


Visual Abstract
Abstract
Preoperative localization of pathologic parathyroids is crucial for minimally invasive treatment of primary hyperparathyroidism (PHPT). This study compared contrast-enhanced 18F-fluorocholine PET/CT, cervical ultrasonography (CU), and conventional scintigraphic imaging modalities (MIBI scintigraphy, consisting of 99mTc-sestamibi/123I-sodium iodide SPECT/CT, 99mTc-sestamibi/123I-sodium iodide planar subtraction imaging, and 99mTc-sestamibi planar dual-phase imaging), combined and individually, for preoperative localization of hyperfunctional parathyroids in PHPT. The gold standard was histologic examination. Methods: Data from consecutive patients with clinically suspected PHPT were retrospectively collected. All 3 imaging modalities were systematically performed. The ability of 18F-fluorocholine PET/CT, CU, and MIBI scintigraphy to identify a hyperfunctional parathyroid and specify the side or identify an ectopic location was noted. Patients underwent surgical exploration if at least 1 examination was positive. The findings of CU + MIBI scintigraphy combined were considered positive if CU and MIBI scintigraphy separately showed a hyperfunctional parathyroid gland on the same side or in the same ectopic location; any findings other than these were considered negative. The composite judgment criterion for pathologic parathyroid was a combination of histologic analysis and normalization of parathyroid hormone and calcium levels. Results: In total, 149 pathologic parathyroids were found in 143 of the 144 included patients. 18F-fluorocholine PET/CT diagnosed 148 of 149 pathologic parathyroids. Only 4 false-positives and 1 false-negative were found. The 18F-fluorocholine PET/CT sensitivity of 99.3% was superior to that of CU, at 75.2% (P < 0.0001); MIBI scintigraphy, at 65.1% (P < 0.0001); and CU + MIBI scintigraphy, at 89.9%, (P = 0.0009). Five of the 5 ectopic locations were diagnosed by 18F-fluorocholine PET/CT, 2 of the 5 by MIBI scintigraphy, and none by CU. Accuracy was better for 18F-fluorocholine PET/CT, at 98%, than for CU, at 84% (P < 0.0001); MIBI scintigraphy, at 81% (P < 0.0001); or CU + MIBI scintigraphy, at 91% (P < 0.0001). Among the 72 (50%) patients who had a negative CU + MIBI scintigraphy result, 18F-fluorocholine PET/CT correctly identified hyperfunctional thyroids in 70 (97.2%). Average uptake in the 18F-fluorocholine PET/CT hyperfunctional parathyroid was higher than that in the adjacent thyroid (SUVmax adjusted for lean body mass, 6.45 vs. 2.15) (P < 0.0001). Conclusion: The accuracy of 18F-fluorocholine PET/CT is higher than that of CU and MIBI scintigraphy for localization of hyperfunctional parathyroids, justifying the systematic use of 18F-fluorocholine PET/CT as the first-line method for PHPT diagnosis.
- 18F-fluorocholine
- primary hyperparathyroidism
- parathyroid adenoma
- 99mTc-sestamibi scintigraphy
- cervical ultrasound
Primary hyperparathyroidism (PHPT) is a pathology characterized by the presence of long-lasting hypercalcemia associated with inappropriate hyperparathyroidism. Idiopathic parathyroid adenomas are the most common cause of this pathology. PHPT treatment is mainly surgical, consisting of resection of pathologic parathyroids (1). Previously, parathyroids were located via an exploration of the 4 parathyroid sites. However, the currently favored technique is to identify and precisely locate the pathologic parathyroids by imaging in order to propose a faster, safer targeted intervention.
For many years, the gold standard for preoperative localization assessment has been cervical ultrasonography (CU) combined with 99mTc-sestamibi (MIBI) scintigraphy (CU + MIBI scintigraphy) to provide supplementary anatomic and functional information. However, the results of these examinations are negative or questionable in 10%–25% of cases (2,3), leading to further surgical explorations, the results of which are often equivocal, or to regular monitoring with repeated examinations. Defining the best diagnostic tool to minimize negative or equivocal identification is an important challenge in the surgical treatment of PHPT.
18F-fluorocholine is a marker of membrane proliferation, initially used to detect cancerous tissue of prostate origin. This radiopharmaceutical can also be sensitively and intensely absorbed by hyperfunctional parathyroid tissue. The preliminary data in the literature suggest that 18F-fluorocholine PET/CT would be beneficial when CU + MIBI scintigraphy of a parathyroid adenoma gives equivocal results (4). In practice, it has quickly become obvious that 18F-fluorocholine PET/CT may have diagnostic value superior to that of CU + MIBI scintigraphy and may soon become the gold standard first-line method for PHPT.
