


Visual Abstract
Abstract
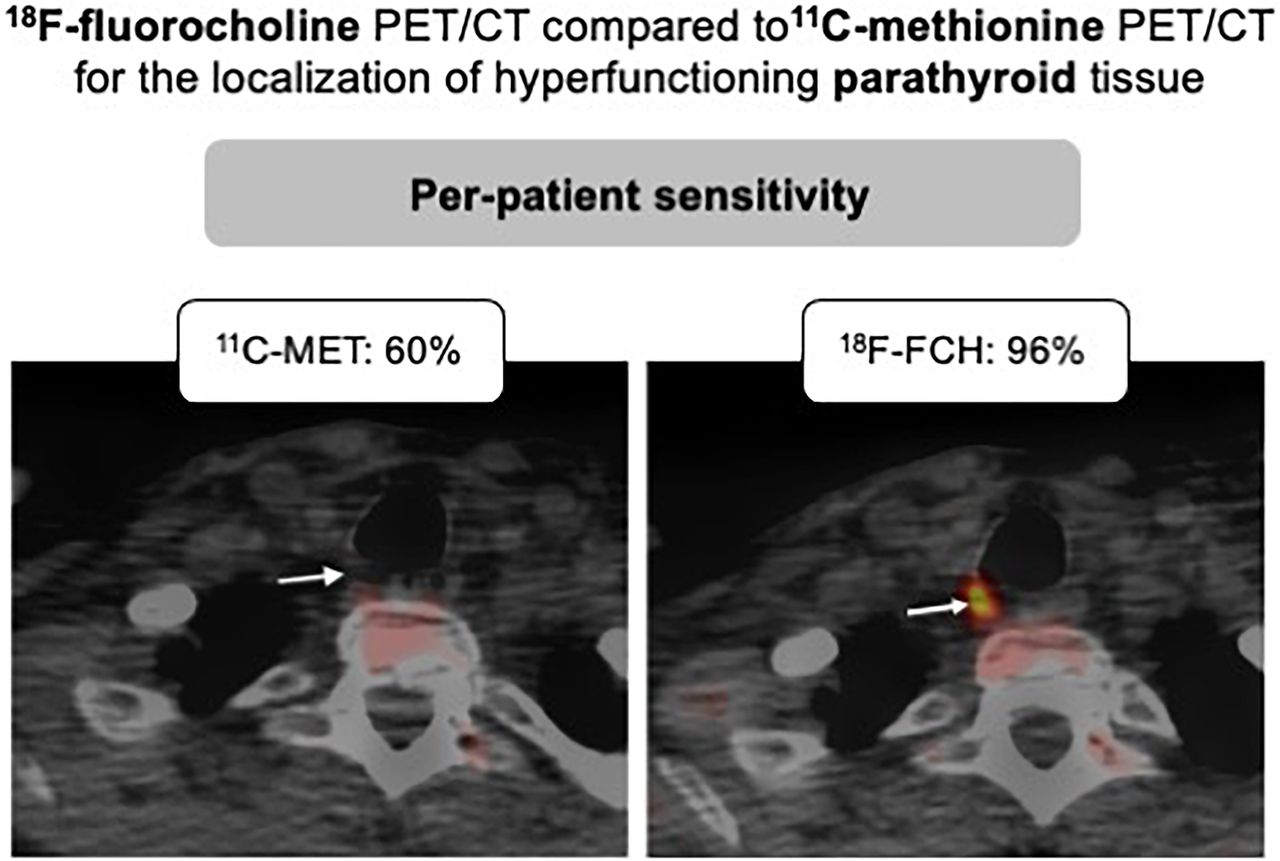
Preoperative molecular imaging is paramount to direct surgery in primary hyperparathyroidism (pHPT). We investigated the diagnostic performance of 18F-fluorocholine (18F-FCH) PET/CT compared with 11C-methionine (11C-MET) PET/CT for localization of hyperfunctioning parathyroid tissue in patients with pHPT and negative or inconclusive 99mTc-sestaMIBI (99mTc-MIBI) SPECT findings. Methods: Fifty-eight patients with biochemical evidence of pHPT and negative or inconclusive 99mTc-MIBI SPECT findings were referred for presurgical detection and localization of hyperfunctioning parathyroid tissue by 11C-MET and 18F-FCH PET/CT. The PET/CT results were classified into 3 categories (positive, inconclusive, or negative) based on the nodular aspect of tracer uptake and the visualization of corresponding nodules on CT. The PET/CT results were correlated with the surgical and histopathologic findings, which were used as the gold standard. Results: Fifty-three patients were included for analysis. 18F-FCH PET/CT was positive in 39 patients (74%), inconclusive in 5 (9%), and negative in 9 (17%), compared with 25 (47%), 12 (23%), and 16 (30%), respectively, for 11C-MET PET/CT. 18F-FCH localized 11 additional foci (6 positive and 5 inconclusive), compared with 11C-MET. Twenty-six patients (sex ratio, 10/16 M/F) underwent surgery, with resection of 31 lesions (22 adenomas, 6 hyperplastic glands, and 3 carcinomas) and 1 normal gland. At follow-up, 21 patients (81%) were considered cured after surgery, whereas 3 patients (12%) had persistence of hypercalcemia. With inconclusive cases being considered negative, 18F-FCH PET/CT correctly localized 26 lesions in 24 of 26 patients (92%), compared with 16 lesions in 15 of 26 patients (58%) localized by 11C-MET PET/CT. Per-patient–based sensitivity and positive predictive value were 96% and 96%, respectively, for 18F-FCH and 60% and 94%, respectively, for 11C-MET (P < 0.0001). Per-lesion–based sensitivity and positive predictive value were 84% and 90%, respectively, for 18F-FCH and 52% and 94%, respectively, for 11C-MET (P < 0.0001). Conclusion: In the presence of biochemical evidence of pHPT with negative or inconclusive 99mTc-MIBI SPECT findings, 18F-FCH PET/CT performs better than 11C-MET PET/CT for the detection of pathologic parathyroid tissue, allowing localization of parathyroid adenoma or hyperplasia in 96% of patients.
