


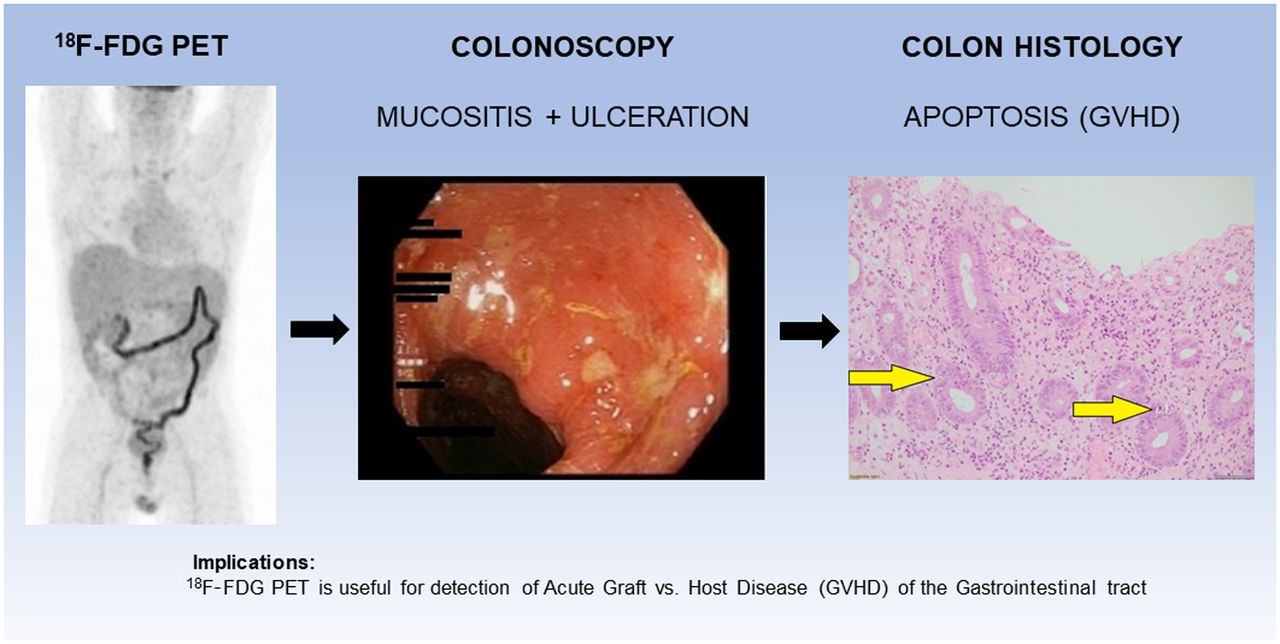
Visual Abstract
Abstract
Acute graft-versus-host disease of the gastrointestinal tract (acute GIT-GVHD) often complicates allogeneic hemopoietic stem cell transplantation (AHSCT). 18F-FDG PET/CT is known to detect active inflammation and may be a useful noninvasive test for acute GIT-GVHD. The objective of this study was to evaluate the diagnostic utility of 18F-FDG PET/CT to noninvasively assess patients with clinically suspected acute GIT-GVHD. Fifty-one AHSCT patients with clinically suspected acute GIT-GVHD prospectively underwent 18F-FDG PET/CT scanning followed by upper and lower GIT endoscopy within 7 d. Endoscopic biopsies of 4 upper GIT and 4 colonic segments were obtained for histology to compare with corresponding quantitative segmental 18F-FDG PET/CT SUVmax. Receiver-operating-characteristic curve (ROC) analysis was performed to determine predictive capacity of 18F-FDG PET/CT SUVmax for acute GIT-GVHD. A separate qualitative visual 18F-FDG PET/CT analysis was also performed for comparison. Results: Twenty-three of 51 (45.1%) patients had biopsy-confirmed acute GIT-GVHD, with 19 of 23 (82.6%) having upper GIT and 22 of 22 (100%) colonic involvement. One of 23 patients did not undergo a colonoscopy. GVHD involved the entire colon contiguously in 21 of 22 patients. For quantitative analysis, histology from 4 upper GIT and 4 colonic segments were compared with 18F-FDG PET/CT SUVmax. Colonic segments positive for GVHD had a higher SUVmax (4.1 [95% CI, 3.6–4.5]) than did normal colonic segments (2.3 [1.9–2.7], P = 0.006). No difference was demonstrated in upper GIT segments. Quantitative 18F-FDG PET/CT yielded a 69% sensitivity, 57% specificity, 73% negative predictive value, and 59% positive predictive value for the detection of GVHD compared with 70%, 76%, 76%, and 68%, respectively, for qualitative analysis. Conclusion: 18F-FDG PET is a useful noninvasive diagnostic test for acute GIT-GVHD, which when present always involves the colon and usually in its entirety, suggesting colonic biopsy obtained by sigmoidoscopy is adequate for histologic confirmation when acute GIT-GVHD is suspected. Of note, 18F-FDG PET cannot distinguish acute GIT-GVHD from non-GVHD inflammatory changes in the colon.