To test this hypothesis, we aimed to compare the diagnostic performance of CU, MIBI scintigraphy, 18F-fluorocholine PET/CT, and CU + MIBI scintigraphy for preoperative identification of hyperfunctional parathyroids in PHPT.
MATERIALS AND METHODS
This was a single-center, retrospective study on patients included from July 2016 to January 2020 at the ear, nose, and throat; endocrinology; and nuclear medicine departments of a French university hospital. The institutional review board approved this retrospective study, and the requirement to obtain informed consent was waived.
Patients
The study included adults who had been referred for surgical consultation regarding PHPT and had at least 1 image indicating a hyperfunctional parathyroid gland on at least 1 of the imaging modalities (CU, MIBI scintigraphy, or 18F-fluorocholine PET/CT) between July 2016 and January 2020. The participants formed a consecutive series. PHPT was defined by hypercalcemia (>2.55 mmol/L) associated with high serum parathyroid hormone (PTH) levels or inappropriate levels in the absence of vitamin D deficiency. Patients who had an associated nodular dystrophy of the thyroid were included, but any who had previously undergone surgery of the thyroid compartment were excluded, as were any who had another pathologic condition that could modify phosphocalcic metabolism, such as chronic renal failure, hyper- or hypovitaminosis D, sarcoidosis, multiple endocrine neoplasia, or progressive neoplasia.
Over the 43-mo recruiting period, 157 patients with PHPT underwent all imaging studies; 144 fulfilled the inclusion criteria by having a positive target on at least 1 of the imaging modalities and underwent surgery. The patient characteristics are described in Table 1. Briefly, we included 26 men and 118 women, with a mean age of 63 y (25–92 y) and a mean preoperative PTH level of 143 pg/mL (39–849 pg/mL).
Characteristics of PHPT Patients Who Underwent Surgery (n = 144)
Preoperative Examinations
All patients underwent CU, MIBI scintigraphy, and 18F-fluorocholine PET/CT in no set order. For each examination, the presence or absence of images suggestive of a hyperfunctional parathyroid gland was noted, along with their position in the left and right thyroid beds and ectopically. We did not differentiate the upper and lower positions. Questionable images were considered negative in the treatment decision and in analysis of the results. The radiologists who evaluated the images knew the results of the other examinations. Patients without surgical targets on the 3 imaging modalities did not undergo surgery and were not included in the study.
High-Resolution CU
CU was performed by an experienced radiologist on an iU22 high-resolution ultrasound scanner (Philips) (first used in 2012). The patient was examined supine, with the neck in extension. CU was performed using high-frequency linear transducers (7–12 MHz) for cervical examination over a field extending from the angles of the mandible to the sternal notch. The upper mediastinum was studied using an endocavitary probe for retrosternal exploration (4.5–7.2 MHz probe). Transversal and longitudinal views were obtained; images of regions of interest were recorded as video images. The parathyroid glands were sought on the posterior side of the thyroid lobes and on all cervical and upper mediastinal ectopic sites. A parathyroid was defined as pathologic (adenoma or hyperplasia) if the gland was elongated or flattened, hypoechoic, and separated from the thyroid parenchyma by a wall, which was mobile on swallowing and well vascularized. The thyroid parenchyma was also analyzed, and any possible dystrophy was described in detail.
