


Visual Abstract

Abstract
Nonspecific lymph node uptake on 18F-FDG PET/CT imaging is a significant pitfall for tumor staging. Fibroblast activation protein α expression on cancer-associated fibroblasts and some tumor cells is less sensitive to acute inflammatory stimuli, and fibroblast activation protein–directed PET may overcome this limitation. Methods: Eighteen patients from our prospective observational study underwent 18F-FDG and 68Ga fibroblast activation protein inhibitor (FAPI) PET/CT scans within a median of 2 d (range, 0–22 d). Lymph nodes were assessed on histopathology and compared with SUV measurements. Results: On a per-patient basis, lymph nodes were rated malignant in 10 (56%) versus 7 (39%) patients by 18F-FDG PET/CT versus 68Ga-FAPI PET/CT scans, respectively, with a respective accuracy of 55% versus 94% for true lymph node metastases. Five of 6 (83%) false-positive nodes on the 18F-FDG PET/CT scans were rated true negative by the 68Ga-FAPI PET/CT scans. On a per-lesion basis, tumor detection rates were similar (85/89 lesions, 96%). Conclusion: 68Ga-FAPI PET/CT imaging demonstrated higher accuracy for true nodal involvement and therefore has the potential to replace 18F-FDG PET/CT imaging for cancer staging.
For whole-body staging of malignancy, 18F-FDG PET/CT imaging has been used for several decades and is now a standard tool. However, nonspecific lymph node uptake leading to false-positive findings and incorrect treatment decisions is a major limitation of 18F-FDG PET/CT imaging (1,2).
Mechanisms behind the increased 18F-FDG uptake include inflammation and recruitment of a great number of invading and activated immune cells with increased metabolic activity (3). Even though the fibroblast activation protein can be induced by inflammatory stimuli, such as transforming growth factor β, the increase in expression (per cell) might be comparatively less, and thus, 68Ga-fibroblast activation protein inhibitor (FAPI) PET/CT imaging may overcome the limitations of 18F-FDG PET/CT imaging (4–6).
MATERIALS AND METHODS
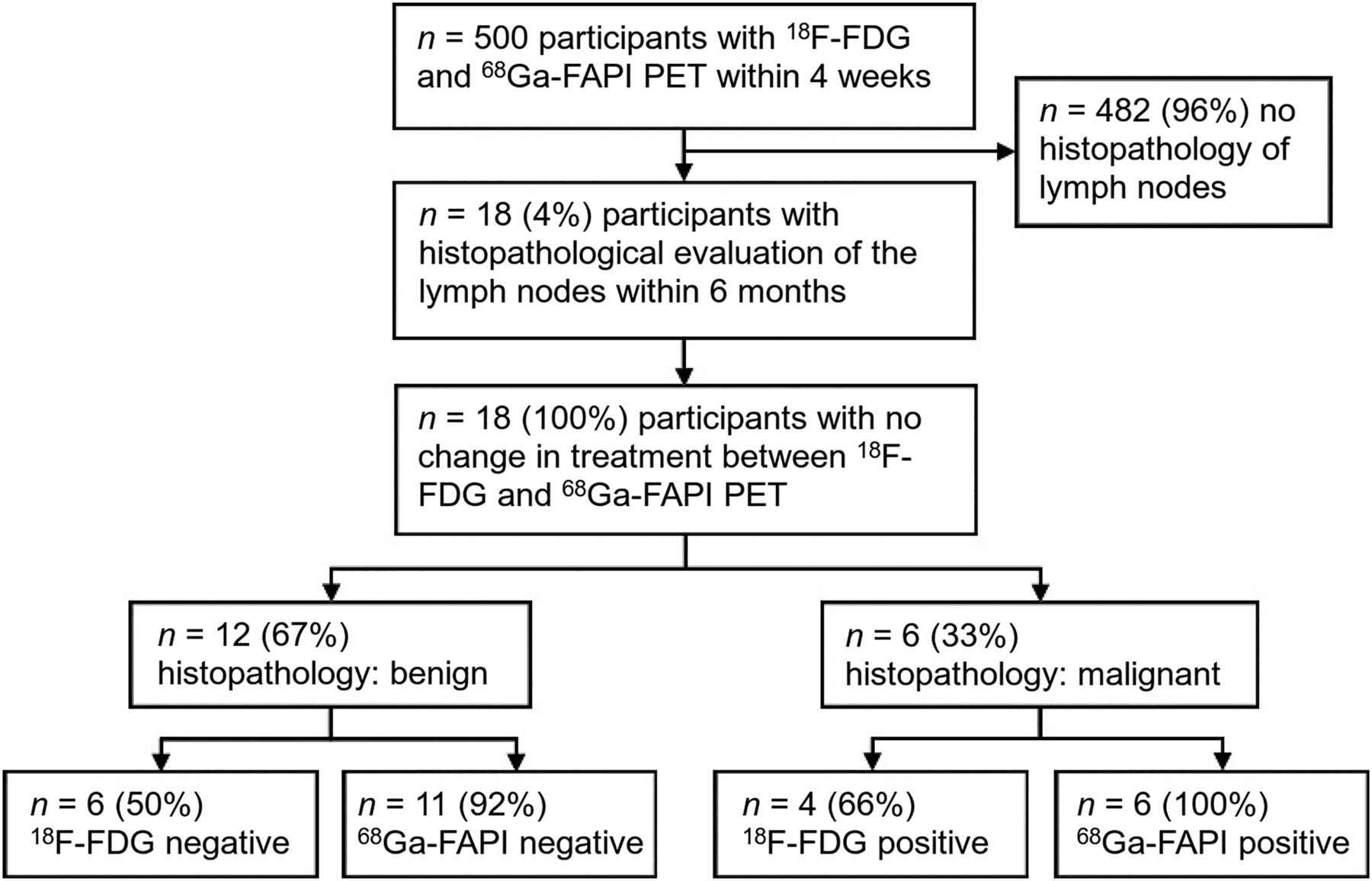
