


Abstract
Arsenic trioxide has in vitro and in vivo radiosensitizing properties. We hypothesized that arsenic trioxide would enhance the efficacy of the targeted radiotherapeutic agent 131I-metaiodobenzylguanidine (131I-MIBG) and tested the combination in a phase II clinical trial. Methods: Patients with recurrent or refractory stage 4 neuroblastoma or metastatic paraganglioma/pheochromocytoma (MP) were treated using an institutional review board–approved protocol (Clinicaltrials.gov identifier NCT00107289). The planned treatment was 131I-MIBG (444 or 666 MBq/kg) intravenously on day 1 plus arsenic trioxide (0.15 or 0.25 mg/m2) intravenously on days 6–10 and 13–17. Toxicity was evaluated using National Cancer Institute Common Toxicity Criteria, version 3.0. Response was assessed by International Neuroblastoma Response Criteria or (for MP) by changes in 123I-MIBG or PET scans. Results: Twenty-one patients were treated: 19 with neuroblastoma and 2 with MP. Fourteen patients received 131I-MIBG and arsenic trioxide, both at maximal dosages; 2 patients received a 444 MBq/kg dose of 131I-MIBG plus a 0.15 mg/kg dose of arsenic trioxide; and 3 patients received a 666 MBq/kg dose of 131I-MIBG plus a 0.15 mg/kg dose of arsenic trioxide. One did not receive arsenic trioxide because of transient central line–induced cardiac arrhythmia, and another received only 6 of 10 planned doses of arsenic trioxide because of grade 3 diarrhea and vomiting with concurrent grade 3 hypokalemia and hyponatremia. Nineteen patients experienced myelosuppression higher than grade 2, most frequently thrombocytopenia (n = 18), though none required autologous stem cell rescue. Twelve of 13 evaluable patients experienced hyperamylasemia higher than grade 2 from transient sialoadenitis. By International Neuroblastoma Response Criteria, 12 neuroblastoma patients had no response and 7 had progressive disease, including 6 of 8 entering the study with progressive disease. Objective improvements in semiquantitative 131I-MIBG scores were observed in 6 patients. No response was seen in MP. Seventeen of 19 neuroblastoma patients continued on further chemotherapy or immunotherapy. Mean 5-year overall survival (±SD) for neuroblastoma was 37% ± 11%. Mean absorbed dose of 131I-MIBG to blood was 0.134 cGy/MBq, well below myeloablative levels in all patients. Conclusion: 131I-MIBG plus arsenic trioxide was well tolerated, with an adverse event profile similar to that of 131I-MIBG therapy alone. The addition of arsenic trioxide to 131I-MIBG did not significantly improve response rates when compared with historical data with 131I-MIBG alone.
Metaiodobenzylguanidine (MIBG) is a guanethidine analog that is taken up via the noradrenaline transporter by neuroendocrine malignancies arising from sympathetic neuronal precursors (1). These neoplasms include neuroblastoma, the most common solid tumor of childhood, which is often metastatic at diagnosis, and malignant paraganglioma/pheochromocytoma (MP). Recent therapeutic advances have led to modest improvements in the outcome of patients with high-risk neuroblastoma; however, approximately half the patients with stage 4 neuroblastoma and a much higher proportion of patients with relapsed or chemorefractory disease succumb to it (2). 123I-MIBG scans are the gold standard for staging of neuroblastoma, with more than 90% of patients having 123I-MIBG–avid disease (3). 131I-MIBG therapy has undergone several trials for neuroblastoma over more than 3 decades (4). A dose of 666 MBq/kg is generally accepted as the maximum per administration (5). The consensus is that treatment, although active against resistant neuroblastoma, especially for disease palliation (6), is not curative. Reported response rates have been no more than 30% even when relatively nonstringent criteria were used to evaluate disease response (4). Similarly, a response in patients with MP is uncommon, although 131I-MIBG therapy is associated with symptomatic relief and hormonal response (7).