Allogeneic hemopoietic stem cell transplantation (AHSCT) offers cure for various life-threatening hematologic malignancies and disorders. The number of transplants performed each year continues to increase (1). Acute graft-versus-host disease (AGVHD) is a recognized complication occurring in 30%–50% of AHSCT recipients (2). It carries significant morbidity and a 25% mortality rate within 100 d of AHSCT (3). Although AGVHD may affect any organ system, there is a strong predilection for involvement of the skin, gastrointestinal tract (GIT), and liver (4).
Acute GIT-GVHD is commonly suspected on the basis of diarrhea after AHSCT. However, the possible differentials are wide and include GVHD, infectious causes such as Clostridioides difficile and cytomegalovirus colitis, drug effects, and chemoradiation toxicity. The current gold standard for acute GIT-GVHD diagnosis is histology acquired via endoscopic biopsy, characterized by crypt cell apoptosis and crypt loss (5). However, endoscopy is an invasive procedure and not without risk. Anesthetic risk, bleeding, and perforation are all potential complications associated with endoscopy, particularly in post-AHSCT patients who are unwell and often thrombocytopenic (6).
Currently, there is no established role for conventional imaging in the diagnosis of acute GIT-GVHD (7). It has been observed that 18F-FDG PET/CT is a sensitive and specific biomarker of acute large and small bowel inflammation in inflammatory bowel disease (8). Furthermore, 2 pilot studies have reported that PET has a negative predictive value (81%–96%) in the assessment of acute GIT-GVHD (9,10), but data remain sparse in this area.
This prospective study aims to evaluate the diagnostic utility of 18F-FDG PET for acute GIT-GVHD and to determine its role as a noninvasive test for this condition.
MATERIALS AND METHODS
Study Design and Patient Selection
This study was conducted at the Alfred Hospital Melbourne, Australia. Written signed, informed consent was obtained from each participant in accordance with the Declaration of Helsinki and approval from the Alfred Hospital research ethics committee. From December 2009 to November 2014, 51 adult patients with clinically suspected acute GIT-GVHD within 180 d of AHSCT who had not commenced any treatment for GVHD, including steroids, were prospectively enrolled into a noninterventional study comparing 18F-FDG PET/CT, endoscopy, and histology.
Clinically suspected acute GIT-GVHD symptoms included persistent diarrhea, abdominal pain, anorexia, nausea, vomiting, or any combination of these symptoms within 180 d of AHSCT with no other apparent cause.
There were no restrictions to entry into study relating to underlying hematologic disorder, stem cell source, or conditioning regimen.
The stem cell source was peripheral blood (PBSC) in 46 cases (90%) and double umbilical cord blood in the remaining 5 cases (10%). Of the 46 PBSC donors, 2 (4%) were human leukocyte antigen (HLA)–identical sibling donors, a further 13 (28%) were HLA-matched related donors, 29 (63%) were HLA-matched unrelated donors, and 2 (4%) were mismatched unrelated donors. The 5 double umbilical cord blood donations showed variable levels of HLA matching.
