


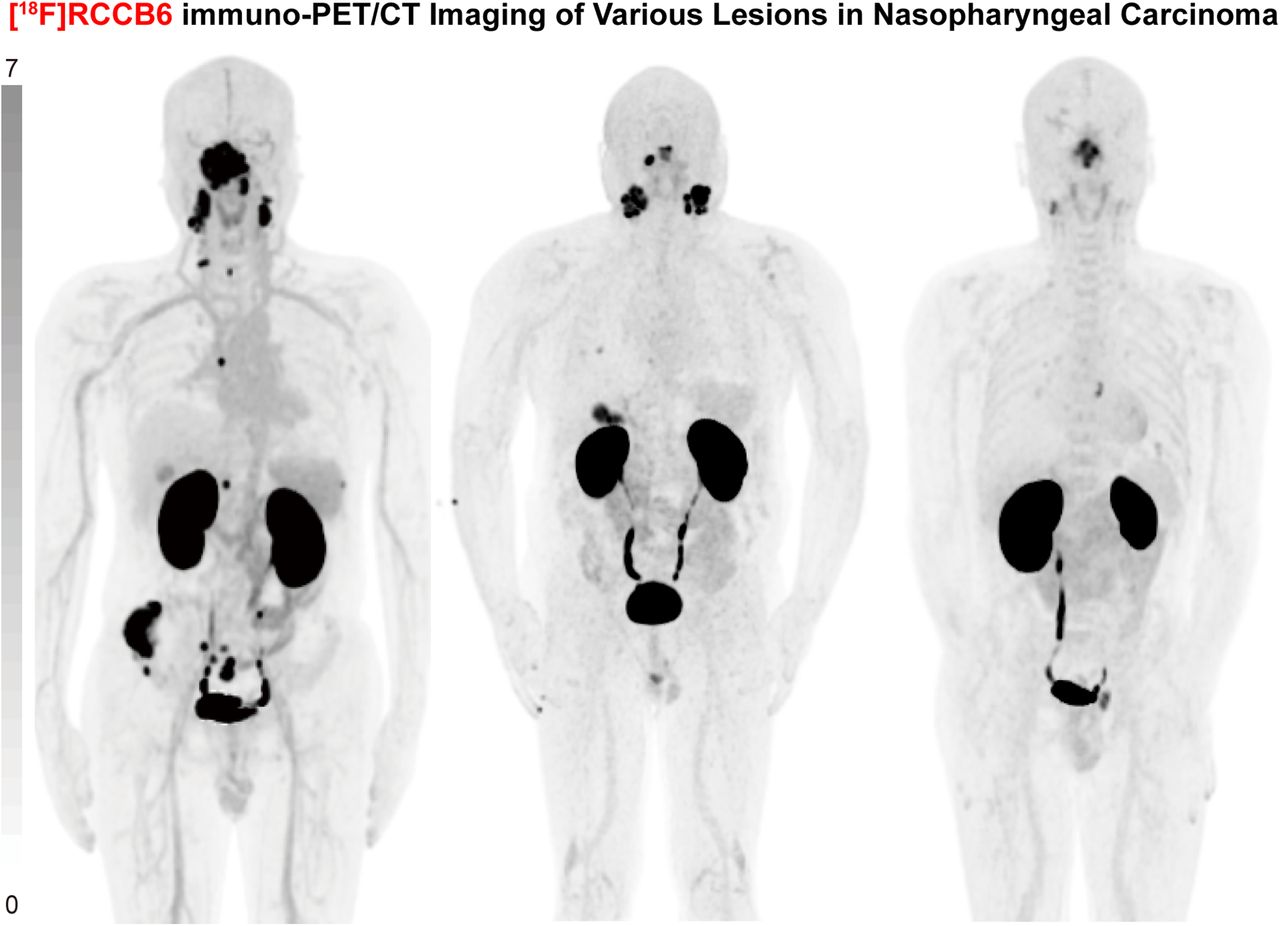
Visual Abstract

Abstract
CD70 has emerged as a promising biomarker for nasopharyngeal carcinoma (NPC). This study investigated CD70 expression patterns in NPC specimens and evaluated the diagnostic potential of CD70-targeted [18F]RCCB6 immuno-PET/CT in patients with NPC. Methods: CD70 expression was analyzed in 80 archived NPC specimens and correlated with clinical and pathologic features. Using [18F]RCCB6, a single-domain antibody–derived tracer specific for human CD70, the diagnostic efficacy of [18F]RCCB6 immuno-PET/CT was assessed in 25 patients with NPC and compared with that of 18F-FDG PET/CT. Results: CD70 was positively expressed in 72 (90%) of 80 NPC specimens, with expression levels strongly correlated with Epstein-Barr virus (EBV) titers (rs = 0.437; P < 0.001) and N-staging (P = 0.006). In all 15 patients with early-stage NPC, [18F]RCCB6 immuno-PET/CT achieved a 100% detection rate of the primary tumor and a 93% detection rate (75/81) of local lymph node metastasis. [18F]RCCB6 uptake correlated well with CD70 expression. In a head-to-head comparison, [18F]RCCB6 demonstrated higher sensitivity than did 18F-FDG in detecting lymph node metastasis (100% [58/58] vs. 90% [52/58], respectively; P = 0.031), and equivalent detection abilities for primary lesions and most distant metastases (100%). Notably, [18F]RCCB6 immuno-PET/CT demonstrated better evaluation of skull-base invasion with a clear border and bone metastases, as indicated by its higher uptake compared with 18F-FDG (7.25 vs. 5.95; P = 0.025). Conclusion: CD70 is a potent biomarker for NPC. [18F]RCCB6 immuno-PET/CT provides precise mapping of CD70 expression and enhances the diagnosis of primary, metastatic, and recurrent NPCs, outperforming 18F-FDG in detecting skull-base invasion and metastases.
Nasopharyngeal carcinoma (NPC) is a cancer associated with Epstein-Barr virus (EBV) infection (1). Various risk factors, including EBV infection, jointly contribute to the pathogenesis and development of NPCs (2). Currently, MRI, CT, and 18F-FDG PET/CT are regularly used to diagnose and stage NPCs. Although MRI is favored for assessing primary tumor extension and infiltration, 18F-FDG PET/CT