


Abstract
Cardiac MR imaging has made major inroads in the new millennium in the diagnosis and assessment of prognosis for patients with cardiomyopathies. Imaging of left and right ventricular structure and function and tissue characterization with late gadolinium enhancement (LGE) as well as T1 and T2 mapping enable accurate diagnosis of the underlying etiology. In the setting of coronary artery disease, either transmurality of LGE or contractile reserve in response to dobutamine can assess the likelihood of recovery of function after revascularization. The presence of scar reduces the likelihood of a response to medical therapy and to cardiac resynchronization therapy in heart failure. The presence and extent of LGE relate to overall cardiovascular outcome in cardiomyopathies. A major role for cardiac MR imaging in cardiomyopathies is to identify myocardial scar for diagnostic and prognostic purposes.
- cardiac MR imaging
- coronary artery disease
- late gadolinium enhancement
- ischemic cardiomyopathy
- nonischemic cardiomyopathy
- infiltrative cardiomyopathy
Cardiac MR imaging (CMR) is considered the gold standard for measurement of the structure and function of the left ventricle (LV) and the right ventricle (RV). Cine imaging is used to cover the LV in the short axis from the apex to the base, essentially creating a 3-dimensional volumetric structure for analysis. In the 1990s, gradient-echo cine imaging was the standard, but this technique was replaced at the turn of the millennium by steady-state free-precession cine imaging, which offers a higher contrast-to-noise ratio between the dark myocardium and the bright blood pool (1). Multiple studies have demonstrated the accuracy and reproducibility of CMR for measuring LV volumes, ejection fraction (EF), and regional function (2). Measurements made with this 3-dimensional dataset do not require geometric assumptions and are therefore less prone to error than 2-dimensional methods, such as 2-dimensional echocardiography, in ventricles deformed by myocardial infarction or cardiomyopathies. Interstudy and interscan reproducibility is high, allowing for reduced sample sizes in clinical trials of heart failure (3,4). Techniques such as myocardial tissue tagging (5) or cine displacement–encoded stimulated-echo imaging (6) allow more detailed analysis of regional myocardial motion and deformation than cine imaging and have been applied to studies of myocardial infarction (7) and hypertrophic cardiomyopathy (HCM) (8).
Late gadolinium enhancement (LGE) refers to the discrimination of regions of scar, necrosis, or inflammation from normal tissue by the prolonged retention of gadolinium-based contrast agents. Since the mid-1980s, investigators have appreciated T1 shortening (increased enhancement) in regions of infarction after gadolinium administration (9–11). However, these early imaging techniques were limited by long acquisition times, artifacts, and insufficient contrast between normal and abnormal regions. With faster approaches and the implementation of an inversion recovery pulse sequence with the inversion time set to null normal myocardium, the signal difference between normal and infarcted segments has been increased by 500%–1,000% (12). Using this approach, Kim et al. demonstrated that the spatial extent of LGE seen on CMR closely mirrored the distribution of myocyte necrosis in the early period after infarction and that of collagenous scar at 8 wk (R = 0.97, P < 0.001) (13), whereas in regions of the heart subjected to reversible injury, the retention of contrast did not occur (Fig. 1) (14). LGE accurately delineates infarction, as defined by histology, at various time points after injury (15). LGE is not unique to infarct scar and can demonstrate any cause of fibrosis or infiltration in cardiomyopathies.

Three-chamber long-axis phase-sensitive inversion recovery LGE image in patient with heart failure and CAD. Transmural LGE can be seen in inferolateral wall (arrow).
T2-weighted imaging can be used to demonstrate myocardial edema or injury. An understanding of the time course of edema is key to the accurate interpretation of T2-weighted imaging. Using a canine model of myocardial infarction, Abdel-Aty et al. noted that the onset of edema on CMR first became apparent 28 ± 4 min after experimental coronary artery occlusion and well before the appearance of LGE or troponin elevation, signifying that CMR can visualize edema before the onset of irreversible myocardial injury (Fig. 2) (16). Microsphere analysis in a canine model of reperfusion after acute myocardial infarction suggested that T2-weighted imaging performed 2 d after myocardial infarction can be used to delineate the area at risk (17). Increased T2 signal intensity can be seen in any cause of myocardial injury, such as acute myocarditis (18). Older T2-weighted imaging approaches were prone to artifacts; more recently, T2 mapping has been used with CMR protocols to overcome these limitations (19).