Conventional Scintigraphic Imaging
Conventional (i.e., non-PET/CT) scintigraphic imaging (MIBI scintigraphy) consisted of 99mTc-sestamibi/123I sodium iodide SPECT/CT, 99mTc-sestamibi/123I-sodium iodide subtraction imaging, and 99mTc-sestamibi dual-phase imaging. A combined-imaging protocol was used, enabling same-day acquisition of all 3 modalities. Scintigraphy was performed on a Discovery 670 imager (GE Healthcare). The γ-camera was equipped, first, with a pinhole collimator allowing a cervical planar acquisition and, second, with low-energy, high-resolution collimators allowing a cervicothoracic planar and tomography acquisition. A matrix of 256 × 256 was used with, for dual-isotope acquisition, a 10% energy window centered on 159 keV (recommended for 123I), and a 15%–20% window centered on 140 keV (recommended for 99mTc). A 16-MBq dose of 123I was injected, followed 2 h later by a 10 MBq/kg dose of 99mTc-sestamibi. Five minutes after the last injection, a double-isotope planar pinhole cervical acquisition was performed for 10 min. After the collimator had been changed, a cervicothoracic early planar double-isotope acquisition and a SPECT double-isotope acquisition combined with cervicothoracic CT were performed for 15 min. Ninety minutes later, another cervical planar acquisition was done (delayed planar image of dual-phase protocol). The following images were obtained: an early and delayed large field-of-view planar image of the neck and mediastinum (from the skull base to the heart base), a pinhole double-isotope view of the thyroid bed region, and a cervicothoracic SPECT/CT double-isotope acquisition. Unless there was a contraindication, iodinated contrast medium was injected 80 s before the CT acquisition to improve visualization of the CT and fused images.
For dual-phase imaging analysis, early and delayed 99mTc-sestamibi planar images were compared; regional uptake of 99mTc-sestamibi with slower washout than from thyroid tissue was considered to represent hyperfunctioning parathyroid tissue.
For dual-tracer protocols, images were inspected visually and normalized to thyroid counts, and 123I images were subtracted from the 99mTc images in the thyroid gland and surrounding soft tissue. Persistence of a focal accumulation of radiopharmaceutical adjacent to the thyroid after subtraction was considered suggestive of a hyperfunctioning parathyroid gland.
For SPECT/CT imaging, regional 99mTc-sestamibi uptake not associated with thyroid tissue visualized on 123I or CT images was considered to represent hyperfunctioning parathyroid tissue. Physiologic hyperuptake (salivary glands, inflammatory lymph nodes) was not retained.
This study performed a combined assessment of the 3 conventional scintigraphic imaging methods, with any positive finding—according to the interpretation criteria described above—being considered to represent hyperfunctioning parathyroid tissue.
18F-Fluorocholine PET
18F-fluorocholine PET/CT was performed 1 h after intravenous injection of a dose ranging from 150 to 185 MBq of 18F-fluorocholine, using a Discovery PET/CT 710 Elite imager (GE Healthcare). The strategy was to obtain first a CT topogram, then a low-dose attenuation-correction CT scan, then a PET acquisition, and finally an additional intravenous contrast-enhanced diagnostic CT scan. When contrast medium was contraindicated, a diagnostic CT scan was performed instead of the attenuation-correction CT scan. The acquisition protocol included a thickness of 2.5 mm, an interval of 1.25 mm, a display field of view of 70, tension of 120 kV, and automatic mA regulation. The acquisition was centered on the cervicothoracic region. Iterative reconstruction of PET images was performed with the Q-Clear algorithm (GE Healthcare) to improve the signal-to-noise ratio using a β of 600. Because contrast-enhanced CT allowed more precise anatomic localization, iodinated contrast medium—unless contraindicated—was injected 80 s before the CT acquisition to optimize the CT and fused-image analysis. Neck or mediastinal hyperuptake matching a scanner image compatible with an adenoma or hyperplasia was considered a hyperfunctional parathyroid. Physiologic hyperuptake (salivary glands, inflammatory lymph nodes) was not retained. The SUVmax adjusted for lean body mass (SULmax) was calculated to quantify the intensity of uptake.
Surgery
All patients with at least 1 image indicating a hyperfunctional parathyroid gland on at least 1 imaging modality underwent surgery. The same 2-cm lateral incision was used, allowing access to both upper and lower locations. If bilateral exploration was necessary, a midline incision was made. The hyperfunctional parathyroid tissue was located and removed with a retrothyroid approach under general or local anesthesia. If there was any doubt about the nature of the resected tissue, an extemporaneous anatomopathologic analysis was used to confirm the presence of parathyroid tissue. Surgery could be combined with a thyroid lobectomy when there were suggestive or questionable thyroid nodules on the preoperative evaluation. When the surgeon found no pathologic parathyroid tissue during the surgical exploration, complete emptying of the laterotracheal fatty cell tissue (level VIb) was performed to limit the risk of operator-related failure to identify a pathologic parathyroid.