Twenty-four patients (47%) received a standard myeloablative conditioning regimen (total-body irradiation based), whereas 13 patients (25%) received a reduced-intensity conditioning and 14 received nonmyeloablative conditioning (27%). Sixteen patients received equine antithymocyte globulin as part of the conditioning regimen. For GVHD prophylaxis, patients who underwent a myeloablative conditioning received cyclosporin, usually with short-course methotrexate. Patients in the reduced-intensity conditioning or nonmyeloablative groups received cyclosporin and mycophenolate mofetil or cyclosporin alone.
Patient and AHSCT characteristics are summarized in Table 1.
Patient Characteristics
18F-FDG PET/CT Evaluation
All participants with clinically suspected acute GIT-GVHD symptoms underwent 18F-FDG PET/CT scanning.
Participants were asked to fast and refrain from vigorous activity for at least 6 h before imaging. Administered 18F-FDG activity was 3 MBq/kg to a maximum of 400 MBq. Molecular imaging was performed on a Gemini PET/CT scanner (Philips) with scan range extending from the skull base to the proximal femora, 60–80 min after intravenous injection of 18F-FDG (3 MBq/kg). Low-dose coregistered CT was used for anatomic localization and attenuation correction.
All images were interpreted independently by nuclear medicine specialists experienced in 18F-FDG PET/CT masked to all investigation results including endoscopy. Results of the 18F-FDG PET/CT scan were not made available to the patient’s treating clinicians and did not influence subsequent clinical management of the patient.
Quantitative 18F-FDG PET/CT Analysis
For quantitative 18F-FDG PET/CT analysis, the GIT was divided into 8 segments: 4 upper GIT segments (esophagus, stomach, duodenum, and terminal ileum) and 4 lower GIT segments (ascending colon, transverse colon, descending colon, and sigmoid/rectum) using the accompanying low-dose CT for anatomic localization.
The highest intensity region within each of the 8 GIT segments was ascertained visually by 2 readers and the SUVmax of this region measured and recorded independently with a standardized 2-dimensional (2D) planar region of interest in the sagittal plane for the esophagus; transaxial plane for the stomach, duodenum, terminal ileum, and sigmoid/rectum; and coronal plane for the ascending, transverse, and descending colon. The size of the 2D planar region of interest used varied according to the GIT segment evaluated to ensure there was no overlap of other organs, and only the SUVmax in the target GIT segment was measured. A 15-mm 2D circular region of interest was placed in the central lumen of the ascending aorta and SUVmean recorded to establish background mediastinal blood-pool 18F-FDG uptake as a reference. The average SUVmax between both expert readers for each GIT segment was used for comparison with histology findings.
To evaluate overall 18F-FDG activity in the entire colon, the parameters Min L4, Max L4, and Sum L4 were used. Min L4 and Max L4 described the lowest and highest SUVmax of the ascending, transverse, descending, and sigmoid/rectal colon segments, respectively. Sum L4 described the combined SUVmax of ascending, transverse, descending, and sigmoid/rectal colon segments.
Qualitative 18F-FDG PET/CT Analysis
For qualitative 18F-FDG PET/CT analysis, the scan was considered positive for acute GIT-GVHD if there was visually increased 18F-FDG uptake greater than 1.5 times background liver uptake involving at least 50% of one or more upper GIT or colonic segments. In the event of disagreement between both expert readers, a third masked expert reader was used to determine the final 18F-FDG PET/CT result.
18F-FDG PET/CT findings were compared with histology, with patients considered positive for acute GIT-GVHD if they had histologic evidence of GVHD in at least 1 upper GIT or colonic segment.
Diagnosis of Acute GIT-GVHD
Gastroscopy and colonoscopy were aimed to be performed within 7 d of the 18F-FDG PET/CT examination, using a segmental unmasking method outlined as follows. Endoscopists were initially masked to the results of the 18F-FDG PET/CT and were asked to macroscopically assess 4 upper GIT segments (esophagus, stomach, duodenum, and terminal ileum) and 4 colonic segments (ascending colon, transverse colon, descending colon, and sigmoid/rectum) for active inflammation.