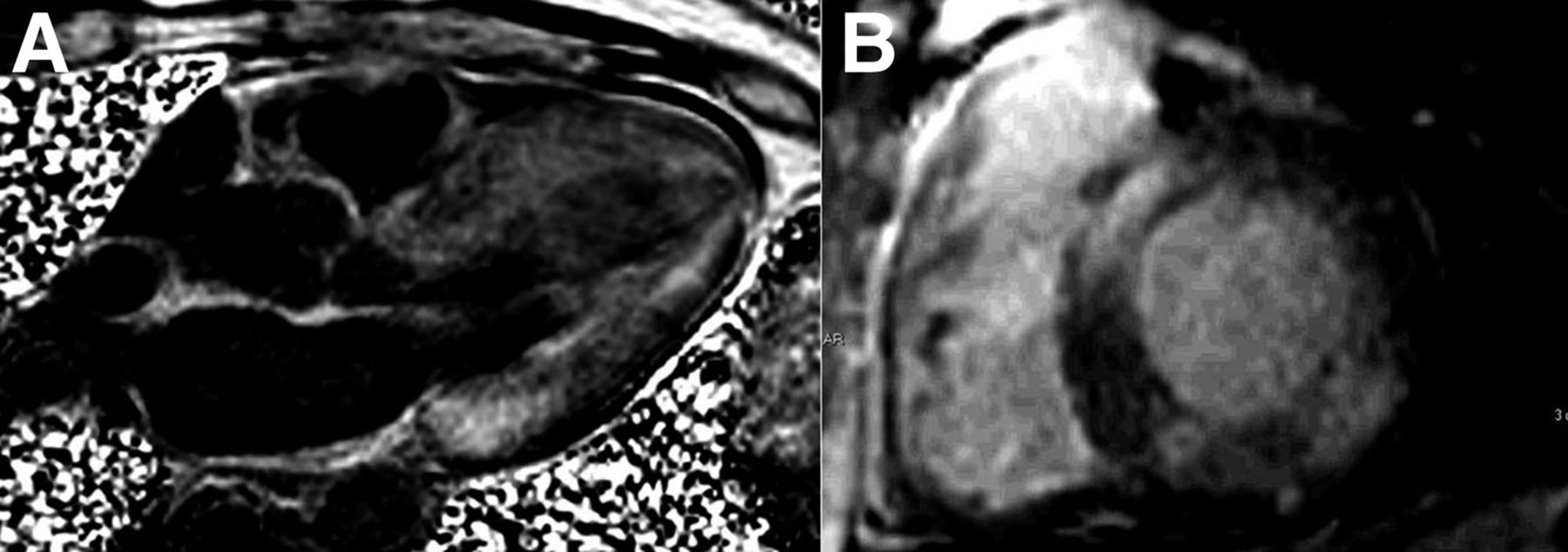
(A) Three-chamber long-axis bright-blood T2-weighted image in patient with spontaneous left anterior descending artery dissection. Bright signal in anterior wall is consistent with edema. (B) Three-chamber long-axis phase-sensitive inversion recovery LGE image in same patient. Absence of LGE in anterior wall but evidence of prior 50% transmural infarct in mid–inferior wall can be seen. Together, these images demonstrate evidence of myocardial stunning without infarction in anterior wall.
T1 of the myocardium can be measured by mapping with a modified Look–Locker inversion recovery sequence (20) and shorter versions of this approach (21). Native or precontrast T1 can be measured before contrast infusion, and then postcontrast T1 measures can be used to calculate the extracellular volume fraction in the myocardium (22). These techniques are being applied to help in the differential diagnosis of cardiomyopathies, as some have characteristically high native T1 values as well as high extracellular volume fractions. Native T1 is especially useful in patients with concomitant renal disease, as patients with stage 4 or 5 chronic kidney disease are not candidates for receiving gadolinium because of concerns about nephrogenic systemic fibrosis.
ESTABLISHING ETIOLOGY OF CARDIOMYOPATHY
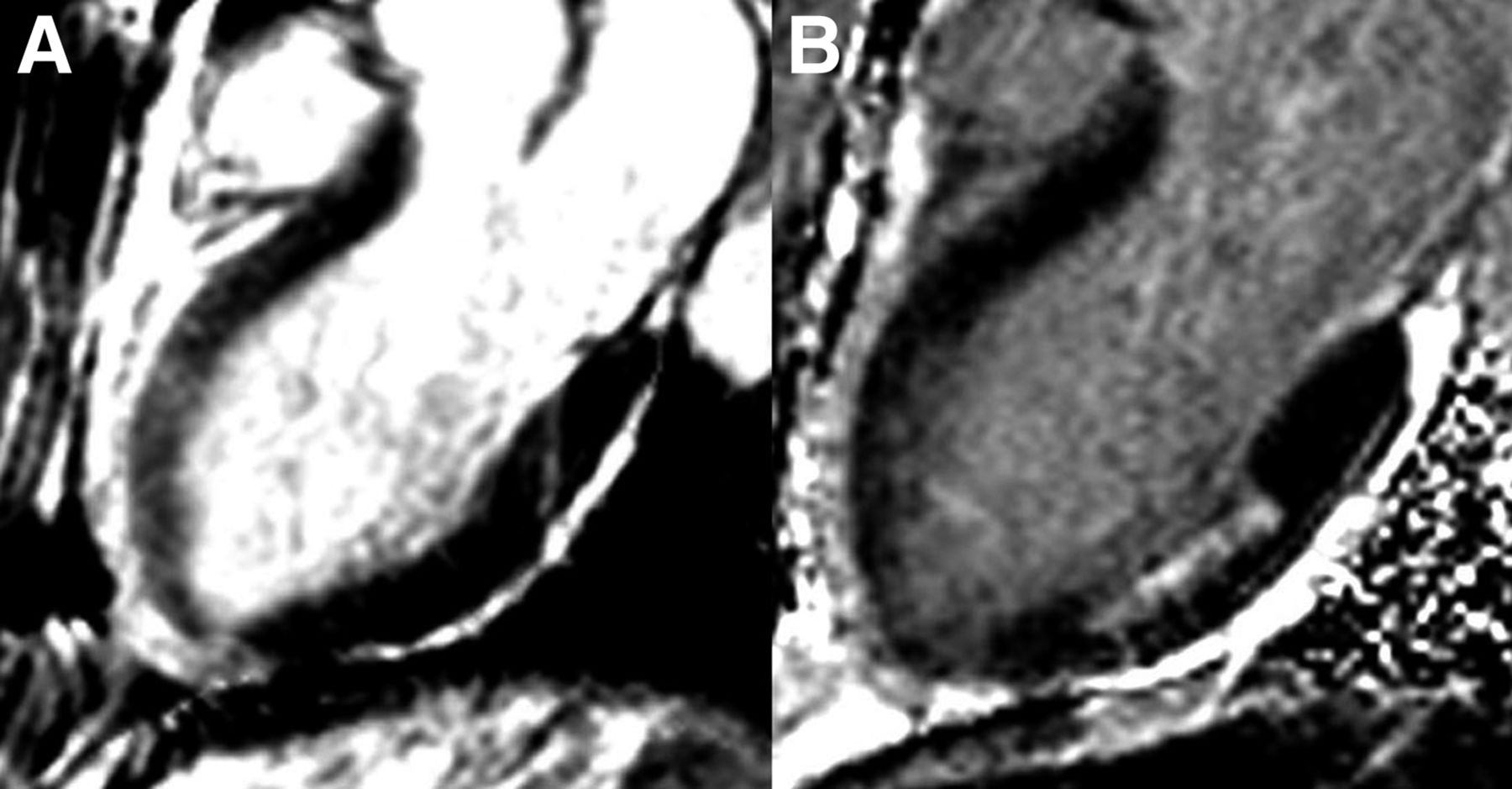
The first step in the evaluation of the patient with new-onset heart failure is to evaluate the underlying etiology and, importantly, to exclude ischemic heart disease as a potentially reversible cause. The presence of LGE in a coronary distribution can support the diagnosis of underlying coronary artery disease (CAD), but its absence does not rule it out, as patients with extensive hibernating myocardium may have no LGE (Fig. 3) (23). In a study by Soriano et al. of 71 patients with new-onset heart failure and systolic dysfunction, the sensitivity of the infarct pattern of LGE for ischemic cardiomyopathy—as defined by the presence of obstructive CAD—was 81%, whereas the specificity was 91% (23). Patients without obstructive CAD may have evidence of LGE in an infarct pattern due to thrombotic occlusion of a nonobstructed artery, embolization, or spontaneous coronary dissection and thereby may be misclassified. This finding was noted in 13% of 63 patients who had the diagnosis of dilated cardiomyopathy (DCM) with chronic heart failure (24). CT coronary angiography may be an excellent way of noninvasively ruling CAD in or out in the setting of new- or recent-onset heart failure, as shown in a study with a combination of CT coronary angiography and LGE determined by CMR as a gold standard for establishing the underlying etiology (25).