Primary hyperparathyroidism (pHPT) is one of the most frequent endocrine disorders, with a prevalence of about 2% in women older than 50 y. Long-term consequences of pHPT affect mainly the skeleton (osteoporosis, fractures) and the kidney (nephrolithiasis, impaired renal function). Diagnosis is based on increased serum calcium, low phosphorus levels, and inappropriate parathyroid hormone (PTH) levels (1). pHPT is associated with a solitary parathyroid adenoma (PA) in 80%–90% of patients or, more rarely, multiglandular disease or diffuse parathyroid hyperplasia (1).
Optimal management of pHPT consists of preoperative localization of the abnormal parathyroid gland, allowing for minimally invasive parathyroidectomy (2,3). Conventional first-line presurgical imaging is based on 99mTc-sestaMIBI (99mTc-MIBI) parathyroid scintigraphy with subtraction images, usually complemented by ultrasonography. It ideally includes a SPECT/CT acquisition, with a detection rate of 84%–88% (4,5).
Currently, in cases of negative or equivocal scintigraphy results, results discrepant with ultrasonography, or persistence or recurrence of HPT after surgery, an alternative investigation is recommended involving hybrid PET/CT technique, usually with an amino acid tracer such as 11C-methionine (11C-MET) (6,7). Use of PET/CT for that purpose offers a shorter acquisition time and higher spatial resolution and sensitivity (8). Metaanalyses reported 11C-MET to have sensitivity of 77%–81% in a per-patient–based analysis in patients with pHPT and negative or inconclusive 99mTc-MIBI SPECT findings (6,9). However, the short half-life of 11C-MET imposes on-site production and strict acquisition conditions (6).
More recently,18F-fluorocholine (18F-FCH) PET/CT used for imaging prostatic neoplasia assessment (10) has been shown capable of localizing an abnormal parathyroid gland in patients with negative or inconclusive 99mTc-MIBI SPECT results (3,8,11,12). It has the advantages over 11C-MET of a longer half-time and a more favorable positron energy. Choline is a precursor of phospholipids, which are essential constituents of cellular lipidic structures. 18F-FCH is therefore a tracer of lipid metabolism whose uptake increases after increased intracellular metabolism requiring synthesis of phospholipids.
The aim of this study was to investigate whether, in patients with pHPT and negative or inconclusive 99mTc-MIBI SPECT results, the diagnostic performance of 18F-FCH PET/CT is similar to that of 11C-MET PET/CT from a preoperative perspective. The secondary objective was to compare the performance of the 2 methods in the detection of individual hyperfunctioning parathyroid lesions.
MATERIALS AND METHODS
Patients
Between November 2015 and December 2018, we prospectively included 58 patients with biologically proven pHPT (hypercalcemia and elevated or inappropriately normal PTH levels) and negative or inconclusive results on 99mTc-MIBI imaging performed at various institutions, including ours, and involving SPECT with or without combined CT.
On inclusion, and when there was no recent blood test (<3 mo) confirming hyperparathyroidism, a blood sample was taken to measure serum values of calcium, phosphorus, PTH, albumin, and vitamin D. The serum calcium level was measured the day after surgery to check for normalization.
Institutional ethics committee approval was obtained before the start of this prospective study, and all subjects signed an informed-consent form (P2015/307).
PET/CT Procedure
All PET/CT was performed on a Gemini GXL (n = 15) or a TF64 (n = 38) PET/CT camera (Philips), with essentially identical protocols on both systems. All patients sequentially underwent 11C-MET and 18F-FCH PET/CT (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org).
11C-MET PET/CT
All patients were injected with an average bolus of 555 MBq of 11C-MET while in a fasting state. Fifteen minutes after injection, unenhanced CT (40 mAs; 120 kV; slice thickness, 2.0 mm; interval, 1.5 mm) was performed, followed by a PET acquisition of the neck and upper mediastinum (3 bed positions, 7 min per bed position). Images were reconstructed with 2 different algorithms depending on the PET camera (blob-basis function ordered-subsets time of flight or line-of-response–based row-action maximum likelihood).
