


Abstract
Intraoperative molecular imaging (IMI) has recently emerged as an important tool in the armamentarium of surgical oncologists. IMI allows real-time assessment of oncologic resection quality, margin assessment, and occult disease detection during real-time surgery. Numerous tracers have now been developed for use in IMI-guided tissue sampling. Fluorochromes localize to the tumor by taking advantage of their disorganized capillary milieu, overexpressed receptors, or upregulated enzymes. Although fluorescent tracers can suffer from issues of autofluorescence and lack of depth penetration, these challenges are being addressed through hybrid radioactive/fluorescent tracers and new tracers that fluoresce in the near-infrared (NIR-II [wavelength > 1,000 nm]) range. IMI is already being used to treat numerous cancers, with demonstrated improvement in cancer recurrence and patient outcomes without incurring significant burden on either clinicians or patients. In this comprehensive review, we discuss history, mechanism, current oncologic applications, and future directions of IMI-guided optical biopsy.
Cancer is the second leading cause of death in the United States, with over 1.9 million new cases and 600,000 deaths expected in the United States in 2022 (1). Surgery remains a mainstay in the treatment of solid tumors, with the most important predictor of postsurgical outcome being complete resection of the tumor with negative margins. Unfortunately, precise intraoperative resection still relies mostly on visual inspection under white light and tactile palpation. This makes it difficult to accurately assess margins and detect additional synchronous/metachronous lesions missed on preoperative studies (Supplemental Videos 1–2; supplemental materials are available at http://jnm.snmjournals.org). White light visualization can also make it difficult to identify vital structures that need to be preserved.
Intraoperative molecular imaging (IMI) has developed rapidly over the past decade to address these challenges. IMI uses optical tracers that target malignant lesions through a variety of means. These tracers fluoresce and can easily be visualized using optical imaging instrumentation, making it possible to accurately identify tumors intraoperatively, remove them with negative margins, and even identify additional lesions that were not visualized preoperatively (2). Fluorescent tracers can also help surgeons identify and avoid vital structures such as nerves and vasculature (3).
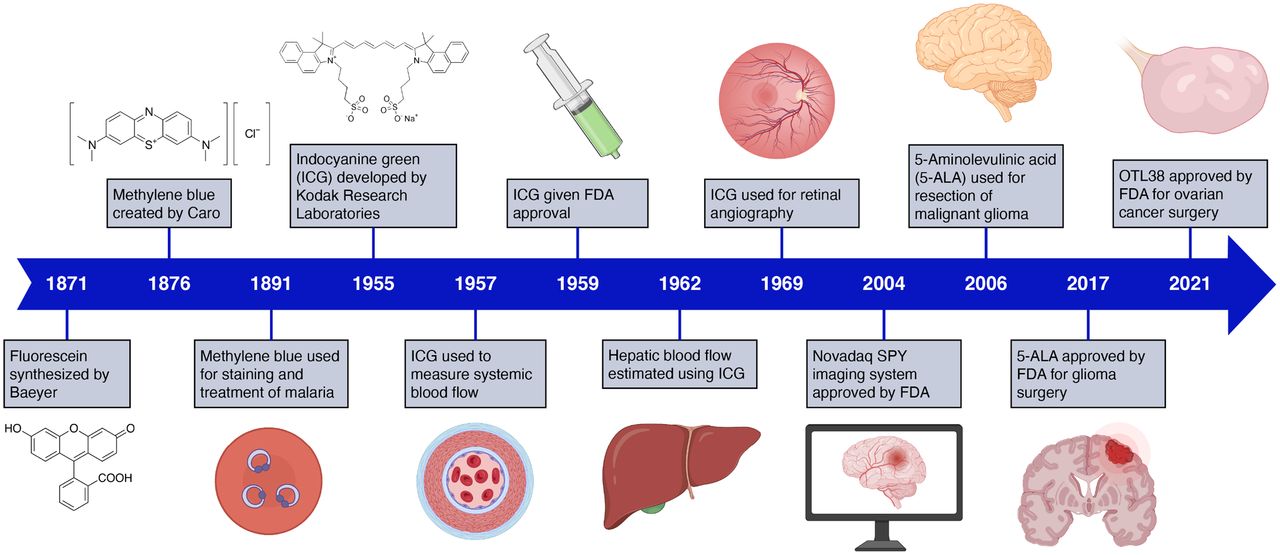
Although biologic imaging traces back to the 1800s with the discovery of the first fluorescent dyes, IMI is a relatively recent method of cancer detection with a history that really begins in the late 1990s (Fig. 1). In 1998, Stummer first described the use of 5-ALA for the detection of malignant gliomas, and it was not until 2017, almost 20 y later, that it became the first Food and Drug Administration (FDA)–approved IMI tracer (4). The first FDA approval for an IMI-compatible imaging system, the Novadaq SPY, also came recently in 2005 (5). Although relatively new, these approvals have spurred hundreds of trials testing a wide array of IMI tracers and imaging systems (6). As of 2022, 4 tumor-targeted probes have reached phase III clinical trials in the United States (pafolacianine, BLZ-100, LUM015, and SGM-101), and around 40 contrast agents are currently being investigated in more than 85 clinical trials within the United States (2,5,6).
