


Abstract
Clinical diagnosis of skeletal tumors can be difficult, because such lesions compose a large, heterogeneous group of entities with different biologic behaviors. The aim of this prospective study was to assess the value of PET in grading tumors and tumorlike lesions of bone. Methods: Two hundred two patients with suspected primary bone tumors were investigated using FDG PET. Uptake of FDG was evaluated semiquantitatively by determining the tumor-to-background ratio (T/B). All patients underwent biopsy, resulting in the histologic detection of 70 high-grade sarcomas, 21 low-grade sarcomas, 40 benign tumors, 47 tumorlike lesions, 6 osseous lymphomas, 6 plasmacytomas, and 12 metastases of an unknown primary tumor. Results: All lesions, with the exception of 3 benign tumors, were detected by increased FDG uptake. Although sarcomas showed significantly higher T/Bs than did latent or active benign lesions (P < 0.001), aggressive benign lesions could not be distinguished from sarcomas. Using a T/B cutoff level for malignancy of 3.0, the sensitivity of FDG PET was 93.0%, the specificity was 66.7%, and the accuracy was 81.7%. Conclusion: FDG PET provides a promising tool for estimating the biologic activity of skeletal lesions, implicating consequences for the choice of surgical strategy.
- diagnosis of bone neoplasms
- bone neoplasms in infants and children
- sarcoma
- staging of bone neoplasms
- radionuclide imaging in diagnosis of neoplasms
Clinical diagnosis of tumors and tumorlike lesions of bone can be difficult, because they compose a multitude of entities with heterogeneous biologic behaviors. The potential for metastatic spread differs significantly between high-grade and low-grade sarcomas and even exists for some benign tumors such as giant cell tumors or benign chondroblastomas (1,2). Furthermore, high local aggressiveness occurs in certain stages of benign lesions.
Classification of skeletal lesions is based on an array of differentiated imaging modalities, implicating different surgical approaches. Some lesions require no treatment, some require biopsy, some curettage, and some en bloc resection as the primary therapeutic step. Malignant primary bone tumors such as osteosarcoma or Ewing's sarcoma typically occur at younger ages, and curative treatment is possible in most of these patients. Early detection and precise classification of these tumors helps to improve the prognosis. Misdiagnoses caused by inappropriate imaging techniques can lead to overtreatment of tumorlike lesions or undertreatment of aggressive or malignant bone tumors, with disastrous consequences. In osseous sarcomas, accurate histologic typing and grading determines surgical margins and the necessity for adjuvant treatment: whereas chondrosarcomas require only surgical therapy, high-grade chondroblastic osteosarcoma can be cured only by combined surgery and polychemotherapy. The reliability of the histologic diagnosis primarily depends on the experience of the pathologist and the quality and size of the biopsy specimen. Frequently, misdiagnoses are the result of biopsies taken from a part of the lesion that is not representative of the entire neoplasm.
With some entities, the diagnosis can be difficult even for an experienced bone tumor pathologist. For example, distinguishing proliferative chondroma from well-differentiated chondrosarcoma (1,2), or an aneurysmal bone cyst from telangiectatic osteosarcoma (1–3), sometimes can be impossible without knowledge of the radiologic appearance. Diagnosis of central, periosteal, or parosteal osteosarcomas, which require different treatment strategies, can be established only with the aid of subtle imaging techniques (1,2).
Elevated uptake of FDG as determined by PET has been reported for malignant mesenchymal tumors in a few studies. FDG PET has been proposed as a diagnostic tool for distinguishing benign from malignant soft tissue and osseous lesions (4–7), for grading sarcomas (6,8–10), and for detecting local recurrences (11,12). In addition, FDG PET has been used for monitoring chemotherapy responses (13) and detecting pulmonary metastases in osteogenic sarcoma (14). However, in a recent study of 26 patients with skeletal lesions, the biologic behavior of the tumors did not correlate with their glucose metabolism as quantified by FDG PET (15). The purpose of this study was to determine whether FDG PET is reliable for grading tumors and tumorlike lesions of bone.
MATERIALS AND METHODS
Patients
In a current prospective study initiated in January 1993, 202 patients (127 males, 75 females; age range, 1–78 y; median age, 28 y) with suspected primary bone tumors were examined by FDG PET. The study inclusion criterion was radiographic evidence of an osseous lesion suggestive of an active benign (Lodwick IB), aggressive benign (Lodwick IC), or malignant primary bone neoplasm and, therefore, the necessity for a biopsy. Patients who had latent lesions with no radiographic signs of activity (Lodwick IA) and without clinical symptoms were excluded, whereas 8 patients who had a Lodwick IA lesion and presented with local pain underwent PET and biopsy. No restrictions on patient age were imposed. All patients or their parents gave written informed consent to be scanned with FDG PET before biopsy.