18F-FCH PET/CT
Approximately 3 h after 11C-MET injection, unenhanced CT (40 mAs; 120 kV; slice thickness, 2.0 mm; interval, 1.5 mm) was acquired. Then, with the patient lying in the PET/CT tomograph, a 4-MBq dose of 18F-FCH per kilogram of body mass was administered intravenously. 18F-FCH was prepared in 2 steps using a fully automated radiochemistry synthesizer (Trasis All-in-One) (13). A 15-min dynamic PET acquisition covering the neck was started at the time of tracer injection, followed by a static acquisition (early 18F-FCH [18F-FCHE]) on the neck and the upper mediastinum (3 bed positions, 7 min per bed position). PET/CT imaging of the neck and upper mediastinum was repeated 60 min after injection (late 18F-FCH [18F-FCHL]) and used for image analysis in the present work. Images were reconstructed with 2 different algorithms depending on the PET camera (blob-basis function ordered-subsets time of flight or line-of-response–based row-action-maximum likelihood).
Image Interpretation
All PET/CT images were analyzed independently by a nuclear medicine physician (11 y of experience) and a radiologist (18 y of experience), who were aware of previous imaging and laboratory findings for the patients, and by a nuclear medicine physician (27 y of experience) masked to any clinical and imaging information. Discordant image interpretation occurred in 11 patients. In all these cases, a consensus reading led to a final common interpretation. There was no pause between 18F-FCH and 11C-MET readings.
The images (maximum-intensity projection and 3-dimensional volume) were evaluated visually to determine the number and exact location of uptake areas suggestive of hyperfunctioning parathyroid glands. The results were classified into 3 categories based on the aspect of the tracer uptake area and the visualization of corresponding nodules on CT: positive, in cases of a clear circumscribed uptake area on PET images or a faint circumscribed uptake area corresponding to a nodular lesion on CT; inconclusive, in cases of a faint uptake area with no corresponding nodule on CT; or negative, in cases of no discernable tracer uptake area. Lesion localization was assigned to 6 anatomic regions: right and left upper, right and left lower, intrathyroidal, and ectopic. In cases of a discrepancy between readers’ assessments, the appropriate category and anatomic localization were assigned by consensus.
The semiquantitative analysis was performed with Philips IntelliSpace Portal software (version 9). The SUVmax and SUVmean of the PA were measured. We estimated the contrast between the lesion and the thyroid using the ratio of PA SUVmax to thyroid SUVmean (PA/thyroid). By this ratio, we evaluated the capacity to identify the parathyroid activity close to the organ it usually lies behind. The SUVmax and SUVmean of the thyroid were measured by placing a spheric volume of interest 1 cm3 in diameter on the contralateral thyroid lobe unless morphologically pathologic or the right lobe in the absence of a lesion.
Surgery and Histology
Surgeons were aware of 11C-MET and 18F-FCH PET/CT data for all patients. They used this information to direct the surgical procedure, which was an open, minimally invasive parathyroidectomy in cases of a single area of uptake on 11C-MET or 18F-FCH PET/CT. If multiple lesions or an ectopic location were suspected, the surgical approach was adapted. In cases of a coexisting multinodular goiter or suggestive thyroid nodules, an additional hemithyroidectomy or total thyroidectomy was performed. All operated cases had at least 1 lesion categorized as positive on either the 11C-MET or the 18F-FCH PET/CT, except for 1 patient with negative results on PET/CT, for whom full surgical exploration was decided for recurrent pHPT.
The results of 11C-MET and 18F-FCH PET/CT were compared with the surgical exploration and histopathologic findings. Surgical success was established according to normalization of postoperative serum calcium level.
Statistical Analysis
Quantitative variables are expressed as mean ± SD for normally distributed continuous variables and as median with 25th and 75th percentiles for nonnormal continuous variables.
For the sake of comparison, negative, inconclusive, and positive lesions were scored 0, 1, and 2, respectively. Tracer comparison of visual scoring performance was evaluated with a Wilcoxon matched-pairs signed-rank test. For visual decision performance on matched pairs of 11C-MET and 18F-FCH PET/CT images, inconclusive results were considered negative, and the McNemar test with the continuity correction was used.
The sensitivity and positive predictive value of PET/CT imaging were evaluated on a per-lesion and per-patient basis and calculated using histology analysis as the gold standard. Since no histologic data were available in most patients with negative results on PET/CT, specificity and negative predictive values were not evaluated.
The D’Agostino and Pearson test and the Shapiro–Wilk test were used to assess the normality of the sample values. Repeated measures of each relevant quantitative parameter (SUVmax PA and PA/thyroid) were analyzed with the Friedman test. Dunn tests were subsequently applied for multiple comparisons between tracers (11C-MET, 18F-FCHE, and 18F-FCHL). Nonparametric Spearman correlation r was calculated between 18F-FCHE and 18F-FCHL PET/CT with respect to 11C-MET images for PA/thyroid. After exclusion of negative cases, simple linear regression was further calculated to evaluate how this quantitative parameter varies in 18F-FCHE and 18F-FCHL PET/CT with respect to the corresponding parameter on 11C-MET images. Runs tests were performed to assess lack of fit. Goodness of fit was assessed with R2. Statistical analyses were performed using Prism, version 9.0 (GraphPad Software), and its online McNemar test calculator. For all tests, a P value of less than 0.05 was considered statistically significant.
