


Visual Abstract

Abstract
In recent years, molecular imaging addressing the C-X-C motif chemokine receptor 4 (CXCR4) has increasingly been used in various clinical settings. Here, we aimed to assess radiopharmaceutical uptake and image contrast to determine the most relevant clinical applications for CXCR4-directed imaging. We also investigated the impact of specific activity on scan contrast. Methods: Patients (n = 690) with a variety of neoplasms underwent a total of 777 PET/CT scans with 68Ga-Pentixafor, serving as the CXCR4-specific radioligand. A semiquantitative target lesion analysis was conducted (providing SUVmax and target-to-blood pool ratio [TBR], defined as SUVmax [from target lesion] divided by SUVmean [from blood pool]). The applied specific activity (in MBq/μg) was compared with semiquantitative assessments. Results: Of the 777 scans, 242 did not show discernible uptake in disease sites, leaving 535 PET scans (68.9%) for further analysis. Very high tracer uptake (SUVmax > 12) was found in multiple myeloma (n = 113), followed by adrenocortical carcinoma (n = 30), mantle cell lymphoma (n = 20), adrenocortical adenoma (n = 6), and small cell lung cancer (n = 12). Providing information on image contrast, comparable results for TBR were recorded, with TBR (>8) in multiple myeloma, mantle cell lymphoma, and acute lymphoblastoid leukemia (n = 6). When comparing specific activity with semiquantitative parameters, no significant correlation was found for SUVmax or TBR (P ≥ 0.612). Conclusion: In this large cohort, 68Ga-Pentixafor demonstrated high image contrast in a variety of neoplasms, particularly for hematologic malignancies, small cell lung cancer, and adrenocortical neoplasms. The present analysis may provide a roadmap for detecting patients who may benefit from CXCR4-targeted therapies.
Because of its pivotal role in cancer progression, the C-X-C motif chemokine receptor 4 (CXCR4) orchestrates organ-specific tumor spread through several mechanisms. These include promotion of angiogenesis, growth of malignant cells, or inhibition of antitumor immune response (1). Numerous CXCR4-directed molecular imaging agents have been developed recently to define precisely the utility of CXCR4 as an anticancer target (2–5). Among them, the 68Ga-labeled radiotracer Pentixafor (cyclo(D-Tyr1-D-[NMe]Orn2(AMBS-68Ga-DOTA)-Arg3-Nal4-Gly5) demonstrated high selectivity for CXCR4 along with rapid renal excretion (6,7). Accordingly, 68Ga-Pentixafor has been used in a wide variety of clinical scenarios in oncology. These include in patients with multiple myeloma (MM), marginal zone lymphoma or solid tumor entities, such as small-cell lung cancer (SCLC) and non–small cell lung cancer, neuroendocrine neoplasms, and adrenocortical carcinoma (8–13). Of note, head-to-head comparison with established imaging modalities or other reference radiotracers revealed improved lesion detection rates by 68Ga-Pentixafor PET (8,14,15). This may promote wider adoption of this imaging agent in patients for whom existing modalities are lacking. Furthermore, 177Lu/90Y-Pentixather, a therapeutic counterpart to target CXCR4, has been applied for targeted radionuclide therapies in hematologic malignancies, such as MM or diffuse large B cell lymphoma (16,17). Such theranostic approaches have demonstrated not only a favorable outcome (16,17), but also tolerable adverse effects, although stem cell support is mandatory (18).
The beneficial use of 68Ga-Pentixafor PET/CT, along with its potential to identify patients eligible for treatment with β-particle emitters, favors wider clinical use. However, before widespread adoption or clinical development programs leading to market authorization, comprehensive characterization of its performance should be undertaken, including assessment of radiopharmaceutical uptake and image contrast among a broad spectrum of neoplasms. In our bicentric study, which, to our knowledge, enrolled the largest cohort of patients imaged with 68Ga-Pentixafor PET/CT or PET/MR to date, we aimed to assess radiopharmaceutical accumulation and image contrast in several cancers to determine the most relevant clinical applications. In addition, lower specific activity characterized by higher amounts of cold mass could hamper image interpretation (19), for example, by an increasing occupation of the (sub)cellular target by nonradiolabeled components. Thus, we also investigated the impact of specific activity on quantification.