The tumors were localized in the femur (n = 56), pelvis (n = 48), humerus (n = 32), lower leg (n = 30), thorax (n = 25), spine (n = 6), forearm (n = 3), or foot (n = 2). The size of the lesions ranged from 2.9 to 78.6 cm2 on transaxial sections.
Incisional, excisional, or needle biopsy was performed within 8 d after PET. All patients with a diagnosis of primary bone neoplasm underwent tumor resection. The majority of high-grade sarcomas received neoadjuvant chemotherapy. Definitive histopathologic evaluation of the surgical specimen revealed 115 malignant and 87 benign lesions, comprising 70 high-grade sarcomas, 21 low-grade sarcomas, 40 benign tumors, 47 tumorlike lesions, 6 osseous lymphomas, 6 plasmacytomas, and 12 metastases of an unknown primary tumor. Sarcomas were classified as high grade or low grade according to Enneking (16), including histologic, radiographic, and clinical criteria. Likewise, benign tumors were classified as latent (stage 1), active (stage 2), or aggressive (stage 3) (16).
FDG PET
FDG PET studies were performed as described by Stollfuss et al. (17) with a commercially available scanner (ECAT 931–08–12; Siemens/CTI, Knoxville, TN) that permits simultaneous acquisition of 15 contiguous sections of 6.75-mm thickness with an axial field of view of 10.1 cm. The minimum resolution was 7 mm full width at half maximum at the center of the field of view. Attenuation was corrected with a rotating 68Ge–68Ga source. Depending on tumor size, transmission scans with a duration of 8 min per bed position were obtained for at least 3 bed positions, without overlap, on the same day as and before emission scans. Thus, repositioning of the patients was necessary using multiple laser-guided landmarks. The patients fasted for at least 8 h before the study; normal plasma glucose levels were documented before FDG administration. In accord with a study by Ichiya et al. (18), semiquantitative assessment of tumoral FDG uptake was based on static emission scans of the tumor site and the corresponding contralateral area, with 2 or 3 contiguous bed positions, starting no earlier than 45 min (range, 45–60 min) after intravenous administration of a body mass–dependent dose of 120–300 MBq FDG. The acquisition time was 10 min per bed position. Images were reconstructed with a multiplicative iterative reconstruction algorithm (19).
Data Analysis
The PET scans were evaluated qualitatively and semiquantitatively by analyzing the zones with elevated FDG uptake on transaxial, coronal, and sagittal sections. Regions of interest (ROIs) were individually defined for each lesion, excluding any areas without detectable uptake within the tumor. ROIs were defined in the transaxial section expressing maximum uptake and were larger than 2.6 cm2 in each instance. Therefore, the ROI was always at least 2 times the minimum resolution of the PET scanner (7 mm). The neoplasm was clearly demarcated from surrounding tissue, and the boundaries of the ROI were just within the apparent hypermetabolic zone of the tumor. Quantitative assessment of FDG uptake was based on transaxial sections exclusively. Tumor-to-background ratios (T/Bs) were calculated using an ROI of identical configuration in the analogous site of the contralateral extremity, pelvic bone, or chest. In patients with a vertebral lesion, an adjacent unaffected vertebral body was used as a reference region. To assess interobserver error, T/Bs were obtained by 2 independent physicians without knowledge of the clinical data and were averaged for statistical evaluation.
Statistical Analysis
The Mann-Whitney test was used to compare the T/Bs of different subgroups, and 95% confidence intervals (CIs) were calculated according to Clopper and Pearson (20).
RESULTS
Of 202 tumors investigated, 1 benign tumor and 2 tumorlike lesions could not be visualized by FDG PET. A stage 1 osteochondroma of the proximal femoral metaphysis, a sclerotic alteration of a thoracic vertebral body, and an osteonecrotic lesion of the humeral head caused by previous radiotherapy did not express any change in glucose metabolism compared with the reference region. All other lesions could clearly be detected by increased FDG uptake, with T/Bs ranging from 1.1 to 73.0. Interobserver deviation of T/Bs ranged from 2% to 12% (median, 4%).