We included 18 patients from our database who were enrolled in a prospective observational study (NCT04571086, Institutional Review Board approval 19-8991) between 2020 and 2022 at our institution. Enrollment was offered to all patients who underwent 68Ga-FAPI-46 PET/CT imaging at our department. The Institutional Review Board approved this study, and all subjects signed a written informed consent form. Patients met the following criteria: 68Ga-FAPI and 18F-FDG PET/CT imaging for oncologic staging within 4 wk, histopathologic evaluation of the lymph nodes, and no change in treatment between 18F-FDG and 68Ga-FAPI PET/CT scans (Fig. 1). Clinical indication was oncologic staging or restaging of a tumor entity that was known to demonstrate elevated fibroblast activation protein expression (sarcoma, pancreatic cancer, colon cancer, etc.). One patient with lymph node uptake was reported previously (6).

Standards for Reporting of Diagnostic Accuracy Studies flow diagram.
The median injected activity was 309 MBq (range, 94–440 MBq) for 18F-FDG and 130 MBq (range, 66–194 MBq) for 68Ga-FAPI. The median uptake time was 70 min for 18F-FDG and 16 min for 68Ga-FAPI. We previously compared early versus late uptake scans for 68Ga-FAPI PET/CT and found nearly equal tumor detection (7). Therefore, in our department, the standard protocol is early image acquisition. Descriptive statistics are provided in Figure 2 and Supplemental Figure 2 (supplemental materials are available at http://jnm.snmjournals.org). The Mann–Whitney U test was used to compare uptake intensity (SUV) and receiver operating characteristic curves with the Youden index to narrow cutoffs.

SUVpeak and TBR of 18 lymph nodes (1 node per patient). (A) SUVpeak of lymph nodes. (B) TBRmuscle with major pectoral muscle. (C) Blood TBR (TBRblood) with aorta as reference. Statistical significance of difference was assessed by Mann–Whitney U test.
For lymph nodes, SUVpeak and target-to-background ratio (TBR) were determined. SUVpeak was measured in accordance with PERCIST (1 cm3 volume of interest). The TBR was calculated in relation to the SUVmean of muscle (pectoralis major) and blood pool (aorta) for 18F-FDG and 68Ga-FAPI (SUVmax lymph node/SUVmean pectoralis or SUVmean aorta). Because of very low physiologic uptake, the liver was unsuitable for calculating the 68Ga-FAPI TBR, and therefore, the liver TBR was not included. Lymph node uptake on PET (positive vs. negative) was determined by PERCIST: SUVmax above the PERCIST cutoff (SUVmean of liver [18F-FDG] or muscle [68Ga-FAPI] + 2 × SD) was defined as visual positive and SUVmax below the PERCIST cutoff as visual negative.