The cause of suboptimal response has not been well characterized and is likely multifactorial (8). Strategies to enhance the clinical response to 131I-MIBG therapy have included increasing the amount (i.e., administered activity) and number of 131I-MIBG doses (5,9), combining them with myeloablative chemotherapy and autologous stem cell transplantation (10), and adding radiation-sensitizing agents (11,12). Preclinical mechanistic justifications for the clinical use of radiosensitizers in combination with 131I-MIBG therapy include enhancement of noradrenaline transporter expression or activity, such as through topoisomerase inhibitors, and a synergistic effect on inhibition of radiation-induced DNA repair, such as through vorinostat (13,14).
Arsenic trioxide is an apoptotic agent that acts via cytotoxic pathways distinct from conventional chemotherapeutic agents and suppresses growth of neuroblastoma xenografts (15,16). Its radiation-sensitizing effects have been demonstrated in preclinical models of several tumors, including fibrosarcoma (17) and glioma (18,19). The combination of 89Sr and arsenic trioxide showed beneficial killing of MCF7 cells (20). In other preclinical experiments, arsenic trioxide synergized with the radioiodinated anti-GD2 monoclonal antibody 131I-3F8 against neuroblastoma xenografts (Modak et al. unpublished data 2003). Clinical evidence suggesting a radiosensitizing effect for arsenic trioxide is derived from reports of response to concurrent arsenic trioxide and external-beam radiotherapy in chemoradioresistant cutaneous breast cancer (21) and extramedullary acute promyelocytic leukemia (22) and from a report of severe radiation recall in a patient previously treated with arsenic trioxide (23). Arsenic trioxide has been established as a highly effective agent for the treatment of acute promyelocytic leukemia in adults and children, and the combination of arsenic trioxide and all-trans retinoic acid may reduce the need for subsequent anthracycline therapy (24). In children with acute leukemia and infiltrating astrocytoma treated with arsenic trioxide in phase I studies, arsenic trioxide was well tolerated, with adverse events similar to those encountered in adults: vomiting, diarrhea, and QTc prolongation (25,26), with a recommended dosage of 0.15 mg/kg/d. However, in children with neuroblastoma and other solid tumors treated with arsenic trioxide as a single agent, dose-limiting toxicity was not encountered even at 0.25 mg/kg/d when serum electrolytes were optimally maintained (clinicaltrials.gov identifier NCT00024258). On the basis of these preclinical and clinical data, and the nonoverlapping toxicities of the two agents, we hypothesized that arsenic trioxide would act as a radiosensitizer for 131I-MIBG therapy, and we conducted a pilot phase II study (NCT00107289) in patients with relapsed or refractory neuroblastoma and MP, the results of which we report below.
MATERIALS AND METHODS
Patient Selection
Eligible patients were those older than 1 y with high-risk neuroblastoma (stage 4 disease diagnosed at >18 mo old or MYCN-amplified tumor of ≥stage 3 at any age) and a history of progressive disease or chemoresistance, and those younger than 21 y with MP. The presence of 123I-MIBG–avid evaluable or measurable disease 3 wk or more after completion of systemic therapy was required for protocol entry. Other salient eligibility criteria included the availability of at least 2 × 106 CD34+ autologous hematopoietic stem cells (cryopreserved for reinfusion) per kilogram of body weight, ability and willingness to comply with radiation safety procedures, and lack of life-threatening infections and nonhematologic toxicity higher than grade 2 (including renal, cardiac, hepatic, pulmonary, gastrointestinal, and neurologic) according to version 3.0 of the Common Toxicity Criteria of the National Cancer Institute.