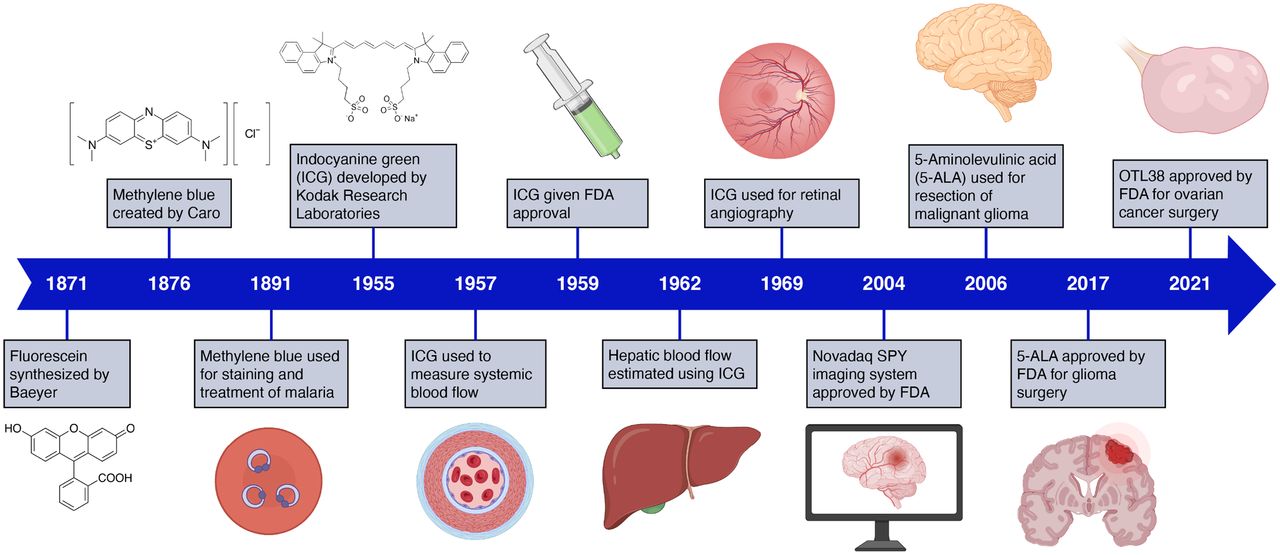
A timeline of notable developments in IMI.
IMI is already uniquely positioned within the perioperative continuum to intraoperatively localize lesions visualized preoperatively by nuclear medicine studies (e.g., PET). However, the marriage between IMI and nuclear medicine is even more intertwined. The forefront of research now involves developing hybrid radioactive and fluorescent tracers, which draw on the unique advantages of fluorescent and radioactive tracers (7). For example, whereas fluorescence excels at real-time direct visualization, it suffers from poor tissue depth penetration and autofluorescence. In contrast, radioisotopes cannot be visualized directly, but can localize tumors deep within tissue. By combining radiotracers and fluorescent molecules, hybrid tracers can provide the best of both worlds (8).
In this review, we will provide an overview of commonly used imaging agents and surgical navigation systems, with context supplied through their use in recently completed and currently active clinical trials. With each technology, we highlight the recent advances and current challenges for clinical implementation, providing perspective on the future development of IMI.
RESULTS
IMI Targeting Mechanisms and Imaging Systems
Most intraoperative optical tracers have been designed to have fluorescence maxima in the near-infrared (NIR) range. In contrast to visible light, NIR fluorescence permits deeper signal penetration, reduced tissue scatter, and decreased background interference from endogenous fluorescent chromophores, such as hemoglobin, NAD(P)H, and flavoproteins (2,9). With increased signal-to-background ratios (SBRs), NIR agents enhance the surgical field of view and enable refinement of resection margins.