Statistical Analysis
The diagnostic values were defined using a judgment criterion combining histologic analysis (pathologic tissue: adenoma/hyperplasia or normal) and the biologic workup (postoperative normalization of PTH and calcium (5)). Images evoking a hyperfunctional parathyroid were considered true-positive if confirmed as a pathologic parathyroid on histologic examination or false-positive if not. In the absence of an evocative image, if surgical exploration was performed (i.e., in the event of conflicting results between the different types of images), the result was considered true-negative if no hyperfunctional parathyroid was found or false-negative if a pathologic parathyroid was found. For parathyroid sites not surgically explored because of negative imaging by all methods, the result was considered true-negative if a hyperfunctional parathyroid was found on contralateral surgical exploration and the biologic test results normalized, or a result was considered impossible to conclude if no hyperfunctional parathyroid was found after contralateral surgical exploration and the biologic test results had not returned to normal. For each examination method, sensitivity, specificity, positive predictive, and negative predictive values and their 95% CIs were calculated.
The accuracy, sensitivity, and specificity of 18F-fluorocholine PET/CT were compared with the performance of CU, MIBI scintigraphy, and CU + MIBI scintigraphy.
The results of CU + MIBI scintigraphy were considered positive if CU and MIBI scintigraphy separately showed a hyperfunctional parathyroid gland on the same side. The results were considered negative if there was a discrepancy between CU and MIBI scintigraphy or if both were negative. A McNemar test for paired data was used for the comparison. A P value of less than 0.02, adjusted for multiple comparisons with a Bonferroni adjustment, was considered statistically significant.
The statistical analyses were done using the RStudio software, version 1.2.5001.
The scientific committee of the Nimes University Hospital Center approved the experiments.
RESULTS
For each patient, the pre- and postoperative PTH levels, the result of each preoperative examination to locate the parathyroids, and the histologic results (including size and weight) of the parathyroids were recorded (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org).
Surgical Results and Anatomopathologic Data
At least 1 hyperfunctional parathyroid was found in 143 of the 144 patients who underwent surgery. In total, 149 pathologic parathyroids were removed: 134 patients had a single parathyroid adenoma, 3 patients had isolated parathyroid hyperplasia, and 6 patients had a hyperfunctional parathyroid at 2 sites. In 1 patient, no pathologic parathyroid was found.
