


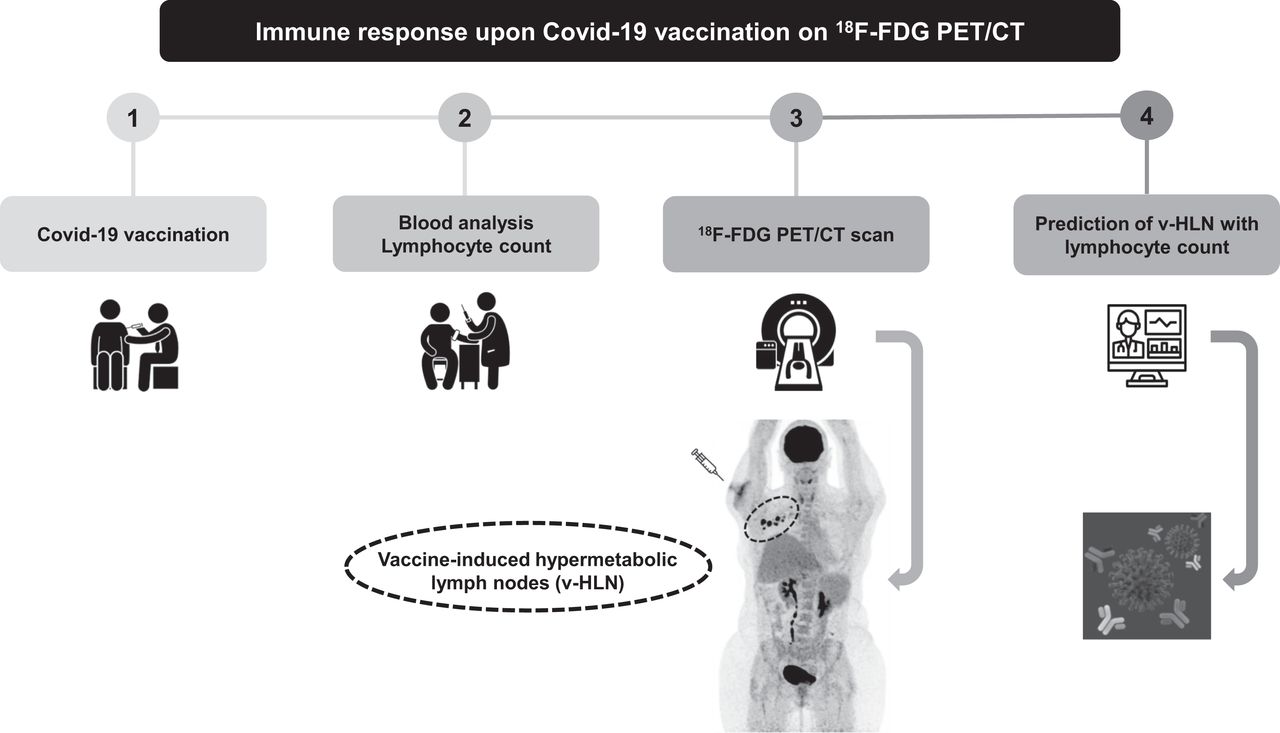
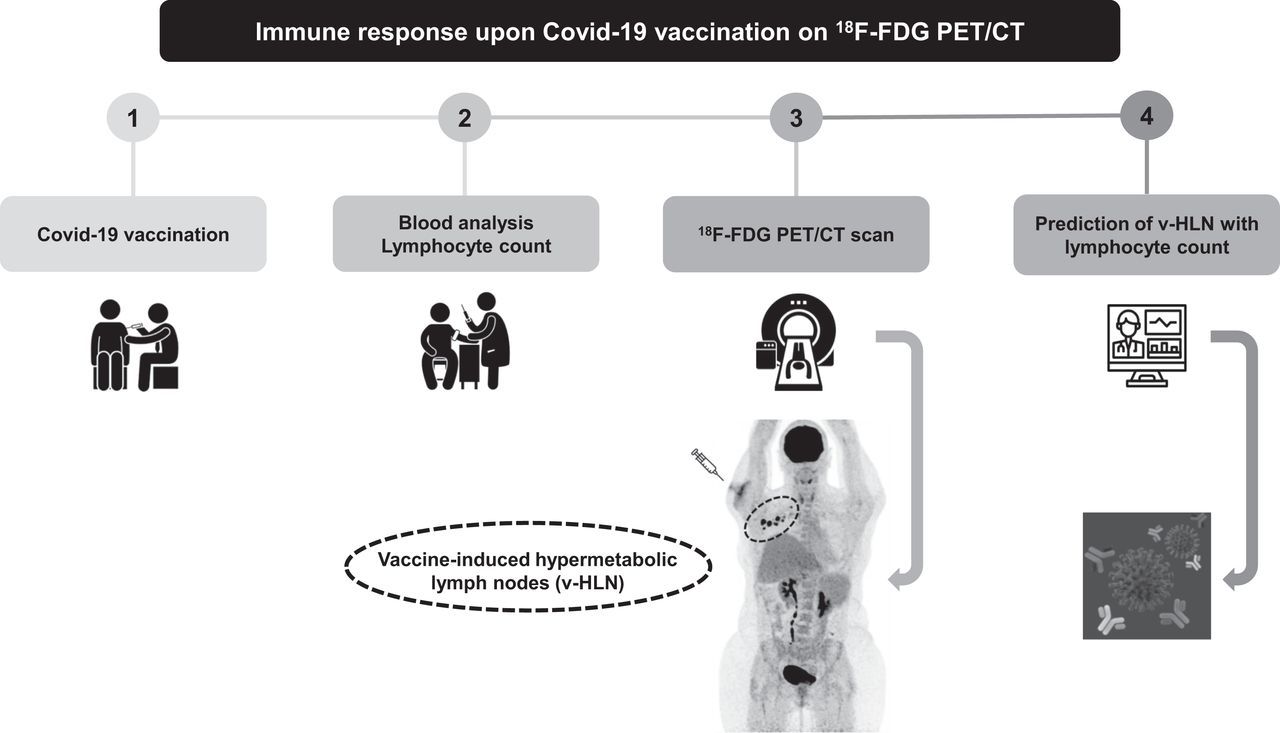
Visual Abstract
Abstract
We aimed to predict the presence of vaccine-induced hypermetabolic lymph nodes (v-HLNs) on 18F-FDG PET/CT after coronavirus disease 2019 (COVID-19) vaccination and determine their association with lymphocyte counts. Methods: In this retrospective single-center study, we included consecutive patients who underwent 18F-FDG PET/CT imaging after messenger RNA– or viral vector–based COVID-19 vaccination between early March and late April 2021. Demographics, clinical parameters, and absolute lymphocyte count (ALC) were collected, and their association with the presence of v-HLNs in the draining territory was studied by logistic regression. Results: In total, 260 patients were eligible, including 209 (80%) women and 145 (56%) with breast cancer. The median age was 50 y (range, 23–96 y). The messenger RNA vaccine had been given to 233 (90%). Ninety (35%) patients had v-HLNs, with a median SUVmax of 3.7 (range, 2.0–26.3), and 74 (44%) displayed lymphopenia, with a median ALC of 1.4 × 109/L (range, 0.3–18.3 × 109/L). An age of no more than 50 y (odds ratio [OR], 2.2; 95% CI, 1.0–4.5), the absence of lymphopenia (OR, 2.2; 95% CI, 1.1–4.3), and less than a 30-d interval from the last vaccine injection to the 18F-FDG PET/CT (OR, 2.6; 95% CI, 1.3–5.6) were independent factors for v-HLNs on multivariate analysis. In breast cancer patients, the absence of lymphopenia was the only independent factor significantly associated with v-HLNs (OR, 2.9; 95% CI, 1.2–7.4). Conclusion: Patients with a normal ALC after COVID-19 vaccination were more likely to have v-HLNs on 18F-FDG PET/CT, both of which might be associated with a stronger immune response to vaccination.