The results of the 18F-FDG PET/CT were then revealed to the endoscopists during endoscopy. Two biopsies were taken of each segment that appeared normal on both 18F-FDG PET/CT and macroscopically on endoscopy. Four biopsies were taken of each segment that was abnormal on either 18F-FDG PET/CT, macroscopic assessment, or both. Hence, a total of 16–32 upper to lower GIT biopsies were obtained in each participant undergoing both gastroscopy and colonoscopy. All segments able to be endoscopically visualized were biopsied.
Histology
Each segmental GIT biopsy was deemed positive or negative for acute GVHD by a pathologist experienced in GVHD interpretation who was masked to both the 18F-FDG PET/CT and the endoscopy macroscopic findings. Bacterial, viral (including cytomegalovirus), parasitic culture and C. difficile toxin and culture testing was also performed and documented to confirm or exclude other potential causes of non-GVHD inflammation.
Statistical Methods
All data were assessed for normality. Group comparisons of individual location data were performed using Student t tests and reported as mean (±SD) while comparison of repeated measures data was performed using repeated-measures ANOVA with results reported as mean (with 95% CI). To further explore the predictive capacity of colonic locations, summary statistics (minimum, maximum, total) were calculated. For quantitative assessment of the relationship between acute GIT-GVHD and SUVmax, sensitivity, specificity, negative predictive value (NPV) and positive predictive value (PPV) were determined from receiver-operating-characteristic curves (ROC) derived from logistic regression. Qualitative assessment was determined by consensus expert visual interpretation of scans. Statistical analysis was performed using SAS (version 9.4; SAS Institute), and a 2-sided P value of 0.05 was used to indicate statistical significance.
RESULTS
Patients
Fifty-one patients were enrolled and underwent 18F-FDG PET/CT within a median of 47 d (range, 12–166 d) after AHSCT. Median time from onset of clinical symptoms suggestive of acute GIT-GVHD to 18F-FDG PET/CT examination was 6 d (range, 0–69 d). Four patients had diabetes and 4 had a history of steroid induced hyperglycemia; however, none was taking metformin. Twenty-two patients had clinical evidence of cutaneous GVHD, whereas 5 patients had elevated bilirubin suggestive of grade I-II hepatic GVHD (only 1 proven case of hepatic GVHD).
Endoscopic Findings
Participants underwent endoscopy within an average of 3 d (range, 0–13 d) of 18F-FDG PET/CT scanning. Two patients were outside the target 7-d period after 18F-FDG PET/CT scanning; 1 patient at 8 d was delayed due to severe illness and the other required urgent treatment for pericardial effusion receiving endoscopy 13 d after 18F-FDG PET/CT.
Eight of 51 (16%) patients did not have all 8 GIT segments biopsied due to logistical reasons or being too acutely unwell. Of these, 1 patient had a rectal biopsy only, 1 patient did not have gastroscopy, 4 patients did not have colonoscopy, and 2 patients had no biopsy of the terminal ileum. Details of endoscopic pathology data in prespecified GIT segments are presented in the Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org).
Per-Patient Histology Findings and Treatment
Twenty-three of 51 (45.1%) patients had biopsy-confirmed acute-GIT GVHD. Nineteen of 23 (83%) had upper GIT and 22 of 23 (96%) colonic involvement. One of 23 GVHD-positive patients did not have colonic biopsies. Twenty-one of 22 (95%) patients with colonic GVHD had contiguous involvement of the entire colon. Fourteen of 51 (27%) patients had non-GVHD inflammation (6 cytomegalovirus infection, 3 C. difficile infection, 5 nonspecific esophagitis and gastritis). Fourteen of 51 (27%) patients had normal upper GIT and colonic segments.
Twenty-one of 23 (91%) patients with histologically proven acute GIT-GVHD required steroid treatment for clinical symptoms, 13 of 21 intravenous methylprednisolone, and 8 of 21 oral budesonide or prednisolone.