Histologic diagnoses and the distribution of T/Bs are listed in Table 1. Table 2 correlates FDG uptake with the biologic activity of the investigated tumors. Among the sarcomas, osteosarcomas had a tendency toward higher T/Bs than did Ewing's sarcomas (P < 0.01) and chondrosarcomas (P < 0.001). Glucose metabolism was greater for high-grade malignant lesions than for low-grade sarcomas (P < 0.01), but no difference was observed in comparisons with aggressive benign tumors. The T/Bs of stage 1 and 2 benign lesions were significantly lower than those of stage 3 benign lesions (P < 0.001) and of low-grade sarcomas (P < 0.001). Benign cartilage tumors showed a lower FDG uptake than did chondrosarcomas (P < 0.01). Among the benign lesions, giant cell tumors disclosed a significantly elevated glucose metabolism (P < 0.001).
Histologic Diagnosis and Distribution of T/B Values for 202 Skeletal Lesions
Distribution of T/B Values for Skeletal Lesions of Different Biologic Activity
Using a T/B cutoff level of 3.0 for malignancy (prevalence, 56.9%), the sensitivity of FDG PET was 93.0% (CI, 87%–96%), the specificity was 66.7% (CI, 56%–76%), the accuracy was 81.7% (CI, 77%–87%), the positive predictive value was 78.7% (CI, 71%–85%), and the negative predictive value was 87.9% (CI, 78%–95%).
