


Abstract
18F-FDG PET/CT plays a significant role in the assessment of various infectious processes. Patients with suspected or known sites of infection are often referred for 18F-FDG imaging while already receiving antibiotic treatment. The current study assessed whether antibiotic therapy affected the detectability rate of infectious processes by 18F-FDG PET/CT. Methods: A 5-y retrospective study of all adult patients who underwent 18F-FDG PET/CT in search of a focal source of infection was performed. The presence, duration, and appropriateness of antibiotic treatment before 18F-FDG imaging were recorded. Diagnosis of an infectious process was based on microbiologic or pathologic data as well as on clinical and radiologic follow-up. Results: Two hundred seventeen patients underwent 243 PET/CT studies in search of a focal source of infection and were included in the study. Sixty-seven studies were excluded from further analysis because of a final noninfectious etiology or lack of further follow-up or details regarding the antibiotic treatment. The final study population included 176 18F-FDG PET/CT studies in 153 patients (107 men, 46 women; age range, 18–86 y). One hundred nineteen studies (68%) were performed in patients receiving antibiotic therapy for a range of 1–73 d. A diagnosis of infection was made in 107 true-positive cases (61%), including 63 studies (59%) in patients receiving appropriate antibiotic therapy started before the performance of the 18F-FDG PET/CT study. There were 52 true-negative (29%) and 17 false-positive (10%) 18F-FDG PET/CT studies. No false-negative results were found. Conclusion: 18F-FDG PET/CT correctly identified foci of increased uptake compatible with infection in most patients, including all patients receiving appropriate antimicrobial therapy, with no false-negative cases. On the basis of the current study results, the administration of antibiotics appears to have no clinically significant impact on the diagnostic accuracy of 18F-FDG PET/CT performed for evaluation of known or suspected infectious processes.
In recent years, there has been increasing literature evidence regarding the role of 18F-FDG PET/CT in the evaluation of various infectious and aseptic inflammatory disorders (1). The accumulation of 18F-FDG in infectious processes is due to the fact that activated leukocytes exhibit high amounts of glucose transporter proteins on the cell membrane (2,3). For patients with suspected bacterial infections, antibiotic treatment is often administered before a definite focus of infection has been identified. Thus, the clinical setting when patients with suspected infections undergo 18F-FDG PET/CT study while already receiving antibiotic therapy is not rare.
The labeling of white blood cells with 99mTc-HMPAO or 111In-oxine has been the gold standard nuclear medicine procedure for diagnosis of various infectious processes in the era before 18F-FDG PET/CT. Some publications have addressed the issue of a potential effect of antibiotic therapy on leukocyte chemotaxis in vitro and on the sensitivity of labeled white blood cell scans with conflicting results (4,5).
To the best of our knowledge, the potential effect of antibiotic treatment on the uptake of 18F-FDG is not well established. The current study aimed at assessing whether antibiotic therapy affected the detectability rate of infectious processes by 18F-FDG PET/CT.
MATERIALS AND METHODS
Patient Population
The study population included all adult patients investigated for suspected infectious process and assessed by 18F-FDG PET/CT over the years 2010–2015. The indications for referral included suspected musculoskeletal, vascular graft, and polycystic kidney infection, as well as patients with fever of unknown origin and bacteremia evaluated in search of a focal source of infection. Patients were identified from a review of 18F-FDG PET/CT referrals over this period. The Institutional Review Board approved this retrospective study, and the requirement to obtain informed consent was waived. Patient files were reviewed for clinical data at the time of imaging. The administration of antibiotic treatment before 18F-FDG PET/CT was performed was recorded. In patients receiving antibiotic treatment, the duration before the PET/CT study and route (intravenous or oral) of administration were recorded. Antimicrobial therapy was considered to be appropriate if administered according to the susceptibility of the specific type of pathogen diagnosed by microbiologic tests or if it led to clinical improvement in cases with no microbiologically documented infection. When these criteria were not met, antibiotic treatment was defined as inappropriate and patients in this subgroup were considered as not treated in further analysis. The final diagnosis of an infectious process was based on microbiologic and pathologic data as well as on clinical and imaging follow-up.