MATERIALS AND METHODS
Patient Population
Patients from 2 study sites were included (University of Würzburg and Medical University of Vienna). Parts of this cohort have been described before to determine the diagnostic usefulness of 68Ga-Pentixafor PET/CT (7–9,11–14,20–26), without evaluation of image contrast (including impact of specific activity) or comparing uptake among all included diagnoses. Patients signed written informed consent forms before the examination. Given the retrospective character of this study, the local ethics committee waived the need for further approval (no. 20210726 02).
Radiotracer Synthesis
Following good manufacturing practice, 68Ga-Pentixafor was provided using a synthesis module (Scintomics) and disposable single-use cassette kits (ABX, Radeberg, Germany), as described previously (27). Peptide mass (in μg), activity (in MBq), and specific activity (in MBq/μg) of injected 68Ga-Pentixafor were recorded for each patient.
Imaging
68Ga-Pentixafor PET was performed either on a Siemens Biograph mCT (64 and 128, Siemens Medical Solutions) or on a Siemens Biograph mMR (Siemens Healthcare GmbH). Whole-body scans (covering the vertex of the skull to the proximal thighs) were conducted 60 min after injection of 68Ga-Pentixafor. We also performed low-dose CT scanning for attenuation correction and anatomic coregistration (120 keV, 512 × 512 matrix, 5-mm slices, increment: 30 mm/s, pitch index: 0.8, and rotation time: 0.5 s). PET images were reconstructed including corrections for CT-based attenuation, random events, and scatter. For MRI, we applied an integrated radiofrequency coil including a multistation protocol (slice thickness, 2 mm), as previously described (12,28).
Image Interpretation
All scans were obtained for clinical or research purposes. As part of this study, all images were reanalyzed by readers who were masked to respective clinical information. At Würzburg, image interpretation was performed as a single-reader analysis, verified by an expert reader. At Vienna, an expert reader performed the assessment.
Semiquantitative Assessment
A target lesion (TL) assessment was performed by investigating the visually most intense TL on PET. Three-dimensional volumes of interest applying an isocontour threshold of 40% were placed on the TL, providing SUVmax, SUVmean, and SUVpeak. A target–to–blood-pool ratio (TBR) was derived by placing a volume of interest over the aortic arch. TBR was then provided by dividing SUVmax (of the TL) by SUVmean (of the blood pool) (12).
Statistical Analysis
Statistical analysis was performed using GraphPad Prism (version 9.2.0, GraphPad Prism Software). Descriptive results are displayed as mean ± SD. Nonparametric Spearman correlation coefficients were calculated to investigate associations between semiquantitative parameters with specific activity (including an outlier correction using the ROUT-Method). A P value of less than 0.05 was considered statistically significant.
RESULTS
Highest Uptake in Hematologic Malignancies, SCLC, and Adrenocortical Neoplasms
No adverse events were recorded after injection of 68Ga-Pentixafor. Two hundred forty-two of 777 (31.1%) of the scans did not show discernible uptake, leaving 535 of 777 (68.9%) cases for further analysis (Table 1). As such, an overall number of 535 TLs were investigated. Among all TLs, SUVmax was 13.01 ± 10.01 and the corresponding TBR was 8.59 ± 15.98. The highest average SUVmax (>12) was found in MM (n = 113), followed by adrenocortical carcinoma (n = 30), mantle cell lymphoma (MCL; n = 20), adrenocortical adenoma (n = 6), and SCLC (n = 12; Figs. 1 and 2). The lowest average SUVmax (<6) was recorded in osteosarcoma (n = 1), followed by bladder cancer (n = 1), mediastinal tumor (not otherwise specified, n = 1), head and neck cancer (n = 2), and Ewing sarcoma (n = 1; Fig. 3). For SUVpeak, comparable results were achieved (Supplemental Fig. 1). Moreover, high average TBR (>8) was recorded in MM, MCL, and acute lymphoblastoid leukemia (n = 6). Low average TBR (<4) was observed in head and neck cancer, colorectal cancer (n = 1), osteosarcoma, Ewing sarcoma, bladder cancer, renal cell carcinoma (n = 1), and mediastinal tumor (Fig. 4).