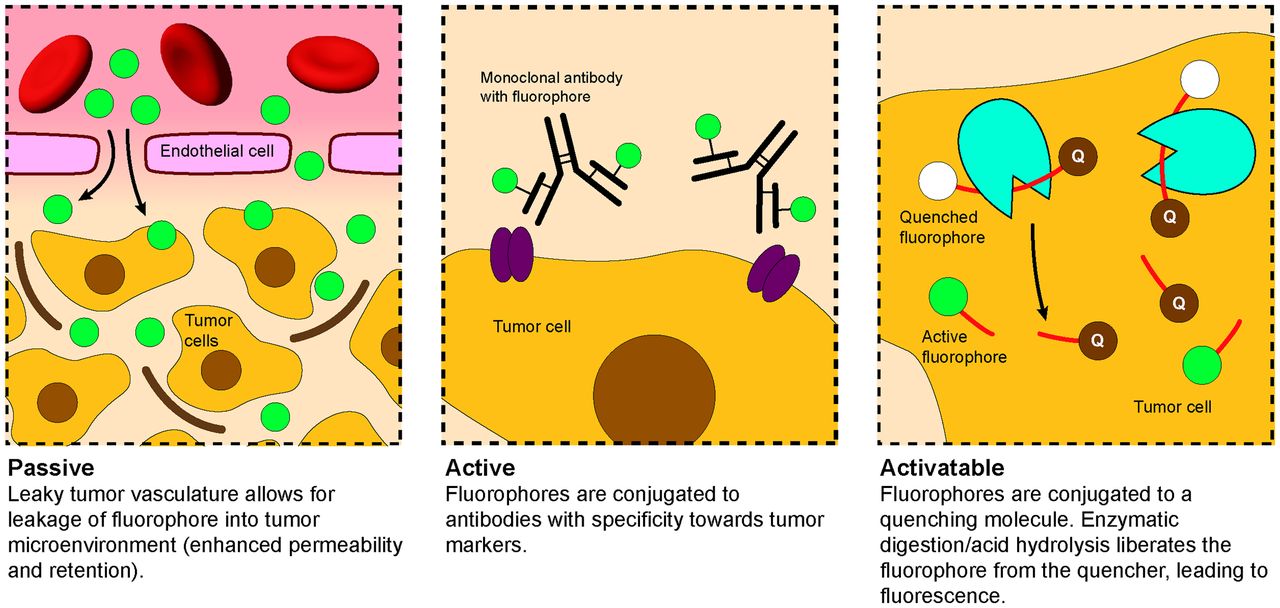
Fluorescent tracers generally act through 1 of 3 mechanisms: passive, active, and activatable (Fig. 2) (5,6). Passive targeting relies on the enhanced permeability and retention effect (EPR), which leverages the increased vascular permeability and decreased lymphatic drainage of cancerous tissue. This causes the tracer to accumulate inside the tumor milieu. Tracers that exploit EPR include methylene blue (excitation: 668 nm; emission: 688 nm), indocyanine green (ICG) (excitation: 780 nm; emission: 805 nm), and fluorescein (excitation: 494 nm; emission: 521 nm) (5).

Fluorophores used in IMI generally use 1 of 3 mechanisms to facilitate specific targeting.
More recently developed tracers actively target abnormally expressed receptors on malignant cells, enhancing labeling specificity and permitting higher resolution imaging. For example, pafolacianine (OTL38) is a folate receptor α (FRɑ)–targeted tracer that has allowed real-time visualization of radiologically occult ovarian and lung tumors (10). SGM-101 is an antibody-dye conjugate against carcinoembryonic antigen (CEA) being assessed for clinical translation in gastrointestinal and pulmonary cancers (11). EMI-137 (GE-137) is a c-MET–targeting cyclic peptide conjugated to a cyanine dye that has been used to improve colorectal polyp detection and facilitate penile cancer resection (2,12).
Activatable probes represent the third mechanistic class, in which the specific microenvironmental and intracellular abnormalities of tumor cells activate the fluorescent probe. LUM015 (excitation: 650 nm; emission: 675 nm) fluoresces only when the quenching moiety is cleaved by cathepsin proteases upregulated in cancer tissue (13). Pegsitacianine (excitation: 780 nm; emission: 805 nm) is a pH-activatable micelle nanoprobe that exploits the metabolic acidosis of solid tumors (14). Table 1 provides an overview of some of the most common IMI agents (2,6).
List of Imaging Agents That Are FDA-Approved or Currently in Clinical Trials in IMI
These 3 mechanisms have all been complemented by the development of hybrid tracers incorporating both a fluorescent molecule and a radioisotope. Hybrid tracers address the problems of tissue penetration, autofluorescence, and photobleaching that occur with fluorescence (7,8). Because γ-radiation can be detected sensitively with little tissue attenuation, the radioisotope enables intraoperative localization even with deeper tumors, whereas the fluorescent tracer allows for direct visual examination and localization. Furthermore, β-emitting radioisotopes allow for preoperative surgical planning (similar to 18F-FDG PET) and provide quantitative information on biodistribution. Many radioisotopes, including 111In, 68Ga, and 89Zr, have been conjugated to fluorescent molecules for use in IMI, with 99mTc emerging as a particularly strong candidate given its favorable decay parameters and low cost (8).
The recent explosion in the development of new experimental molecules for IMI has been paralleled by a similarly exponential growth in the number of imaging systems available in the market. Although the discussion of individual systems is beyond the scope of this review, Supplemental Table 1 provides an overview of several popular systems, and Supplemental Figure 1 depicts components common to many imaging systems. Although most IMI systems have been designed for open surgical procedures, many systems have also been adapted for laparoscopic and robotic use, including the Firefly (Intuitive Surgical) and the Artemis (Quest). Most available imaging systems have been optimized for use with ICG, and development of new systems operating in other light wavelengths is required.