- 18F-FDG PET/CT
- COVID-19 vaccination
- absolute lymphocyte count
- hypermetabolic lymph nodes
- immune response
A billion doses of the currently authorized and recommended messenger RNA (mRNA) (1,2) or viral vector vaccine (3) against coronavirus disease 2019 (COVID-19) have been administered worldwide. Such vaccination has been shown to promote immunity against the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) by inducing strong T- and memory B-cell responses (4,5).
Because generation of an immune response increases glucose metabolism in lymphoid organs, which are critical modulators of T- and B-cell immunity (6,7), 18F-FDG PET/CT might be used as a potent tool to assess immune response after vaccinations against several infections, including SARS-CoV-2 (8), influenza virus (9), and human papillomavirus (10), as well as against cancer (11). Recently, several findings on 18F-FDG PET/CT have been reported in patients vaccinated against COVID-19, most likely related to immune activation in lymphoid organs, hypermetabolic lymph nodes (HLNs) in the drainage territory (12–19), or increased glucose metabolism in the spleen (20–22).
In patients who received mRNA vaccines for COVID-19, the prevalence of vaccine-induced HLNs (v-HLNs) on 18F-FDG PET/CT was approximately 45% (12,14,23). Indeed, v-HLNs were more commonly observed in young and immunocompetent patients (14). Additionally, the interval between the last vaccine dose and the number of vaccine doses was also significantly associated with the presence of v-HLNs (14). Furthermore, v-HLNs appeared to correlate with an effective humoral response induced by the mRNA vaccination (13). However, it remains unclear whether similar results would be obtained after the administration of another type of vaccine (e.g., viral vectors).
Lymphoma patients and breast cancer (BC) patients are considerably more susceptible to v-HLNs than are patients with other types of cancer, as stated by Cohen et al. (12). Among BC patients, v-HLNs in the axillary area and beyond can mimic tumor lesions and lead to confounding of imaging results (16). Recent publications have emphasized the importance of documenting vaccination history at the time of scanning to avoid false-positive results (21,24) and all the attendant negative consequences: unnecessary biopsy/cytology or lymphadenectomy for early-stage BC or unjustified changes in systemic treatment for advanced-stage BC.
In the present study, we specifically aimed to predict the presence of v-HLNs on 18F-FDG PET/CT after COVID-19 vaccination and to investigate their relationships to lymphocyte counts, with a special focus on a subgroup of BC patients.
MATERIALS AND METHODS
Patients
We conducted a retrospective review of 702 consecutive patients who underwent 18F-FDG PET/CT imaging at Institut Curie Hospital, Saint-Cloud, France (the flow chart is provided in Fig. 1). Four hundred forty-two patients were not vaccinated (n = 437) or did not want to participate in medical research (n = 5) and were excluded. This retrospective data collection complied with the requirements of our Institutional Review Board (DATA210128), which waived the need to obtain informed consent (rule of nonopposition), and the study was conducted according to the Declaration of Helsinki.

Flowchart.
Clinicobiologic Data
Clinical data consisted of the patient’s age, sex, disease (cancer type if applicable), and current specific treatment (chemotherapy, endocrine therapy, immunotherapy with immune checkpoint inhibitors, or targeted therapy). All patients were asked for the date of their COVID-19 vaccination, the type or brand of vaccine that had been used (mRNA or viral vector), and the injection site for the first and (if applicable) second doses.
We considered a subgroup of patients who theoretically had a weakened immune system, whom we called immunosuppressed, caused by any of the following treatments: chemotherapy within the last 3 mo, rituximab-containing regimens or bone marrow transplantation within the last 6 mo, or current steroid therapy with more than 10 mg/d of prednisone-equivalent. Biologic characteristics, including the absolute lymphocyte count (ALC), were obtained from peripheral blood samples after vaccination (at least 1 dose) and before 18F-FDG PET/CT. For ALC, we used the lower limit of normal for each center. Blood samples were analyzed when performed after vaccination and in the previous 28 d before 18F-FDG PET/CT.