Overview of Positive 68Ga-Pentixafor PET Scans and Individual Diagnoses of Patients Included

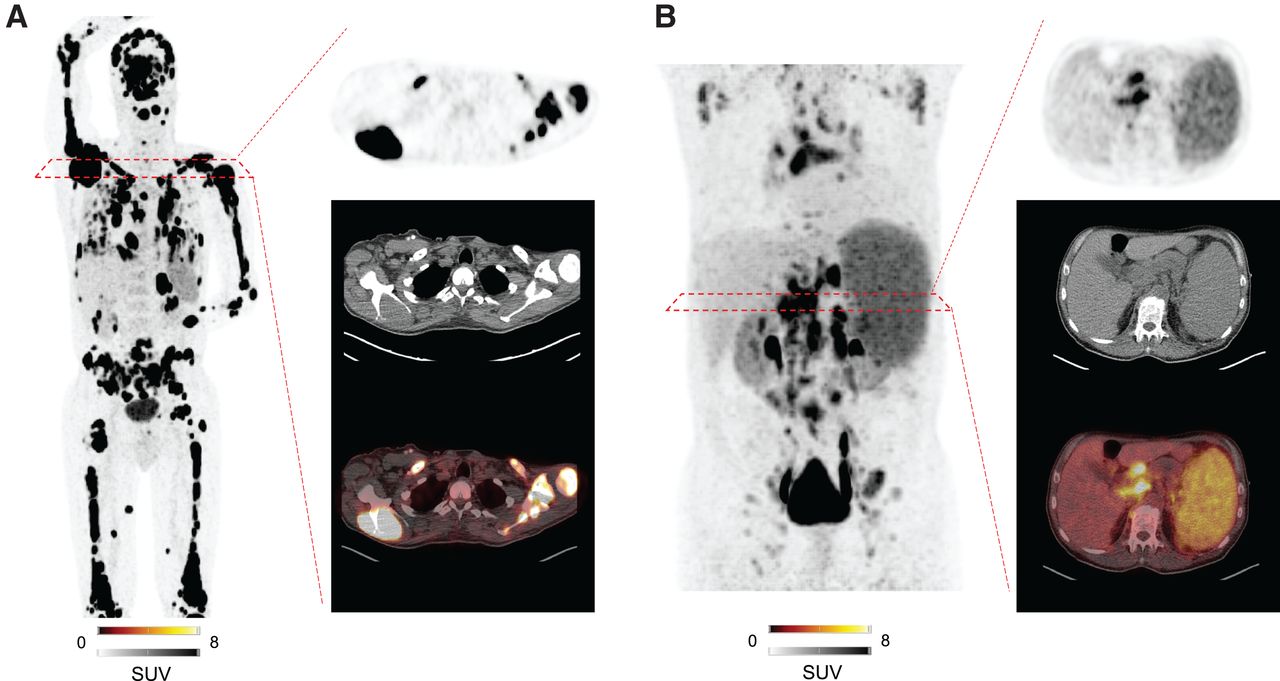
Maximum-intensity projections of patients with hematologic malignancies imaged with CXCR4-directed 68Ga-Pentixafor. Target lesion is also displayed on transaxial PET, CT, and PET/CT. Patient diagnosed with MM (A; SUVmax in target lesion, 74.3) and MCL (B; SUVmax in target lesion, 17.2). Substantially low background activity allowed for precise determination of disease sites.