can detect both primary and metastatic NPCs with higher accuracy. The combined use of MRI and 18F-FDG PET/CT is generally recommended for patients with advanced NPCs. NPCs are highly sensitive to ionizing radiation; therefore, radiotherapy is the primary treatment option for nonmetastatic NPCs. Practical challenges in precisely delineating clinical target volumes and organs at risk necessitate the development of dedicated molecular imaging approaches that facilitate more-accurate delineation. Concurrent chemoradiotherapy and induction chemotherapy are used for locoregionally advanced or metastatic diseases. Among the active research directions in the field of NPCs, the development of novel biomarker-driven molecular imaging and staging strategies, as well as paratactic therapeutics, is of great clinical significance.
CD70 is a member of the tumor necrosis factor superfamily, and it is highly expressed in a small subgroup of activated memory T and B cells under normal conditions (3). CD70 is a ligand for CD27, and this interaction plays a crucial role in regulating the immune system. The CD70–CD27 interaction promotes the development of regulatory T cells. CD70 is highly expressed in various solid tumors, especially in clear cell renal cell carcinoma (ccRCC) and NPC (4–7). CD70 is crucial in the immune response to EBV infection, and positive expression of CD70 by NPC cells has been significantly correlated with EBV infection (8). The CD70–CD27 interaction provides a necessary costimulatory signal that enhances the proliferation of EBV-specific T cells, which are essential for controlling EBV infection (9). Inherited CD70 deficiency can severely impair the immune system’s ability to fight EBV, leading to chronic or severe EBV-related disease. The expression of CD70 is regulated at both the translational and transcriptional levels. Past studies have found that latent membrane protein 1 induces the expression of CD70 in NPC (10,11), and a recent study demonstrated that NFKB2 transcriptionally regulates CD70 in NPC via an EBV-dependent epigenetic modification (12). Unlike this regulatory mechanism, CD70 expression in ccRCC is primarily controlled by the α-subunit of hypoxia-inducible factor 1 (13,14).