Oncologic Applications of IMI of Brain Cancer
Surgical treatment for high-grade gliomas (HGGs) made a remarkable advance with the 2017 FDA approval of 5-ALA (Gleolan) for the identification of HGGs (15). Although 5-ALA has revolutionized HGG treatment, its 635-nm emission wavelength is problematic in that many other anatomic structures are also visible at this shorter wavelength, detracting from the contrast provided by the fluorochrome. Toward this end, NIR agents such as ICG are being tested as alternatives.
Second-window ICG, also known as TumorGlow, involves administering ICG at a high concentration and waiting 24 h for the ICG to clear out of normal tissue. A phase I trial by Lee et al. (NCT02280954) found that TumorGlow had an average SBR of 7.5 and sensitivity and positive predictive value both around 85% (16). TumorGlow could visualize tumors through the dura to a depth of 13 mm (17).
In pediatric neurosurgery, tozuleristide, a chlorotoxin and ICG--conjugated tracer, has been studied with success in 4 phase I clinical trials (9). The cohorts in these studies demonstrated a more than 95% malignant lesion localization ex vivo and 89% specificity in a wide variety of neurologic malignancies. There is currently a PNOC012 (Pacific Pediatric Neuro-oncology Consortium) sponsored randomized controlled trial ongoing (NCT03579602) (18).
Lung Cancer
IMI has demonstrated strong success in identifying lung adenocarcinomas by facilitating tumor removal and enabling visualization of nearby vital structures (Fig. 3). However, the high smoking prevalence in this patient population renders unique challenges, as anthracosis generates significant autofluorescence that can reduce IMI efficacy (19). Nevertheless, several clinical trials have provided strong evidence for the value of IMI in thoracic surgery.

IMI has been used with great success in thoracic surgery, where it can clearly delineate tumor boundaries and facilitate complete R0 resection.
On the basis of the high expression of FRɑ by lung adenocarcinomas, fluorescent tracers have been conjugated to folic acid for thoracic surgery. Pafolacianine (OTL38), a cyanine based-NIR dye conjugated to folic acid, has demonstrated success in identifying positive margins and occult synchronous lesions. A phase I trial conducted at the University of Pennsylvania found that pafolacianine identified all (21/21) preoperatively identified lung adenocarcinomas and could also detect subcentimeter pulmonary nodules and ground glass opacities (20). In a subsequent phase II trial of 110 patients, pafolacianine found 24 previously undetected nodules, 9 of which were cancers (10%), and detected 8 positive margins (9%). These findings changed clinical staging for 7 patients and improved outcome for 26% of patients (21). A phase III trial is currently ongoing (NCT04241315). Pafolacianine fluorescence quantification by TBR measurements generally do not provide information about the histopathologic nature of the tumor (22).
TumorGlow (second-window ICG) has also been used in the operative evaluation of primary and metastatic lung nodules. Okusanya et al. found that TumorGlow detected 16 of 18 primary nodules previously identified with manual palpation and visual inspection, and also identified 5 additional lesions, including some as small as 0.2 cm (23). Although TumorGlow has a high success rate in identifying lesions, it is limited by dye accumulation in areas of inflammation and consequently may overestimate the size of the tumor (24). TumorGlow has also been used to identify pulmonary sarcoma metastases with a sensitivity of 93.1% (25). In addition, TumorGlow can locate occult synchronous metastases, leading to increased surveillance, higher rates of adjuvant systemic chemotherapy, and overall improved progression-free survival (26).
As a result of these successes, several fluorescent tracers are in preclinical development for intraoperative detection of lung tumors. JAS239, a fluorescent carbocyanine that competitively inhibits choline kinase, is currently in veterinary clinical trials for the intraoperative detection of early stage adenocarcinomas in canines (27). Additionally, DDAO-arachidonate, a cytosolic phospholipase A2 activatable probe, is scheduled to enter veterinary trials in late 2022 (28).
Sentinel Lymph Node Biopsy
Sentinel lymph node (SN) biopsy is of critical importance in the surgical management of nearly all cancers, particularly breast cancer and melanoma. The use of fluorescence-guided SN biopsy is rising, but this field has benefited strongly from nuclear medicine; radiotracer–dye combinations for SN biopsy have existed since the 1990s with lymphoscintigraphy together with patent blue dye. Since then, refinements in technology and dyes (e.g., introduction of ICG) have increased SN biopsy efficiency, with greater numbers of SNs identified without increasing overall operation time (29).