RESULTS
Among 58 patients who prospectively underwent 11C-MET and 18F-FCH PET/CT, 53 patients were included in the analysis (Fig. 1). Five patients were excluded because of unconfirmed pHPT (n = 4) or technical problems (n = 1). The characteristics of the 53 patients are summarized in Table 1. Among them, 7 had a previous history of parathyroidectomy and persistent or recurrent pHPT. Four patients with familial pHPT were included, 3 of whom had previous surgery. Participants underwent 11C-MET and 18F-FCH PET/CT on the same day, except for 7 patients who underwent their 2 PET/CT scan within 5 mo. Twenty-six patients (16 women and 10 men) had parathyroidectomy, with histopathologic confirmation of the presence of adenoma or hyperplasia in 24 patients. Fourteen patients had negative (9/53) or inconclusive (5/53) PET/CT results. Goiter was present in 10 patients (19%), and 29 patients had nodular thyroid disease (55%).
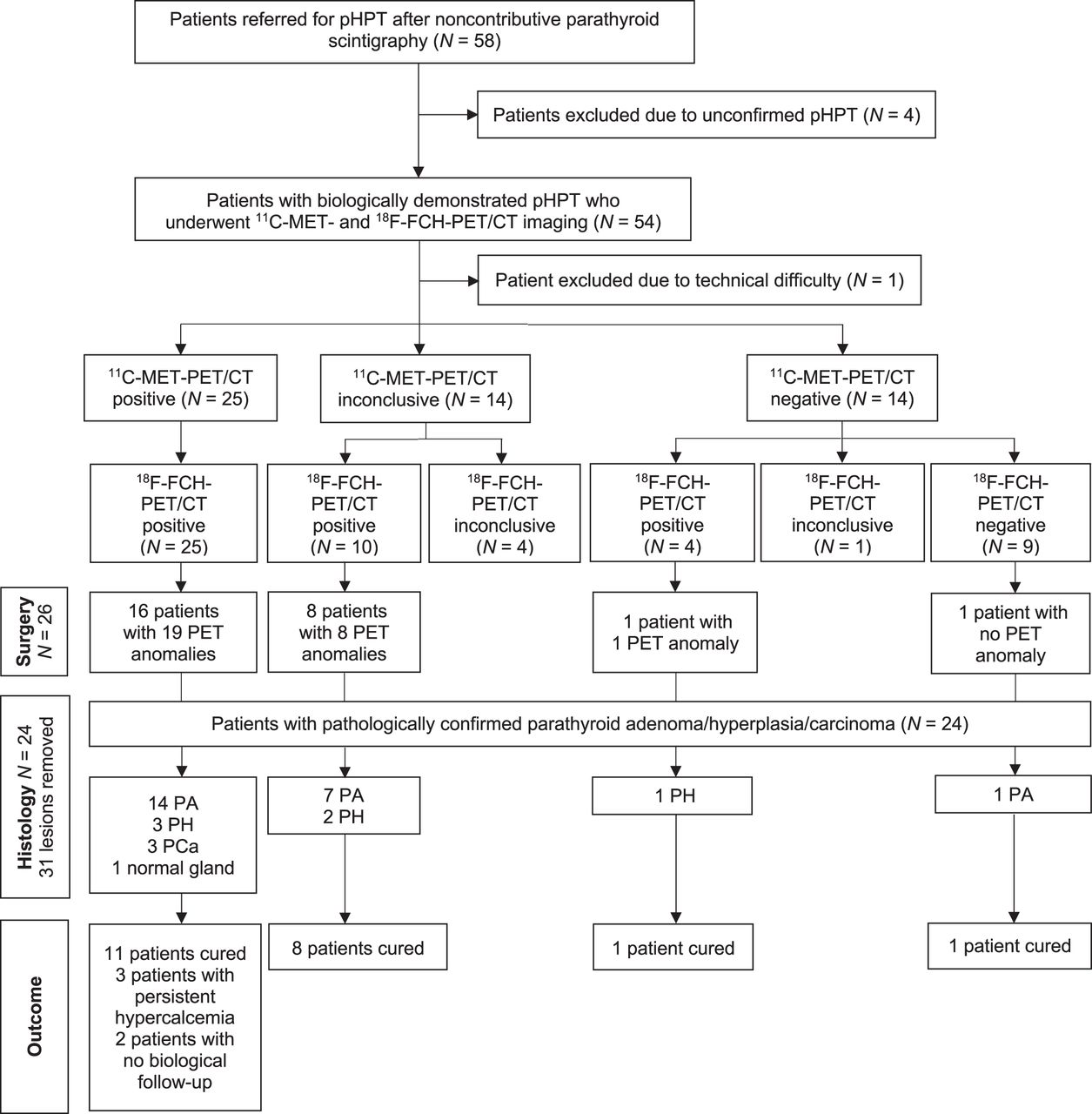
Flowchart. PCa = parathyroid carcinoma; PH = parathyroid hyperplasia.
Patient Characteristics (n = 53)
18F-FCH PET/CT Outperforms 11C-MET PET/CT for Lesion Localization at Both Early and Late Time Points in the Prospect of Surgery Guidance
18F-FCH PET/CT was positive in 39 patients (74%) and inconclusive in 5 patients (9%), compared with 25 patients (47%) and 12 patients (23%), respectively, for 11C-MET PET/CT (Table 2). The visual scoring performance of 18F-FCH PET/CT was greatly superior to that of 11C-MET PET/CT on a per-patient basis (Wilcoxon P < 0.0001). Also, the McNemar test of matched-pairs discordant results also demonstrated the superiority of 18F-FCH over 11C-MET PET/CT in visual decision performance on a per-patient basis (P = 0.0005; χ2 = 12.071 with 1° of freedom), with 14 patients positive only with 18F-FCH PET/CT and no patient positive only with 11C-MET PET/CT, whereas 25 patients were positive and 14 were negative with both tracers. Of 26 patients with negative or inconclusive 99mTc-MIBI results and positive PET/CT results (either 11C-MET or 18F-FCH) who had surgery, 17 were switched from a cervical exploration to a minimally invasive parathyroidectomy approach.