Per-GIT Segment Histology Findings
Of the intended GIT segments, 376 (191 upper GIT/185 colonic) of 408 (92%) were biopsied in 51 patients: 131 of 376 (35%) were positive for GVHD (52 upper GIT/79 colonic), 42 of 376 (11%) were positive for non-GVHD inflammation (25 upper GIT/17 colonic), 199 of 376 (53%) (113 upper GIT/86 colonic) were normal, and 4 of 376 (1.0%) were equivocal for GVHD (1 upper GIT/3 colonic).
Relationship of 18F-FDG PET/CT SUVmax with Histology
No difference in SUVmax was demonstrated in normal upper GIT segments (2.38 [95% CI, 2.24–2.52]) or those with GVHD (2.57 [95% CI, 2.36–2.77]) or non-GVHD inflammation (2.63 [95% CI, 2.34–2.91]) (Fig. 1A).

(A) Upper GIT segments. (B) Colonic segments.
SUVmax was significantly increased in both colonic segments with GVHD (4.06 [95% CI, 3.64–4.47]) and non-GVHD inflammation (5.03 [95% CI, 4.13–5.93]) compared with normal colonic segments (2.29 [95% CI, 1.89–2.69]) (Fig. 1B).
18F-FDG PET/CT and histology images of patient 49 are provided as an example of a positive case of acute GVHD involving both the upper GIT and colon on histology with 18F-FDG uptake only visibly increased in the colon on 18F-FDG PET/CT (Fig. 2).

18F-FDG PET/CT and histology images of patient 49. (A) 18F-FDG uptake only increased in colon and not upper GIT. (B) Lymphocytic infiltration and necrosis (arrow) of stomach crypt epithelium in keeping with acute GIT-GVHD. (C) Extensive colonic crypt destruction with frequent apoptotic bodies (arrows), the histologic hallmark of acute GIT-GVHD.
GIT segment histology and corresponding SUVmax for all 51 patients are provided in Supplemental Table 2.
Quantitative 18F-FDG PET/CT SUVmax Analysis
Upper GIT and colonic segment 18F-FDG PET/CT SUVmax were compared between the 23 patients positive and 28 patients negative for acute GIT-GVHD (Table 2). Patients positive for GVHD had significantly higher SUVmax in all colonic segments other than ascending colon than did patients negative for GVHD. The minimum SUVmax in any of the 4 colonic segments (Min L4) was significantly higher in GVHD-positive patients than GVHD-negative patients. Similarly, the total SUVmax of all 4 colonic segments (Sum L4) was also significantly higher in GVHD-positive patients than GVHD-negative patients. No difference in SUVmax was demonstrated in any of the 4 upper GIT segments between GVHD-positive and -negative patients.
Upper GIT and Colonic Segment SUVmax: Positive- Versus Negative-GVHD Patients
Area under receiver-operating-characteristic curve (AUROC) analysis demonstrated 18F-FDG PET/CT SUVmax of all colonic segments other than ascending colon was independently predictive of acute GIT-GVHD (Table 3). The Min L4 ROC curve was chosen to generate sensitivity, specificity, NPV, and PPV for GVHD as it had the highest AUROC and took into account all colonic segments.
AUROC Analysis: SUVmax as a Predictor for GVHD
As seen from the Min L4 ROC curve in Figure 3, a Min L4 of 1.73 (uptake greater than mean background mediastinal blood-pool activity) resulted in a sensitivity of 69%, specificity of 57%, NPV of 73%, and PPV of 59% for the detection of acute GIT-GVHD.

Min L4 ROC.
Qualitative 18F-FDG PET/CT Analysis
18F-FDG PET/CT scans of all 51 patients were qualitatively visually assessed for acute GIT-GVHD in the upper GIT and colon. Both expert readers were concordant in their appraisal of the presence or absence of GVHD on 18F-FDG PET/CT in 46 of 51 (90%) of cases. Five cases required a third expert reader for final consensus determination of 18F-FDG PET/CT status. Qualitative visual assessment resulted in a 18F-FDG PET/CT sensitivity of 70%, specificity of 76%, NPV of 76%, and PPV of 68% for the detection of acute GIT-GVHD.