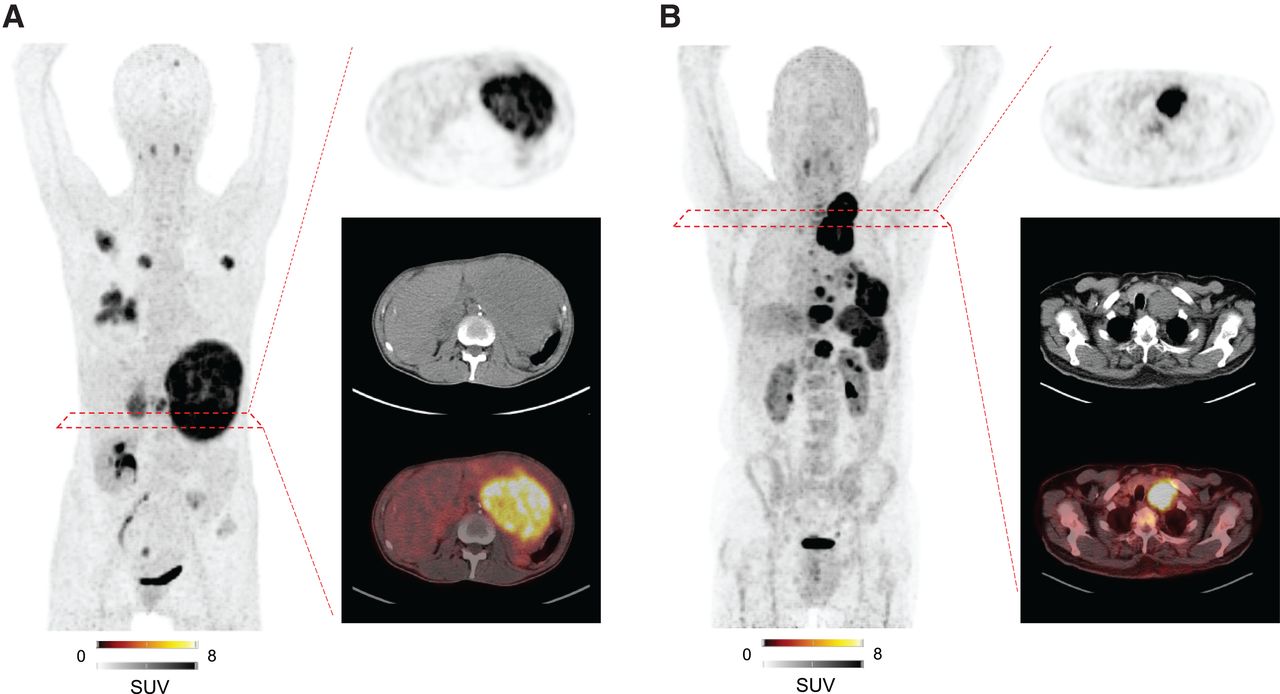
Maximum-intensity projections of patients with solid tumor entities imaged with CXCR4-directed 68Ga-Pentixafor. Target lesion is also displayed on transaxial PET, CT, and PET/CT. Patient diagnosed with adrenocortical carcinoma (A; SUVmax in target lesion, 13.2) and small cell lung carcinoma (B; SUVmax in target lesion, 19.4). Background activity was substantially low, providing a precise read-out of disease sites.

Bar chart displaying average SUVmax. Mean ± SD is indicated. Black dotted lines show SUVmax cutoffs of 6 and 12, respectively. BP = blood pool (red dotted line); AML = acute myeloid leukemia; CCC = cholangiocarcinoma; NSCLC = non–small cell lung carcinoma; NEN = neuroendocrine neoplasm; DSRCT = desmoplastic small round cell tumor; ALL = acute lymphoblastoid leukemia; CLL = chronic lymphocytic leukemia; MZL = marginal zone lymphoma; SCLC = small cell lung carcinoma; MM = multiple myeloma. In individual lesions, a markedly increased SUVmax of up to 85.8 was observed. Number of investigated patients (n) per diagnosis group is given in parentheses.

Bar chart displaying average TBR. Mean ± SD is indicated. Black dotted lines show TBR cutoffs of 4 and 8, respectively. NSCLC = non–small cell lung carcinoma; NEN = neuroendocrine neoplasm; AML = acute myeloid leukemia; CCC = cholangiocarcinoma; CLL = chronic lymphocytic leukemia; MZL = marginal zone lymphoma; DSRCT = desmoplastic small round cell tumor; SCLC = small cell lung carcinoma; ALL = acute lymphoblastoid leukemia; MM = multiple myeloma. Number of investigated patients (n) per diagnosis group is given in parentheses.