CD70 is being actively explored for use in the development of anticancer therapeutics. Antibody therapeutics (e.g., cusatuzumab, SGN-CD70A) and chimeric antigen receptor T-cell immunotherapies (e.g., CTX130, CTX131) are being actively investigated in ongoing clinical trials (15–17). Cusatuzumab is a CD70-specific humanized monoclonal antibody of camelid origin, exhibiting a favorable safety profile in solid tumors and hematologic malignancies (18–20). However, clinicians face challenges in accurately assessing heterogeneous CD70 expression before and after the use of CD70-targeted antibody and cell therapies. In response to this challenge, we recently reported the preclinical development and clinical translation of CD70-targeted single-domain antibody tracers. Pilot clinical use of the tracers demonstrated superior diagnostic value in patients with metastatic ccRCCs (6,21–23). Although CD70-targeted immuno-PET/CT imaging might change the diagnostic landscape of ccRCC (24,25), its diagnostic efficacy in other tumors remains unknown.
In this study, we determine the expression of CD70 in archived NPC specimens and explore the diagnostic value of [18F]RCCB6 immuno-PET/CT in patients with NPC.
MATERIALS AND METHODS
All materials and methods are described in the supplemental materials, available at http://jnm.snmjournals.org (6,21–23).
RESULTS
Patient Cohorts and CD70 Expression Patterns in NPC Specimens
This study retrospectively analyzed the clinical data of 80 NPC patients treated in our radiotherapy department from December 2017 to December 2024 (Table 1). CD70 expression was positive in 72 patients (90%), with nonkeratinizing squamous cell carcinoma being the predominant pathologic type (98% of patients). Normal nasopharyngeal tissues did not express CD70, and representative CD70 expression patterns in different pathologic types are illustrated in Figure 1A. CD70 expression significantly correlated with the N category, with advanced N categories (N2–N3) showing higher positivity (3% negative, 59% low, and 37% high) compared with early N categories (N0–N1) (29% negative, 38% low, and 33% high) (P = 0.006) (Fig. 1B). No significant correlations were observed with T category (P = 0.674) (Fig. 1B), M category (P = 0.768), or overall disease stage (P = 0.550).
Relationship Between CD70 Expression and Clinical Characteristics

CD70 expression in NPC. (A) Representative images illustrating CD70 expression in NPC, with examples of both positive and negative staining across various pathologic types. (B) Percentage profile of CD70 expression levels in patients with NPC, stratified by N and T categories. (C) Correlation analysis of CD70 immunohistochemistry (IHC) scores with EBV DNA copies and Ki-67 proliferation index. KSCC = keratinizing squamous cell carcinoma; NKSCC = nonkeratinizing squamous cell carcinoma.
A positive correlation was found between pretreatment EBV DNA copies and CD70 immunohistochemistry scores (rs = 0.437; P < 0.001) (Fig. 1C). In contrast, Ki-67 proliferation index showed no correlation with CD70 expression (rs = 0.110; P = 0.524) (Fig. 1C). Moreover, progression-free survival analysis of 48 patients who underwent radiotherapy revealed no significant difference among patients with varying CD70 expression levels (P = 0.667) (Supplemental Fig. 1). These findings highlight CD70 as a robust biomarker for NPC, particularly in advanced N categories and EBV-associated disease. Its consistent expression across disease stages and correlation with EBV viral load underscore the potential of CD70 as a diagnostic and therapeutic target.
Distribution and Threshold Value of [18F]RCCB6 in Patients with NPC
The study flowchart for the [18F]RCCB6 immuno-PET/CT imaging in the study is depicted in Figure 2. In this CD70-targeted clinical trial, 25 patients with NPC were stratified into 4 cohorts: early-stage NPC (initial diagnosis without distant metastasis) (n = 15), advanced NPC (with distant metastasis (n = 3), recurrent NPC (n = 4), and follow-up group (lesion-free) (n = 3), with administered activity and characteristics detailed in Supplemental Tables 1 and 2. The representative maximum-intensity projection image of [18F]RCCB6 immuno-PET/CT imaging in patient 10 is presented in Supplemental Figure 2A, demonstrating prominent renal accumulation (SUVmax, 150.50 ± 34.250) due to tracer excretion. Minimal uptake was observed in brain (0.688 ± 0.173), lung (0.634 ± 0.155), and muscle (0.551 ± 0.150) (Supplemental Fig. 2B). By analyzing the [18F]RCCB6 immuno-PET/CT imaging results in patients without NPC at our center, we calculated the mean SUVmax for thresholds to be 1.981 for normal nasopharynx and 1.634 for normal cervical lymph nodes. The low background uptake of [18F]RCCB6 lays the foundation for the precise identification of skull-base invasion and diverse metastases.