The use of radiotracers mitigates the current inability of fluorescent markers to image deeply in the tissue, while the fluorescent molecule adds the benefit of direct visualization. Several recent trials have used ICG-99mTc-nanocolloid for SN biopsy, with strong results. In a trial of 495 patients, KleinJan et al. used ICG-99mTc-nanocolloid to identify 1,643 SN specimens. Radiation identified more than 98% of SNs, and fluorescence identified more than 95% of SNs. For nodes deeper than 0.5–1 cm, the radioactive signature allowed for accurate localization and removal (7). Another study of 404 patients with penile cancer found that ICG-99mTc-nanocolloid identified 98% SNs with the γ-probe and 96% with fluorescent imaging, with 100% of histologically tumor-positive SNs visualized intraoperatively by fluorescence (30).
Fluorescent tracers have also been tested in combination with photoacoustic imaging guidance, which can image deep tumors with high resolution (31). Many novel molecules have been tested for dual photoacoustic–fluorescent imaging, including various nanoparticles doped with fluorescent molecules. Recently, a trimodal imaging system has been developed that uses fluorescence, photoacoustic, and ultrasound guidance to identify SNs and reduce false-negative rates (32). Some of these multimodal systems have entered clinical trials. For example, Nishio et al. showed that panitumumab-IRDye800CW could be used for dual photoacoustic and fluorescence imaging (NCT02415881). They found that metastatic nodes had a photoacoustic signal 5 times and fluorescence signal double that of benign nodes (33).
Breast Cancer
Breast cancer therapy is being revolutionized by the Lumicell (LUM) Imaging System, which uses a far-red fluorescent, PEGylated, protease-activated molecule (LUM015). LUM015 requires only 1 s to image a 2.6-cm-diameter area, allowing examination of the entire lumpectomy cavity in less than a minute (13). A study of 45 patients and 570 cavity margin images found a sensitivity of 84% for tumor detection and specificity of 73%. In the 8 patients with positive margins, LUM015 could detect residual tumor with a sensitivity of 100% (34). A follow-up multisite phase II study (NCT03321929) enrolling 234 patients showed that LUM015 can detect residual disease missed by histopathologic evaluation in 10% of patients, sparing them from reoperation (35).
Numerous other fluorescent molecules and imaging systems are currently being studied for breast cancer treatment. For example, bevacizumab-IRDye800CW can detect microscopic margins in 10% of excised masses (36). A nanoparticle-based formulation of ICG (ONM-100) has shown strong ability to identify occult lesions and positive margins in a phase II study (14). Other fluorescent molecules such as gGlu-HMRG and AVB-620 are also being studied. The Smart Goggle system, a wearable, stereoscopic imaging modality with a handheld microscopy unit, is being used to study ICG accumulation in SNs of patients with breast cancer (NCT02802553). IMI has also been used in breast reconstruction to assess tissue perfusion during nipple-sparing mastectomies.
Several hybrid tracers have been studied in preclinical trials for breast cancer. Sampath et al. labeled the HER2 antibody trastuzumab with 64Cu and IRDye800, generating (64Cu-DOTA)n-trastuzumab-(IRDye800)m. The radioactive signature could detect lung metastases, and ex vivo fluorescence measurements could detect malignant cells in the lung, muscle, skin, and lymph nodes (37). Two trials of ICG-99mTc-nanocolloid also recently showed that fluorescence and lymphoscintigraphy could be used together to detect SNs and identify additional SNs that were not detected preoperatively (38,39).
Head and Neck Malignancies
IMI may be particularly important in the surgical management of head and neck cancers due to the difficulty of orienting resected masses, the need to remove all lymph node metastases, and the proximity to neurovascular structures. Hybrid tracers are of great importance given the need for lymph node dissection. Stoffels et al. evaluated ICG-99mTc-nanocolloid in a prospective trial of 40 patients with head and neck cancer (DRKS00004622), finding that the hybrid tracer could identify sentinel nodes in 100% of patients (40).
Several IMI agents target epidermal growth factor receptor (EGFR), which is expressed in more than 90% of head and neck cancers. Early trials have shown strong results for IRDye800CW conjugated to either cetuximab or panitumumab. The pilot study of cetuximab-IRDye800CW in 12 patients (NCT01987375) found a tumor-to-background ratio of 5.2 and correlation of fluorescence intensity with EGFR histologic expression (41). Panitumumab-IRDye800CW had similarly strong results (NCT02415881) (42).
Equally important to tumor removal is the preservation of nerve structures and microvascular perfusion of thyroid and parathyroid. Although nerve labeling has been a challenge in IMI because of their low metabolic rate, several molecules have demonstrated potential. ALM-488, a peptide-fluorescein derivative conjugate, received fast-track designation by the FDA in 2021 after strong data from a phase I/II clinical trial (NCT04420689). Since most tracers used to identify tumors have NIR emission wavelengths, ALM-488 can be used concurrently with other agents to identify the tumor and nearby nerves (9). On the other hand, efforts to create nerve NIR tracers seek to leverage the low autofluorescence and scattering of NIR. Such experimental compounds include synthetic oxazine derivatives, which can identify nerves buried to a depth of 3 mm (43).
