


Visual Abstract

Abstract
Eighty percent of colorectal cancers (CRCs) overexpress epidermal growth factor receptor (EGFR). Kirsten rat sarcoma viral oncogene (KRAS) mutations are present in 40% of CRCs and drive de novo resistance to anti-EGFR drugs. BRAF oncogene is mutated in 7%–10% of CRCs, with even worse prognosis. We have evaluated the effectiveness of [225Ac]Ac-macropa-nimotuzumab in KRAS mutant and in KRAS wild-type and BRAFV600E mutant EGFR-positive CRC cells in vitro and in vivo. Anti-CD20 [225Ac]Ac-macropa-rituximab was developed and used as a nonspecific radioimmunoconjugate. Methods: Anti-EGFR antibody nimotuzumab was radiolabeled with 225Ac via an 18-membered macrocyclic chelator p-SCN-macropa. The immunoconjugate was characterized using flow cytometry, radioligand binding assay, and high-performance liquid chromatography, and internalization was studied using live-cell imaging. In vitro cytotoxicity was evaluated in 2-dimensional monolayer EGFR-positive KRAS mutant DLD-1, SW620, and SNU-C2B; in KRAS wild-type and BRAFV600E mutant HT-29 CRC cell lines; and in 3-dimensional spheroids. Dosimetry was studied in healthy mice. The in vivo efficacy of [225Ac]Ac-macropa-nimotuzumab was evaluated in mice bearing DLD-1, SW620, and HT-29 xenografts after treatment with 3 doses of 13 kBq/dose administered 10 d apart. Results: In all cell lines, in vitro studies showed enhanced cytotoxicity of [225Ac]Ac-macropa-nimotuzumab compared with nimotuzumab and controls. The inhibitory concentration of 50% in the DLD-1 cell line was 1.8 nM for [225Ac]Ac-macropa-nimotuzumab versus 84.1 nM for nimotuzumab. Similarly, the inhibitory concentration of 50% was up to 79-fold lower for [225Ac]Ac-macropa-nimotuzumab than for nimotuzumab in KRAS mutant SNU-C2B and SW620 and in KRAS wild-type and BRAFV600E mutant HT-29 CRC cell lines. A similar trend was observed for 3-dimensional spheroids. Internalization peaked 24–48 h after incubation and depended on EGFR expression. In the [225Ac]Ac-macropa-nimotuzumab group, 3 of 7 mice bearing DLD-1 tumors had complete remission. Median survival was 40 and 34 d for mice treated with phosphate-buffered saline and [225Ac]Ac-macropa-rituximab (control), respectively, whereas it was not reached for the [225Ac]Ac-macropa-nimotuzumab group (>90 d). Similarly, median survival of mice bearing HT-29 xenografts was 16 and 12.5 d for those treated with [225Ac]Ac-macropa-rituximab and phosphate-buffered saline, respectively, and was not reached for those treated with [225Ac]Ac-macropa-nimotuzumab (>90 d). One of 7 mice bearing HT-29 xenografts and treated using [225Ac]Ac-macropa-nimotuzumab had complete remission. Compared with untreated mice, [225Ac]Ac-macropa-nimotuzumab more than doubled (16 vs. 41 d) the median survival of mice bearing SW620 xenografts. Conclusion: [225Ac]Ac-macropa-nimotuzumab is effective against KRAS mutant and BRAFV600E mutant CRC models.
Overexpression of epidermal growth factor receptor (EGFR) I is associated with most aggressive cancers of epithelial origin, particularly in 80%–85% of colorectal cancers (CRCs) (1). Mutations in EGFR, such as Kirsten rat sarcoma viral oncogene (KRAS), lead to constitutive overactivation of the receptor and hence resistance to anti-EGFR treatments. KRAS is an intracellular effector molecule that routes ligand-bound EGFR to the nucleus, where it stimulates proliferation (2–4). B-rapidly accelerated fibrosarcoma murine sarcoma viral oncogene homolog B (BRAF) is a serine–threonine protein kinase that causes enhanced proliferation in EGFR-positive CRC cells (5,6). BRAFV600E is the most common BRAF mutation in EGFR-positive CRC cells (5,6).