18F-FDG PET/CT Scans
18F-FDG PET/CT was performed in accordance with the applicable European Association of Nuclear Medicine procedure guidelines (25). Patients fasted for at least 6 h before scanning to ensure a blood glucose level of less than 10 mmol/L. Scanning was performed using a Philips Vereos PET/CT device, combining the small lutetium-yttrium oxyorthosilicate scintillator crystal with the silicon photomultiplier block design. PET images were reconstructed with a fully 3-dimensional time-of-flight iterative method (VUE Point FX [an ordered-subsets expectation maximization algorithm; GE Healthcare], a matrix of 288 × 288, 3 iterations, 5 subsets, and a 2-mm postprocessing filter). Images were converted to SUV units by normalization using the patient’s body weight.
Measurement and Interpretation of 18F-FDG PET/CT Parameters
Four certified nuclear medicine physicians analyzed the 18F-FDG PET/CT images. Measures of SUVmean or SUVmax were obtained from HLNs detected in the drainage territory using the PET tumor segmentation tool in Philips IntelliSpace Portal, version 9.0. Readers were masked and did not know the patients’ characteristics.
Draining lymph node uptake values were measured on the PET images, assisted by CT data for the anatomic location. As previously published by Thomassen et al. (9), we also recorded contralateral lymph node uptake values, which were used for reference. Similarly, an HLN was defined as having an SUVmax ratio of at least 1.5 between the ipsilateral and contralateral reference sites (9,14). The HLN SUVmax was defined as the highest SUVmax among all HLNs detected in the drainage territory (axillary or supraclavicular for vaccination in the deltoid, inguinal for vaccination in the thigh or buttock). The size of most HLNs was recorded using short-axis diameter on CT images. v-HLNs were characterized using the clinical background: type, stage and site of disease, histologic findings (biopsy or cytology), and other available imaging results (enhanced MRI, CT, or previous 18F-FDG PET/CT). Where there was any uncertainty about HLN etiology (disease-related or vaccine-induced), we categorized the patients into an indeterminate-HLN group.
Statistical Analysis
Continuous and categoric variables are reported as median with range (minimum and maximum) and as frequency and percentage, respectively. Factors associated with v-HLNs were tested by logistic regression analysis using a stepwise Akaike information criterion method for variable selection (26). All reported P values are 2-sided, and P values of less than 0.05 were considered to be significant. Analyses were performed with R software (version 4.0.2).
RESULTS
Whole Cohort
Patient Characteristics
Table 1 summarizes the detailed demographic and clinicobiologic characteristics and PET imaging parameters of the 260 patients. The median age was 50 y (range, 23–96 y), and 80% were women. Two hundred thirty-three patients (90%) received the mRNA vaccine, including 110 (42%) who had 2 doses. The median time between the last vaccination dose and 18F-FDG PET/CT scanning was 14 d (range, 1–51 d) for patients who received only 1 dose and 23 d (range, 1–67 d) for patients who received a second dose. More than half the patients were referred for BC (56%), and 24% were considered immunosuppressed (n = 62). Blood sample analysis after vaccination and before PET was available in 170 patients. Among them, median ALC was 1.4 × 109/L (range, 0.3–18.3 × 109/L), and 74 (44%) displayed lymphopenia. Overall, 90 patients (35%) had v-HLNs, with a median SUVmax of 3.7 (range, 2.0–26.3).
Patient Characteristics
Association Between v-HLNs on 18F-FDG PET/CT and Clinicobiologic Parameters
An age of no more than 50 y (odds ratio [OR], 2.2; 95% CI, 1.0–4.5), the absence of lymphopenia (OR, 2.2; 95% CI, 1.1–4.3), and a less than 30-d interval from the last vaccine injection to the date of 18F-FDG PET/CT (OR, 2.6; 95% CI, 1.3–5.6) were statistically significant factors associated with v-HLNs (Fig. 2) on univariate analysis (Table 2). All parameters remained independent predictors of the v-HLN status on multivariate analysis. Interestingly, for patients displaying lymphopenia after vaccination, we evaluated the dynamic of ALC and found that a low ALC existed before vaccination in most patients (67%, n = 36) suggesting that lymphopenia was not related to vaccination. The immunosuppression, the type of vaccine, and the number of doses were not associated with v-HLNs.