Of the 22 acute GIT-GVHD patients with positive results who had colonic biopsies, 16 of 22 (73%) had at least 1 colonic segment, 15 of 22 (68%) at least 2 colonic segments, 13 of 22 (59%) at least 3 colonic segments, and 9 of 22 (41%) all 4 colonic segments considered 18F-FDG PET/CT–positive on qualitative visual assessment.
DISCUSSION
The main aim of our study was to determine the diagnostic utility of 18F-FDG PET/CT as a noninvasive test for acute GIT-GVHD in patients with suggestive clinical symptoms after AHSCT. The few published studies (9,10) in this field have relied predominantly on qualitative assessment of 18F-FDG PET/CT for detection of acute GIT-GVHD by consensus expert visual assessment, which may be difficult to reliably reproduce across institutions.
In addition to qualitative visual 18F-FDG PET/CT assessment, we evaluated 18F-FDG PET/CT quantitatively using SUVmax. SUVmax is a widely accepted and validated parameter used both clinically and for research purposes to quantify and convey the degree/intensity of radiotracer uptake on 18F-FDG PET/CT scans (11). The higher the SUVmax, the higher the degree of radiotracer uptake (inflammatory activity in this clinical scenario) on the 18F-FDG PET/CT scan.
Because SUVmax is objective and generally reproducible across 18F-FDG PET/CT cameras and institutions, it allows objective criteria and definitive thresholds to be defined when determining whether a 18F-FDG PET/CT scan is considered positive or negative for acute GIT-GVHD (12). This could provide a robust standardized technique for 18F-FDG PET/CT evaluation of acute GIT-GHVD that is widely applicable across all institutions with 18F-FDG PET/CT.
One of the strengths of our study is the rigorous nature of data collection, which included obtaining 376 biopsies of a possible 408 upper GIT and colonic segments (92%) in 51 patients for direct correlation with 18F-FDG PET/CT scan findings. This novel method of data collection provided an extremely robust dataset, which is difficult to obtain in this patient population. Twenty-three of 51 (45.1%) patients in our cohort had biopsy-confirmed acute GIT-GVHD, confirming the reasonably high prevalence of this condition when clinically suspected.
The involvement of the colon in all GVHD-positive patients and in its entirety in 96% of positive patients is a significant finding as it suggests that when acute GIT-GVHD is suspected, sigmoidoscopy alone, a less-invasive and resource-consuming procedure, may suffice for histologic confirmation. Eliminating gastroscopy and/or colonoscopy as part of work-up for acute GIT-GVHD (13) would markedly reduce the number of endoscopic procedures and the associated risk of up to 1.8% mortality and morbidity in this vulnerable patient cohort (6).
We demonstrated quantitative 18F-FDG PET/CT assessment using SUVmax is only useful for assessing the presence of GVHD in the colon because no difference in SUVmax was demonstrated between GVHD-positive and normal segments in the upper GIT. Stelljes et al. also reported similar findings and postulated that higher lipopolysaccharide and microbial proinflammatory stimuli in the colon, compared with the upper GIT (9), might account for this. Interestingly, Stelljes et al. found 18F-FDG uptake was invariably increased in the ascending colon in patients positive for acute GIT-GVHD. On the contrary, we found the ascending colon was the only colonic segment not predictive for acute GIT-GVHD on 18F-FDG PET/CT.
We demonstrated GVHD and non-GVHD causes of GIT inflammation in the colon are indistinguishable and have similarly increased SUVmax. As such, further investigations including biopsy are required to determine the cause of inflammation when suggested on 18F-FDG PET/CT.
Our study yielded quantitative and qualitative 18F-FDG PET/CT sensitivity of 69% and 70%, specificity of 57% and 76%, NPV of 73% and 76%, and PPV of 59% and 68%, respectively, for the detection of acute GIT-GVHD. This finding suggests that quantitative analysis using SUVmax is no better than qualitative visual analysis and qualitative analysis alone is sufficient.