(A) Four-chamber long-axis phase-sensitive inversion recovery LGE image in patient with heart failure and EF of 20%. No LGE can be seen. (B) Two-chamber long-axis phase-sensitive inversion recovery LGE image in same patient. No LGE can be seen. (C) Right anterior oblique CT angiogram demonstrating 3-vessel CAD with occluded left circumflex artery, occluded right coronary artery that fills through collateral vessels, and significant left anterior descending artery disease. Thus, this patient had severe LV dysfunction in setting of 3-vessel CAD without LGE, signifying extensive hibernating myocardium.
ISCHEMIC CARDIOMYOPATHY
In addition to identifying CAD as the underlying etiology, CMR can define appropriate therapy as well. A response to β blockade can be predicted by the presence and extent of LGE. Bello et al. demonstrated an inverse relationship between the extent of LGE and the likelihood of contractile improvement with 6 mo of β blockade (26). Fifty-six percent of segments with no scar demonstrated improved function, whereas only 3% of segments with greater than 75% transmural scar demonstrated improvement (26).
CMR plays an important role in the assessment of myocardial viability for the selection of patients for revascularization. An LV wall thickness of less than 5.5 mm at the end of diastole on rest cine CMR is generally considered a marker of nonviable myocardium (27). One study, however, demonstrated that in a minority of patients who had wall thinning without a substantial LGE burden (4% of 1,055 patients with CAD), contractile recovery could occur after revascularization (28). Nontransmural infarcts typically do not result in severe end-diastolic wall thinning. The extent of LGE is a useful marker of the likelihood of functional recovery with revascularization. In a landmark study, Kim et al. studied 50 patients who had LV dysfunction and were evaluated with contrast-enhanced CMR before surgical or percutaneous revascularization (29). LGE was noted in 80% of the patients. There was an inverse relationship between the transmural extent of LGE and functional recovery with revascularization (Fig. 4). Segments with greater than 50% transmural LGE were nonviable, whereas segments with no LGE had an approximately 80% likelihood of functional recovery. Similar findings were noted in a study of 52 patients undergoing coronary artery bypass surgery; in that study, 36% of segments developed new areas of LGE after surgery (30).

Inverse relationship between transmurality of LGE on x-axis and likelihood of improved function after revascularization. (Adapted with permission of (29).)