FDG PET revealed false-negative results for 6 low-grade sarcomas (G 1) and 2 plasmacytomas. No false-negative results occurred among high-grade sarcomas, lymphomas of bone, and skeletal metastases. In particular, false-negative results were found for 6 patients with low-grade chondrosarcoma (n = 12), among them 1 woman with Ollier's disease, in which malignant transformation of a chondroma had occurred. However, both patients with high-grade chondrosarcoma had markedly elevated glucose metabolism. No false-negative findings occurred for patients with osteosarcoma (n = 44; Fig. 1), Ewing's sarcoma (n = 14), malignant fibrous histiocytoma of bone (n = 6), or angiosarcoma of bone (n = 3).

A 14-y-old boy with thoracic high-grade chondroblastic osteosarcoma. (A) Radiograph shows osteolytic destruction of seventh rib. (B) MR image shows inhomogeneous uptake of gadolinium–diethylenetriaminepentaacetic acid within primary lesion and highly vascularized tumor satellite adjacent to diaphragm. (C) PET image before neoadjuvant chemotherapy shows inhomogeneous FDG uptake in primary lesion (T/B, 10.3) and homogeneous hypermetabolism of satellite (T/B, 11.7).
Using a T/B cutoff level of 3.0, malignancy was falsely predicted for 29 benign lesions, including all cases of giant cell tumor (n = 5; Fig. 2), fibrous dysplasia (n = 3), eosinophilic granuloma (n = 2), chondroblastoma (n = 2), chondromyxoid fibroma (n = 1), desmoplastic fibroma (n = 1), and parathyroid osteopathy (n = 1); 6 of 15 cases of aneurysmatic bone cyst; 3 of 6 cases of nonossifying fibroma; 1 simple bone cyst complicated by pathologic fracture; and 3 of 10 cases of hematogenous osteomyelitis. As far as the biologic activity of benign tumors is concerned, PET revealed false-positive results for all stage 3 aggressive lesions (n = 12), 13 of 43 stage 2 active lesions (30.2%), and no stage 1 latent lesions (n = 11).
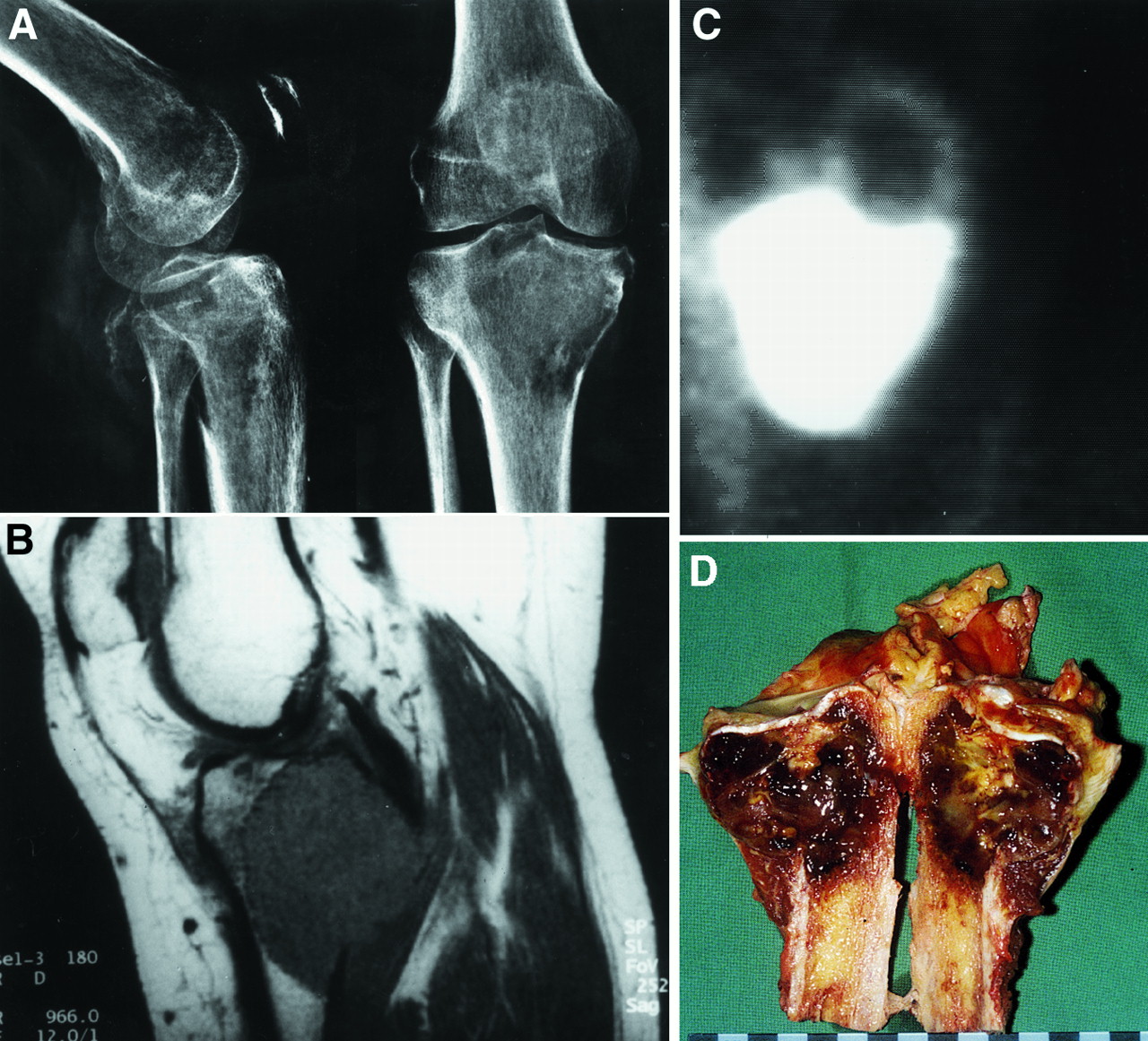
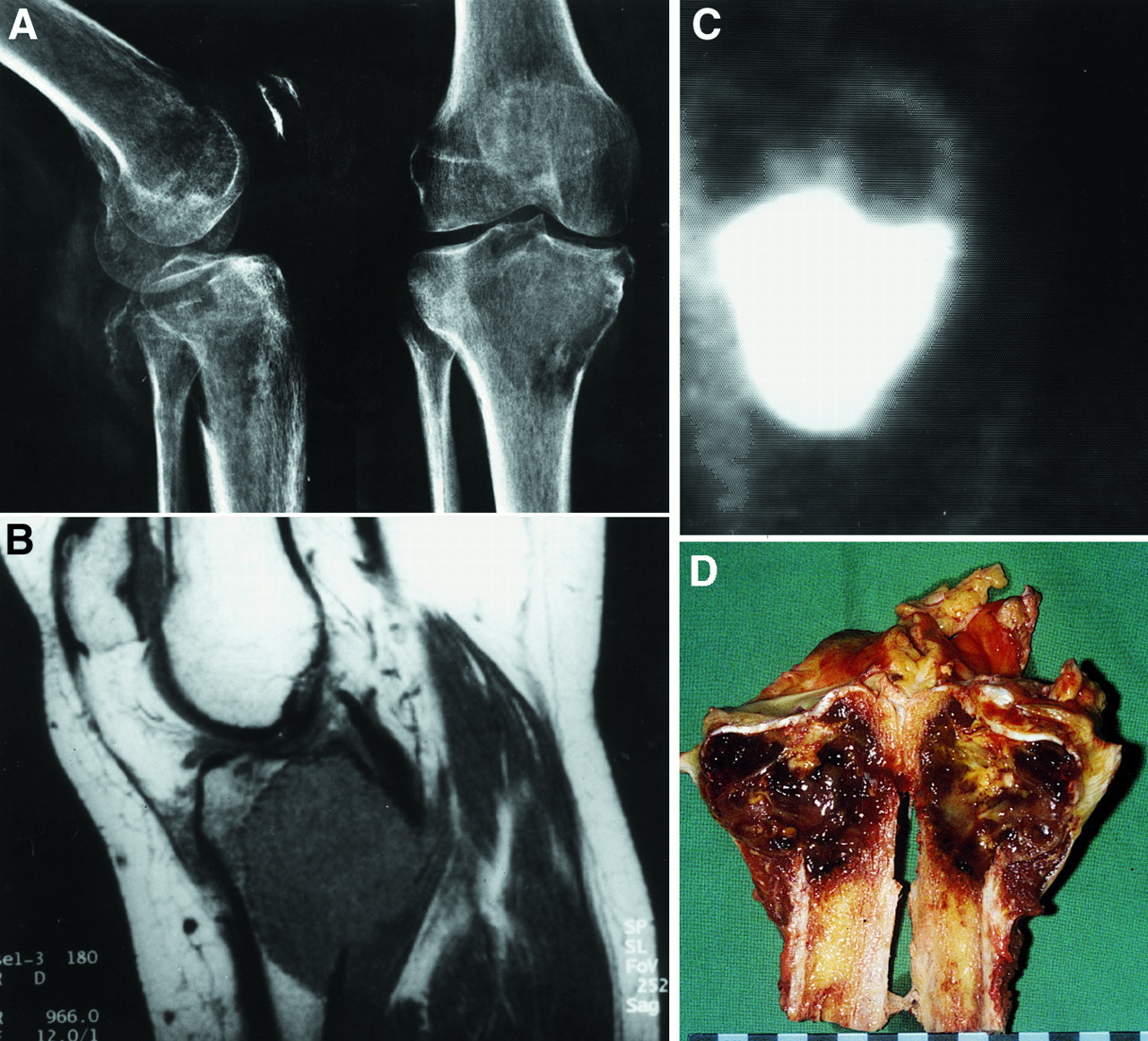
A 32-y-old woman with stage 3 giant cell tumor of tibial head. (A) Radiograph shows radiolucent, ill-defined lesion located eccentrically in epiphysis and adjacent metaphyseal region with destruction of dorsomedial cortex. (B) MR image shows homogeneous uptake of gadolinium–diethylenetriaminepentaacetic acid within lesion and tumoral infiltration of popliteus muscle. (C) PET image shows highly hypermetabolic lesion suggestive of malignant tumor (T/B, 35.0). (D) Gross specimen shows subchondral extension, cortical destruction, and typical hemorrhagic aspect of giant cell tumor.