PET/CT Acquisition
Patients were instructed to fast, except for glucose-free oral hydration, for at least 4 h before the injection of 185–592 MBq (5–16 mCi) of 18F-FDG. The patients kept their regular drug schedule. Oral contrast was administered selectively. Patients evaluated for fever of unknown origin, bacteremia, and suspected polycystic kidney infection underwent eye-to-midthigh PET/CT acquisition, with lower limb scanning added when clinically indicated. Patients investigated for suspected musculoskeletal and vascular graft infection were scanned according to the clinical area of interest. PET/CT (Discovery 690; GE Healthcare) images were acquired 60 min after the injection of the radiopharmaceutical and reviewed in axial, coronal, and sagittal planes on a dedicated workstation (Xeleris; GE Healthcare).
Interpretation and Analysis of PET/CT Images
All studies were reviewed by 2 nuclear medicine physicians with knowledge of the clinical history and results of previous imaging studies but unaware whether antibiotic treatment had been administered. Studies showing at least 1 site of 18F-FDG uptake with intensity higher than that of surrounding tissues, localized to an area that did not correspond to the physiologic biodistribution of the tracer, were defined as positive. Studies showing 18F-FDG activity only in areas of physiologic tracer distribution were defined as negative. A positive 18F-FDG PET/CT study in a patient further confirmed as having a focal active infectious process was defined as true-positive (TP). A positive 18F-FDG study in patients with no final diagnosis of focal infection or with pathology identified in a location different from the site demonstrated on PET/CT was defined as false-positive (FP). A negative PET/CT study was true-negative if no localized infectious process was further diagnosed whereas in patients with further evidence of an active infection it was defined as false-negative (FN).
SUVmax was measured in all clinically relevant foci of increased 18F-FDG activity. In studies, showing multiple foci of increased 18F-FDG uptake, the highest SUVmax was recorded and used for further analysis.
Statistical Analysis
Comparison of SUVmax measurements of 18F-FDG uptake in sites of infection between different groups of patients was performed using the Mann–Whitney test. Differences with a P value of less than 0.05 were considered statistically significant.
RESULTS
Between March 2010 and October 2015, a group of 217 patients underwent 243 PET/CT studies in search of a focal source of infection. After initial evaluation of patients’ clinical records, 67 studies were excluded from further analysis, including 23 studies in patients lacking information regarding administered antibiotics, 14 studies in patients with fever of unknown origin with a final noninfectious diagnosis, and 30 studies in patients with no further follow-up.
Therefore, the final study population included 176 18F-FDG PET/CT studies in 153 patients (107 male and 46 female patients; age range, 18–86 y). Fifteen patients underwent multiple PET/CT studies. The reasons for performing 18F-FDG PET/CT included suspected musculoskeletal infection (n = 70), vascular graft infection (n = 39), bacteremia (n = 31), fever of unknown origin (n = 30), and suspected polycystic kidney infection (n = 6). Elevated levels of C-reactive protein (a value >5 mg/L) and leukocytosis (>12,000/μL) were found in 116 and 71 patients, respectively. Fever (temperature >38°C) was measured in 64 patients, with a mean duration of 5 d (1–38 d). A focal infectious process was diagnosed in 92 of the 153 patients (60%).
One hundred nineteen studies (68%) were performed in patients receiving antibiotic therapy for a mean duration of 13 d (range, 1–73 d) (Table 1). Antibiotics were administered intravenously in 63 patients, orally in 17 patients, and both intravenously and orally in 39 patients. Fifty-seven studies (32%) were performed in patients who did not receive antibiotic treatment.
Demographic and Clinical Characteristics of Study Population
There were 124 positive (70%) PET/CT studies showing focal pathologic 18F-FDG uptake. There were 107 TP cases, including 63 studies (59%) in patients receiving appropriate antibiotic therapy (Fig. 1) for a mean duration of 11 d (range, 2–32 d). Five of these TP patients received appropriate antimicrobial treatment for a duration of about a month (range, 27–32 d). There were 44 TP studies in untreated patients, including 27 studies in untreated patients and 17 in those receiving inappropriate treatment (and thus considered as untreated), for a mean duration of 10.1 d (range, 1–60 d) (Fig. 2). The final diagnosis in the TP group included musculoskeletal (n = 46), vascular graft (n = 25), and postsurgical soft tissue (n = 11) infection; abscesses in the kidney and lung (n = 9 each) and abdomen (n = 5); and central line infection and tuberculosis in 1 case each. In 67 of the 107 TP cases (63%), the final diagnosis was made by microbiology or pathology and in the remaining 40 cases by clinical and imaging follow-up for a period of 2–24 mo. There were 17 FP studies, including 13 (76%) in patients not receiving antimicrobial therapy and 4 in treated patients. The final diagnosis in these FP studies was chronic granulomatotic or reactive postsurgical changes (n = 7); an inflammatory soft-tissue process (n = 3); and retroperitoneal fibrosis, Charcot osteoarthropathy, insufficiency fractures of pelvic bones, subcutaneous gluteal granuloma, and physiologic uptake in the aortic root (n = 1 case each). Two additional FP studies showed increased pericardial and vertebral 18F-FDG uptake of unclear etiology. MRI and clinical follow-up of 12 mo in these 2 cases did not reveal any pathology in these areas.