Sarcoma
TumorGlow (second-window ICG) has been shown to be a valuable tool for localization of pulmonary sarcoma metastasis (Supplemental Videos 1–2). In a study of 30 patients undergoing IMI-guided metastasectomy, Predina et al. found that TumorGlow identified 24 occult lesions, of which 21 (88%) were malignant (25). In a long-term follow-up study, Azari et al. demonstrated that patients who underwent TumorGlow infusion had increased occult lesion detection, follow-up surveillance, use of adjuvant therapy, and survival compared with patients who received standard care (non–IMI-guided metastasectomy) (26). There are plans to initiate a phase III randomized controlled trial evaluating TumorGlow for sarcoma metastasectomy.
Targeted fluorochromes have also been studied for sarcoma resection, with EGFR being a popular target given its frequent overexpression in sarcomas. ABY-029, an anti-EGFR Affibody conjugated to IRDye800CW, was found to have excellent localization to various extremity soft-tissue sarcomas with an average TBR of 3.25 (NCT03154411) (9). Importantly, the fluorescence patterns were not affected by neoadjuvant chemoradiotherapy, which is significant as aggressive upfront therapy is a mainstay of treatment for high-grade disease.
Gastrointestinal Malignancies
CEA is expressed in more than 90% of colorectal malignancies, particularly adenocarcinomas. SGM-101 (Surgimab), an anti-CEA antibody conjugated to the far-red absorbing fluorochrome BM-104, has been studied in multiple clinical trials. Schaap et al. showed in a multicenter pilot study (NCT02973672) that SGM-101 had a sensitivity of 98.5%, specificity of 62.2%, positive predictive value of 82.3%, and negative predictive value of 95.8% in detecting lesions (11). Boogerd et al. and de Valk et al. have similarly demonstrated utility of SGM-101 in CEA-positive (CEA+) primary lesion localization and detection of occult satellite lesions in the peritoneum, liver, and omentum (44,45). There is currently a phase I trial exploring SGM-101 in the detection of CEA+ lung metastases and primary CEA+ lung tumors (NCT04315467).
Pancreatic adenocarcinoma is currently the fourth leading cause of cancer-related death in the United States and is increasing in incidence (1). The desmoplastic reaction and dense stroma present a difficulty for IMI by blocking both the tracer and the excitation source. Nevertheless, some studies have demonstrated potential. Newton et al. have demonstrated that TumorGlow could identify positive microscopic margins, with fluorescence visualized in 11 of 12 pancreatic ductal adenocarcinoma tumors. TumorGlow was also able to detect dysplastic and premalignant mucinous neoplasms. Lack of fluorescence correlated with complete response to neoadjuvant chemoradiotherapy, significant because response to neoadjuvant therapy is difficult to discern due to anatomic and treatment-related changes (46).
Ovarian Cancer
Cytoreductive surgery is important in the management of ovarian cancer and improves outcomes, especially if patients have no residual disease. Given the frequent overexpression of FRɑ in ovarian cancer, trials have investigated the use of pafolacianine in ovarian cancer resection. A multicenter phase II clinical trial (NCT02317705) evaluated 225 lesions from 29 patients, finding that pafolacianine had a sensitivity of 86% and positive predictive value of 88%. Additional lesions not detected preoperatively were found in almost half of the patients (47). The follow-up phase III trial of 150 patients (NCT03180307) found that intraoperative imaging detected additional lesions not identified by white light in 33% of patients. Complete resection was achieved in 62.4% of patients (48). These strong results spurred the November 2021 FDA approval of pafolacianine for ovarian cancer.
Prostate Cancer
Radical prostatectomy with lymph node dissection is efficacious for prostate cancer treatment but still results in recurrence rates of 20%–40%. IMI can improve lymph node dissection, especially given the atypical location of some nodes and their proximity to nerves. Several targeted tracers have been developed that take advantage of the high expression of prostate-specific membrane antigen (PSMA) on prostate cancer (49).
PSMA-targeting fluorochromes have existed since 2005, when Humblet et al. conjugated the IRDye78 to the PSMA inhibitor GPI (GPI-78) and found that it accumulated in xenograft tumors (50). Many other PSMA ligands have since been conjugated to dyes such as IRDye800 and Cy5.5, although most of these molecules are still in preclinical development. However, the ProMOTE IR800 IAB2 M trial in the United Kingdom is currently enrolling and evaluating the efficacy of IRDye800CW conjugated to IAB2 M, a minibody engineered from an anti-PSMA antibody.