Flowchart of study design. Patients with NPC undergoing [18F]RCCB6 immuno-PET/CT imaging (n = 25) were included; 14 underwent 18F-FDG PET/CT imaging for head-to-head comparison.
[18F]RCCB6 Immuno-PET/CT Imaging in Patients with Early-Stage NPC
[18F]RCCB6 immuno-PET/CT demonstrated high detection rates for primary tumors in all in all 15 patients with early-stage NPC (100%) and in 75 (93%) of 81 lesions with lymph node metastases. Additionally, [18F]RCCB6 detected all 5 MRI-confirmed skull-base invasions without interference from tracer uptake in the brain. The calculated median SUVmax for primary lesions was 8.11 (interquartile range [IQR], 11.21 − 4.84), whereas the corresponding SUVmax for local lymph node metastases was 7.46 (IQR, 10.00 − 4.17). Patients with and without cervical lymph node metastases showed no statistically significant difference in tracer uptake in primary lesions (8.19 vs. 6.26; P > 0.999). The median SUVmax for primary tumors in patients with NPC (P < 0.001) and cervical lymph node involvement (P < 0.001) were significantly higher than the established threshold.
Due to its negligible uptake in the brain, [18F]RCCB6 exhibited a distinct advantage in detecting skull-base invasion by the primary tumor, as illustrated by [18F]RCCB6 immuno-PET/CT images in patient 3 with nonkeratinizing squamous cell carcinoma (Fig. 3A). In patient 5, [18F]RCCB6 immuno-PET/CT detected both the primary tumor and local lymph node metastases, consistent with MRI and 18F-FDG PET/CT findings (Fig. 3B; Supplemental Fig. 3). Both patients showed positive CD70 expression, with the former case showing more intense and uniform CD70 expression (Supplemental Fig. 4). Overall, [18F]RCCB6 immuno-PET/CT demonstrates high diagnostic accuracy for early-stage NPCs, especially in delineating skull-base invasion, underscoring its application value in NPC patients.

[18F]RCCB6 immuno-PET/CT imaging in patients with early-stage NPC. (A) Maximum intensity projection (MIP), CT, and fused PET/CT images of [18F]RCCB6 in patient 3, showing skull-base invasion (SBI) (green arrowhead), cervical lymph node metastases (LNM) (yellow arrowheads), and nonspecific uptake in left eighth thoracic vertebra (black arrowhead). (B) MIP, CT, and fused PET/CT images of [18F]RCCB6 in patient 5, revealing primary tumor (PT) (red arrowhead) and LNM (yellow arrowhead).
[18F]RCCB6 Immuno-PET/CT Imaging in Patients with Advanced NPC
We further evaluated the diagnostic efficacy of [18F]RCCB6 immuno-PET/CT imaging in 3 patients with NPC with distant metastases. For these 3 patients, 93 metastatic lesions were analyzed in the lesion-based analysis, revealing varying [18F]RCCB6 uptake values in different metastases: 4.00 for distant lymph node metastases (IQR, 5.20–2.80; n = 19), 6.60 for liver metastases (IQR, 8.50–5.175; n = 18), 4.30 for lung metastases (IQR, 5.60–1.30; n = 15), and 8.00 for bone metastases (IQR, 11.96–4.835; n = 41). No significant difference in uptake in cervical lymph node metastases was observed between early-stage and advanced NPCs (7.70 vs. 7.46, respectively; P = 0.816). The superior target-to-background contrast of [18F]RCCB6 immuno-PET/CT imaging allows for precise delineation of spatially heterogeneous metastatic lesions. For instance, patient 20 demonstrated multiple metastatic lesions in the bone, liver, and lung, accompanied by distant lymph node involvement, with biodistribution patterns comparable to those observed with 18F-FDG PET/CT (Figs. 4A and 4B).

[18F]RCCB6 and 18F-FDG PET/CT imaging in patient with advanced NPC. (A) [18F]RCCB6 immuno-PET/CT images showing primary NPC (red arrowhead) and multiple systemic metastases, including cervical lymph nodes (yellow arrowheads), bone (green arrowhead), lung (orange arrowhead), liver (blue arrowhead), and Omental bursa lymph nodes (pink arrowhead) in patient 20. (B) 18F-FDG PET/CT images of same patient, demonstrating corresponding lesions.