Metastatic CRC (mCRC) is the second leading cause of death from cancer, with a 5-y survival rate of less than 10% (stage IV) (7), likely because more than 45% of CRC patients have metastatic disease at initial diagnosis. Surgery, which is a primary treatment option, is contraindicated in patients with advanced disease, and even when it is possible, the local recurrence rate is high (38%–88%) (8). In EGFR-positive mCRC patients with KRAS wild-type mutation, the addition of anti-EGFR antibodies (e.g., cetuximab) to chemotherapy results in small—albeit significant—improvements in survival, but there is no benefit in patients with KRAS and BRAF mutations (9). Mutations in KRAS occur in up to 40% of CRCs, whereas BRAF mutations are present in 7%–10% of CRCs (5). The concurrent presence of KRAS and BRAFV600E mutations has not been observed in the same patient (10). However, BRAFV600E and other BRAF mutations occur in patients with KRAS wild-type cancers and have been associated with even worse prognosis in CRCs (11). EGFR-positive mCRCs (especially those with KRAS and BRAF mutations) represent an unmet clinical need.
Anti-EGFR antibodies—for example, cetuximab, panitumumab, and nimotuzumab—are used to treat EGFR-positive cancers, including CRC. With the exception of nimotuzumab, anti-EGFR antibodies have been associated with significant cutaneous toxicity in 45%–100% of patients (12). In contrast, nimotuzumab is better tolerated and has low skin toxicities, because its affinity-optimized binding characteristics ensure low transient binding to low EGFR–expressing healthy tissues, such as the skin and intestinal mucosa.
High linear energy transfer makes α-emitting radionuclides the ideal isotopes for targeted radiopharmaceutical therapy of metastatic disease. α-emitters such as 213Bi- and 225Ac-labeled agents have shown promising results in preclinical and clinical studies in ovarian cancer, neuroendocrine tumors, breast cancer, and prostate cancer (13–16). The characteristics of 225Ac—a half-life of 10.0 d, energy range of 6–8 MeV (cumulative emission of 28 MeV/decay) with the emission of 4 αs (range, 50–80 µm), and 3 β− emissions with linear energy transfer of up to 0.16 MeV/µm—make it an ideal isotope for radioimmunotherapy.
We describe the use of [225Ac]Ac-macropa-nimotuzumab for radioimmunotherapy of KRAS mutant and of KRAS wild-type and BRAFV600E mutant CRC models. We evaluate the in vitro (2-dimensional [2D] cell culture and 3-dimensional [3D] spheroid models) and in vivo characteristics and the in vivo effectiveness of [225Ac]Ac-macropa-nimotuzumab in these models with different numbers of EGFR copies per cell.
MATERIALS AND METHODS
Conjugation, Quality Control of Immunoconjugates, and Internalization
The conjugation and in vitro characterization of nimotuzumab and of nonspecific control IgG anti-CD20 rituximab to 6-((16-((6-carboxypyridin-2-yl)methyl)-1,4,10,13-tetraoxa-7,16-diazacyclooctadecan-7-yl)methyl)-4-isothiocyanatopicolinic acid (p-SCN-macropa) are provided in supplemental materials (supplemental materials are available at http://jnm.snmjournals.org) (17). All cell lines were obtained from the American Type Culture Collection. DLD-1, SNU-C2B, and SW620 are KRAS mutant cells with KRASG13D, KRASG12D, and KRASG12V mutations, respectively, whereas HT-29 is a KRAS wild-type but BRAFV600E mutant CRC cell line (18,19).
Radiolabeling and Quality Control
p-SCN-macropa–conjugated nimotuzumab or rituximab was radiolabeled using 225Ac-nitrate dissolved in 0.1 M hydrogen chloride (Optima grade; Fisher Scientific) at a targeted specific activity of 10 kBq/µg, as reported (20). Quality control and purification were done after labeling, following lab standard operating procedures (20). Radioligand binding assay was studied in DLD-1 cells as described previously (20).
Cytotoxicity in 2D Monolayer and 3D Spheroids
The in vitro cytotoxicity of [225Ac]Ac-macropa-nimotuzumab was studied in 2D monolayer cultures and 3D spheroids using the Incucyte S3 live-cell imaging system (Essen BioScience) in DLD-1, SNU-C2B, HT-29, and SW620 CRC cell lines. The details are provided in the supplemental materials (21).