Cine imaging of long- and short-axis views of the LV after the administration of low-dose dobutamine (10 μg/kg/min) can be used to assess contractile reserve and to predict areas of functional recovery with revascularization (27,31). Bove et al. studied patients before and after coronary artery bypass surgery and divided segments into those with no LGE and those with 1%–25%, 26%–50%, or greater than 50% transmural LGE (31). Dysfunctional segments were defined as those having wall thickening of less than 27% (2 SDs less than normal myocardium). After revascularization with coronary artery bypass surgery, the improvement in wall thickening in segments with 1%–50% transmural enhancement was 22% ± 4% for dobutamine-responsive segments; this improvement was significantly higher than that for non–dobutamine-responsive segments (9% ± 4%). These findings suggested that contractile reserve was more predictive of functional recovery than infarct transmurality in infarcts with 1%–50% transmural LGE. In a complementary study, 29 patients with ischemic cardiomyopathy and a severely reduced EF underwent both LGE and low-dose dobutamine cine imaging (32). On the basis of the area under the receiver operating characteristic curve, contractile reserve with low-dose dobutamine was superior to the presence of LGE in predicting the recovery of LV function, especially when myocardial segments had less than 75% transmural LGE. A recent metaanalysis of 24 studies involving 698 patients suggested that although LGE provided the highest sensitivity and negative predictive value (95% and 90%, respectively) for predicting functional recovery after revascularization, low-dose dobutamine cine imaging offered the highest specificity and positive predictive value (91% and 93%, respectively) (33).
Cardiac resynchronization therapy (CRT) with biventricular pacing has emerged as an important part of the therapeutic armamentarium for heart failure. Several studies have demonstrated that scar in the posterolateral wall is associated with a lower rate of response to CRT because the LV lead is usually placed in the lateral cardiac veins and may not appropriately capture scarred myocardium. Bleeker et al. demonstrated that, among 14 of 50 patients with greater than 50% transmural posterolateral scar, only 2 (14%) responded to CRT, whereas 81% of the remainder responded (34). Another study, involving 23 patients, showed that LV scarring of greater than 15% had a sensitivity of 85% and a specificity of 90% for indicating a response to CRT (35). Bilchick et al. studied 75 patients and demonstrated that the absence of posterolateral scar was an important predictor of a response to CRT, in addition to dyssynchrony markers determined by CMR (36).
The presence and amount of LGE are important for prognosis in the setting of CAD. Kwong et al. studied 195 patients and found that the presence of any LGE was associated with a hazard ratio of 8.3 for a major adverse cardiac event and a hazard ratio of 10.9 for cardiac mortality (37). In another study, in which 857 patients were monitored for an average of 4.4 y, a scar index based on LGE was an independent predictor of all-cause mortality or cardiac transplantation, in addition to other, well-known risk factors, including EF and age (38).