Hybrid tracers have also been developed for prostatectomy. For example, Lütje et al. conjugated the anti-PSMA antibody D2B with IRDye800CW and 111In, finding that xenograft tumors could be detected using both fluorescence and SPECT/CT imaging (51). Hensbergen et al. synthesized several hybrid tracers featuring the PSMA-inhibiting motif glutamate-urea-lysine (EuK), labeled them with 99mTc, and found 99mTc-EuK-(SO3)Cy5-mas3 to have good kinetics and high tumor-to-muscle ratio (52). There are myriad combinations of fluorescent molecules with targeting molecules and radiotracers, such as 111In-LICOR-800CW-Lys-DOTA-EuK and 68Ga-NIR 800CW-PSMA-11, although these are all still in preclinical development.
DISCUSSION
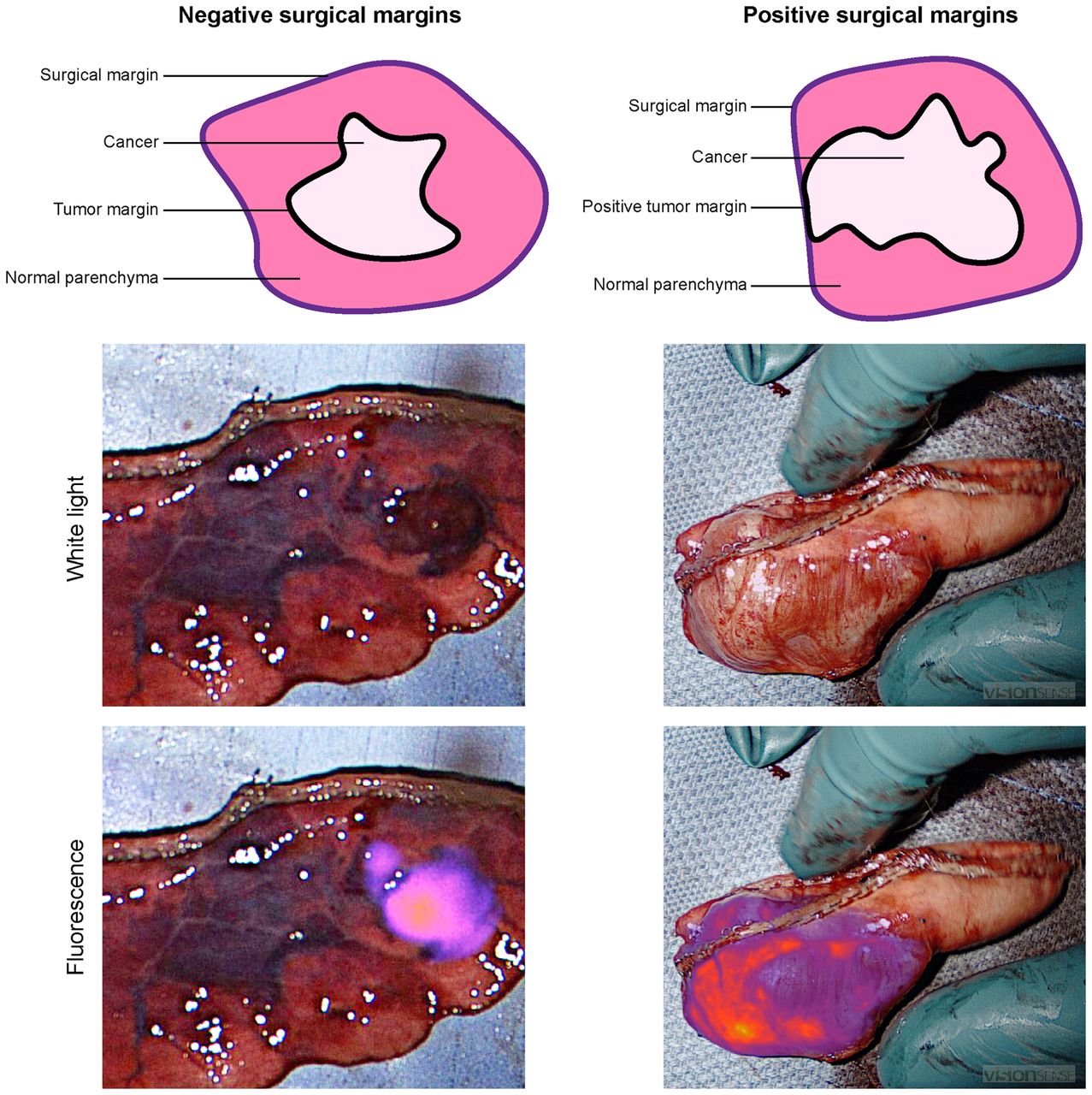
Thanks to exponential advances in nuclear medicine, today’s patients can walk into the clinic, and within a day, a surgeon will know the anatomic location and aggressiveness of the tumor, as well as the functional limitations of performing surgical intervention. However, this precision medicine often stops at the doors of the operating room. Surgeons still rely on tactile and visual feedback to perform oncologic resection, a technique that has not changed since the first days of modern surgery. IMI promises to address the challenge of complete tumor removal with negative margins (Fig. 4) and improve outcomes.