Biodistribution, Dosimetry, and In Vivo Toxicity
To estimate radiation dose to organs, healthy BALB/c mice were administered 13 kBq of 225Ac-nimotuzumab via a tail vein and euthanized 1, 24, 48, 120, or 264 h after injection, followed by biodistribution studies. Carcasses were collected and analyzed using a γ-counter, and activity was expressed as percentage injected activity (%IA) and %IA per gram organ weight (%IA/g). The mouse biodistribution (%IA/g) data were extrapolated to human data (%IA) using the following formula: %IA (human) = %IA/g (mouse) × total body weight of mouse (in kilograms) × mass of human organ (in grams) per total body weight of human (in kilograms). For each organ, this was plotted against sampling time and used to obtain an estimate of the residence time (in megabecquerel hours per megabecquerel) of the agent in the organ, represented by the area under the time–activity function integrated to infinity (complete decay) of the 225Ac. The residence time was fitted into the OLINDA kinetics model (OLINDA/EXM version 2.2; Hermes Medical Solutions) to generate absorbed doses in units of centigray per millicurie of 225Ac administered.
Biodistribution of 225Ac-nimotuzumab was also studied in athymic nude BALB/c mice bearing EGFR-positive DLD-1 xenografts. Animals (n = 4/group) were administered 13 kBq of [225Ac]Ac-macropa-nimotuzumab and euthanized 24, 72, 120, or 288 h after injection. Organs were harvested for biodistribution studies and expressed as %IA/g. Toxicity was also studied in healthy BALB/c mice and is reported in the supplemental materials.
Radioimmunotherapy
Biodistribution of [225Ac]Ac-macropa-nimotuzumab showed clearance from almost all organs after 10 d, with retention in tumors. For in vivo α-particle therapy, mice were divided into 3 groups (n ≥ 5/group): [225Ac]Ac-macropa-nimotuzumab, [225Ac]Ac-macropa-rituximab, and phosphate-buffered saline (PBS). Mice received 3 doses of 13 kBq (39 kBq in total) administered on days 0, 10, and 20 via a tail vein. Tumor growth was monitored by measuring the greatest length and width of each tumor using a digital caliper. Tumor volume was calculated using the following formula: volume = (length × width2)/2. At the start of the study, tumor volumes for DLD-1, HT-29, and SW620 were not statistically different among the groups treated with [225Ac]Ac-macropa-nimotuzumab, [225Ac]Ac-macropa-rituximab, and PBS (P > 0.05). Initial tumor volumes ± SEM for the [225Ac]Ac-macropa-nimotuzumab, [225Ac]Ac-macropa-rituximab, and PBS groups were 153.2 ± 73.3, 67.9 ± 3.8, and 149.3 ± 19.3 mm3 for DLD-1 xenografts; 129.2 ± 40.3, 188 ± 86, and 119.8 ± 65.9 mm3 for HT-29 xenografts; and 39.2 ± 21.3, 73.4 ± 63.9, and 33.8 ± 58.67 mm3 for SW620 xenografts, respectively. The study was terminated when tumor volume reached at least 1,500 mm3, and then survival was determined using a Kaplan–Meier curve. The individual body weights of mice were recorded during the study period.
Statistical Analysis
All data were expressed as the mean ± SEM of at least 3 independent experiments. Comparisons between groups were performed via either Student t test with Welch correction (2-group comparison) or 1-way ANOVA with Bonferroni multiple comparison post hoc test (multiple-group comparison). Graphs were prepared and P values were calculated using GraphPad Prism (version 9; GraphPad Software).
Ethics Statement
All animal studies were approved by the University of Saskatchewan Animal Care and Use Committee protocol 20220021.
RESULTS
Quality Control
The conjugation of p-SCN-macropa to nimotuzumab or control antibody rituximab was obtained as a clear solution with no particulate matter or milky appearance. The high-performance liquid chromatography purity of macropa-nimotuzumab and macropa-rituximab was at least 98%. Immunoconjugates were further characterized for binding to EGFR, aggregation, and size (Supplemental Figs. 1 and 2; Supplemental Table 1). Bioanalyzer showed that macropa-nimotuzumab was more than 86% pure, with a molecular weight of 162.8 kDa (vs. 161.2 kDa for nimotuzumab). This indicates that there were an estimated 3 macropa per antibody molecule. Saturation binding of nimotuzumab to EGFR on DLD-1, SNU-C2B, HT-29, and SW620 cells was studied using flow cytometry (Supplemental Fig. 3). The dissociation constant and the maximum specific binding were 5.6 ± 0.06 nM and 610,576 for DLD-1, 20.1 ± 0.73 nM and 321,040 for SNU-C2B, 6.4 ± 1.6 nM and 1,484,086 for HT-29, and 5.4 ± 2.4 nM and 43,518 for SW620 cell lines, respectively.