Because PET offered better spatial resolution than did conventional bone scanning, the topographic information provided could contribute to the differential diagnosis in several cases. For example, in a patient with a low-grade periosteal osteosarcoma, which characteristically does not affect the medullary cavity, PET clearly showed a high FDG accumulation around the diaphyseal cortex and inconspicuous uptake within the medullary cavity (Fig. 3).
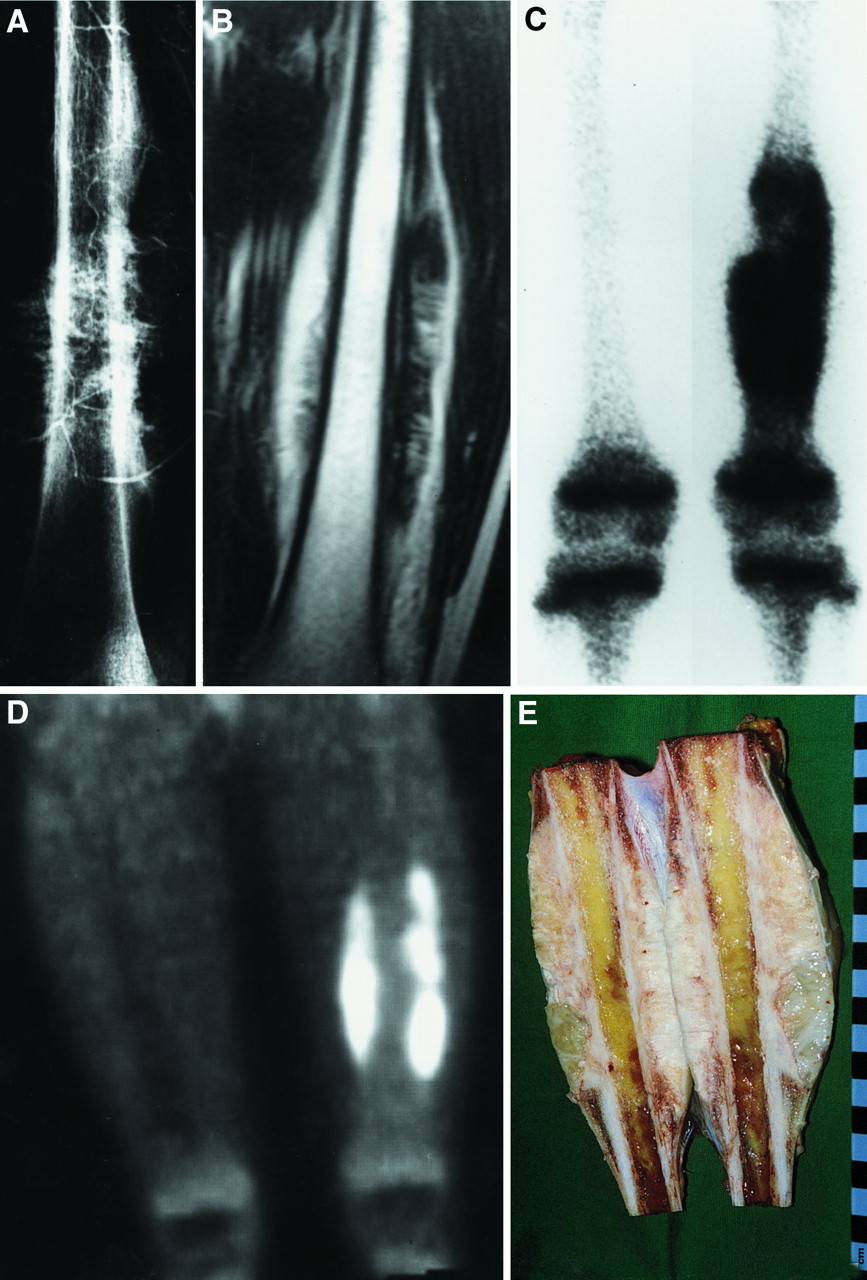
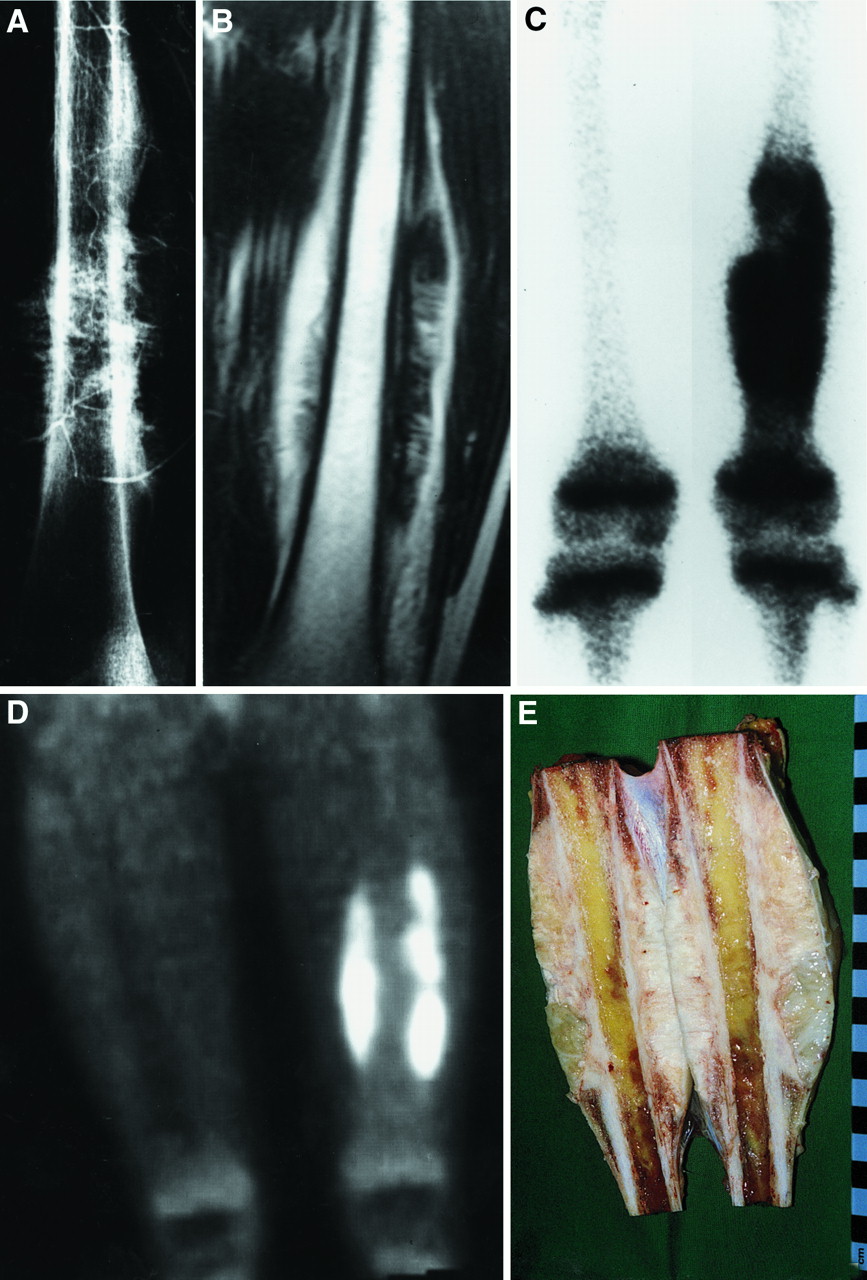
A 10-y-old girl with low-grade periosteal osteosarcoma of femur. (A) Angiogram shows moderate vascularization, saucerization of adjacent cortex, and radiating spicules. (B) MR image shows tumor located at external surface of bone without involvement of marrow cavity. (C) Bone scintigram shows hypermetabolic diaphyseal lesion without anatomic details. (D) PET image shows that tumor is surrounding femur (T/B, 6.1) and that medullary cavity is without elevated uptake, enabling definitive exclusion of classic central osteosarcoma. (E) Gross specimen shows lesion limited to external surface of bone, without medullary penetration.