Studies by Stelljes et al. (9) and Bodet-Milin et al. (10), which both used only qualitative visual PET assessment, reported more favorable sensitivity of 82% and 81%, specificity of 100% and 90%, and NPV of 81% and 96%, respectively. They both provided limited details on how their images were standardized for review and did not have GIT segment histology datasets as comprehensive as those in our study. Interestingly, Stelljes et al. did provide quantitative SUVmax data as a figure, which showed findings strikingly similar to those in our Figures 1A and 1B.
Noninvasive clinical algorithms based on patient symptoms, conventional imaging, and serum biomarkers are not well established for acute GIT-GVHD, hence the low threshold for clinicians to proceed to more invasive procedures such as endoscopy (14,15).
The NPV of 73% (quantitative) and 76% (qualitative) for 18F-FDG PET/CT detection of acute GIT-GVHD in our study is reasonable and adds to the literature increasingly supporting the use of 18F-FDG PET/CT as a noninvasive diagnostic test for acute GIT-GVHD. Our findings suggest 18F-FDG PET/CT fills a clinical need where endoscopy may not be readily accessible, the patient too unwell, or risks of endoscopy too great.
A major factor that likely limits the sensitivity and specificity of 18F-FDG PET for acute GIT-GVHD is the marked variability in physiologic 18F-FDG uptake that can be seen in the GIT. It is not unusual to see intense physiologic 18F-FDG uptake in the GIT, which may relate to underlying peristaltic smooth muscle activity at the time of imaging.
The use of antispasmodic agents such as N-butylscopoolamine before scanning may decrease physiologic gastrointestinal 18F-FDG uptake and may improve the performance of 18F-FDG PET/CT in this cohort of patients (16). Metformin is also well known to significantly increase physiologic gastrointestinal 18F-FDG uptake and should be withheld for at least 48 h when assessing the GIT on 18F-FDG PET/CT (17). Importantly, no patients in our study were taking metformin before their 18F-FDG PET/CT scan.
Combining PET with other noninvasive markers such as serum inflammatory cytokines IL-17, IFN gamma, tumor necrosis factor, and granulocyte macrophage colony-stimulating factor, which are known to be elevated in acute GIT-GVHD (18,19), may also be an option to further improve noninvasive diagnostic test performance.
Novel PET radiotracers targeting cellular apoptosis (20,21), the histologic hallmark of acute GIT-GVHD, may provide significantly improved sensitivity and specificity for detection of GVHD compared with 18F-FDG PET and should be explored further.
Limitations of our study include no formal grading of severity of acute GIT-GVHD on histology; however, 21 of 23 (91%) patients required steroid therapy (13 intravenous, 8 oral), suggesting most acute GIT-GVHD cases were at least moderately severe.
CONCLUSION
18F-FDG PET is a useful noninvasive diagnostic test for acute GIT-GVHD particularly in the colon. Acute GIT-GVHD, when present, always involves the colon and usually in its entirety, suggesting that only colonic biopsy is required for histologic confirmation when acute GIT-GVHD is suspected. Of note, 18F-FDG PET cannot distinguish acute GIT-GVHD from non-GVHD inflammatory changes in the colon.
DISCLOSURE
The Alfred Foundation and Marian and E.H. Flack Trust provided financial support to conduct the trial. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: How useful is 18F-FDG PET/CT for noninvasive assessment of patients with clinically suspected acute GIT-GVHD after allogeneic hemopoietic stem cell transplantation?
PERTINENT FINDINGS: In a prospective study evaluating 18F-FDG PET/CT in 51 patients with clinically suspected acute GIT-GVHD with upper and lower gastrointestinal histology obtained from endoscopy, 18F-FDG PET/CT was found to be a useful noninvasive test with sensitivity and specificity of 70% and 76%, respectively, for acute GIT-GVHD. The colon appears to always be involved in patients with acute GIT-GVHD and is the location of greatest increase in SUVmax on 18F-FDG PET/CT.
IMPLICATIONS FOR PATIENT CARE: 18F-FDG PET/CT is a useful adjunctive noninvasive diagnostic test when acute GIT-GVHD is clinically suspected.
Footnotes
Published online Apr. 21, 2022.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication January 3, 2022.
- Revision received April 8, 2022.





{kind=link}
{kind=link}
{kind=link}
{kind=link}