Radiolabeling, Characterization, and Internalization
Macropa-nimotuzumab and control immunoconjugate macropa-rituximab were quantitatively radiolabeled using 225Ac (>90% radiochemical yield) and in high radiochemical purity (>99% in each case) at a specific activity of 10 kBq/µg. The purity was confirmed by instant thin-layer chromatography and high-performance liquid chromatography (Supplemental Figs. 2C and 2D).
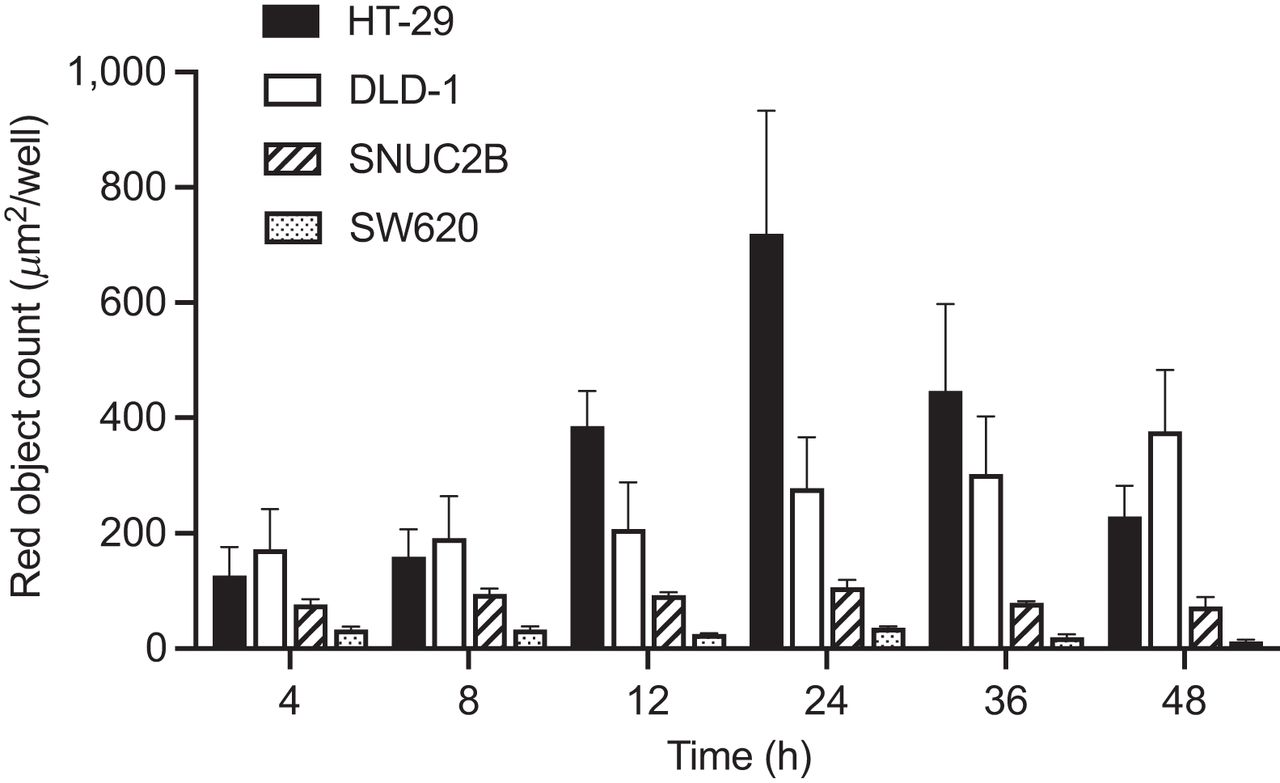
Internalization efficiency of nimotuzumab compared with control IgG was estimated by total red counts observed at the end of 48 h after treatment. In all cell lines except for DLD-1, internalization peaked at 24 h and depended on EGFR expression on the surface of the cell (Fig. 1). At 48 h after incubation, the internalization of nimotuzumab in DLD-1 (376.82 ± 106.5, high EGFR expression) was 30.9 times greater than in SW620 (12.18 ± 3.28, low EGFR expression). Similarly, at 24 h, nimotuzumab was 20 times more internalized in HT-29 (719.21 ± 213.5, high EGFR expression) than in SW620 (35.98 ± 3.095, low EGFR expression).