[18F]RCCB6 Immuno-PET/CT Imaging in Patients with Recurrent NPC
[18F]RCCB6 immuno-PET/CT effectively identified recurrent NPC lesions in all 4 patients, with 2 patients having nasopharyngeal recurrence and 1 patient having cervical lymph node recurrence. One patient had a concomitant recurrence in the nasopharynx and lymph node. The primary tumor and bilateral cervical lymph node metastases of patient 25 were eradicated by concurrent chemoradiotherapy. The patient then presented with epistaxis, indicating a recurrence of the disease. Both 18F-FDG PET/CT and [18F]RCCB6 immuno-PET/CT identified nasopharyngeal recurrence infiltrating the ethmoid sinus, with the latter imaging approach enabling a more-confident diagnosis (Figs. 5A and 5B; Supplemental Fig. 5). Moreover, [18F]RCCB6 immuno-PET/CT accurately excluded suspected tumor recurrence indicated by MRI in patient 10. The pathology confirmed nasopharyngeal inflammation with negative CD70 expression, whereas the staining of the primary tumor collected at baseline demonstrated prominent CD70 expression (Supplemental Fig. 6). These cases demonstrate the value of [18F]RCCB6 immuno-PET/CT in accurately detecting recurrent NPC and excluding false-positive findings on MRI, particularly in cases of diagnostic dilemmas and suspected disease recurrence.

Dynamic changes in primary lesion and lymph node metastases in patient with recurrent NPC. (A) 18F-FDG PET/CT images at initial diagnosis revealing primary lesion (red arrowhead) infiltrating ethmoid sinus (green arrowhead) with bilateral lymph node metastases (yellow arrowheads) in patient 25. (B) Dual-tracer PET/CT images after concurrent chemoradiotherapy (CCRT) identifying nasopharyngeal recurrence (red arrowhead) infiltrating ethmoid sinus (green arrowhead) and regression of previously metastatic lymph nodes.
Comparison of [18F]RCCB6 Immuno-PET/CT with 18F-FDG PET/CT
We compared the differential diagnostic efficacies of [18F]RCCB6 immuno-PET/CT and 18F-FDG PET/CT in 14 patients with dual-tracer imaging within 2 wk. In general, [18F]RCCB6 immuno-PET/CT demonstrated noninferior diagnostic performance to 18F-FDG PET/CT across all categories, achieving identical detection rates (100%) for primary tumors (n = 13), bone (n = 20), liver (n = 5), lung (n = 15), and distant lymph node metastases (n = 6). Notably, [18F]RCCB6 showed higher sensitivity in detecting lymph node metastasis (100% [58/58] vs. 90% [52/58]; P = 0.031). [18F]RCCB6 showed statistically lower uptake than 18F-FDG in the primary lesions (8.51 vs. 15.89; P = 0.030), lung metastases (4.30 vs. 13.50; P < 0.001), and distant lymph node metastases (4.85 vs. 12.70; P = 0.031). However, we found higher uptake of [18F]RCCB6 than 18F-FDG in bone metastases (7.25 vs. 5.95; P = 0.025). In contrast, uptake of the 2 tracers was comparable in cervical lymph node metastases (7.90 vs. 7.55; P = 0.173) and liver metastases (6.10 vs. 7.50; P = 0.125), suggesting heterogeneous CD70 expression across metastases and the unique value of [18F]RCCB6 immuno-PET/CT in mapping differential expression patterns (Fig. 6A).

Comparative analysis of [18F]RCCB6 and 18F-FDG PET/CT imaging in patients with NPC, showing SUVmax in primary tumor (PT), bone metastasis (BM), pulmonary metastasis (PM), liver metastasis (LM), cervical lymph node metastasis (CLNM), and distant lymph node metastasis (DLNM). (A) Head-to-head comparison of [18F]RCCB6 and 18F-FDG uptake in terms of SUVmax in primary and metastatic lesions. (B) Histopathologic analyses of PTs, confirming positive CD70 expression, in patients 1 and 14. (C) 18F-FDG and [18F]RCCB6 PET/CT images of patient 1, showing primary lesion infiltrating skull base (red arrowhead) and bone metastases with higher [18F]RCCB6 uptake (green arrowhead). (D) 18F-FDG PET/CT, [18F]RCCB6 PET/CT, and MR images of patient 14, highlighting primary lesion (red arrowhead), lymph nodes detected by both tracers (yellow arrowhead), and lymph nodes detected only by [18F]RCCB6 (blue and pink arrowheads). MRI-confirmed regression of lymph node marked by blue arrowhead. T1-CE = T1-weighted contrast-enhanced.