No Relevant Impact of Specific Activity on Visual or Semiquantitative Assessment
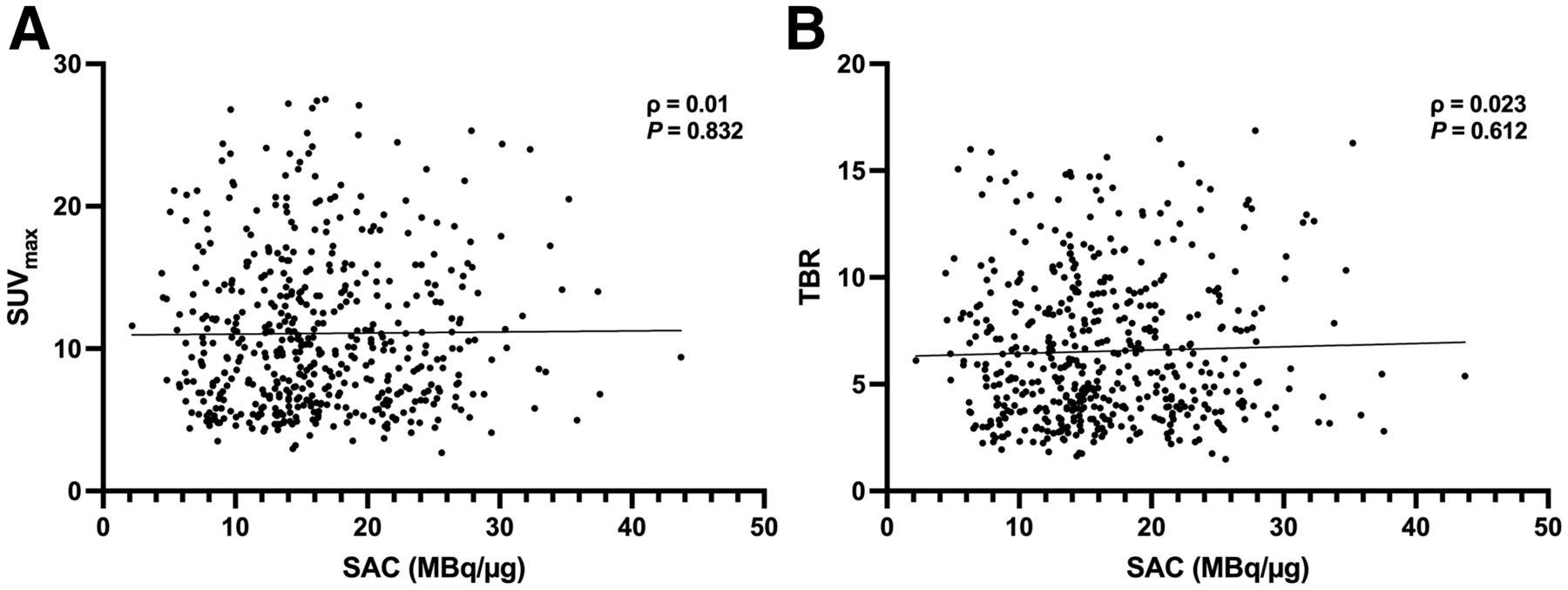
Median injected peptide mass was 8.5 μg (range, 2.56–35.61 μg), injected activity was 143 MBq (range, 38–239 MBq), and specific activity was 15.39 MBq/μg (range, 2.19–43.70 MBq/μg). Comparing specific activity with semiquantitative parameters, only SUVmean (ρ = −0.138, P = 0.002), but none of the other correlative indices, reached significance (SUVmax: ρ = 0.01, P = 0.832; TBR: ρ = 0.023, P = 0.612; SUVpeak: ρ = −0.087, P = 0.053; Fig. 5).