These pathologic glands were in the right thyroid compartment in 45.4% of cases (65/143), the left compartment in 46.9% of cases (67/143), the right and left thyroid compartments in 4.2% of cases (6/143), and an ectopic location in 3.5% of cases (5/143): 2 superior mediastinal, 1 midanterior mediastinal, 1 left retroesophageal, and 1 behind the left sternoclavicular joint. No adverse events were noted during the various imaging examinations.
Diagnostic Values for CU, MIBI Scintigraphy, and 18F-Fluorocholine PET/CT
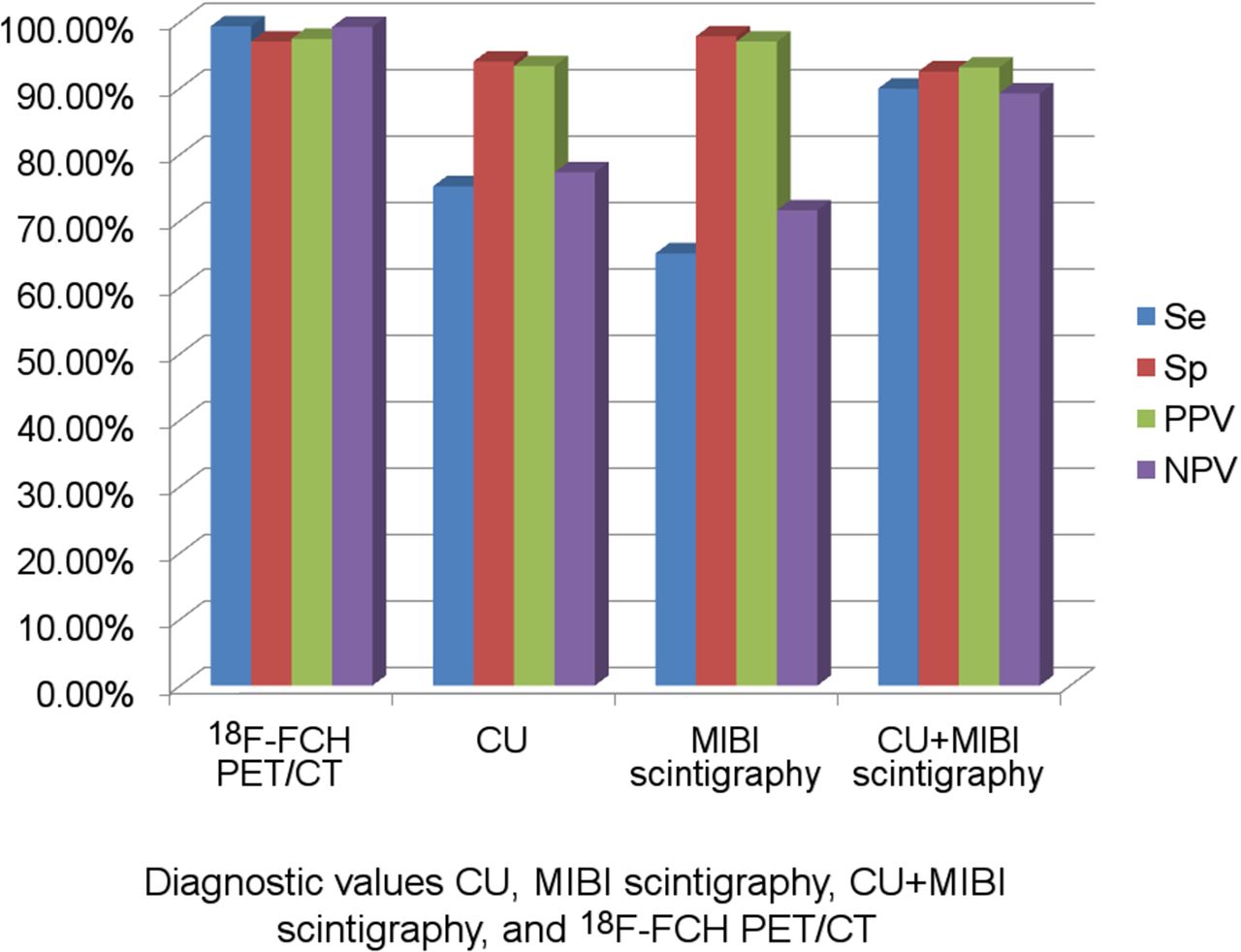
The diagnostic values for CU, MIBI scintigraphy, CU + MIBI scintigraphy, and 18F-fluorocholine PET/CT are given in Table 2. According to histologic confirmation, hyperfunctional parathyroids were correctly identified (true-positive) in 112 (75%) of the 149 cases by CU, in 97 (65%) by MIBI scintigraphy, in 148 (99%) by 18F-fluorocholine PET/CT, and in 134 (90%) by CU + MIBI scintigraphy (reference standard).
Diagnostic Values for CU, MIBI Scintigraphy, CU + MIBI Scintigraphy, and 18F-Fluorocholine PET/CT (n = 288)
CU wrongly diagnosed a hyperfunctional parathyroid (false-positive) in 8 cases, compared with 3 for MIBI scintigraphy and 4 for 18F-fluorocholine PET/CT.
The 18F-fluorocholine PET/CT sensitivity was higher than that of CU (P < 0.0001) or MIBI scintigraphy (P < 0.0001), alone or combined (P = 0.0009). Finally, accuracy was better for 18F-fluorocholine PET/CT, at 98%, than for CU, at 84% (P < 0.0001), MIBI scintigraphy, at 81% (P < 0.0001), or CU + MIBI scintigraphy, at 91% (P < 0.0001).
In 72 patients (50%), the results of CU versus MIBI scintigraphy were conflicting or found no adenomas. In these negative or equivocal situations, 18F-fluorocholine PET/CT correctly identified hyperfunctional thyroids in 70 (97.2%) patients.
Analysis of Incorrect 18F-Fluorocholine PET/CT Results
18F-fluorocholine PET/CT generated 4 false-positive images (patients 4, 64, 82, and 124), which might have been due to localization to a thyroid nodule or lymph node. 18F-fluorocholine PET/CT generated 1 false-negative image (patient 87).
Ectopic Locations
Five patients had a hyperfunctional parathyroid in an ectopic location (2 superior anterior mediastinal, 1 midanterior mediastinal, 1 left retroesophageal, and 1 behind the left sternoclavicular joint). CU did not locate pathologic parathyroids in these ectopic situations (0/5 cases), and MIBI scintigraphy found only 1 case. In contrast, 18F-fluorocholine PET/CT located all of them.