Internalization of nimotuzumab in DLD-1, SNU-C2B, HT-29, and SW620 cell lines at different time points after incubation using live-cell imaging. All data shown are mean of 3 wells ± SEM.
The binding of [225Ac]Ac-macropa-nimotuzumab to the EGFR-positive DLD-1 cell line was studied using radioligand binding assay. The estimated dissociation constant and maximum specific binding were 14.8 ± 41.7 nM and 10,050, respectively (Supplemental Fig. 4).
In Vitro Cytotoxicity (2D and 3D Spheroids)
Live-cell imaging was used to study the in vitro cytotoxicity (2D cells) of nimotuzumab and [225Ac]Ac-macropa-nimotuzumab in DLD-1, SW620, SNU-C2B, and HT-29 mCRC cells (Table 1; Supplemental Figs. 5 and 6). Despite the low specific activity, [225Ac]Ac-macropa-nimotuzumab was more potent than unlabeled nimotuzumab. In DLD-1 cells, the inhibitory concentration of 50% (IC50) of [225Ac]Ac-macropa-nimotuzumab (1.8 ± 1.0 nM) was 46.7-fold lower than that of cold (unlabeled) nimotuzumab (84.1 ± 0.3 nM; P < 0.001). Similar trends were observed for SNU-C2B and SW620 cell lines (Table 1). Phase contrast images showed a higher concentration of cell death with [225Ac]Ac-macropa-nimotuzumab than with unlabeled nimotuzumab. Unlabeled nimotuzumab had no effect on HT-29, but [225Ac]Ac-macropa-nimotuzumab was cytotoxic (IC50, 10.1 nM) to the cell.
IC50 Values of Immunoconjugates in KRAS Wild-Type and BRAFV600E HT-29 and KRAS Mutant DLD-1, SW620, and SNU-C2B CRC Monolayer Cells with Different Levels of EGFR Expression
Live-cell imaging was used to study the in vitro cytotoxicity of nimotuzumab and [225Ac]Ac-macropa-nimotuzumab in DLD-1, SW620, SNU-C2B, and HT-29 mCRC 3D spheroids (Table 2; Supplemental Figs. 7 and 8). In DLD-1 spheroids, the IC50 of [225Ac]Ac-macropa-nimotuzumab (10.6 ± 0.6 nM) was 32.4 times lower than that of nimotuzumab (342.4 ± 0.1 nM). Similar differences were observed in SNU-C2B and SW620 spheroids (Table 2). Phase contrast images displayed a decrease in spheroid sizes after treatment with [225Ac]Ac-macropa-nimotuzumab (Supplemental Fig. 7), indicating the enhanced cytotoxic effect of [225Ac]Ac-macropa-nimotuzumab compared with nimotuzumab. In HT-29 spheroids, unlabeled nimotuzumab had no effects. Enhanced cytotoxicity was observed with [225Ac]Ac-macropa-nimotuzumab (IC50, 41.5 ± 1.4 nM).
IC50 Values of Immunoconjugates in KRAS Wild-Type and BRAFV600E HT-29 and Mutant CRC DLD-1, SW620, and SNU-C2B Spheroids with Different Levels of EGFR Expression
Biodistribution, Dosimetry, and In Vivo Toxicity
Biodistribution of [225Ac]Ac-macropa-nimotuzumab was studied in healthy BALB/c mice and in athymic nude BALB/c mice bearing EGFR-positive DLD-1 xenografts. In healthy BALB/c mice, the uptake of [225Ac]Ac-macropa-nimotuzumab was high in the kidney, liver, and blood at early time points, but only the liver (11.5 ± 0.6 %IA/g) and the blood (8.1 ± 1.1 %IA/g) had high uptake 11 d after injection (Fig. 2; Supplemental Table 2). Projected human radiation dose estimates were calculated with OLINDA/EXM version 2.2 using the human scaling factor and biodistribution data obtained from healthy BALB/c mice (Table 3). As expected, the liver received the highest organ dose of [225Ac]Ac-macropa-nimotuzumab, followed by the spleen. In mice bearing DLD-1 xenografts, uptake of [225Ac]Ac-macropa-nimotuzumab was higher in the tumor at all time points than in other organs, with a maximum at 120 h (DLD-1 tumor, 32.0 ± 13.8 %IA/g; liver, 4.0 ± 2.9 %IA/g; kidney, 3.2 ± 2.2 %IA/g; blood, 5.1 ± 4.3 %IA/g; Supplemental Table 3). There were no changes in most hematopoietic parameters after administration of 11.1 kBq of [225Ac]Ac-macropa-nimotuzumab in healthy mice (Supplemental Table 4).