Contingency Tables
In 24 of 26 (92%) patients who had surgery, hyperfunctioning parathyroid tissue (adenoma/hyperplasia/cancer) was correctly localized with 18F-FCH (26 lesions), compared with 15 patients with 11C-MET (16 lesions). On a per-patient basis, the positive predictive value was 96% for 18F-FCH and 94% for 11C-MET. One patient was negative on both PET/CT scans and underwent a surgical exploration allowing the resection of a PA followed by calcemia normalization. No hyperfunctioning parathyroid tissue was found in a patient with persistent pHPT after surgery. The per-patient sensitivity of 18F-FCH PET/CT was 96%, compared with 60% for 11C-MET PET/CT (P < 0.0001). In addition, 5 patients had multiglandular disease detected on 18F-FCH PET/CT (19%). Postoperative calcemia used to define therapeutic success was obtained at 11.5 ± 6.9 mo after surgery. Twenty-one (81%) patients who underwent parathyroidectomy were considered cured, 3 (12%) patients had recurrent or persistent hypercalcemia, and 2 patients were lost to follow-up.
The comparison of lesion visual scoring performance between the 2 tracers is reported in Supplemental Table 1. 18F-FCH PET/CT detected a single uptake area in 37 of 53 patients and multiple uptake areas in 7 of 53 patients. On per-lesion basis (Table 2), 18F-FCH PET/CT showed 47 positive and 9 inconclusive uptake areas. 18F-FCH PET/CT allowed detection of 11 additional uptake areas (6 positive and 5 inconclusive) compared with 11C-MET PET/CT. Thirteen inconclusive uptake areas on 11C-MET were positive on 18F-FCH. Three ectopic parathyroid glands in the superior mediastinum and 2 intrathyroidal localizations were identified with both PET tracers. Comparison of tracers for visual scoring performance on a per-lesion basis revealed the superiority of 18F-FCH over 11C-MET PET/CT (Wilcoxon P < 0.0001). Again, the McNemar test revealed, as well, the superiority of 18F-FCH over 11C-MET PET/CT for visual decision performance on a per-lesion basis (P < 0.0001; χ2 = 17.053 with 1° of freedom), with 19 lesions positive only with 18F-FCH PET/CT and no lesion positive only with 11C-MET PET/CT, whereas 28 lesions were positive and 18 were negative with both tracers. Except for 2 lesions with rapid washout visualized only on 18F-FCHE, and 1 uncertain lesion found only on 18F-FCHL, all lesions were visualized on early and late acquisitions, without a significant difference in visual scoring assessment of contrast. Two cases are illustrated in Supplemental Figure 2.
In total, 31 glands were surgically removed, and histology revealed 22 PAs, 6 hyperplastic glands, and 3 parathyroid carcinomas (Supplemental Table 2). The locations of removed glands are listed in Supplemental Table 1.
All localizations described on PET/CT were concordant with surgery, except for 1 patient with a multiple endocrine neoplasia in which the uptake area was found in the lower left retropolar region on PET/CT whereas the PA was identified in the lower right retropolar region; 2 normal glands were also surgically removed on the left in this patient. In another patient with multiple foci observed on 18F-FCH and 11C-MET, pathologic tissue had probably been left in place because he was not cured after removal of 1 correctly localized lesion (parathyroid hyperplasia) and 2 thyroid nodules. One uptake area found on both PET/CT scans was not explored during surgery, and in 4 cases, parathyroid hyperplasia was found in false-negative 18F-FCH PET/CT locations. On a per-lesion basis (Supplemental Table 2), sensitivity and positive predictive value were 84% and 90%, respectively, for 18F-FCH PET/CT and 52% and 94%, respectively, for 11C-MET PET/CT (P < 0.0001).
Contrast-to-Thyroid and PA Uptake Are Significantly Higher with 18F-FCH PET/CT Than with 11C-MET PET/CT
The visual comparison of the contrast-to-background in the detected anomalies for 18F-FCH and 11C-MET revealed a superiority of 18F-FCH over 11C-MET, both at early and at late imaging times (Supplemental Fig. 3). Higher uptake was observed in 71%–82% (39–45/55) of anomalies for 18F-FCH than for 11C-MET, and a similar uptake of the 2 tracers was observed in 25% (14/55) and 16% (9/55) of cases for 18F-FCHE and 18F-FCHL, respectively. When we consider only the cases that underwent parathyroidectomy, we found similar proportions. Only 1 case operated on had a lesion better visualized on 11C-MET than on 18F-FCH PET/CT.