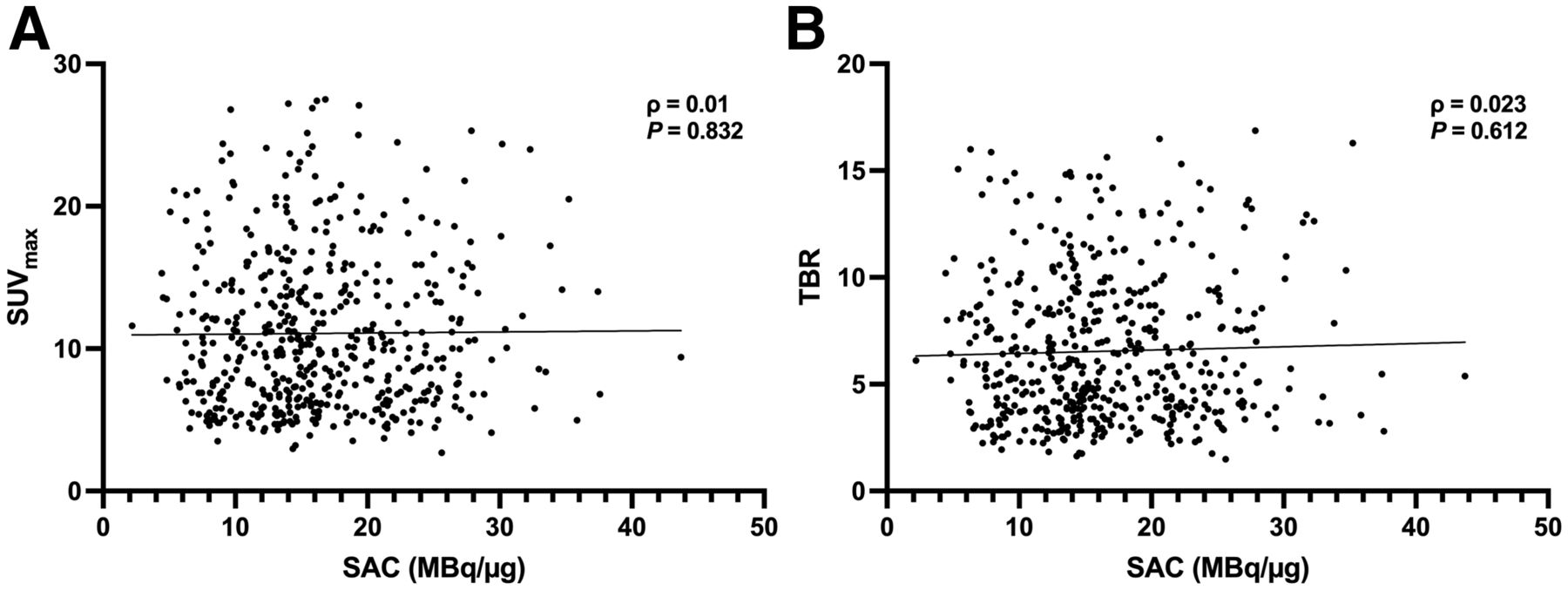
Correlation plots between specific activity in MBq/μg and SUVmax (A) and TBR (B). Significant Spearman ρ and P are displayed. No significance was reached.
DISCUSSION
In the present bicentric study investigating a large cohort imaged with 68Ga-Pentixafor, discernible uptake in putative sites of disease was noted in more than 68% of the scans. Among neoplasms studied, we determined MM had the highest uptake (SUV), with adrenocortical carcinoma and MCL closely after. Comparable results were recorded for image contrast (TBR). Specific activity had no impact on a semiquantitative level, supporting the notion that an excellent read-out can be achieved, even after administration at low specific activities.
A growing body of evidence supports the clinical utility of CXCR4-targeted 68Ga-Pentixafor PET/CT in a variety of disease entities, including hematologic malignancies (7,22) and solid tumors (29). Some of these studies also revealed that 68Ga-Pentixafor provided an increased detection rate at sites of disease when compared with conventional imaging or other PET agents such as 18F-FDG or somatostatin receptor–directed radiopharmaceuticals, thereby indicating that this agent can image malignancies that lack a more suitable modality (15,23,26). Here we aimed to provide a precise cohort of neoplasms that exhibit high tracer avidity and excellent TBR. By investigating 690 patients with 35 different types of cancer, we demonstrated that 68Ga-Pentixafor PET exhibits the most intense uptake in hematologic malignancies, such as MM, MCL, or acute lymphoblastoid leukemia. 68Ga-Pentixafor PET did not perform as well in solid tumors. Nevertheless, a TBR of more than 4 was still achieved in certain cases, for example, adrenal, SCLC, liver, ovarian, neuroendocrine neoplasms, or pancreatic cancer (Fig. 4). We also checked whether low specific activity may have hampered image contrast (19), for example, by an increasing occupancy of the target by carrier. However, we ruled out a relevant impact on a semiquantitative level (Fig. 5). This is also in line with previous affinity studies, demonstrating that 68Ga-Pentixafor completely interacts with the binding pocket of CXCR4 (30). Nonetheless, novel second-generation radiotracers based on iodoCPCR4 analogs with altered linker structure may further increase tumor retention (31).