NONISCHEMIC CARDIOMYOPATHIES
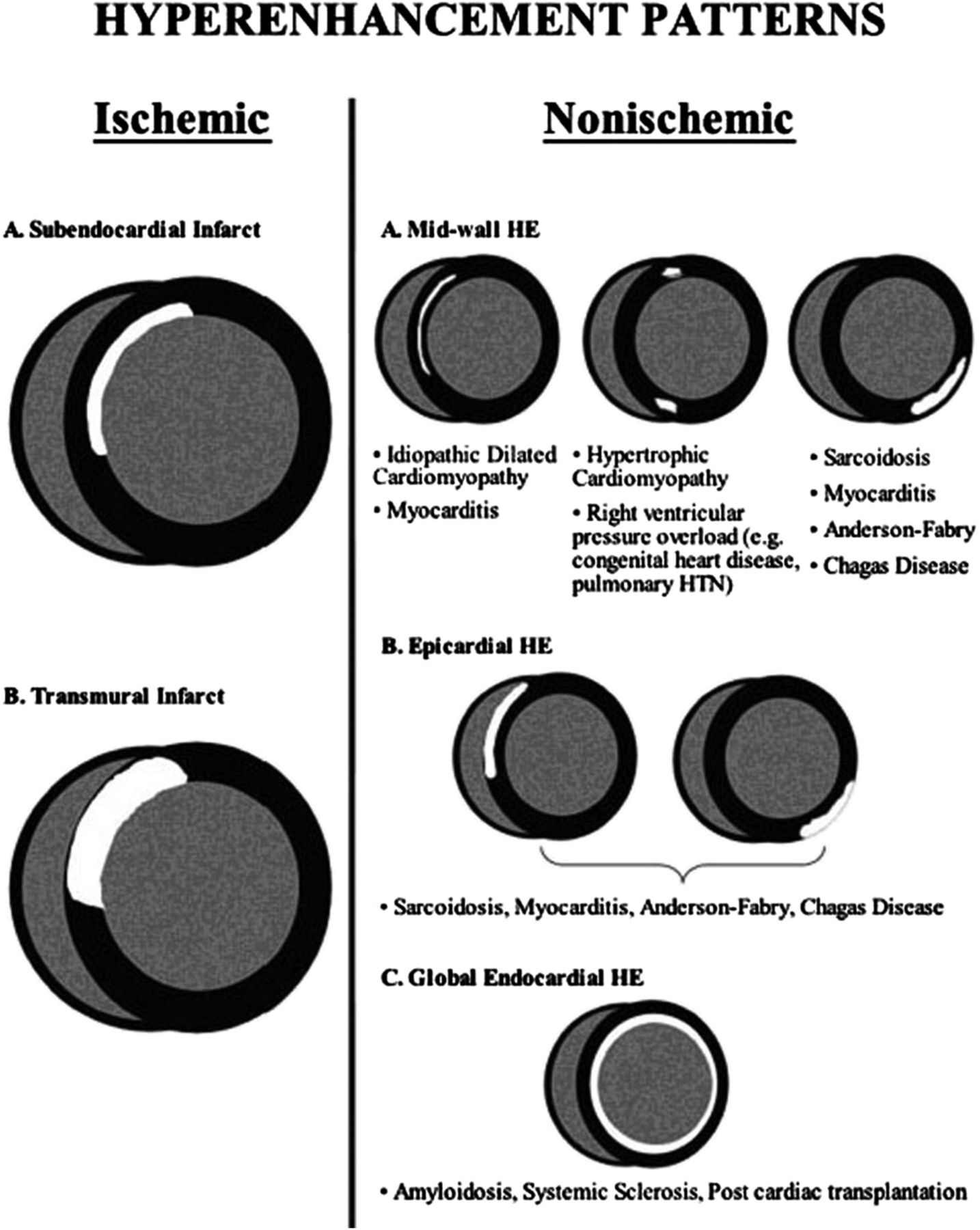
Tissue characterization by CMR is quite useful for differentiating the etiologies of nonischemic cardiomyopathies (Fig. 5). LGE can differentiate infiltrative cardiomyopathies (39), and T1 mapping can identify certain hypertrophic and infiltrative cardiomyopathies that have characteristically high native T1 values (40). The finding of LGE has prognostic implications for nonischemic cardiomyopathies as well as for ischemic cardiomyopathies. In a recent metaanalysis of 9 studies involving 1,488 patients who had nonischemic cardiomyopathy and were monitored for an average of 30 mo, the presence of LGE was noted in 38% of the patients and was associated with odds ratios of 3.3 for mortality and 5.3 for sudden cardiac death (SCD) or aborted SCD (41).

Patterns of LGE seen in ischemic and nonischemic cardiomyopathies. HE = hyperenhancement of LGE; HTN = hypertension. (Reprinted with permission of (75).)
Dilated Cardiomyopathy
Most patients who have heart failure without obstructive CAD have no evidence of LGE (24). A minority of patients (13%) have LGE in an infarct pattern and may be misclassified as having nonischemic cardiomyopathy (24). Approximately one-fourth of patients with DCM have evidence of midwall fibrosis (Fig. 6) (24). This likely represents the chronic healing phase of myocarditis. In a study of 472 patients who had DCM and were monitored for 5.3 y, 142 patients with midwall fibrosis had hazard ratios of 3.0 for all-cause mortality and 5.2 for a composite endpoint of SCD and aborted SCD (42). A study of 65 patients who had dilated nonischemic cardiomyopathy with an EF of less than or equal to 35% showed that the presence of LGE was associated with an 8-fold increase in heart failure, appropriate implanted cardiac device (ICD) firing, and cardiac death (43). The presence of midwall fibrosis is also an independent predictor of mortality and morbidity of patients who have DCM and are undergoing CRT (44). In fact, in that study of 97 patients with DCM and 161 patients with ischemic cardiomyopathy, the patients who had DCM with midwall fibrosis had outcomes similar to those of the patients with ischemic disease (44). Thus, as with ischemic cardiomyopathy, the presence of fibrosis or scar is a marker of an adverse outcome and a poorer response to device therapy.
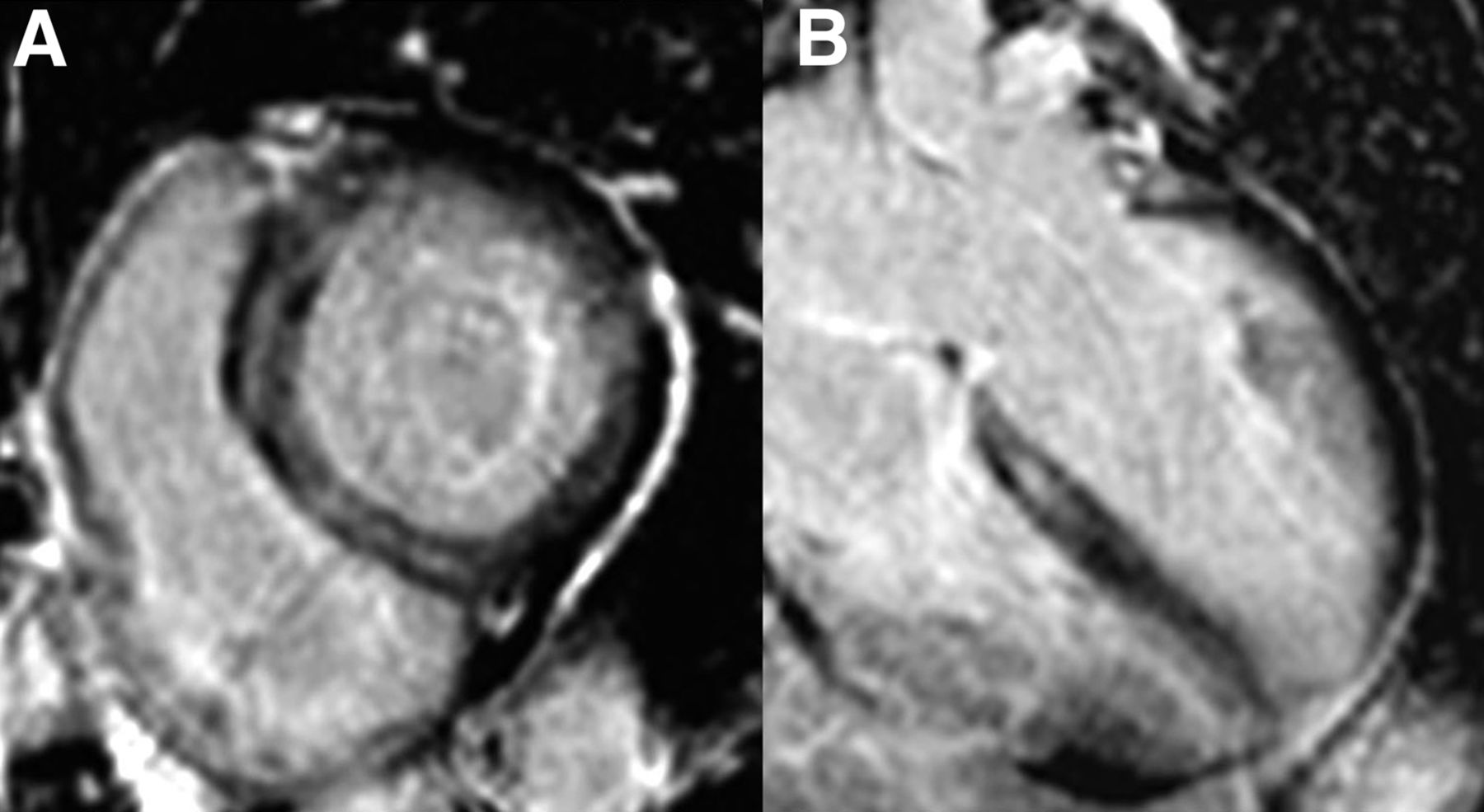
(A) Basal short-axis phase-sensitive inversion recovery LGE image in patient with heart failure, global LV systolic dysfunction, and EF of 25%. Midwall stripe of LGE can be seen in septum. (B) Four-chamber long-axis phase-sensitive inversion recovery LGE image in same patient, again showing midseptal stripe of LGE.
Myocarditis