Patients 1 and 14 had pathologically diagnosed NPC with positive CD70 expression (Fig. 6B). Dual-tracer PET imaging of patient 1 showed the advantages of [18F]RCCB over 18F-FDG in precisely outlining the boundary of the skull-base invasion and in detecting distant metastases, especially occult bone metastases (Fig. 6C). Dual-tracer PET imaging of patient 14 showed the advantage of [18F]RCCB over 18F-FDG in detecting more metastatic cervical lymph nodes, and follow-up MRI showed shrinkage of the lymph nodes after therapy (Fig. 6D). With minimal physiologic uptake and the resultant clear background, [18F]RCCB immuno-PET/CT showed superior diagnostic contrast compared with that achieved with 18F-FDG PET/CT. However, the property of enlarged lymph nodes with [18F]RCCB6 uptake requires validation in extended follow-up. The full diagnostic and predictive value of [18F]RCCB6 needs to be validated in larger, well-characterized patient cohorts in subsequent clinical investigations.
DISCUSSION
Biomarker-derived cancer theranostics is continuously shaping the management landscape of human malignancies, such as prostate cancer and neuroendocrine tumors (26,27). CD70 is an emerging biomarker for solid tumors and hematologic malignancies (28). We previously reported the high expression of CD70 in ccRCC and developed a series of single-domain antibody–derived immuno-PET/CT imaging tracers (6,21,22). CD70-targeted immuno-PET/CT imaging accurately detects metastatic ccRCCs, especially occult metastases in the muscle, pancreas, adrenal gland, bone, lymph nodes, brain, and meninges. [18F]RCCB6 immuno-PET/CT enables whole-body CD70 visualization, CD70-driven patient selection, and response monitoring, with potential utility in postoperative follow-up to monitor recurrence and metastasis. The routine clinical application of CD70-targeted immuno-PET/CT imaging may improve the management of patients with ccRCC. In this setting, actively exploring the potential of CD70-targeted tracers in other tumors may further broaden the value of the cutting-edge imaging approaches.
The current study further indicates the viability of CD70 as a diagnostic biomarker for NPC and demonstrates that [18F]RCCB6 immuno-PET/CT can detect both primary and metastatic NPCs, with minimal uptake in normal tissues and organs, except the kidneys, which are involved in excretion. Based on our results, CD70 expression increases with the progression of lymph node metastasis. However, further validation in larger cohorts is necessary to confirm these findings. A notable observation suggests that a higher EBV viral load is associated with increased expression of CD70. Although the role of EBV infection has been extensively studied, the role of CD70 in the pathogenesis and progression of NPC remains unclear, underscoring the need for further basic research to elucidate its underlying functions.
From a diagnostic perspective, the diagnosis and staging of NPCs rely on MRI and 18F-FDG PET/CT. The TNM classification for EBV-related NPC is undergoing rapid evolution. For instance, a recent report proposes reclassifying T3 NPC with early skull-base invasion as T2 and elevating N1−N2 NPC with grade 3 extranodal extension identified by medical imaging to N3. Metastatic NPC is classified as M1a (1 − 3 metastatic lesions without liver involvement) and M1b (>3 metastatic lesions or with liver involvement) (29). Since the first reports of 18F-FDG PET imaging in NPC were published (30,31), accumulating evidence has established the diagnostic and surveillance value of 18F-FDG PET/CT in patients with NPC (32–34). However, the physiologic uptake of 18F-FDG in inflammatory nasopharyngeal mucosa and lymph nodes apodictically affects the reading of the imaging findings. Progress has been made to overcome the inherited shortages of 18F-FDG PET/CT (35–38). However, molecular imaging tracers with high diagnostic accuracy are still needed for NPCs, particularly those targeting biomarkers with therapeutic or theranostic potential. Here, we have proposed and validated the value of CD70-targeted [18F]RCCB6 immuno-PET/CT in primary and metastatic NPCs. The minimal physiologic uptake in normal organs, including the brain and nasopharynx, leads to accurate identification of tumor residues, tumor recurrence, infiltration of the skull base, and local lymph node metastases. As is well known, MRI is superior to 18F-FDG PET/CT in identifying T categories, and the combined use of MRI and 18F-FDG PET/CT can significantly improve the long-term prognostic stratification of patients with NPC (39). It remains to be determined whether [18F]RCCB6 PET/MR has additional diagnostic value than [18F]RCCB6 immuno-PET/CT in this population.