Study Design
The protocol was approved by the institutional review board of Memorial Sloan Kettering Cancer Center. Written informed consent was obtained from patients or their guardians. Since this was the first study of this novel combination, it was decided not to proceed with maximal doses unless no serious adverse events were encountered in a pilot group of 5 patients who were treated with reduced doses of the therapeutic agents. Treatment consisted of a single intravenous dose of 131I-MIBG (444 [12 mCi/kg] or 666 MBq/kg [18 mCi/kg]) administered over 1 h on day 0 followed by intravenous arsenic trioxide as a single daily dose of 0.15 mg/kg or 0.25 mg/kg administered over 2 h on days 5 through 9 and days 12 through 16. 131I-MIBG was radiolabeled at Nuclear Diagnostic Products and had a confirmed radiochemical purity of at least 99% within 4 h before injection. Toxicities were graded with Common Toxicity Criteria, version 3.0, and response for neuroblastoma patients was assessed 4–6 wk after 131I-MIBG therapy, with International Neuroblastoma Response Criteria (27) modified to include 123I-MIBG scans. Response was classified as complete remission (no evidence of disease including in bone marrow), very good partial response (primary mass reduced by >90%, no evidence of distant disease and normal catecholamines), partial remission (>50% decrease in measurable disease, number of positive bone sites decreased by 50%, and ≤1 positive bone marrow site), mixed response (no new lesions, >50% decrease in any measurable lesion and <50% decrease in any other), no response (<50% decrease but <25% increase in any existing lesion), and progressive disease (new lesion or >25% increase in an existing lesion). Patients with no response or mixed response were categorized as having stable disease. For patients with MP, RECIST criteria were used if there was measurable disease. For both groups of patients, objective changes in 123I-MIBG scans were recorded using the semiquantitative Curie score (28,29). Relative 123I-MIBG score was calculated by dividing Curie score after treatment by prior Curie score. Dosimetry and pharmacokinetic data were obtained using serial whole-body imaging and peripheral venous blood specimens; typically, up to 10 blood samples were obtained from less than 1 h after to 10 d after 131I-MIBG injection. The activity concentrations in weighed aliquots of blood were measured in a scintillation well counter calibrated for 131I, fit to a biexponential time–activity concentration function, and analytically integrated to yield the area under the curve. The resulting cumulated activity concentration was then multiplied by the equilibrium dose constant for the 131I β-rays, Δβ = 0.405 g-cGy/37 MBq, to yield the mean absorbed dose to blood. Implicit in the foregoing absorbed-dose calculation were the standard assumptions that the 131I β-rays are completely absorbed in blood and the contribution of the highly penetrating γ-rays was negligible.
Safety Precautions
Thyroid protection included oral administration of a saturated solution of potassium iodide (5–7 drops [250–330 mg] thrice daily) and liothyronine (25–75 μg once daily) starting about 7 d before 131I-MIBG and continuing for 14 and 42 d, respectively, after 131I-MIBG infusion. 131I-MIBG was administered on an in-patient basis, only after demonstration of thyroid suppression as documented by subnormal thyroid-stimulating hormone levels. Urinary bladder protection was provided by maintenance of a Foley catheter for at least 72 h after 131I-MIBG therapy. Radiation safety precautions were followed to minimize exposure to family, public, and staff, including use of isolation rooms and rolling lead shields. Patients were discharged only after the whole-body dose rate had fallen to less than 7 cGy/h at a distance of 1 m. Arsenic trioxide was administered only if the absolute QT interval was more than 500 ms. During arsenic trioxide therapy, serum potassium and magnesium levels were maintained at more than 4 mEq/dL and more than 1.8 mg/dL, respectively. Filgrastim was given to maintain an absolute neutrophil count of more than 500/μL. Platelet and red blood cell transfusions were administered as clinically indicated. Patients were required to receive autologous stem cell rescue (ASCR) if their absolute neutrophil count remained less than 500/μL for more than 14 d despite filgrastim, if they required platelet transfusions more than twice weekly for 4 wk after 131I-MIBG therapy, or if they experienced life-threatening infection in the setting of neutropenia.
Biostatistical Considerations
Since this was the first study of the novel combination of 131I-MIBG therapy and arsenic trioxide, we instituted early-stopping rules for unacceptable toxicity: therapy was stopped early if at least 4 of the first 10 patients or 6 patients at any time experienced a nonhematologic toxic event higher than grade 3 or if at least 3 patients experienced graft failure after ASCR. The primary endpoint was efficacy of the combination as assessed by response. We proposed declaring treatment effective if the probability of response was at least 0.4. A Simon 2-stage design that differentiated between response rates of 0.4 and 0.65 was used, with plans to treat 13 evaluable neuroblastoma patients at maximal doses of 131I-MIBG and arsenic trioxide in the first phase and to add 15 neuroblastoma patients only if more than 5 responses (complete remission plus partial remission) were observed in the first cohort. The efficacy rule did not apply to patients with MP. Survival was analyzed using Kaplan Meier and log-rank tests (SPSS).
