than by standard pulmonary function tests. QPLS added valuable information and should be used in the follow-up of these patients.
Acknowledgments
This study was presented in part at the annual meeting of the Society of Nuclear Medicine, Los Angeles, CA, June 1999.
Footnotes
Received Oct. 19, 1999; revision accepted Apr. 4, 2000.
For correspondence or reprints contact: Ruth Hardoff, MD, DSc, Department of Nuclear Medicine, Rabin Medical Center, Beilinson Campus, Petach Tikva 49100, Israel.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.