A typical patient with acute myocarditis has chest pain, troponin elevation, and normal coronary arteries. The finding of LGE in the midwall and subepicardium of the LV is characteristic of viral myocarditis and has been validated against histology (45). Older studies suggested that early postcontrast T1-weighted enhancement of the myocardium could be a marker of inflammation in myocarditis (46). In addition, T2-weighted imaging demonstrating myocardial edema can be a diagnostic sign. The Lake Louise Consortium in 2009 suggested that basing diagnosis on positive results from 2 of 3 techniques (early enhancement ratio, LGE, or increased T2 signal) may be an ideal approach (47).
However, the early enhancement ratio has lost favor because of a lack of reproducibility, and T2-weighted imaging has been replaced by more quantitative T2 mapping. In addition, T1 mapping, both native and with contrast for measurement of the extracellular volume, is also being used for diagnosis. Ferreira et al. studied 50 patients with suspected acute myocarditis and 45 age-matched controls and showed that the patients had higher T2 signal intensity ratios and native myocardial T1 values than the controls (48). In fact, a T1 cutoff of 990 ms at 1.5 T demonstrated sensitivity, specificity, and diagnostic accuracy of 90%, 91%, and 91%, respectively. A combination of these techniques may be the best way to accurately identify acute myocarditis. In a recent study of 104 patients and 21 controls, a stepwise approach involving LGE and a myocardial extracellular volume of greater than 27% showed an overall accuracy of 90% (49). In another study, involving 61 patients with acute myocarditis and 67 patients with chronic myocarditis, the diagnostic accuracies for acute myocarditis were 99% for native T1, 86% for LGE alone, and 72% for increased T2 signal (50). For chronic myocarditis, LGE alone performed better than T1 mapping (94% vs. 84% accuracies), but the combination of the 2 techniques performed even better, with a 98% overall accuracy.
HCM
Approximately two-thirds of patients with HCM may have LGE with a characteristic pattern of patchy involvement, particularly at RV septal insertion sites and in walls with the greatest hypertrophy. Several studies have examined the relationship between the presence of LGE and outcome in patients with HCM. Two recent studies, although underpowered, showed that LGE was associated with an increased risk of cardiovascular events. Bruder et al. monitored 243 patients with HCM for 3 y for all-cause mortality and cardiac mortality (51). LGE was seen in 67% of the patients, and the presence of LGE was associated with odds ratios of 5.5 for all-cause mortality and 8.0 for cardiac mortality. O’Hanlon et al. monitored 217 patients for 3 y for a composite endpoint including cardiovascular death, unplanned cardiovascular admission, sustained ventricular tachycardia or ventricular fibrillation, or appropriate ICD discharge (52). Sixty-three percent of the patients had LGE, and the presence of LGE was associated with an odds ratio of 3.4 for the primary endpoint. A metaanalysis of data pooled from 1,063 patients monitored for an average of 3.1 y in 4 studies, including the latter 2, demonstrated that the presence of LGE was associated with odds ratios of 2.9 for cardiac death, 5.7 for heart failure death, and 4.5 for all-cause mortality but only a trend for SCD (53). These studies treated LGE in a binary fashion, but it is likely that the extent of LGE adds discriminatory value.