Biodistribution of [225Ac]Ac-macropa-nimotuzumab in selected healthy organs in athymic nude BALB/c mice (n ≥ 3/group) bearing DLD-1 xenografts at different time points after injection, expressed as %IA/g.
Human Radiation Dose Estimates for Women Estimated Using OLINDA/EXM Version 2.2
Efficacy of [225Ac]Ac-Macropa-Nimotuzumab
We evaluated the efficacy of [225Ac]Ac-macropa-nimotuzumab and control [225Ac]Ac-macropa-rituximab in mCRC KRAS mutant DLD-1 (high EGFR expression) and in KRAS wild-type and BRAFV600E mutant HT-29 (high EGFR expression) and SW620 (low EGFR expression) mouse xenograft models (Figs. 3–5). Tumor growth inhibition was evaluated using a digital caliper. In mice bearing DLD-1 xenografts treated with 3 doses of [225Ac]Ac-macropa-nimotuzumab, 3 of 7 mice had complete tumor regression on days 13, 100, and 130, whereas tumor volume reached 1,500 mm3 for a partially responding mouse on day 76. The remaining 3 mice in this group had tumor volumes of less than 100 mm3 at the end of the study. Two of 7 mice treated with 3 doses of control [225Ac]Ac-macropa-rituximab reached 1,500 mm3 on day 30, and the rest reached 1,500 mm3 by day 64. In the PBS group, all 8 mice reached the study endpoint (1,500 mm3) by day 42. In HT-29 mice treated with [225Ac]Ac-macropa-nimotuzumab, 1 of 7 mice had complete tumor regression and 4 mice showed a partial response to therapy, evidenced by reduction in tumor growth (75, 57, 200, and 550.4 mm3 on day 90). However, 1 mouse from this group reached the tumor endpoint on day 35. In the 225Ac-rituximab group, 3 of 4 mice reached the endpoint on day 16. In KRAS mutant SW620 mice (low EGFR copies per cell) treated with [225Ac]Ac-macropa-nimotuzumab, 2 of 8 mice showed a partial response to therapy, whereas the others reached 1,500 mm3 by days 16, 21, 35, 38, and 41. All mice in the [225Ac]Ac-macropa-rituximab and PBS groups reached the endpoint of this study within 33 and 47 d, respectively.

Efficacy of 225Ac-labeled radioimmunoconjugates in mice bearing EGFR-positive KRAS mutant (KRASG13D) DLD-1 colorectal xenografts. Mice were treated using saline (A), three 13-kBq doses (39 kBq total, administered 10 d apart) of control anti-CD20 antibody [225Ac]Ac-macropa-rituximab (B), and three 13-kBq doses (39 kBq total, administered 10 d apart) of anti-EGFR antibody [225Ac]Ac-macropa-nimotuzumab (C). (D) Kaplan–Meier survival curves of different groups. Study endpoint was when xenografts reached ≥1,500 mm3.

Efficacy of 225Ac-labeled radioimmunoconjugates in mice bearing EGFR-positive BRAFV600E mutant HT-29 colorectal xenografts. Mice were treated using saline (A), three 13-kBq doses (39 kBq total, administered 10 d apart) of control anti-CD20 antibody [225Ac]Ac-macropa-rituximab (B), and three 13-kBq doses (39 kBq total, administered 10 d apart) of anti-EGFR antibody [225Ac]Ac-macropa-nimotuzumab (C). (D) Kaplan–Meier survival curves of different groups. Study endpoint was when xenografts reached ≥1,500 mm3.

Efficacy of 225Ac-labeled radioimmunoconjugates against EGFR-positive SW620 colorectal xenografts. Mice were treated using saline (A), three 13-kBq doses (39 kBq total, administered 10 d apart) of control anti-CD20 antibody [225Ac]Ac-macropa-rituximab (B), and three 13-kBq doses (39 kBq total, administered 10 d apart) of anti-EGFR antibody [225Ac]Ac-macropa-nimotuzumab (C). (D) Kaplan–Meier survival curves of different groups. Study endpoint was when xenografts reached ≥1,500 mm3.