DISCUSSION
Established imaging modalities for distinguishing benign from malignant skeletal lesions comprise conventional radiography, 3-phase bone scintigraphy, CT, and contrast-enhanced dynamic MRI (21). Although conventional radiography remains the mainstay in the evaluation of any bone lesion and allows reliable assessment of lesion aggressiveness, this imaging method often does not permit a determination of whether a lesion is malignant; on radiographs, some malignant lesions appear nonaggressive and some benign lesions appear highly aggressive. Bone scintigraphy is highly sensitive for detecting intraosseous lesions but generally does not enable discrimination between benign and malignant causes of increased uptake of radiopharmaceutical (22). The principal role of bone scintigraphy in evaluating osseous lesions is determining whether the process is monostotic or polyostotic or, less frequently, whether a tumor is aggressive or nonaggressive (22). Evaluation of the arterial blood supply of an osseous lesion using the first phase of the bone scan suggests the aggressiveness and prognosis of the lesion, whereas an increase in 99mTc-phophate compounds seen on delayed bone scans is a nonspecific finding (23). Methylene diphosphonate reflects osteoblastic activity in the bone tissue surrounding the tumor, whereas the accumulation of FDG is associated with the metabolic activity of the tumor itself (24). The high specificity of PET, compared with bone scintigraphy, improves estimates of biologic behavior and enables a more precise assessment of tumor topography. CT and MRI reveal excellent anatomic detail for primary bone tumors and allow accurate preoperative local staging. In addition, these techniques permit assessment of the intramedullary extent of the disease and soft-tissue involvement, particularly the relationship between the tumor mass and major neurovascular structures (25). Additionally, dynamic MRI enhanced by gadolinium–diethylenetriaminepentaacetic acid (DTPA) provides information about the grading of primary bone tumors, with a degree of overlap between benign and malignant tumors (26). In general, the ability of CT and MRI to distinguish between certain benign and malignant osseous lesions is limited (27).
In planning surgical strategy, one has to consider not only the grade of malignancy but also local aggressiveness, which may occur both in malignant and in benign lesions. Therefore, we primarily attempted to evaluate the biologic activity of osseous tumors and tumorlike lesions using FDG PET. The parameters for quantification of FDG uptake are standardized uptake values and T/Bs. For practicability and independence of transmission scanning, we used T/Bs instead of standardized uptake values. Studies on grading soft-tissue tumors (7) and predicting the response of osteosarcomas to neoadjuvant chemotherapy (13) have shown that the exclusive use of T/Bs estimates the biologic activity of skeletal lesions with great accuracy.
Sarcomas and aggressive benign tumors, both of which require resection with wide surgical margins, showed a markedly elevated glucose metabolism compared with latent and active benign lesions. Therefore, preoperative analysis of glucose metabolism can help in choosing the best surgical procedure for benign tumors with inconclusive radiologic findings. In the identification of skeletal lesions for which curative treatment requires wide surgical excision, analysis of glucose metabolism can improve the diagnostic value of FDG PET with a sensitivity of 93.7% (CI, 86%–98%), a specificity of 76.3% (CI, 65%–85%), an accuracy of 87.1% (CI, 82%–91%), and a positive predictive value of 86.8% (CI, 80%–91%).