Analysis of SULmax of Hyperfunctional Thyroids and Comparison with Physiologic SULmax of Thyroid
We compared the SULmax of the parathyroids against that of the adjacent thyroid parenchyma with physiologic 18F-fluorocholine uptake. The average SULmax was 6.45 (SD, 3.15) for hyperfunctional parathyroids, compared with 2.15 (SD, 0.79) for the thyroid. Thus, the SULmax of hyperfunctional parathyroids averaged 200% higher than that of the thyroid parenchyma (P < 0.0001). The difference in 18F-fluorocholine uptake between the parathyroid and thyroid, combined with the spatial analysis of the distant parathyroid, facilitates interpretation of the examination. Only patient 31 had a parathyroid SULmax lower than the thyroid SULmax (4.00 vs. 4.82, −17%). This patient had a previous history of Hashimoto thyroiditis with a relatively high thyroid uptake, which might explain the current high thyroid uptake. However, there were no difficulties in diagnosing the hyperfunctional parathyroid in this patient, as the parathyroid tissue was anatomically distinct from the thyroid.
DISCUSSION
This study was conceived because of the increasing number of centers using 18F-fluorocholine PET/CT to localize hyperfunctional parathyroid glands during PHPT, despite lack of sufficient data in the literature to justify use of this examination instead of the gold standard, CU + MIBI scintigraphy. The aim of this work was to compare the diagnostic value of 18F-fluorocholine PET/CT versus that of CU + MIBI scintigraphy. In this study, 18F-fluorocholine PET/CT had a sensitivity and negative predictive value of 99.0% (95% CI, 97%–100%), a specificity of 97.0% (95% CI, 95%–99%), and a positive predictive value of 97.4% (95% CI, 94%–99%). These diagnostic values are superior to those of CU (P < 0.0001) and MIBI scintigraphy (P < 0.0001), alone or combined (P = 0.0009). These results confirm and reinforce previously published preliminary data (6–16) on a larger series of patients.
Previous publications have suggested reserving 18F-fluorocholine PET/CT for situations in which CU + MIBI scintigraphy has failed to detect hyperfunctional thyroids. Our study demonstrated the clear diagnostic superiority of 18F-fluorocholine PET/CT and justifies its indication as a first-line technique in suspected PHPT.
Michaud et al. compared the 3 examinations for preoperative evaluation of primary and secondary hyperparathyroidism in 17 patients (6). Only 1 case of adenoma was poorly recognized by the 3 imaging methods. In this limited series, the sensitivities of CU, MIBI scintigraphy, and 18F-fluorocholine PET/CT were 42%, 83%, and 96%, respectively.
Another study evaluated the benefit of MIBI scintigraphy and 18F-fluorocholine PET/CT in 24 patients with PHPT (7). Sensitivity was significantly better with 18F-fluorocholine PET/CT (92%) than with MIBI scintigraphy (44%–64%, depending on the acquisition technique). A prospective study on 54 patients with PHPT compared CU, MIBI scintigraphy, and 18F-fluorocholine PET/CT (8). In this study, the sensitivity of the 3 imaging techniques was 69.3%, 80.7%, and 100%, respectively, and the positive predictive values were 87.1%, 97.7%, and 96.3%, respectively.
In a prospective series of 18 suspected parathyroid adenoma sites, 17 adenomas were correctly located by 18F-fluorocholine PET/CT, with 1 false-positive, producing a sensitivity of 89% (9), comparable to the sensitivity of 90% and a positive predictive value of 100% found in another prospective series of 10 patients (10). A retrospective series of 151 patients who underwent surgery for PHPT and for whom 18F-fluorocholine PET/CT was performed at the preoperative evaluation (11) found a positive predictive value of 96.8%. Unfortunately, CU and MIBI scintigraphy were not systematically performed, preventing direct comparison.
Finally, in a recent metaanalysis on 20 studies including a total of 796 patients, Whitman et al. reported that 18F-fluorocholine PET/CT had a superior sensitivity of 96% (95% CI, 94%–98%), compared with 54% (95% CI, 29%–79%) for MIBI scintigraphy (P < 0.001). In these studies, like ours, limited to patients with PHPT, 18F-fluorocholine PET/CT had a superior sensitivity of 97% (95% CI, 94%–100%), compared with 55% (95% CI, 32%–78%) for MIBI scintigraphy (12). In our study, MIBI scintigraphy had a sensitivity of 65.1% (95% CI, 57%–72%); this can be compared with the 10 studies (301 patients) included for comparison with MIBI scintigraphy in the metaanalysis. Six (including 41% of the analyzed patients) used dual-phase, dual-tracer sestamibi imaging with SPECT/CT. Three used SPECT, 2 of which used use sestamibi alone. One did not describe the sestamibi imaging. The heterogeneity of techniques used for MIBI scintigraphy can lead to inconsistencies between the studies used for the comparison analysis. The same conventional scintigraphic imaging methods (99mTc-sestamibi SPECT/CT, 99mTc-sestamibi/pertechnetate subtraction imaging, and 99mTc-sestamibi dual-phase imaging) were used by Cuderman et al. on 103 PHPT patients imaged preoperatively, with a sensitivity of 65%. This sensitivity was similar to that found in our study (13).