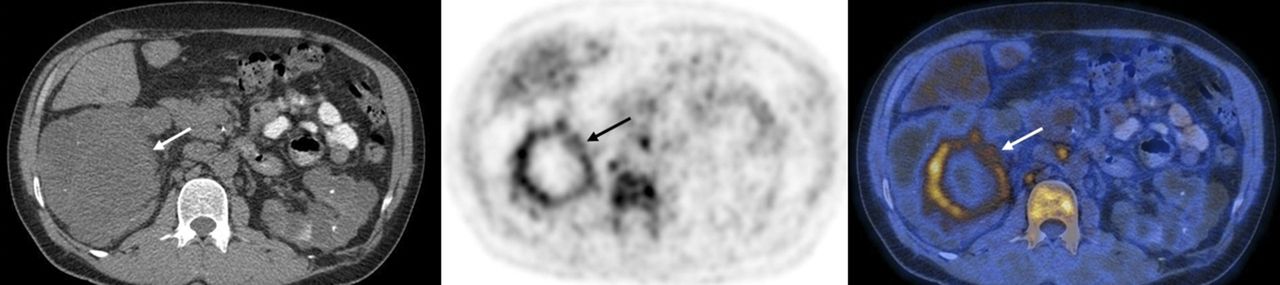
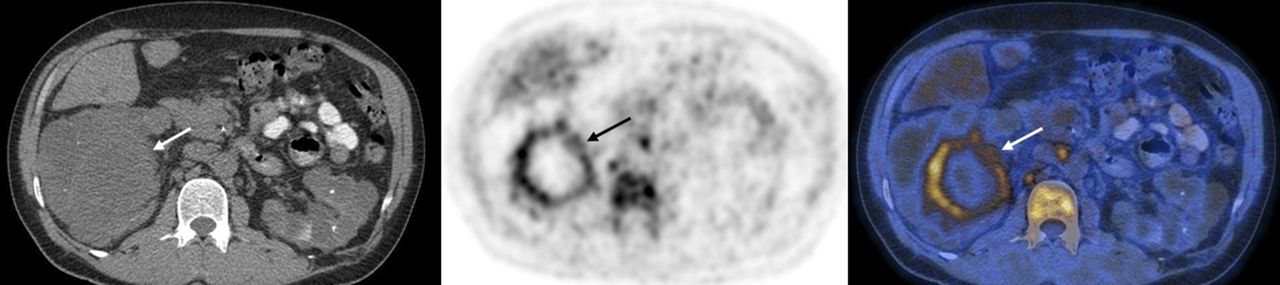
A 53-y-old man with polycystic kidney disease with suspected infected renal cyst. Patient received appropriate antibiotic therapy for 11 d before study. PET/CT images show increased 18F-FDG uptake at margins of right renal cyst (arrows) consistent with infection. Patient continued antibiotic treatment, with clinical improvement shown, but later underwent nephrectomy because of recurrent infection.