Increased CXCR4 expression on the tumor cells has been tightly linked to poor outcome in hematologic malignancies and solid tumors (32,33), suggesting it as a viable therapeutic target. For example, the stromal cell–derived factor 1 neutralizing agent Olaptesed pegol (NOX-A12) or the CXCR4 antagonist Plerixafor have each been used in patients with refractory MM. In clinical phase I/II studies, such drugs achieved an overall response rate in almost half of the patients (Plerixafor) or partial response in 68% (NOX-A12) (34,35). Theranostic approaches based on 68Ga-Pentixafor scan results have also been conducted using the therapeutic analogs 177Lu/90Y-Pentixather (16,18). Although there is no study reporting an association between PET-based SUVmax and absorbed doses in lesions on CXCR4-directed imaging and radionuclide therapies to date, the markedly increased SUVmax observed in certain cases suggests that a substantial fraction of patients may also be eligible for CXCR4-directed radioligand therapies. However, CXCR4-targeted endoradiotherapy causes bone marrow ablation and, thus, subsequent stem cell support is needed (18), further emphasizing the importance of well-established algorithms for adequate patient selection.
Future studies should also evaluate the ability of CXCR4-directed molecular imaging to assess the retention capacities of nonradiolabeled CXCR4 neutralizing agents in vivo, preferably before treatment onset. For instance, a phase I study evaluating the CXCR4 inhibitor LY2510924 in patients with advanced solid cancers revealed favorable antitumor activity (36). Of note, a substantial patient fraction treated with this “cold” CXCR4 inhibitor had clinical diagnoses identical to those in the present study, for example, ovarian, lung, or pancreatic cancer (all demonstrating SUVmax > 6). As such, a baseline 68Ga-Pentixafor PET/CT revealing increased CXCR4 expression at disease sites may allow identification of patients who would most likely be suitable for nonradiolabeled CXCR4-directed drugs, including LY2510924 (36). This would then further expand the theranostic concept beyond identifying patients for treatment with β-emitters, but also to selecting individuals for nonradiolabeled CXCR4-targeted therapeutic options.
Our study has several limitations. We included both CT- and MR-based hybrid imaging, which may provide an additional variable that could be controlled better in future studies. Despite investigating the largest cohort to date, prospective trials should also be undertaken. In addition, the numbers of investigated patients per tumor entity substantially varied. Thus, resulting low numbers of cases and inter- and intrapatient heterogeneity of in vivo CXCR4 expression may have biased the results presented herein. Future studies should therefore consider more balanced subgroups enrolling comparable numbers of patients diagnosed with the identical tumor entity.
CONCLUSION
We found high uptake and image contrast for a variety of neoplasms imaged with 68Ga-Pentixafor PET, such as MM and MCL, but also for adrenal neoplasms and SCLC. These results suggest clinical scenarios in which 68Ga-Pentixafor PET may prove beneficial for directing CXCR4-targeted therapies.
DISCLOSURE
Hans-Jürgen Wester is founder and shareholder of Scintomics. Anja Zehndner is an employee of Pentixapharm, Würzburg. No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the tracer avidity of malignant lesions, and what are the most avid tumors for CXCR4-targeted 68Ga-Pentixafor PET?
PERTINENT FINDINGS: We observed high uptake and image contrast of the radiopharmaceutical, in particular for hematologic malignancies as well as adrenal neoplasms and small cell lung cancer. Specific activity had no effect on 68Ga-Pentixafor uptake.
IMPLICATIONS FOR PATIENT CARE: Among a broad spectrum of neoplasms, the present bicentric study suggests entities eligible for CXCR4-directed molecular imaging and therapy.
Footnotes
Published online Mar. 3, 2022.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication December 21, 2021.
- Revision received March 2, 2022.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}