18F-fluorocholine PET/CT has numerous advantages that justify its systematic use for the initial evaluation of hyperfunctional parathyroids in patients with clinically suspected PHPT. First, its diagnostic values are statistically better than those of CU + MIBI scintigraphy, making the preoperative evaluation more reliable for locating hyperparathyroids. Second, 18F-fluorocholine PET/CT is more efficient and generated a lower radiation dose than MIBI scintigraphy. Indeed, 18F-fluorocholine PET/CT requires shorter acquisition times—1 h after injecting the tracer for 18F-fluorocholine PET/CT compared with over 2 h for MIBI scintigraphy—and the patient spends less time under the camera and thus experiences less discomfort. 18F-fluorocholine PET/CT produces better image quality due to a higher spatial resolution (13–16), around 4 mm on the latest-generation PET scanner, and a better-quality mobile scanner, allowing diagnosis of smaller lesions and increased sensitivity. Whole-body 18F-fluorocholine PET/CT emits less radiation than MIBI scintigraphy, with an effective dose of 2.8 mSv versus 6.8 mSv (17).
Third, 18F-fluorocholine PET/CT is the best examination for identifying ectopic adenomas. In a previous study on 54 patients, of whom 6 had hyperfunctional thyroids in ectopic locations (2 mediastinal, 2 in the tracheoesophageal corner, 1 paravertebral, and 1 in the mammary tissue), only 18F-fluorocholine PET/CT correctly identified all parathyroid adenomas (8). Similarly, in another study, 1 ectopic parathyroid adenoma in 10 patients was correctly identified by 18F-fluorocholine PET/CT and MIBI scintigraphy but was missed by CU (10). In another study, consisting of 63 patients, 5 patients underwent 18F-fluorocholine PET/CT because of discordant CU and MIBI scintigraphy, and 1 case of mediastinal adenoma was diagnosed, having been missed by the 2 other imaging techniques (18). For Taywade et al., of 7 parathyroid adenomas diagnosed, 3 were ectopic parathyroids with strong 18F-fluorocholine uptake (19). In our study, all 5 ectopic parathyroids from 144 patients were correctly identified with 18F-fluorocholine PET/CT.
Finally, 18F-fluorocholine PET/CT is a less operator-dependent examination and therefore more reliable than ultrasound scanning. Thyroid nodular dystrophy can easily lead to confusion between a thyroid nodule and the parathyroid on ultrasound scans, even with a skilled operator. In our experience, this confusion is much less common with an 18F-fluorocholine PET/CT examination. Indeed, physiologic 18F-fluorocholine uptake is low in the thyroid and is almost always lower than that of the parathyroid tissue. In the rare cases of hot thyroid nodules, CT analysis can easily distinguish between intraparenchymal uptake and uptake at a distance from the thyroid parenchyma. To the best of our knowledge, in the literature no association has been described between thyroiditis and strong 18F-fluorocholine uptake of the thyroid. In our study, the only patient with a parathyroid SULmax lower than that of the thyroid had Hashimoto thyroiditis. Therefore, we suggest particular attention when one is interpreting a 18F-fluorocholine PET/CT scan that shows positivity for antithyroid antibodies and a parathyroid adenoma contiguous with the thyroid, as the risk of a false-negative could be greater in such a case. This situation may also lead to problems in rare cases of intrathyroid parathyroid adenomas.
The fact that all CUs in our study were performed by a highly experienced operator (∼100 ultrasound parathyroid scans and 1,200 thyroid ultrasound scans per year) probably explains why the diagnostic values of the ultrasound scan were above those generally described in the literature. The MIBI scintigraphy was performed with injected iodine in our study, thus increasing its diagnostic values compared with other centers. The nuclear medicine physicians were experienced in analyzing 18F-fluorocholine PET/CT cervical images but not for this indication. Nevertheless, the diagnostic values of 18F-fluorocholine PET/CT were higher than those of CU, demonstrating the less operator-dependent nature of this examination than of ultrasound scanning.