RESULTS
Patient Demographics
Twenty-one patients (12 male and 9 female, with a median age of 7.8 y and a range of 2–30.4 y) were treated from 2005 to 2008: 19 with neuroblastoma, including one treated as per protocol after compassionate approval from the Memorial Sloan Kettering Cancer Center institutional review board and two with MP (Table 1). Two patients received a 444 MBq/kg dose of 131I-MIBG plus a 0.15 mg/kg dose of arsenic trioxide and 3 received a 666 MBq/kg dose of 131I-MIBG plus a 0.15 mg/kg dose of arsenic trioxide. Fourteen patients (including one treated as per protocol) received 131I-MIBG plus arsenic trioxide at maximal dosages of 666 MBq/kg plus 0.25 mg/kg, respectively.
Patient Demographics, Response, and Survival
Neuroblastoma patients had undergone heavy prior treatment, with a median of 3 previous therapeutic regimens; 15 patients were treated after prior relapse (median, 2 prior relapses), and 4 had chemorefractory metastatic disease. Fourteen had stage 4 disease at diagnosis, whereas one (patient 8; Table 1) was diagnosed with stage 2B neuroblastoma and then relapsed with metastatic disease before study entry. Both MP patients had germline mutations in the succinyl dehydrogenase B gene, had multiple skeletal metastatic sites (123I-MIBG Curie scores of 7 and 9, respectively), and had recurrent disease 2 and 7 mo after alkylator-based chemotherapy. Most patients had a relatively high disease burden at entry, with a median (±SD) Curie score of 9 ± 5.9 (range, 2–21).
Toxicity
Treatment was well tolerated in general, without mortality or severe morbidity (Table 2). None of the 5 patients treated with reduced doses experienced severe adverse events, and a further 14 patients received both agents at maximal doses. One patient (patient 6; Table 1) did not receive any arsenic trioxide because of the development of central line–related arrhythmia before commencing arsenic trioxide. A second patient developed arsenic trioxide–related grade 3 vomiting and diarrhea with accompanying grade 3 hypokalemia and hyponatremia and received only 6 of 10 planned doses of arsenic trioxide. Other expected toxicities higher than grade 2 were those that have previously been described with 131I-MIBG therapy (9,30) and included neutropenia (n = 16 patients), thrombocytopenia (n = 18), lymphopenia (n = 18), anemia (n = 12), and hyperamylasemia due to transient sialoadenitis (n = 12/13 patients evaluated). No patient experienced febrile neutropenia or serious infection. All patients with thrombocytopenia received platelet transfusions. As defined in the protocol criteria, ASCR was not required for any patient. Thyroid-stimulating hormone levels assessed 3–6 mo after therapy were normal (n = 12).
Toxicity Related to Therapy
Pharmacokinetics, Dosimetry, and Targeting
123I-MIBG in blood exhibited biphasic kinetics (evaluated in 16 patients), with an initial rapid component (87% of the blood activity on average) having a mean biologic half-life of 1.37 ± 1.41 h and a second slower component (13% of the blood activity on average) having a biologic half-life of 28.1 ± 5.62 h. A typical blood time–activity curve is shown in Figure 1. The absorbed dose to blood averaged 0.134 ± 0.0928 cGy/MBq, with a maximum of 0.354 cGy/MBq. The total absorbed dose to blood was 46.0 ± 25.0 cGy. Posttreatment 131I-MIBG γ-camera scanning was performed on 20 patients. All sites of disease detected by pretherapy 123I-MIBG scans showed targeting with therapeutic 131I-MIBG. In addition, a significantly higher number of skeletal lesions were detected on post–131I-MIBG therapy scans in all (neuroblastoma and MP) patients with skeletal disease (n = 17), with 3.3 ± 1.6 (range, 2–7) additional lesions noted (P < 0.05 by t testing for pretherapy vs. posttherapy 123I-MIBG scores). However, no extra lesions were detected in patients who had only soft-tissue disease (n = 3).