Grading mesenchymal skeletal lesions using FDG PET can be helpful for equivocal tumors, particularly lesions for which a discrepancy exists between histopathologic diagnosis and clinical findings. If, in a lesion described as harmless by the pathologist, FDG uptake is high, a bone tumor specialist should reevaluate the biopsy specimen, or—if the biopsy specimen is considered nonrepresentative—a second biopsy should be obtained. Alternatively, the tumor may be resected with extended surgical margins, if such a resection is possible without major risks or functional loss. If FDG uptake is low in a lesion histologically characterized as malignant, the specimen should be reevaluated carefully, especially if mutilating surgical procedures or chemotherapy is intended. In our study, all high-grade sarcomas, lymphomas, and bone metastases were detected as malignant lesions by markedly increased glucose metabolism.
The limitations of FDG PET in discriminating between certain malignant and benign primary bone tumors are obvious: FDG PET failed to reveal malignancy in 6 cases of low-grade chondrosarcoma, whereas the specificity for malignant cartilaginous tumors is high. In a patient with Ollier's disease, multiple chondromas of the long bones showed the same moderately increased glucose metabolism (maximal T/B, 2.7) as did a histologically confirmed malignant transformation of a subtrochanteric lesion into a low-grade chondrosarcoma (T/B, 2.6) in the same patient. Several active or aggressive stage 2 or 3 benign lesions, such as giant cell tumors and some aneurysmatic bone cysts, could not be distinguished from malignant tumors using FDG PET. Interestingly, dynamic gadolinium-DTPA–enhanced MRI of aggressive benign bone tumors such as giant cell tumors, for which histologic evaluation of biologic behavior is difficult even for experienced pathologists, showed a pattern of increased signal intensity similar to that of malignant tumors (26). Nevertheless, in a case of telangiectatic osteosarcoma, PET revealed a higher FDG uptake (T/B, 6.6) for the malignancy than for aneurysmatic bone cysts (maximal T/B, 5.9). However, why skeletal lesions with moderate biologic activity, such as fibrous dysplasia or osteofibrous dysplasia, appear strongly hypermetabolic remains unclear. Malignant transformation is known to occur in approximately 1% of fibrous dysplasia cases (1,2). We observed a patient with rhabdomyosarcoma of the innominate bone that disclosed a markedly increased FDG uptake (T/B, 15.9). Some years ago, this patient underwent several surgeries because of histologically proven fibrous dysplasia at the same location.
A general problem with FDG PET in tumor diagnosis is the known accumulation of the glucose analog FDG not only in tumor cells but also in macrophages and granulation tissues (28) and in inflammation, such as osteomyelitis (5,29). We observed 3 false-positive results caused by inflammatory processes.
CONCLUSION
PET is valuable for assessing osseous lesions in several situations. If the character of an asymptomatic bone lesion as shown on standard radiographs is questionable, the level of metabolic activity can be used to decide whether a histologic evaluation is required, particularly if biopsy would be difficult, as for the pelvis. PET also is useful in cases of discrepancy between the histologic diagnosis and the imaging or clinical data. Finally, the high sensitivity of PET in detecting malignant skeletal primary tumors implies that it would be useful for diagnosing skip lesions as well as occult skeletal, lung, and visceral metastases. This aspect of tumor staging deserves further evaluation.
Acknowledgments
This study was presented in part at the international annual meeting of the German Society of Nuclear Medicine, Leipzig, Germany, April 1–4, 1998.
Footnotes
Received May 24, 1999; revision accepted Aug. 31, 1999.
For correspondence or reprints contact: Michael Schulte, MD, Department of Trauma, Hand and Reconstructive Surgery, Steinhövelstr. 9, D 89075 Ulm, Germany.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- False-Positive Positron Emission Tomography in Patients With History of Malignancy
- Correlation Between Glycolytic Phenotype and Tumor Grade in Soft-Tissue Sarcomas by 18F-FDG PET
- NCCN Task Force: Clinical Utility of PET in a Variety of Tumor Types
- Imaging Bone and Soft Tissue Tumors with the Proliferation Marker [18F]Fluorodeoxythymidine
- PET for Sarcomas Other Than Gastrointestinal Stromal Tumors
- Imaging of Bone Sarcomas
- Diagnostic Value and Limitations of Fluorine-18 Fluorodeoxyglucose Positron Emission Tomography for Cartilaginous Tumors of Bone
- PET Imaging of Osteosarcoma
- Whole-Body 18F-FDG PET Identifies High-Risk Myeloma
- Prognostic Significance of 18F-FDG and 99mTc-Methylene Diphosphonate Uptake in Primary Osteosarcoma
- The Role of Quantitative 18F-FDG PET Studies for the Differentiation of Malignant and Benign Bone Lesions
- Is There a Role for FDG PET in the Diagnosis of Musculoskeletal Neoplasms?