Supplemental Figure 4 shows the distribution of SUVmax PA and PA/thyroid for each tracer. SUVmax PA on 18F-FCHE and 18F-FCHL, given as median, was 3.26 (25th–75th percentiles, 2.45–4.74) and 3.52 (25th–75th percentiles, 2.58–4.91), respectively, whereas the median SUVmax PA on 11C-MET was 1.51 (25th–75th percentiles, 0.96–2.73). So, the SUVmax PA on 18F-FCHE and 18F-FCHL was approximatively twice higher than 11C-MET SUVmax (P < 0.0001). There was no statistically significant difference between SUVmax PA and PA/thyroid on 18F-FCHE and 18F-FCHL (P = 0.3569). PA/thyroid on 18F-FCHE and 18F-FCHL was 1.39 (25th–75th percentiles, 1.29–1.54) and 1.39 (25th–75th percentiles, 1.29–1.68), respectively (P = 0.1005). The quantitative analysis resulted in nonsignificant differences for both SUVmax and PA/thyroid between adenoma and hyperplasia on both 18F-FCH and 11C-MET PET/CT.
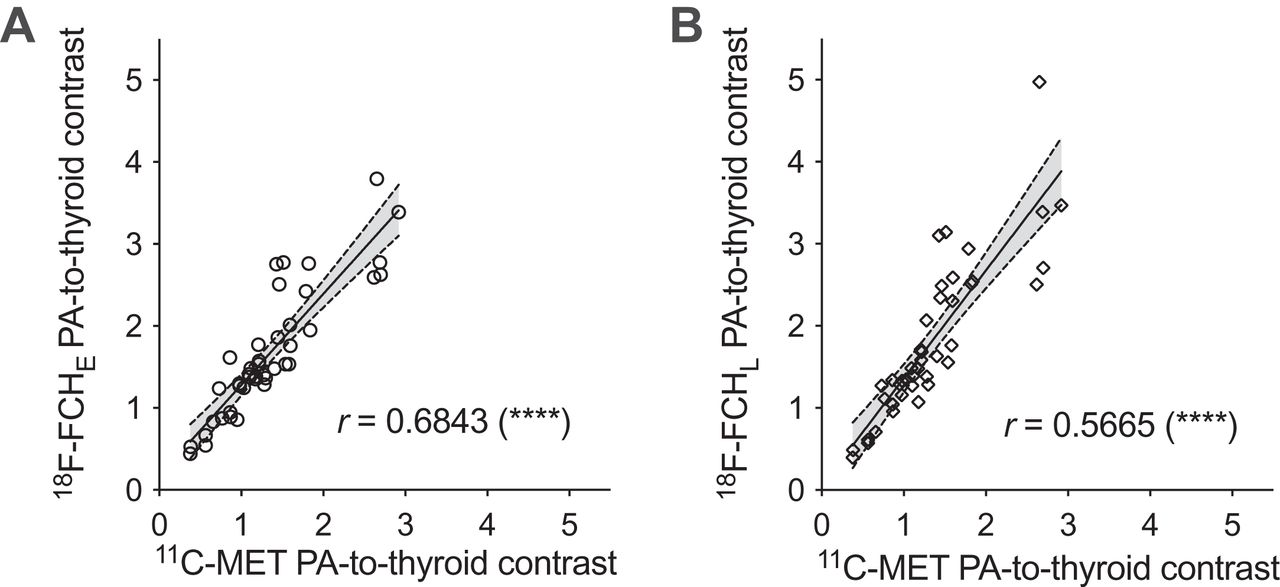
We observed a positive correlation between PA/thyroid on 11C-MET and 18F-FCH PET/CT, despite the difference in the incorporation mechanisms (Fig. 2). Linear fit revealed that PA/thyroid was 11% higher in 18F-FCHE and 31% higher in 18F-FCHL than in 11C-MET: for 18F-FCHE, r = 0.6843, with a slope of 1.11 and an intercept of 0.0175, and r2 = 0.79; for 18F-FCHL, r = 0.5665, with a slope of 1.315 and an intercept of 0.046, and r2 = 0.75.

Correlation between 18F-FCH (early [A] and late [B]) and 11C-MET uptake. ****P < 0.0001.
DISCUSSION
To the best of our knowledge, this was the first study comparing 11C-MET and 18F-FCH tracers for the preoperative detection and localization of hyperfunctioning parathyroid tissue. Our results demonstrate the diagnostic superiority of 18F-FCH over 11C-MET PET/CT for PA and hyperplasia detection in patients with negative or inconclusive results on 99mTc-MIBI exploration.
Precise preoperative localization of a hyperfunctioning parathyroid gland is a prerequisite for efficient minimally invasive surgery. For this purpose, PET/CT recently emerged as a complementary second-line imaging technique with the advantage of a higher resolution associated with PET than with SPECT, as well as a shorter acquisition time (14).
Several publications concluded that the diagnostic performance of 18F-FCH and 11C-MET PET/CT for the localization of parathyroid lesions is better than that of conventional imaging methods (3,7,8,11,15–17). The present study confirmed the added value of this new tracer in the detection and precise localization of hyperfunctioning parathyroid tissue in the subgroup of patients with pHPT and negative or inconclusive results for 99mTc-MIBI with SPECT. The sensitivity of 18F-FCH PET/CT was 96% on a per-patient basis and 84% on a per-lesion basis. As in the APACH1 study (8), we considered the histopathologic results as the gold standard for per-lesion analyses (8). Our findings are comparable to those reported in previous studies. A recent metaanalysis (18) concluded on pooled sensitivity of 93.7% and 91.3% on patient-based and lesion-based analyses, respectively. The detection rates of lesions were 77%–94% (on a patient basis) and 80%–96% (on a lesion basis) (15).