Maximum-intensity-projection 18F-FDG PET images of 45-y-old woman with relapsed DLBCL in mediastinum. Patient was treated with brentuximab and nivolumab and experienced complete metabolic response 2 mo after initiation of therapy (January 2021). Although continuing lymphoma therapy, she received 2 mRNA COVID-19 vaccine injections in right deltoid. 18F-FDG PET/CT scan 4 d after last vaccine dose (April 2021) showed several HLNs (encircled). On subsequent 18F-FDG PET/CT scan 1 mo later, HLNs disappeared, strongly suggesting their relation to vaccination. This clinical presentation thus highlights presence of v-HLNs in patient younger than 50 y and with normal ALC at time of 18F-FDG PET/CT, which was performed less than 30 d after last vaccine dose. CR = complete response; DLBCL = diffuse large B-cell lymphoma.
Parameters Associated with v-HLNs in Whole Cohort (260 Patients) on Univariate and Multivariate Logistic Regression Analyses
BC Cohort
Patient Characteristics
Table 1 summarizes the detailed demographic and clinicobiologic characteristics and PET imaging parameters of the 145 BC patients. All patients were women. About one third had early-stage BC, and the remaining two thirds had advanced-stage BC, treated mainly with endocrine therapy with or without targeted therapy or chemotherapy. Whole blood counts were available for 106 BC patients after vaccination and before PET. Among them, median ALC was 1.5 × 109/L (range, 0.4–5.0 × 109/L), and 41 (39%) displayed lymphopenia. Fifty-six patients (37%) had v-HLNs, with a median SUVmax of 3.7.
Association Between v-HLNs on 18F-FDG PET/CT and Clinicobiologic Parameters
Logistic regression analysis summarizing the association between v-HLNs on 18F-FDG PET/CT after COVID-19 vaccination and clinicobiologic parameters is provided in Table 3. The absence of lymphopenia was the only independent factor significantly associated with v-HLNs (OR, 2.9; 95% CI, 1.2–7.4). The patients’ age and immune status, the type of vaccine, the number of doses, or the interval from the last vaccine injection to the date of 18F-FDG PET/CT were not significantly associated with v-HLNs in this subgroup of BC patients.
Parameters Associated with v-HLNs in BC Cohort (145 Patients) on Univariate and Multivariate Logistic Regression Analyses
Early-Stage BC Patients with Vaccination Ipsilateral to the Tumor
We identified 7 BC patients who had axillary HLNs ipsilateral to the recently vaccinated arm but also ipsilateral to the known tumor. Their demographic characteristics, vaccination information, 18F-FDG PET/CT parameters, ALC, and histologic data are reported in Table 4. Six of the cases had been histologically documented by fine-needle aspiration cytology (n = 3) or sentinel lymph node biopsy (n = 3). One patient (14%) was not investigated and began neoadjuvant endocrine therapy; the planned partial mastectomy with sentinel lymph node biopsy will help determine the cause of HLNs afterward. Although all fine-needle aspiration cytology evidenced signs of malignancy, with tumor cells (43%) (Fig. 3), all sentinel lymph node biopsies revealed benign reactive changes (43%) (Fig. 4).
Early-Stage BC Cohort with Vaccination Ipsilateral to Tumor

In patient with early-stage BC who received vaccine injection ipsilateral to tumor, maximum-intensity-projection 18F-FDG PET image (top) shows HLN in left axilla, axial 18F-FDG PET/CT image (middle) also shows left axillary HLN, and fine-needle aspiration cytology specimen shows tumor cells (May-Grünwald/Giemsa staining, ×20) (bottom).

In patient with early-stage BC who received vaccine injection ipsilateral to tumor, maximum-intensity-projection 18F-FDG PET image (top) shows HLN in left axilla, axial 18F-FDG PET/CT image (middle) also shows left axillary HLNs, and sentinel lymph node biopsy sample shows benign reactive changes (hematoxylin-eosin-saffron staining, ×5) (bottom).