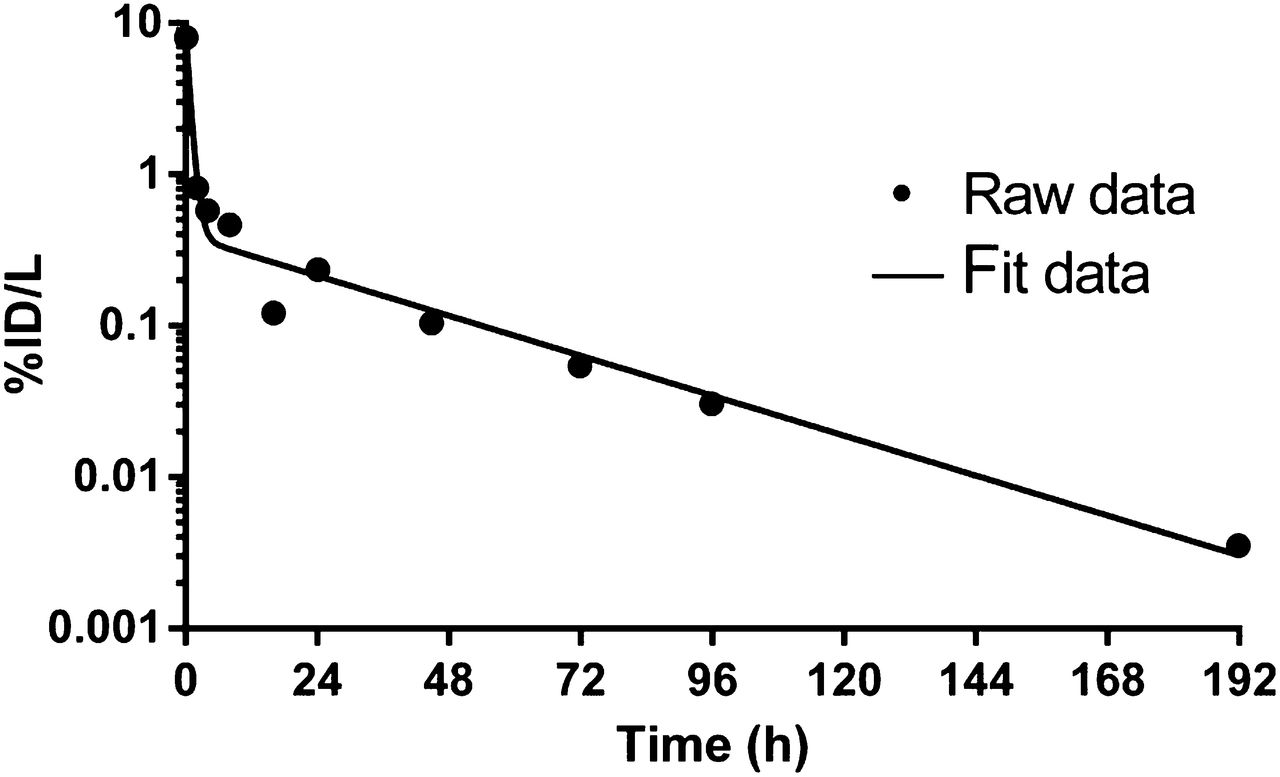
Typical 131I-MIBG blood time–activity concentration curve. Data points represent measured values and curve best-fit function, with initial component having zero-time intercept of 891.7 kBq (24.1 μCi)/mL (94% of activity in blood) and biologic half-life of 1.88 h and second component having zero-time intercept of 55.5 kBq (1.5 μCi)/mL (6% of activity in blood) and biologic half-life of 23.9 h. ID = injected dose.