Our cohort included patients for whom the choice of surgical management was challenging (familial hyperparathyroidism, relapsing or persistent HPT, multiglandular forms) compared with most previous studies. Five of the 6 patients with persistent or relapsed postsurgical pHPT had areas of abnormal uptake revealed by 18F-FCH, and we detected 19% of histologically confirmed multiglandular diseases. Still, most of our patients presented with a confirmed solitary lesion (81%), which was consistent with the rate reported in the literature (74% in Beheshti et al. (5)). There was no SUVmax cutoff in 18F-FCH that could be set to distinguish PA from parathyroid hyperplasia.
The optimal time point for 18F-FCH image acquisition remains controversial (3,17,19,20). This controversy results from a 3-phase temporal pattern of 18F-FCH PA uptake, with an early washout followed by an intermediate phase of stability and a late phase of increase (21). We therefore opted for a dual-time-point mode of acquisition in this study. On the basis of the visual evaluation of the images and the analysis of PA/thyroid, that is, a target-to-background ratio, we did not better discern lesions on the late images than on the early ones. Rep et al. (17) described in late-acquisition images a greater accumulation of 18F-FCH in PA than in the thyroid, with a slightly slower decrease in signal, translating into a better lesion contrast. In agreement with our results, Broos et al. (19) reported a decrease in absolute uptake in PA over time, with an increase in contrast relative to the thyroid because of a weaker retention in the thyroid. Conversely, Michaud et al. (16) concluded that late images did not yield additional findings over early ones. Noticeably, in all previous studies, early images were acquired at 5 min after injection, whereas we decided for a slightly later acquisition. We found 2 patients with lesions showing a rapid 18F-FCH washout in our population. Nevertheless, since most parathyroid lesions were observed on both acquisitions, we recommend performing the acquisition at 15 min, reserving additional late imaging for patients whose early acquisition has negative or inconclusive results, as also suggested by Uslu-Besli (22).
Before 18F-FCH, 11C-MET has been widely used as a reliable second-line agent in pHPT. Overall, in our study, 18F-FCH showed a significantly higher sensitivity, with more cases diagnosed and higher accuracy than for 11C-MET. The advantage of 18F-FCH imaging over 11C-MET imaging seems to be strongly related to the fact that it produces more conclusive data. Indeed, 13 anomalies judged inconclusive on 11C-MET PET/CT were considered positive on 18F-FCH PET/CT. The superior imaging qualities of 18F-labeled radiotracers over 11C-labeled ones probably contribute to this better performance of 18F-FCH. Apart from an effect of the positron energy, differences in the molecular properties and uptake mechanisms involved probably explain the differences in diagnostic performance between 18F-FCH and 11C-MET. Indeed, the 2 tracers explore very different biochemical pathways. 11C-MET uptake most probably depends on expression and activity of amino acid transporters such as l-type amino acid transporter 1 and secondarily on its incorporation in the protein prepro-PTH. So, 11C-MET uptake may be closely dependent on the level of synthesis and release of PTH. In contrast, 18F-FCH uptake enters chief cells—those responsible for PTH production—and oxyphilic cells of parathyroid tissue through a specific membrane transporter. After reaching the cytoplasm, 18F-FCH accumulates in the mitochondria in relation to its positive charge, as is the case for 99mTc-MIBI. In the chief cells, 18F-FCH is also phosphorylated by a choline-kinase, which is overexpressed in patients with pHPT, leading to a phosphorylated form—that is, phosphatidylcholine—incorporated into the cytoplasmic membrane. The fact that 2 different mechanisms favor 18F-FCH incorporation into the PTH-producing cells may represent an advantage over the other tracers such as 11C-MET and 99mTc-MIBI (23).
For the evaluation of patients with pHPT and negative or inconclusive 99mTc-MIBI SPECT results, a pooled sensitivity of 86% had been reported in a per patient-based analysis of 11C-MET PET/CT (24). Two other metaanalyses reported sensitivity ranging from 69% to 81% and a detection rate per patient of 70% (6,9). In our population, we reached a slightly lower sensitivity (60%), probably related to a high prevalence of clinical statuses that negatively influence the outcome of presurgical localization imaging, that is, postsurgical recurrence and familiar forms of pHPT (12,15). The visual analysis more frequently resulted in inconclusive uptake on 11C-MET than on 18F-FCH PET/CT. Noticeably, as in other analyses (11), we assimilated inconclusive results to negative ones because we considered that such results would preclude valuable image-guided planning of a minimally invasive parathyroidectomy. Such a position is not adopted by all authors (8).
Our study had some limitations. First, it did not directly compare 18F-FCH PET/CT with 99mTc-MIBI SPECT/CT. Such analyses have already been made, showing the far superiority of 18F-FCH imaging (3,8,11,15–17). This comparison was not among the objectives of our study since we selected only patients with pHPT and negative or inconclusive 99mTc-MIBI exploration. Consequently, our results cannot be extrapolated to patients with tertiary hyperparathyroidism and cannot determine to what extent 18F-FCH should replace 99mTc-MIBI as first-line molecular imaging in pHPT. Also, not all patients underwent surgery after presurgical PET/CT. So, our findings on the diagnostic impact of 18F-FCH PET/CT relate only to the 26 of 53 patients for whom histopathologic data were available.