A recent study of 1,293 patients monitored for 3.3 y showed that LGE of greater than or equal to 15% of the LV mass was associated with a 2-fold increase in SCD event risk (54). In addition to the amount, the location or pattern of LGE may be more predictive of adverse outcome than the presence of LGE alone. The ongoing National Institutes of Health–funded natural history study, “HCMR: Novel Predictors of Prognosis in Hypertrophic Cardiomyopathy” (NCT01915615), involving CMR, genetics, and biomarker evaluation of 2,750 patients with HCM, is likely to offer further insight in this regard.
Amyloidosis
In addition to the classic findings of thick LV walls, valves, and interatrial septum and the presence of a pericardial effusion in cardiac amyloidosis, the existence of amyloid protein in the myocardial interstitium is associated with characteristic patterns of LGE due to abnormal gadolinium kinetics in the infiltrated myocardium (55). Validation against endomyocardial biopsy was performed in 33 patients with diastolic dysfunction and features suggesting the presence of amyloid protein (56), and the pattern of circumferential subendocardial LGE had a sensitivity of 80% and a specificity of 94% (Fig. 7). When the volume of distribution of gadolinium was quantified with serial measures of T1 in the myocardium after gadolinium contrast infusion, it was found to be markedly larger than that in healthy controls (57). In addition, the “native” T1 of the myocardium was significantly longer in patients with amyloidosis than in controls (57) or in patients with left ventricular hypertrophy due to aortic stenosis (58).
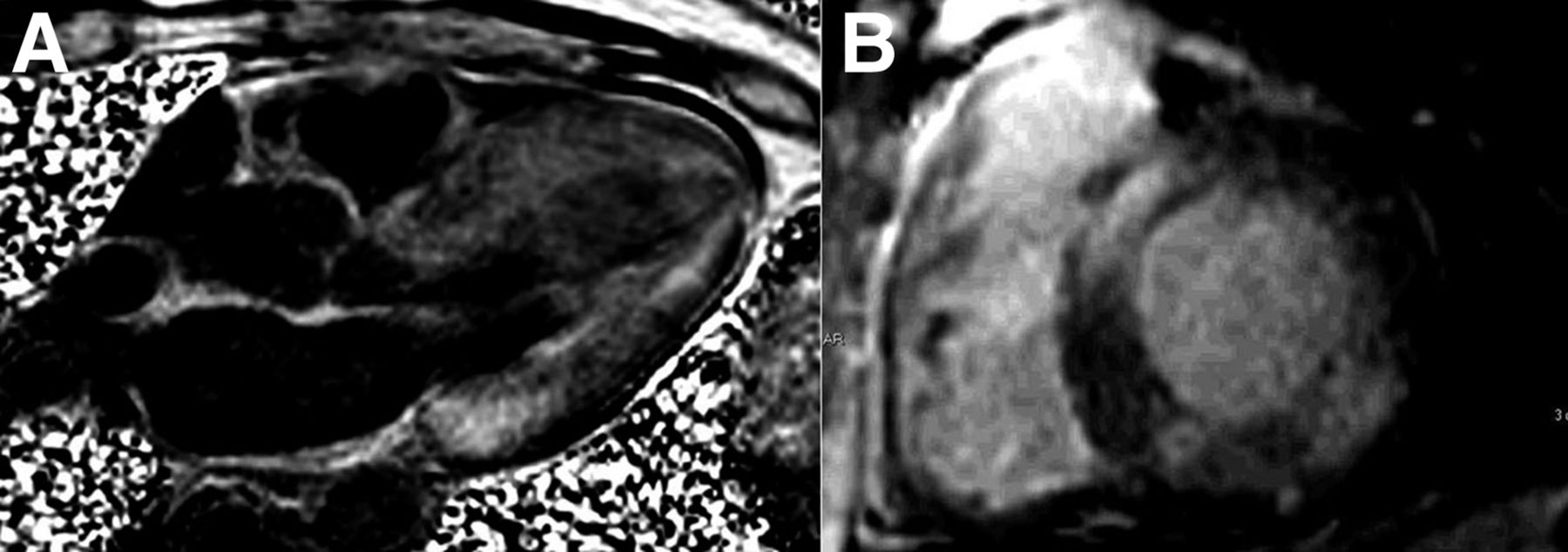
(A) Four-chamber long-axis phase-sensitive inversion recovery LGE image in patient with heart failure and EF of 30%. Diffuse subendocardial LGE and signal nulling in blood pool, all characteristic of amyloidosis (most likely ATTR variety), can be seen. (B) Basal short-axis phase-sensitive inversion recovery LGE image in different patient with heart failure, global LV systolic dysfunction, and EF of 25%. In this patient, LGE is patchy and distribution is noncoronary—more consistent with AL amyloidosis—which was subsequently diagnosed by fat pad biopsy.