Disease Response
Neuroblastoma
Overall, no major response (complete remission plus partial remission) was observed in neuroblastoma patients (Table 1). Twelve patients had no response by International Neuroblastoma Response Criteria, and 7 had progressive disease. Of 8 patients with progressive disease at study entry, 6 had further progressive disease, whereas 10 of 11 patients with stable nonprogressing disease immediately before protocol therapy had no response to treatment. There was no reduction in measurable soft-tissue disease (n = 9) or in bone marrow neuroblastoma as assessed by histology (n = 6). Fifteen of 19 patients had 123I-MIBG–avid skeletal metastases, and 4 of 19 had only 123I-MIBG–avid soft-tissue disease before therapy. Of 15 patients with skeletal disease, 9 had no change on 123I-MIBG scanning (relative 123I-MIBG score of 1) and 6 had an objective response on 123I-MIBG scanning but a relative 123I-MIBG score greater than 0.5, thus not meeting the extended International Neuroblastoma Response Criteria for partial remission (Table 3). Three of the 4 patients with only soft-tissue disease before therapy had progressive disease. Urine catecholamine levels were reduced in 4 of 7 patients with elevated levels.
Objective Response Rates in Patients with Neuroblastoma
MP
Both patients with MP had extensive skeletal disease (123I-MIBG scores of 7 and 9, respectively), and one had measurable soft-tissue disease; neither had an objective response to therapy with 131I-MIBG plus arsenic trioxide. Urine normetanephrines decreased by 50% in one patient, whereas the other did not secrete metanephrines.
The study was terminated after the first phase since it did not meet the response criteria for continuation.
Postprotocol Therapy and Survival
Seventeen neuroblastoma patients went on to receive additional therapy for their residual or progressive disease after leaving the study. Although ASCR was not indicated for any patient during the study, 10 patients underwent ASCR after high-dose myelosuppressive (but nonmyeloablative) chemotherapy after completing the required protocol observations, and all patients engrafted after ASCR. Other postprotocol therapies included immunotherapy with the anti-GD2 monoclonal antibody 3F8 (n = 7). One patient had early progressive disease and did not receive any further therapy, whereas another did not receive any further therapy but is a long-term survivor at more than 91 mo after therapy despite having persistent 123I-MIBG–avid pancreatic disease. All patients were followed for late toxicities, none of which were observed. The contribution of 131I-MIBG plus arsenic trioxide in prolonging survival could not be evaluated. Five-year overall survival for neuroblastoma patients is 37% ± 11%, with 7 long-term survivors, all but one of whom (patient 17; Table 1) have residual disease. Patient 17 achieved complete remission after further therapies after 131I-MIBG and remains a long-term disease-free survivor. Median overall survival was 23.7 ± 9.1 mo, and median time to progressive disease was 6.5 ± 2 mo. However, patients with progressive disease at study entry had a significantly worse survival (P < 0.001 for overall and progression-free survival) than those with stable disease before therapy, with a median overall and progression-free survival of 9.8 ± 1 and 1.4 ± 0.3 mo, respectively. Both patients with MP survive with residual but progression-free disease, at 63.1 and 100.2 mo after therapy. One was treated with a second dose of high-dose 131I-MIBG therapy without arsenic trioxide, whereas the other did not receive any postprotocol therapy.
DISCUSSION
The combination of high-dose 131I-MIBG therapy and arsenic trioxide, even at maximal doses, was well tolerated and had no significant unexpected toxicity. As anticipated with 131I-MIBG doses of at least 444 MBq/kg, myelosuppression higher than grade 3 and requiring blood product support was encountered, though no patient developed serious infections or required inpatient admission after discharge after 131I-MIBG infusion. In only one patient did arsenic trioxide add significant toxicity. Neither 131I-MIBG nor arsenic trioxide had an effect on response or toxicity, with the only nonhematologic toxicity higher than grade 2 being observed in the patient who received 6 of ten 0.25 mg/kg doses of arsenic trioxide. Posttherapy scans showed excellent targeting of 131I-MIBG to lesions and, similar to previous reports (31), revealed lesions not detected on pretherapy 123I-MIBG scans. However, response rates for resistant neuroblastoma were not better than the historical data on single-agent high-dose 131I-MIBG, suggesting that arsenic trioxide did not have a radiosensitizing or other beneficial effect for 131I-MIBG therapy. Objective responses were not seen in the two MP patients.