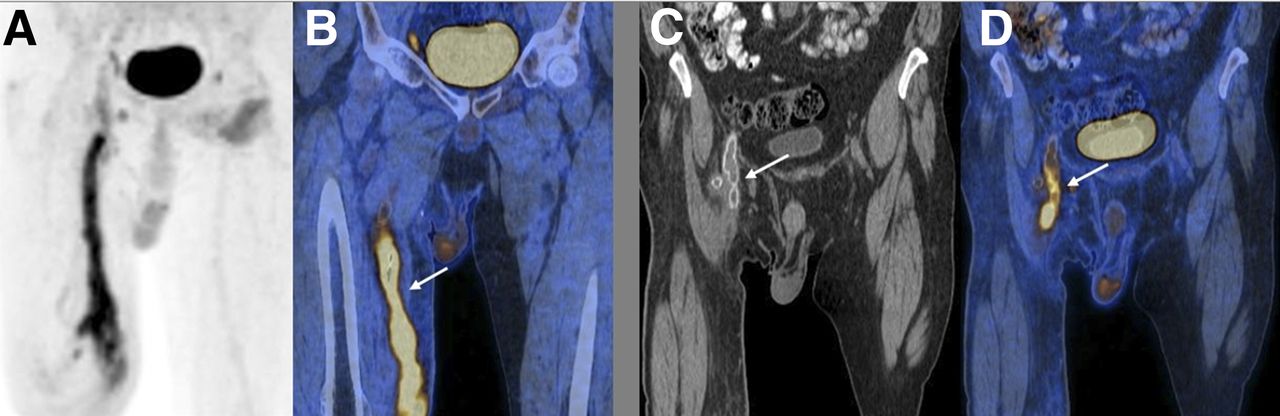
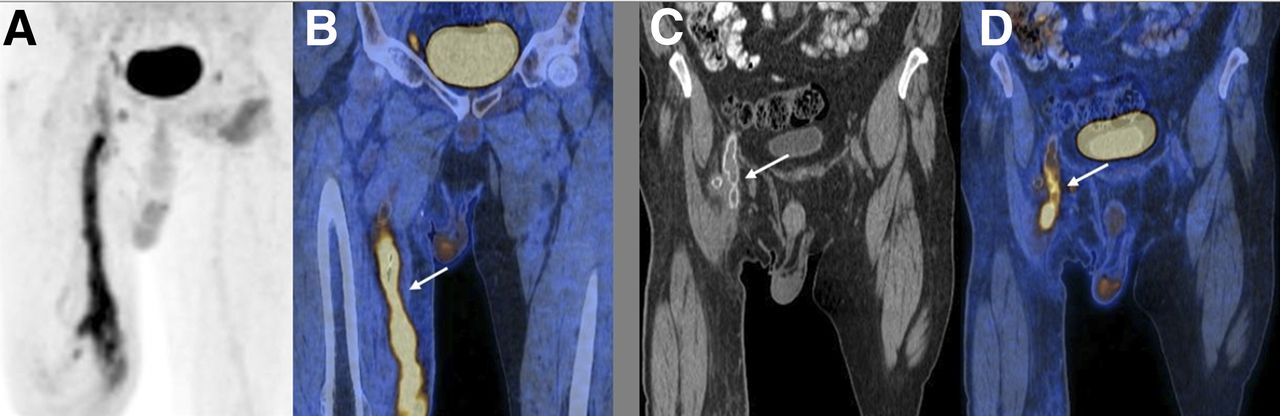
A 62-y-old man after right femoropopliteal bypass graft surgery, presented with right groin soft-tissue infection and suspected vascular graft involvement. Patient had received inappropriate antibiotic treatment for 4 d before PET/CT study. 18F-FDG maximum-intensity projection (A) and PET/CT images (B–D) demonstrate increased tracer uptake along medial aspect of right thigh involving soft tissues and proximal part of graft (arrows). Infected graft was removed, and diagnosis of infection was proven by pathology.
Fifty-two 18F-FDG PET/CT studies with no sites of pathologic 18F-FDG uptake and no significant findings on imaging and clinical follow-up of 2–24 mo were defined as true-negative. There were no FN results in the whole study population, including the treated and untreated patient groups.
SUVmax measurements at the TP sites of infection ranged from 1.6 to 17.9 (8.3 ± 3.5) and in FP foci from 3.9 to 15 (7.5 ± 3.2). SUVmax in 63 TP studies performed in appropriately treated patients ranged from 1.6 to 17.9 (7.8 ± 3.4), in 17 studies under inappropriate antibiotic treatment from 3.7 to 13.9 (8.2 ± 3.3), and in 27 TP studies in patients who were not receiving antibiotic therapy from 4.0 to 16.7 (9.5 ± 3.7). There was no statistically significant difference in the SUVmax measured in sites of infection between studies performed under appropriate antibiotic treatment and the untreated group (Table 2). Further analysis of SUVmax in sites of infection in patients receiving appropriate antibiotic therapy was performed according to the duration of treatment using an arbitrary threshold of 6 d. There was no statistically significant difference in SUVmax measured in sites of infection treated for more or less than 6 d (Table 3).