The Kaplan–Meier survival curves of DLD-1, HT-29, and SW620 xenografts are presented in Figures 3, 4, and 5, respectively. Compared with the control [225Ac]Ac-macropa-rituximab and PBS groups, 225Ac-nimotuzumab significantly extended survival in all models (P < 0.01). For KRAS mutant DLD-1 xenografts, median survival was 34 and 27 d for the [225Ac]Ac-macropa-rituximab and PBS groups, respectively, but was not reached for the 225Ac-nimotuzumab group after 130 d. For KRAS wild-type and BRAFV600E mutant HT-29 xenografts, median survival was 16 and 12.5 d for the [225Ac]Ac-macropa-rituximab and PBS groups, respectively, but was not reached for the [225Ac]Ac-macropa-nimotuzumab group (>90 d). For SW620 xenografts, median survival was 16, 24.5, and 41 d for the [225Ac]Ac-macropa-rituximab, PBS, and [225Ac]Ac-macropa-nimotuzumab groups, respectively. There was no gross toxicity in 225Ac-treated groups compared with control, as evidenced by the body weights of the mice (Supplemental Fig. 10).
DISCUSSION
Continuous activation of EGFR by oncogenic KRAS and BRAF abrogates antitumor activity of anti-EGFR targeted therapeutics (2). Because of their decay properties, 225Ac-targeted radioimmunoconjugates are considered molecular nanogenerators and can be ideal in the setting of KRAS and BRAF mutant CRC. To our knowledge, no prior study has evaluated an α-particle–labeled anti-EGFR agent in KRAS or BRAF wild-type and mutant CRC models. Others have evaluated the anti-EGFR antibodies [212Pb]Pb-TCMC-panitumumab and [212Pb]Pb-TCMC-cetuximab, or [213Bi]Bi-CHX-A′′-DTPA-cetuximab preclinically in other disease models (22,23). Hence, this study was undertaken to explore the effectiveness of an 225Ac-labeled anti-EGFR radioimmunoconjugate in KRAS and BRAF mutant CRC. CRC has 4 major types of KRAS mutations, namely, KRASG12D (34.2%), KRASG12V (21%), KRASG13D (20%), and KRASG12C (8.4%) (24). Compared with other mutations that show no sensitivity to anti-EGFR agents, KRASG13D shows some sensitivity to cetuximab, albeit less than the wild type (9).
We found that internalization depended on receptor density rather than KRAS status and was lowest in SW620, with the lowest EGFR expression, but similar between HT-29 and DLD-1, both with high EGFR copies per cell. Similarly, the binding (dissociation constant) of anti-EGFR antibodies observed in this and previous studies depended not on KRAS but on EGFR copies per cell (25). In vitro cytotoxicity was studied using Incucyte S3 live-cell imaging and a Cytotox red agent (Essen BioScience), which allows the quantification of dead cells (Table 1) in real time. Unlabeled nimotuzumab had no effect on the survival of BRAFV600E mutant HT-29 cells despite high EGFR expression, confirming the same observations by others (26,27). However, [225Ac]Ac-macropa-nimotuzumab was effective against 2D monolayer and 3D spheroids of HT-29 cells, albeit at a higher dose than for DLD-1 with similar EGFR copies per cell (Tables 1 and 2). DLD-1 with KRASG13D mutation is a bit responsive to unlabeled anti-EGFR antibodies and antibody–drug conjugates (27). We previously showed that nimotuzumab antibody–drug conjugate (nimotuzumab-PEG6-DM1, with a drug-to-antibody ratio of 3:4) (27) was cytotoxic to DLD-1, with IC50 of 32.6 nM (compared with 1.8 nM for [225Ac]Ac-macropa-nimotuzumab in this study), but was not cytotoxic to HT-29. Hence, the in vitro potency of [225Ac]Ac-macropa-nimotuzumab was severalfold more than the naked antibody or antibody–drug conjugate in the HT-29 model. In vitro cytotoxicity was also observed in SW620 with KRAS mutation and low EGFR copies per cell. Hence, [225Ac]Ac-macropa-nimotuzumab is advantageous over antibody–drug conjugates or other anti-EGFR inhibitors.