Tumor detection efficacy was determined independently and without access to histopathology data for both modalities by consensus of a nuclear medicine physician and a radiologist, each with at least 5 y of training.
RESULTS
After database screening, we included 18 patients (12 men and 6 women). Figure 1 shows a Standards for Reporting of Diagnostic Accuracy Studies flow diagram for the patients. Patient characteristics are shown in Supplemental Table 1. Two (11%) patients had sarcoma, and 16 (89%) patients had carcinoma of various origins. Eleven (61%) patients had locoregional lesions only, and 7 (39%) patients showed distant metastases in bone, organs, or distant lymph nodes (Supplemental Table 2).
The mean age of the patients was 56 y (range, 31–73 y). PET scans were performed on 9 (50%) patients for staging and 9 (50%) for restaging of malignancy. The median time between 18F-FDG PET/CT and 68Ga-FAPI PET/CT imaging was 2 d (range, 0–22 d). Biopsy was performed on average 24 d (range, 1–164 d) after the PET scan.
Measured lymph nodes had a median size of 0.7 cm (range, 0.4–1.7 cm) in short-axis diameter and were obtained by open surgery in 12 (67%) patients, by endobronchial ultrasound-guided transbronchial needle aspiration in 3 (17%) patients, by laparoscopy in 2 (11%) patients, and by ultrasound in 1 patient (6%). Four (22%) patients underwent PET scans while being treated with chemotherapy; the remaining patients were not on active therapy during imaging. Three of these patients had matching 18F-FDG PET/CT and 68Ga-FAPI PET/CT findings. In the remaining patient, the axillary reactive lymph node was positive on 18F-FDG PET/CT and negative on 68Ga-FAPI PET/CT 3 wk after coronavirus disease 19 vaccination on the ipsilateral side (Supplemental Table 3).
Table 1 shows the accuracy of 18F-FDG PET/CT and 68Ga-FAPI PET/CT findings as validated by histopathology. Sensitivity, specificity, positive predictive value, and negative predictive value were higher for 68Ga-FAPI PET/CT than for 18F-FDG PET/CT for lymph node evaluation. Overall accuracy of lymph node assessment was 94% versus 55% for 68Ga-FAPI PET/CT versus 18F-FDG PET/CT.
Accuracy of 18F-FDG PET/CT Vs. 68Ga-FAPI PET/CT for Nodal Staging in 18 Patients
Figure 2 compares the uptake of 68Ga-FAPI and 18F-FDG in benign and malignant lymph nodes. The Mann–Whitney U test showed that SUVpeak and TBRs were significantly higher in malignant than benign lymph nodes on the 68Ga-FAPI PET/CT scan (average SUVpeak, 3.5 vs. 1.3, P = 0.01; muscle TBR [TBRmuscle], 3.5 vs. 1.0, P < 0.001; blood TBR, 3.6 vs. 1.2, P = 0.005) but not on the 18F-FDG PET/CT scan (average SUVpeak, 3.1 vs. 3.5, P = 0.77; TBRmuscle, 8.7 vs. 8.6, P = 0.98; blood TBR, 3.0 vs. 3.3, P = 0.68).
Tracer uptake was higher for 18F-FDG than for 68Ga-FAPI in benign lymph nodes of patients 5, 6, 10, 12, 13, and 16 (average SUVpeak, 5.6 vs. 1.7) and was higher for 68Ga-FAPI than for 18F-FDG in malignant lymph nodes of patients 8 and 11 (1.6 vs. 0.9) (Supplemental Fig. 1).
Analysis of the receiver operating characteristics showed an overall model quality of less than 0.5 for 18F-FDG PET/CT (SUVpeak, TBRmuscle, and blood TBR) and thus was too low for a reliable cutoff determination. For 68Ga-FAPI PET/CT imaging, the most appropriate cutoff was 1.7 for SUVpeak (sensitivity, 83%; specificity, 75%), 1.5 for TBRmuscle (sensitivity, 100%; specificity, 92%), and 1.9 for blood TBR (sensitivity, 83%; specificity, 91%) (Supplemental Fig. 2).