The main disadvantages of 18F-fluorocholine PET/CT are the inaccessibility and high cost. Certain authors suggest reserving 18F-fluorocholine PET/CT for when there is a disagreement or negative results with CU and MIBI scintigraphy (6,9,10,20–22). In our study, the results of CU and MIBI scintigraphy were discordant or negative for 50% of cases, and in 97.2% of these situations 18F-fluorocholine PET/CT gave the correct location of hyperfunctional parathyroids. These results reinforce the idea of using 18F-fluorocholine PET/CT alone as a first-line option, as suggested by Bossert et al. (23).
This work had limitations. It was a single-center, retrospective analysis, with the biases that this design entails, especially regarding a center effect. The study included only patients with at least 1 positive image, probably leading to selection of patients with higher biochemical profiles and larger adenomas or hyperplastic glands and excluding patients with milder disease. This effect would inflate the diagnostic accuracy measures. The median weight of resected parathyroids was 1.12 g (range, 0.1–7.5 g), compared with 0.4 g (range, 0.1–10.9 g) in the 103 patients tested in a previous study (15). Nevertheless, the mean preoperative PTH level was 143 pg/mL (range, 39–849 pg/mL), similar to the 145 pg/mL (range, 40–1,076 pg/mL) in that previous study. Moreover, we did not consider in this study patients affected by hyperparathyroidism with normal levels of calcium, even though patients with normal levels of calcium but with symptoms may be scheduled for surgery. The result could be a bias in the accuracy evaluation. For some authors, 18F-fluorocholine PET/CT could be considered a first-line imaging technique for the identification of pathologic parathyroid glands in patients with normocalcemic and hypercalcemic hyperparathyroidism, even when the parathyroid volume is small (22). Furthermore, the order of the examinations was not standardized, and comparisons were not performed with masking of the results of the other imaging techniques. We also did not differentiate the upper and lower localizations on the imaging results. This distinction is highly subjective and interpreter-dependent, and there is little value to distinguishing between upper and lower because the same surgical approach is used. Making this distinction would have no impact on the different diagnostic values. The 18F-fluorocholine PET/CT acquisition was performed using a 60-min delay after injection, rather than 15 min as chosen by some teams; thus, adenomas with fast tracer washout might have been missed (24). This is relevant in only a small number of cases (potentially 1 in our series). It is essential to pursue this work by performing a complete medicoeconomic study on the 3 techniques.
CONCLUSION
The diagnostic values of 18F-fluorocholine PET/CT found in this study were clearly superior to those of CU and MIBI scintigraphy for preoperative localization of pathologic hyperfunctional parathyroid glands in PHPT. To the best of our knowledge, with 144 patients having undergone surgery, this is the largest comparative cohort in the literature. This superiority seems related to a strong contrast between the uptake of hyperfunctional parathyroids and the neighboring tissue and to a high spatial resolution allowing detection of small or ectopic parathyroids, which may be missed by other imaging techniques. We suggest using 18F-fluorocholine PET/CT as a first-line examination in preference to CU and MIBI scintigraphy.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: How does 18F-fluorocholine PET/CT compare with CU, MIBI scintigraphy, or CU + MIBI scintigraphy for diagnostic localization of hyperfunctional parathyroid glands during PHPT?
PERTINENT FINDINGS: In this single-center, retrospective study of 144 patients, 18F-fluorocholine PET/CT had a sensitivity and negative predictive value of over 99.0%, a specificity of 97.0%, and a positive predictive value of 97.3%. These diagnostic values are superior to those of CU and MIBI scintigraphy, alone or combined, and confirm and reinforce—in a larger series of patients—previously published preliminary data.
IMPLICATIONS FOR PATIENT CARE: Previous publications have suggested reserving 18F-fluorocholine PET/CT for situations in which CU + MIBI scintigraphy has failed to detect hyperfunctional thyroids, but our study demonstrated the clear diagnostic superiority of 18F-fluorocholine PET/CT and justifies its use as a first-line technique in suspected PHPT.
ACKNOWLEDGMENT
We thank Sarah Kabani, medical writer, for editing the manuscript.
Footnotes
Published online Dec. 2, 2021.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication January 22, 2021.
- Revision received November 8, 2021.
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.