From a therapeutic perspective, external beam radiotherapy and chemotherapy (concurrent chemoradiotherapy and induction chemotherapy) are the backbones of treatment for patients with NPCs. Meanwhile, the use of other radiotherapy options, including intensity-modulated radiotherapy, volumetric-modulated arc therapy, and TomoTherapy (Accuray), as well as immunotherapy, has been increased. The delineation of skull-base target volumes in NPC radiotherapy relies on multimodal imaging to define high-risk regions and optimize the therapeutic margins (40). [18F]RCCB6 immuno-PET/CT may facilitate the precise drawing of clinical target volumes and contouring while sparing organs at risk, particularly in complex anatomic zones adjacent to critical neural structures. We believe that [18F]RCCB6 immuno-PET/CT has the potential to enhance the clinical application of advanced radiotherapies for NPCs, given its minimal physiologic uptake. However, further studies are needed to support this hypothesis. Along with this progress, targeting CD70 to eliminate CD70-positive tumor cells or to block the CD70–CD27 signaling axis was a possible direction for treating CD70-positive tumors. CD70-specific therapeutic monoclonal antibodies, antibody–drug conjugates, and chimeric antigen receptor T-cell therapies have entered clinical trials (41–43). Of the various treatment options, CD70-targeted antibody therapeutics might reduce immunosuppression by regulatory T cells and eradicate CD70-expressing NPC cells (12). The inconsistent expression of CD70 in primary and metastatic tumors can lead to inaccurate patient selection when using traditional immunohistochemistry staining methods, resulting in unsatisfactory outcomes for CD70-targeted therapies. In this setting, the adaptation of the [18F]RCCB6 immuno-PET/CT imaging approach may enhance treatment outcomes by facilitating more-accurate patient selection and the timely assessment of treatment responses.
Finally, the development of CD70-specific therapeutic radiopharmaceuticals may further enrich the treatment options for CD70-positive tumors. However, efforts are still needed to balance treatment efficacy and toxicity, particularly nephrotoxicity, for radiopharmaceuticals derived from a single-domain antibody (44,45). Half-life extension modification and enhanced clearance strategies may partially address some of the existing bottlenecks (46). However, the development of CD70-targeted therapeutic radiopharmaceuticals that balance treatment efficacy with manageable side effects is still needed. Clinical trials thoroughly investigating [18F]RCCB6 immuno-PET/CT in NPCs will establish the clinical value of this approach and guide the use of CD70-targeted therapeutics.
CONCLUSION
CD70-targeted [18F]RCCB6 immuno-PET/CT imaging accurately detects primary and metastatic NPCs, potentially improving disease management by optimizing subsequent CD70-targeted or systemic treatments. Further studies are needed to unleash the theranostic potential of CD70-targeted radiopharmaceuticals.
DISCLOSURE
This work was partially supported by the National Natural Science Foundation of China (grant 82372014). No other potential conflict of interest relevant to this article was reported.
KEYPOINTS
QUESTION: Can we develop a cutting-edge immuno-PET/CT imaging approach for NPC?
PERTINENT FINDINGS: CD70 is highly and constantly expressed in NPCs, with a positive rate of 90%. Positive expression of CD70 is associated with EBV infection and the advanced N category of NPCs. CD70-targeted [18F]RCCB6 immuno-PET/CT accurately detects local and metastatic NPCs, with minimal uptake in normal tissues and organs, facilitating a more-accurate assessment of tumor burdens.
IMPLICATIONS FOR PATIENT CARE: CD70-specific [18F]RCCB6 immuno-PET/CT imaging enables the precise diagnosis and stratification of patients with NPCs, potentially improving disease management by optimizing subsequent CD70-targeted or systemic treatments.
Footnotes
Published online Apr. 30, 2025.
- © 2025 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication January 25, 2025.
- Accepted for publication April 8, 2025.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.