18F-FDG PET/CT and 68Ga-FAPI PET/CT images demonstrating a mismatch of tracer uptake in a benign lymph node are shown in Figure 3, and additional images of matching tracer uptake are shown in Supplemental Figures 3–6.

Patient 10, 72-y-old man with urothelial carcinoma of bladder being evaluated for restaging after chemotherapy, showing mismatch of tracer-avid lymph node in 18F-FDG PET/CT and non–tracer-avid lymph node in 68Ga-FAPI PET/CT. Histopathology result was benign. 18F-FDG PET/CT images (A and B) and 68Ga-FAPI PET/CT images (C and D), maximum-intensity projections (A and D), axial CT (B and C, top), PET (B and C, middle), and fused PET/CT (B and C, bottom) are shown.
In our study, the overall tumor detection efficacy on a per-lesion basis was the same for 18F-FDG PET/CT as it was for 68Ga-FAPI PET/CT (96% vs. 96%) (Supplemental Table 4).
DISCUSSION
We demonstrate in patients with various types of cancer that 68Ga-FAPI PET/CT imaging identifies nodal involvement with higher accuracy than 18F-FDG PET/CT imaging because of a lower rate of false-positive and false-negative findings. In addition, in these patients with local or advanced disease, overall tumor detection rates were the same with 68Ga-FAPI PET/CT and 18F-FDG PET/CT imaging.
In line with our findings, several previous studies have reported a high accuracy of 68Ga-FAPI PET/CT imaging for tumor staging. 68Ga-FAPI PET/CT imaging was superior to 18F-FDG PET/CT imaging for the detection of sarcoma, pancreatic and breast cancers, and bone, liver, and peritoneal metastases (8–11).
In our study, 68Ga-FAPI uptake was significantly higher in malignant versus benign lymph nodes, which facilitated correct identification of all malignant lymph nodes. Conversely, almost all benign lymph nodes demonstrated low or absent radiotracer uptake, with false-positive findings in only 1 patient on 68Ga-FAPI PET/CT imaging.
In addition, a lower background uptake for 68Ga-FAPI than for 18F-FDG PET allows for improved delineation of physiologic versus metastatic uptake (10). In contrast, 18F-FDG PET/CT imaging demonstrated uptake above the PERCIST threshold, with false-positive judgment for lymph node assessment in 6 patients. This well-known limitation of 18F-FDG PET/CT imaging is due to the unfavorable properties of its molecular target. 18F-FDG, as a sugar-based tracer, is taken up into cells through glucose transporter 1 in most metabolically active tissues (2,3); 68Ga-FAPI binds to the fibroblast activation protein, which is selectively expressed on activated fibroblasts and some mesenchymal cancer cells (4,5). On 18F-FDG PET/CT imaging, inflammation and associated reactive activation of tissue lead to nonspecific uptake in immune cells, complicating diagnostic interpretation. Publications of vaccine-related 18F-FDG uptake and tracer uptake in inflammatory tissue (arthritis, sarcoidosis) are consistent with the low positive predictive value of 18F-FDG PET/CT scans in our evaluation (6,12,13).
Because of the different molecular mechanism of 68Ga-FAPI PET/CT imaging, it is not as prone to mild immune reactions, which represent most diagnostic pitfalls. However, large or chronic inflammation with associated fibroblast activation might cause an uptake of 68Ga-FAPI as well (14,15). In our study, patient 16 was the only patient with a false-positive uptake of 68Ga-FAPI. Images demonstrated accumulation of both tracers in lymph nodes affected by sarcoidosis, however, with a 7 times higher TBRmuscle on the 18F-FDG PET/CT scan than on the 68Ga-FAPI PET/CT scan.
Although the SUV for the 68Ga-FAPI PET/CT imaging showed an overlap for benign and malignant nodes as well (16), the overlap was much less with 18F-FDG PET/CT imaging. Specifically, absolute SUV proved to be less accurate than TBRmuscle.
Nodal staging is a critical element for initial treatment as it affects tumor stage directly and, consequently, therapy. Reactive tracer accumulation is particularly common in exposed locations such as axillary, mediastinal, or inguinal lymph nodes. Reactive uptake in the ipsi- and contralateral axillary lymph nodes interferes with staging of lung or breast cancer and significantly influences therapy decisions, as does reactive uptake in the inguinal region in prostate or lower-extremity cancers (2,6,11).