DISCUSSION
We have shown that patient age (≤50 y), ALC (<lower limit of normal), and timing of last injection dose (<30 d before PET) significantly correlated with v-HLNs on 18F-FDG PET/CT after COVID-19 vaccination in a retrospective cohort of 260 patients. Moreover, among patients with BC, the ALC before 18F-FDG PET/CT remained the most strongly implicated factor associated with v-HLN status. Indeed, BC patients with a normal value of ALC were more likely to have v-HLNs on 18F-FDG PET/CT.
Our results are consistent with previously published data, suggesting that v-HLNs are significantly less common in elderly patients and conversely more frequent in patients who received their last vaccine injection a few days before 18F-FDG PET/CT (14). In addition to providing information on the HLN status, which may help nuclear medicine physicians with image interpretation and oncologists with medical management, these findings also raise the question of whether the COVID-19 vaccine is triggering a more robust immune response in this population (≤50 y or ALC > lower limit of normal). In the specific setting of hematologic malignancies, Cohen et al. demonstrated that the rate of v-HLNs after mRNA vaccination was significantly higher in patients with positive serology than in those with negative serology (13). This essential result might be the missing link between the presence of v-HLNs and vaccine effectiveness in inducing a strong immune response and, therefore, robust immunity.
Another interesting aspect of our work is that ALC after vaccination and before 18F-FDG PET/CT was an independent factor significantly associated with v-HLNs in the whole cohort of 260 patients—an observation that was further reinforced by our findings in the specific cohort of 145 BC patients. Such important results have been previously demonstrated after vaccination, especially against SARS-CoV-2 (27,28) but also against other viruses (29). Indeed, Achiron et al. showed a correlation between the level of SARS-CoV-2 antibodies on serology and lymphocyte count at 1 mo after the second dose in a cohort of 125 multiple sclerosis patients who were fully vaccinated with BNT162b2 COVID-19 vaccine (27). These results have been confirmed in 427 patients with hematologic malignancies who also received 2 doses of BNT162b2 COVID-19 vaccine, explored by serology (28). In this study, ALC correlated with a higher seropositivity likelihood and antibody titers. This observation is not surprising given the pivotal role of lymphocytes in the immune response, specifically because these are instrumental in the formation of antibodies (30). All these parameters are closely related to the humoral immune response; however, as stated by the authors of the previously cited studies, the role of lymphocytes in cell-mediated immune response after COVID-19 vaccination remains to be investigated.
On the basis of our findings, there is no evidence to support the conclusion that immunosuppression leads to a lower incidence of v-HLNs. Although we could say that chemotherapy or rituximab-containing regimens are likely to block the serologic response to COVID-19 (13) or influenza A (H1N1) vaccinations (31,32), the relationship between immunodepression and reactive HLNs in the drainage territory remains unclear from the literature. On the one hand, Thomassen et al. showed that immunosuppressive drugs given within 2 wk from vaccination did not affect axillary lymph node uptake in 293 patients who had been vaccinated with at least 1 influenza vaccination in the deltoid region (9). On the other hand, Cohen et al. revealed that lymphoma patients treated during the year before COVID-19 vaccination with rituximab-containing regimens (9%) had significantly lower rates of v-HLNs than did all other lymphoma patients (41%), associated with a strong relationship between v-HLNs and positive serologies (Spearman ρ = 0.64 in patients who received the 2 doses of mRNA vaccine) (13). These results are strengthened by a study by Eifer et al. demonstrating a strong inverse association between v-HLNs and immunosuppressive therapies (OR, 0.37; 95% CI, 0.20–0.64; P < 0.01) in a large cohort of 377 patients after mRNA-based COVID-19 vaccination (14). However, the determinants that correlated with the high glucose metabolism in the lymph node could be multiple, with, for example, age or lymphocyte count or timing of last injection dose having a higher degree of association. Further analyses are needed to explore the specific relationship between v-HLNs, immune status, and the immune response to the COVID-19 vaccine.