CMR is increasingly being used to discriminate light-chain (AL) amyloidosis from the transthyretin (ATTR) form of the disease. Fontana et al. studied native T1 mapping in 85 patients with ATTR disease, 79 patients with AL disease, 52 healthy subjects, and 46 patients with HCM (59). AL disease showed the highest native T1, followed by ATTR disease, although the areas under the receiver operating characteristic curves were similar for both forms of amyloidosis versus HCM (0.84). The potential utility of native T1 is critically important, as many patients with amyloidosis have concomitant renal dysfunction and are not candidates for receiving gadolinium because of concerns about nephrogenic systemic fibrosis. In another study, LGE findings in 46 patients with biopsy-proven AL amyloidosis and 51 patients with ATTR amyloidosis were compared (60). LGE was much more extensive in patients with ATTR amyloidosis, with 90% demonstrating transmural LGE, compared with only 37% of patients with AL amyloidosis. These investigators developed an LGE scoring system that differentiated the 2 types with 87% sensitivity and 96% specificity.
Sarcoidosis
CMR can readily identify characteristic features of cardiac sarcoidosis, including biventricular dilation and dysfunction. The pattern of LGE seen with cardiac sarcoid is variable; a classic pattern of midwall or epicardial LGE can be seen, but subendocardial or transmural enhancement in almost any distribution is also possible. A study of CMR involving 58 patients with biopsy-proven pulmonary sarcoid found 19 patients with evidence of LGE, mostly in the basal and lateral myocardium; this prevalence was higher than that identified by standard Japanese Ministry of Health guidelines (61). In another study, involving 81 patients who had extracardiac sarcoidosis and were monitored for an average of 21 mo, a 2-fold-higher rate of cardiac involvement was demonstrated by CMR than by Japanese Ministry of Health guidelines (62). Patients with LGE had a 9-fold-higher incidence of adverse events than those without LGE. In addition, T2 mapping may have a role in delineating the activity of sarcoidosis. In a study of 28 patients, regions of LGE showed decreased T2; this finding may have reflected an inactive phase of the disease (63).
Arrhythmogenic Right Ventricular Cardiomyopathy
CMR is the gold standard for the diagnosis of arrhythmogenic RV cardiomyopathy. Diagnostic findings in this disease include RV dilatation and global or regional dysfunction, including focal RV systolic bulging or aneurysm, and are carefully defined to meet Task Force criteria (64). In certain cases, LGE of the RV free wall can be identified (65), although it can be difficult to identify because of the thin RV wall in this disorder.
Noncompaction Cardiomyopathy
Noncompaction cardiomyopathy is defined on CMR as a ratio of noncompacted myocardium to compacted myocardium of 2.3 at the end of diastole (66). This ratio should be measured at a distance from the true apex. Newer definitions for a CMR diagnosis are frequently entertained (67), although the ratio of noncompacted myocardium to compacted myocardium of 2.3 remains the standard at present. Additional CMR findings in this disorder may include LV systolic dysfunction and LV thrombus.
Other Nonischemic Cardiomyopathies
CMR is also able to diagnose a variety of other nonischemic cardiomyopathies, including takotsubo cardiomyopathy, demonstrating myocardial edema without LGE (68); iron-overload cardiomyopathy (with T2* mapping) (69); Anderson–Fabry disease, with characteristic findings of basal and lateral LGE (70); and Chagas disease, with various LGE findings (71).
LIMITATIONS OF CMR IN CARDIOMYOPATHIES
There are several limitations to the use of CMR for cardiomyopathies. For one, many patients with heart failure and a reduced EF receive ICDs, and some with more severe heart failure refractory to medical therapy receive CRT devices. At present, both ICDs and CRT devices are contraindicated for performing CMR. This contraindication limits the use of CMR in patients with more advanced heart failure. However, there is growing evidence of the safety of many of these devices under stringent conditions in MR scanners (72). In addition, with the growth in the implantation of MR-conditional pacemaker systems, there is recognition of the ability to perform cardiac imaging safely in patients with these devices (73). Another limitation is that patients with stage 4 or 5 chronic kidney disease cannot receive gadolinium because of concerns about the potential of causing nephrogenic systemic fibrosis in this population (74). Patients who have active heart failure and are unable to lie flat are also not candidates for CMR.
CONCLUSION
CMR is an extremely useful imaging technique for cardiomyopathies. CMR is the gold standard for the measurement of cardiac chamber size and function. With tissue characterization by LGE as well as T1 and T2 mapping, the underlying etiology of heart failure can be readily established. In addition, the presence and extent of LGE in cardiomyopathies are associated with adverse cardiovascular outcomes and poor responses to standard medical and interventional therapies. Thus, CMR has a major role to play in determining diagnosis and assessing prognosis for patients with cardiomyopathies.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. Christopher M. Kramer is supported in part by R01 HL075792 and U01HL117006-01A1; receives equipment support from Siemens Healthcare; and has consulted for Bristol–Meyers Squibb, Merck, Myokardia, and Heart Metabolomics. No other potential conflict of interest relevant to this article was reported.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication November 13, 2014.
- Accepted for publication December 26, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cardiac magnetic resonance for ventricular arrhythmias: a systematic review and meta-analysis
- Overview of complications of acute and chronic myocardial infarctions: revisiting pathogenesis and cross-sectional imaging
- Role of Cardiac Magnetic Resonance in the Diagnosis and Prognosis of Nonischemic Cardiomyopathy