Although suggestive lymph nodes can be biopsied for validation, this invasive procedure comes with additional costs and potential complications such as bleeding or nerve damage (15). To avoid complications, further studies with larger cohorts are needed to compare the accuracy of both tracers, which will help to reduce additional histopathologic workup and incorrect management decisions.
Our study has limitations: we present a small cohort of patients who were highly selected for suggestive lymph nodes with a histopathology workup. Although histopathology is the gold standard, sampling errors during biopsy cannot be ruled out. Furthermore, the use of PERCIST in general and the use of muscle as a reference region have not yet been validated for 68Ga-FAPI PET/CT imaging.
CONCLUSION
False-positive lymph node staging due to inflammation is a well-known limitation of 18F-FDG PET/CT imaging. Here, we demonstrate in patients with various types of cancer that a 68Ga-FAPI PET/CT scan identifies nodal involvement with higher accuracy because of a lower rate of false-positive findings than for 18F-FDG PET/CT. In the future, 68Ga-FAPI PET/CT staging may help to avoid additional workup or unnecessary treatment.
DISCLOSURE
Kim Pabst has received a Junior Clinician Scientist stipend from the University Medicine Essen Clinician Scientist Academy (UMEA) sponsored by the faculty of medicine and Deutsche Forschungsgemeinschaft (DFG), travel fees from IPSEN, and research funding from Bayer. Katharina Lueckerath reports fees from Sofie Biosciences (consultant) and research funding from Mariana Oncology. Hubertus Hautzel reports fees from PARI Medical Holding (research funding, travel grant) and Urenco Germany (personal fees) outside the submitted work. Rainer Hamacher is supported by the Clinician Scientist Program of the University Medicine Essen Clinician Scientist Academy (UMEA) sponsored by faculty of medicine and Deutsche Forschungsgemeinschaft (DFG) and has received travel grants from Lilly, Novartis, and PharmaMar as well as fees from Lilly and PharmaMar. Jens Siveke received honoraria as a consultant or for continuing medical education presentations from AstraZeneca, Bayer, Bristol-Myers Squibb, Eisbach Bio, Immunocore, Novartis, Roche/Genentech, and Servier; his institution receives research funding from Bristol-Myers Squibb, Celgene, Eisbach Bio, and Roche/Genentech; he holds ownership and serves on the Board of Directors of Pharma15, all outside the submitted work. Ken Herrmann reports personal fees from Bayer; personal fees and other from Sofie Biosciences; personal fees from SIRTEX; nonfinancial support from ABX; personal fees from Adacap, Curium, and Endocyte; grants and personal fees from BTG; and personal fees from IPSEN, Siemens Healthineers, GE Healthcare, Amgen, Novartis, ymabs, Aktis Oncology, Theragnostics, and Pharma15, outside the submitted work. Wolfgang Fendler reports fees from Sofie Biosciences (research funding), Janssen (consultant, speaker), Calyx (consultant, image review), Bayer (consultant, speaker, research funding), Novartis (speaker, consultant), Telix (speaker), GE Healthcare (speaker), and Eczacıbaşı Monrol (speaker) outside the submitted work. Kelsey Pomykala reports personal fees from ABX. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Can 68Ga-FAPI PET/CT scanning prevent pitfalls of inflammatory uptake in lymph nodes?
PERTINENT FINDINGS: We compared PET/CT uptake and lymph node biopsy results for 18F-FDG and 68Ga-FAPI using a head-to-head study. Accuracy for nodal assessment was higher for 68Ga-FAPI PET/CT (94%) than for 18F-FDG PET/CT (55%) because of a lower rate of false-positive and false-negative findings. Both imaging modalities revealed an equal tumor detection rate.
IMPLICATIONS FOR PATIENT CARE: 68Ga-FAPI was superior to 18F-FDG at assessing dignity of lymph nodes by PET/CT.
ACKNOWLEDGMENTS
We thank the patients who volunteered to participate in this trial and the investigators and staff who cared for them.
Footnotes
Published online Sep. 21, 2023.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 19, 2023.
- Revision received August 18, 2023.





{kind=link}
{kind=link}
{kind=link}
{kind=link}