In the specific case of early-stage BC patients, it is usually recommended that vaccine be administered in the arm opposite the BC side. However, in rare cases, early-stage BC patients could have bilateral cancers or receive the vaccine injection in the arm ipsilateral to the known tumor, which might falsely influence the PET report. We thus studied patients with axillary HLNs ipsilateral to the recently vaccinated arm but also ipsilateral to the known tumor, and we found signs of malignancy, with tumor cells in half the patients whereas the other half had benign reactive changes. The sample size (n = 7) was too small to allow a statistical analysis or to draw any conclusion. Unfortunately, because blood sample analysis was not available for all these patients, we could not determine whether patients with benign reactive changes had significantly higher ALCs than patients with signs of malignancy. Since the date of PET examination could hardly be postponed in cancer patients, predicting the nature of HLNs on 18F-FDG PET/CT has become an area of intensive investigation to avoid unnecessary biopsies or aggressive treatments. As a result, the 3 parameters (age, timing of last injection dose, and ALC) that we identified in the current study may help to guide nuclear medicine physicians in interpreting 18F-FDG PET/CT images and oncologists in choosing whether to perform a biopsy. Further research is required to validate such findings and identify clinical, biologic, and imaging factors associated with the nature of HLNs (benign vs. malignant) ipsilateral to the breast tumor in a larger cohort of patients with early-stage BC.
The strength of our study is the large sample size. The main limitation concerns the retrospective nature and single-center design. We did not include sex in our logistic regression analysis because of a sample-selection bias, explained by the predominance of women, who account for 80%. Indeed, this sex bias in favor of women is due to the nature of our center, which is a referral one for BC treatment. Moreover, only 10% of patients received the viral vector–based COVID-19 vaccine. Consequently, we cannot conclude with sufficient power the specific vaccine-subtype effects on the 18F-FDG PET/CT response to SARS-CoV-2 vaccination.
Studies deciphering metabolic patterns on 18F-FDG PET/CT after vaccination are needed because annual vaccination against SARS-CoV-2 might be needed.
In any case, our work confirms the potential of 18F-FDG PET/CT as a potent tool to assess immune response after COVID-19 vaccination, as can be explained by the fact that immune response increases glucose metabolism in lymphoid organs (e.g., regional lymph nodes), which are critical modulators of immunity (33). Now proven to be more than 90% effective against SARS-CoV-2, the mRNA technology will probably modify the therapeutic armamentarium in patients with solid malignant tumors (34). However, it remains to be demonstrated that 18F-FDG PET/CT can, in its widest sense, become a relevant imaging tool for in vivo quantification of the immune response in healthy lymphoid tissues after mRNA vaccination (8).
CONCLUSION
In this large cohort of 260 patients, we demonstrated that patient ALC was a critical determinant of v-HLNs on 18F-FDG PET/CT after mRNA based- or viral vector–based COVID-19 vaccination, as well as patient age and timing of last injection dose. In BC patients, normal values of ALC after vaccination and before 18F-FDG PET/CT were the best indicator of the v-HLN status. Both of these interrelated elements (age and ALC) might modulate the quality of the immune response after COVID-19 vaccination. Further prospective studies are warranted to investigate whether the metabolism of lymphoid organs on 18F-FDG PET/CT is a crucial effector of the immune response after COVID-19 vaccination.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Can we use ALC to predict the presence of v-HLNs in the drainage territory on 18F-FDG PET/CT after COVID-19 vaccination?
PERTINENT FINDINGS: Patient ALC (>lower limit of normal), patient age (≤50 y), and timing of last injection dose (<30 d before PET) significantly correlated with v-HLNs.
IMPLICATIONS FOR PATIENT CARE: Patients displaying a normal ALC after COVID-19 vaccination are more likely to show v-HLNs on 18F-FDG PET/CT and may subsequently have a higher seropositivity likelihood and antibody titers.
Footnotes
Published online Dec. 2, 2021.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
Immediate Open Access: Creative Commons Attribution 4.0 International License (CC BY) allows users to share and adapt with attribution, excluding materials credited to previous publications. License: https://creativecommons.org/licenses/by/4.0/. Details: http://jnm.snmjournals.org/site/misc/permission.xhtml.
REFERENCES
- Received for publication August 20, 2021.
- Accepted for publication November 9, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.