Finally, although 18F-FCH PET/CT shows good performance for hyperfunctioning parathyroid tissue localization, potential drawbacks must be considered before adopting this modality as the single presurgical imaging procedure in pHPT. As in previous studies (12), we observed false-positive and false-negative findings. The 3 false-positive results related to 1 case of localization discordance between PET/CT and surgery, 1 case of uptake in a normal parathyroid gland, and 1 case of uptake in a thyroid nodule. Even if all 3 cases are classified as false-positive because of the lack of histologic evidence of PA or parathyroid hyperplasia, 2 patients were not cured after surgery, leaving open the possibility that resection did not involve the lesions pointed out by 18F-FCH PET/CT. Five false-negative results concerned 4 cases of parathyroid hyperplasia and 1 patient with recurrent pHPT who ultimately had a PA resection during an extensive bilateral neck exploration. As in previous studies (11,14,16), discordant PET/CT interpretation between readers occurred in 2 situations in which nodular uptake was found within the thyroid gland. The differential diagnosis between a hypermetabolic thyroid nodule and an intrathyroidal PA appeared difficult because of the lack of comparison with a specific thyroid tracer (14). Still, as illustrated in Figure 3 and Supplemental Figure 2, mild to moderate physiologic 18F-FCH uptake by the thyroid did not affect image interpretation in most of our cases, contrary to what has been reported (5). Another source of potential misinterpretation (Supplemental Table 3) is the presence of reactive lymph nodes in classic locations for PAs. Globally, despite the high prevalence of nodular thyroid in our patients and the frequent occurrence of hypermetabolic lymph nodes, both 18F-FCH and 11C-MET PET/CT correctly localized the parathyroid lesions in most surgically treated patients.
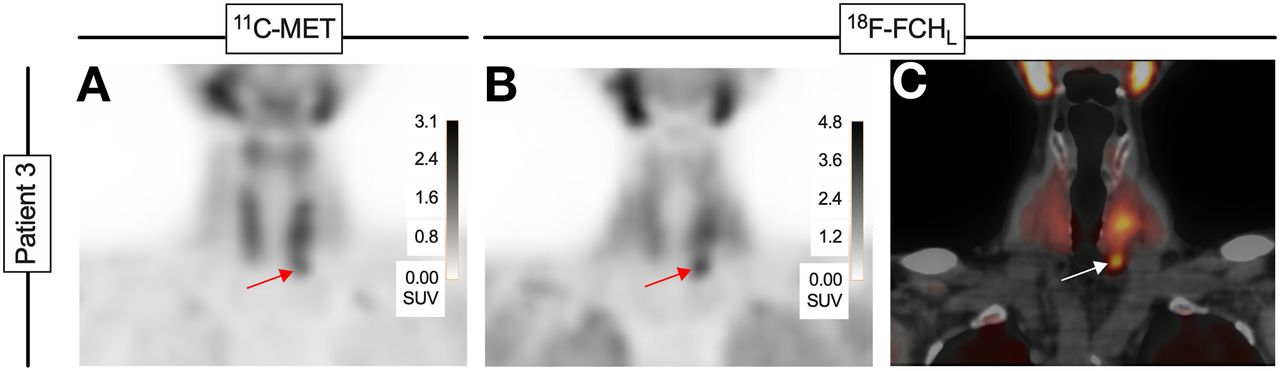
Patient 3. Coronal PET/CT images of 67-y-old woman with pHPT and inconclusive 99mTc-MIBI SPECT/CT (doubtful right inferior focus). (A) 11C-MET images show asymmetric thyroid lobes with lower extension on left (arrow). (B) 18F-FCHL images shows nodular uptake under base of left thyroid lobe (arrow). (C) PET/CT images detail nodular aspect of 18F-FCH uptake (arrow) in PA confirmed at histopathologic analysis.
To determine which PET tracer should be privileged for a particular indication, various factors must be considered, including availability, diagnostic performance, and duration of examination (25). 18F-FCH outperforms 11C-MET for these 3 criteria.
CONCLUSION
Our study demonstrated that in the presence of biochemical evidence of pHPT with negative or inconclusive 99mTc-MIBI results, 18F-FCH PET/CT performs better than 11C-MET PET/CT for the detection of pathologic parathyroid tissue, allowing localization of PA or hyperplasia in 96% of patients. Since 18F-FCH has been proved to be superior to 99mTc-MIBI in previous studies, our results position 18F-FCH PET/CT as the modality of choice for lesion localization in pHPT.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is 18F-FCH superior to 11C-MET PET/CT for the localization of hyperfunctioning parathyroid tissue in patients with pHPT and negative or inconclusive 99mTc-MIBI SPECT findings?
PERTINENT FINDINGS: In this prospective clinical study, 18F-FCH correctly localized lesions in 92% of patients, compared with 58% by 11C-MET.
IMPLICATIONS FOR PATIENT CARE: 18F-FCH is more sensitive than 11C-MET for the localization of hyperfunctioning parathyroid tissue in patients with pHPT and negative or inconclusive 99mTc-MIBI SPECT results.
Footnotes
Published online Aug. 19, 2021.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 22, 2021.
- Revision received August 5, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.