3D spheroids are a more relevant in vitro model than monolayer cells when studying in vitro cytotoxicity, particularly because they more accurately mimic micrometastatic lesions. Spheroid diameters for DLD-1, HT-29, SNU-C2B, and SW620 were in the range of 200–650 mM. In all spheroids tested, [225Ac]Ac-macropa-nimotuzumab was 22- to 33-fold more potent than the unlabeled nimotuzumab. These results suggest that [225Ac]Ac-macropa-nimotuzumab is potent against both KRAS and BRAFV600E mutant spheroids and would be effective in micrometastatic lesions in vivo.
We previously showed that the effective organ dose of 89Zr-nimotuzumab was more than 2-fold lower than that of 89Zr-cetuximab (25). Organ doses in this study showed similar trends compared with work using other anti-EGFR antibody conjugates, such as [213Bi]Bi-CHX-A′′-DTPA-cetuximab (28), as well as our previous study using [89Zr]Zr-DFO-nimotuzumab (25). [225Ac]Ac-macropa-nimotuzumab was cleared from almost all organs after 10 d and was retained in tumors, hence the justification for dose fractionation every 10 d. We recently showed using anti-EGFR antibody [89Zr]Zr-DFO-matuzumab that tumor uptake of CRC xenografts depended on EGFR expression rather than KRAS and BRAF mutational status, with a similar uptake in DLD-I and HT-29 xenografts, both with high EGFR density, that was more than 3-fold higher than in SW620 xenografts, with low EGFR density (29). In addition, the high internalization rate of nimotuzumab likely contributed to the prolonged retention of 225Ac in the tumor and hence the effectiveness. These characteristics make [225Ac]Ac-macropa-nimotuzumab a potentially effective molecular nanogenerator with continuous delivery of high linear energy transfer radiation doses to the tumor. A few BRAF inhibitors, including vemurafenib, dabrafenib, and encorafenib, are approved for treating BRAF mutant melanomas and show significant benefits in this population (30–32). However, these inhibitors show no benefits in CRC patients with BRAFV600E mutation, confirming preclinical data that showed the activation of this pathway is different for both cancer types (33). KRAS mutant DLD-1 xenografts and BRAF mutant HT-29 xenografts showed a similar response to [225Ac]Ac-macropa-nimotuzumab. However, [225Ac]Ac-macropa-nimotuzumab had less of an effect on KRAS mutant SW620 xenografts, likely because of its low EGFR expression. In all cell lines, [225Ac]Ac-macropa-rituximab showed no significant response. Therefore, the benefits (>6-fold improvement in survival, including complete remission) of [225Ac]Ac-macropa-nimotuzumab in mice bearing HT-29, as demonstrated in this study, could have a significant clinical implication in CRC patients with BRAFV600E mutation when translated. In addition, we demonstrated enhancement in survival in KRAS mutant xenografts, including some complete remissions of DLD-1 tumors, and more than 2-fold enhancement in median survival of mice bearing KRAS mutant SW620 xenografts, despite low EGFR expression.
CONCLUSION
This work showed the benefits of α-particle [225Ac]Ac-macropa-nimotuzumab as an anti-EGFR molecular nanogenerator against KRAS and BRAFV600E mutant xenografts. [225Ac]Ac-macropa-nimotuzumab was more effective in KRASG13D DLD-1 and BRAFV600E HT-29, with high EGFR expression, than in KRASG12V SW620, with low EGFR expression. This effectiveness results from its high internalization rate in these cells and high tumor retention. Preliminary hematopoietic studies showed that [225Ac]Ac-macropa-nimotuzumab was safe, and animals tolerated 3 doses of the agent. These promising data warrant further investigation and potential clinical translation.
DISCLOSURE
This work was funded by a Canadian Institute for Health Research project grant (437660) to Humphrey Fonge. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Can an anti-EGFR antibody radiolabeled with an α-emitting radioisotope (225Ac) be effective against EGFR-positive CRC xenografts that are irresponsive to naked antibodies, such as cetuximab?
PERTINENT FINDINGS: Anti-EGFR radioimmunotherapeutic [225Ac]Ac-macropa-nimotuzumab was effective in prolonging the survival of mice bearing EGFR-positive CRC xenografts that harbor KRAS and BRAFV600E mutations.
IMPLICATIONS FOR PATIENT CARE: [225Ac]Ac-macropa-nimotuzumab could result in significant survival improvements in patients with EGFR-positive CRC with or without KRAS or BRAFV600E mutations, which represent up to 80% of patients, when or if translated in clinical trial.
Footnotes
Published online Feb. 15, 2024.
- © 2024 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 28, 2023.
- Accepted for publication January 5, 2024.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.