18F-FDG SUVmax in Foci of Infection in 107 TP Studies According to Antibiotic Treatment
18F-FDG SUVmax in Foci of Infection in 63 TP Studies According to Duration of Appropriate Antibiotic Treatment
DISCUSSION
18F-FDG PET/CT plays a significant role in the assessment of various infectious processes such as osteomyelitis in the setting of a complicated diabetic foot (6,7), infected orthopedic (8,9) or vascular prostheses (10,11), and fever of unknown origin (12–14). Patients with suspected bacterial infection are frequently referred for 18F-FDG imaging while already receiving antibiotic treatment. Several investigators have questioned whether there are factors that can affect and specifically decrease 18F-FDG uptake in malignant and infectious processes. The effect of diabetes mellitus and hyperglycemia on the presence and intensity of 18F-FDG activity in malignant and infectious processes has been previously evaluated. The study showed that although hyperglycemia led to a higher FN rate in cancer patients it had, in contrast, no significant effect on the detectability rate of infectious processes. There was no statistically significant difference in the number of FN studies in this patient group (15).
The possible impact of antibiotic treatment on the diagnostic accuracy of 18F-FDG PET/CT in patients with suspected infectious processes has, to the best of our knowledge, not been previously investigated. In addition, no study has addressed the timing for performing 18F-FDG imaging in patients with infection in relationship to antibiotic treatment.
Present results in a large retrospective study of 153 patients demonstrate that 18F-FDG PET/CT correctly identified foci of increased uptake compatible with infection in more than half of the study population, including all studies performed in patients receiving appropriate antibiotic therapy (59%) before imaging, with no FN results.
Of the 63 patients receiving appropriate therapy with TP studies, 5 were treated for a long time (∼1 mo). All 5 patients had microbiologically documented infections, and the appropriateness of antibiotic treatment was based on the in vitro susceptibilities. The fact that their PET/CT studies were still positive after such a long duration of appropriate antimicrobial treatment is most probably due to the type, severity, or location of their disease and the lack of response despite the appropriateness of the administered antibiotics.
In the current study, SUVmax in sites of infection was slightly lower but with no statistically significant difference in patients who underwent 18F-FDG PET/CT while receiving appropriate antibiotic treatment in comparison to a group of untreated patients. The same results were obtained when a comparison of SUVmax in sites of infection in patients receiving appropriate antibiotic therapy divided into 2 groups according to the duration of treatment using an arbitrary threshold of 6 d was made. Scarce literature in small series of patients has discussed the use of 18F-FDG imaging for antibiotic therapy control. In a study of 38 patients with spondylodiscitis, the degree of change in SUVmax had a higher sensitivity for early identification of responders than C-reactive protein levels (16). The response to antibiotic treatment was defined by a significant reduction in SUVmax between baseline and posttreatment PET/CT studies in a smaller group of 15 patients with infectious discitis (17). 18F-FDG PET/CT was also a useful tool in monitoring therapy results in 25 patients with prosthetic vascular graft infections, defining partial response as a decrease in SUVmax of more than 20% (18).
Because the current study includes mainly single examinations in patients with no serial, longitudinal studies performed before and after antibiotic therapy, this previously published data showing the value of SUVmax changes in treatment monitoring cannot be confirmed. Further prospective well-designed studies are needed to determine whether serial SUVmax 18F-FDG measurements will indeed be able to demonstrate therapy control and define response to antibiotics in various infectious processes.
One limitation of this retrospective study may be related to the unavailability of follow-up data and information regarding administered antibiotics in 67 of the 243 studies. Because the study includes such a large number of patients underscores the significance of the present results despite the relative heterogeneity of the study population, including patients with a variety of clinical indications treated with different antibiotic regimens.
CONCLUSION
18F-FDG PET/CT accurately detected infection in more than half of our large study population, including patients receiving appropriate antibiotic therapy before imaging, with no FN results. Antibiotic treatment appears to have no clinically significant impact on the diagnostic accuracy of 18F-FDG PET/CT performed for the assessment of known or suspected infectious processes.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online May 4, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 22, 2017.
- Accepted for publication April 11, 2017.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.