Similar observations have been made for other radiosensitizers, though toxicity has generally been worse than that encountered with 131I-MIBG plus arsenic trioxide. Specifically, the addition of irinotecan and vincristine to 131I-MIBG therapy yielded response rates of 25% but with an increase in toxicity, whereas combination with vorinostat was associated with a response rate of 12%–17% (12,32). The combination of 131I-MIBG therapy and myeloablative chemotherapy followed by autologous stem cell transplantation has been investigated by several groups. 131I-MIBG therapy followed by myeloablative chemotherapy with carboplatin, etoposide plus melphalan (10), or busulfan plus melphalan (33) was associated with significant toxicity, especially hepatic sinusoidal obstructive syndrome, without a response improvement in chemoresistant neuroblastoma (34). The contribution of 131I-MIBG therapy to response could not be defined, and there remains a need to optimize the use of 131I-MIBG therapy followed by myeloablative chemotherapy for patients with neuroblastoma. Small, nonrandomized studies have reported better response rates when 131I-MIBG therapy has been used in the upfront treatment of neuroblastoma, though these studies included children with low-stage, intermediate-risk disease and imaging did not consistently include sensitive 123I-MIBG scans (35,36). Possible reasons for the low major response rate observed in neuroblastoma patients in our study could include a high disease burden at time of treatment (median pretherapy 123I-MIBG score of 9) and a high proportion (74%) of patients treated after multiple relapses, with a median of 3 relapses before treatment with 131I-MIBG plus arsenic trioxide. Furthermore, outcomes were even worse in patients with progressive disease who commenced therapy immediately before study entry (further progressive disease in 75%), suggesting that 131I-MIBG therapy should be initiated only after disease has been stabilized with other modalities such as salvage chemotherapy.
Patients with refractory and relapsed metastatic neuroblastoma are considered to have a poor prognosis (37,38). Although we observed few objective responses to therapy, a higher than expected number of neuroblastoma patients treated in our study (37% [7/19]) are long-term survivors, although all but one have residual MIBG–avid disease. The survivors include 3 patients treated at first relapse. Since 17 of 19 patients received further therapies, including 3F8, dissecting out the possible role of 131I-MIBG plus arsenic trioxide to their improved survival is impossible.
The natural history of MP is often marked by prolonged remissions even without any anticancer therapy (39). Therefore, the contribution of 131I-MIBG plus arsenic trioxide to the long-term progression-free status of the two treated patients is unclear. Nevertheless, for both patients, the current progression-free intervals are significantly (10×) higher than the time from prior therapy to relapse.
Extensive blood time–activity data were successfully collected and analyzed in 16 patients, with uniformly excellent fitting of biexponential functions to these data. On the basis of this analysis, the total absorbed dose to blood averaged only 46 cGy, well below myeloablative doses. This finding is consistent with the rapid initial clearance of 131I-MIBG, with 87% of the blood-borne activity being cleared and a biologic half-time of 1.37 h on average. It is somewhat unexpected that these dose estimates would result in grade 3 or 4 bone marrow toxicity. However, all patients had been heavily treated beforehand with chemotherapy. An additional contribution to toxicity could be bone marrow involvement with neuroblastoma. Similar severe myelosuppression has been reported in all other studies using 131I-MIBG doses of 444 MBq/kg or higher.
CONCLUSION
High-dose 131I-MIBG plus the radiosensitizer arsenic trioxide was well tolerated in patients who had a substantial disease burden and had received heavy prior treatment. Antineuroblastoma activity was modest and approximated that observed in similar patient populations treated with high-dose 131I-MIBG with or without other radiosensitizers.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Rodney Prosser and the team at Nuclear Diagnostic Products for assisting with radiolabeling protocols and methods, Dr. Peter Smith-Jones for quality control, Samantha Leyco for data management, and Joe Olechnowicz for editorial input. We also thank Amabella Lindo, Louise Harris, and the radiopharmacy, radiation safety, and pediatric nursing teams at Memorial Sloan Kettering Cancer Center for dispensing and facilitating the administration of 131I-MIBG.
Footnotes
Published online Jan. 7, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication June 3, 2015.
- Accepted for publication October 13, 2015.





{kind=link}