Oncologic resection prioritizes complete tumor removal with negative margins. Residual tumor left behind at the margin frequently necessitates reoperation and leads to poorer outcomes for patients.
The oncologic potential of IMI has been demonstrated in numerous cancers. In the lung, for example, pafolacianine can delineate primary tumors, identify occult synchronous lesions, and assess margin adequacy (20,21). Surgeons can confirm complete lesion removal within minutes and proceed with appropriate surgery, without waiting for frozen section confirmation. This saves patients time under anesthesia, reduces operating room costs, and ensures oncologically sound resection even if the lesion is not seen or felt by the surgeon (53). Furthermore, with the development of ALM-488 and oxazine derivatives, IMI can also identify neurovascular structures and prevent their damage (3,9). In our experience, IMI-guided evaluation does not add undo inconvenience and easily incorporates into routine thoracoscopic techniques and equipment.
Despite recent exponential developments in IMI, this modality is still in its technologic infancy and has significant challenges to overcome. Fluorescent tracers suffer from limited tissue depth penetration, fluorescence bleaching, and background autofluorescence, all of which can make in vivo imaging difficult (5). Autofluorescence is a particularly significant problem in lung resection, where smoking-induced anthracosis is common (19). NIR-II (>1,000 nm) and hybrid radioactive-fluorescent tracers will help with these issues, as will hybrid radioactive-fluorescent tracers, which have much less tissue attenuation (7). The same radioisotope used for intraoperative guidance can also be used for preoperative imaging studies. However, hybrid tracers bring their own set of limitations, particularly with dosing—many radioisotopes are used at picomolar concentrations to minimize radiation exposure, whereas most fluorescent tracers are used at micromolar concentrations (8). Microdosing techniques show promising results in combining nuclear medicine with fluorescence guidance to improve intraoperative localization.
There are already dozens of fluorochromes, radioisotopes, and targeting molecules that have been conjugated in hundreds of combinations, with possibly thousands of experimental compounds on the way (2,5,6). However, the history of IMI use in oncologic surgery is short (<20 y), resulting in the research on these compounds being mostly preclinical. The few clinical studies that have been conducted include fewer than a hundred patients. Randomized controlled trials involving at least several hundred patients, such as those being conducted or recently concluded for pafolacianine, LUM015, and ICG-99mTc-nanocolloid, are necessary to better delineate the added value of IMI over the current standard of care (21,30,35). It will be critical to not only collect data on the number of additionally identified lesions and positive margins, but also note whether patients have a change in their staging, adjuvant treatment, and overall survival.
CONCLUSION
IMI-guided surgical resections are becoming commonplace in the management of oncologic diseases, with dozens of fluorescent molecules being investigated. The technology lies in the continuum of radiologic diagnostic evaluation and histologic confirmation, drawing on significant advances developed by nuclear medicine (Fig. 5). Although preclinical and early clinical trials have already shown the ability of IMI to refine oncologic resections, further studies are needed to elaborate on the optimal patient characteristics that stand to benefit from IMI. Continued innovation in combining radiotracers with fluorescent molecules, together with development of novel NIR-II fluorophores, will alleviate some of the current challenges of IMI implementation. Clinicians should be aware of the developments in this field, as IMI will likely be added to the mainstay arsenal of tools in surgical oncology.
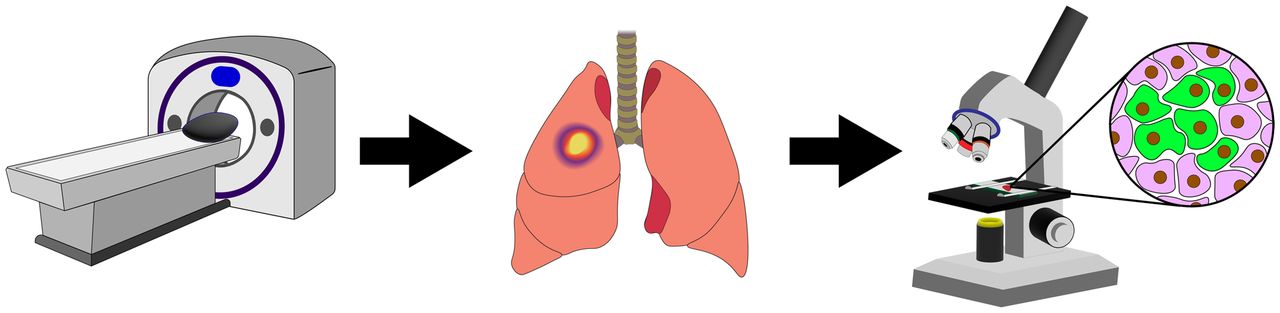
IMI lies within the continuum of preoperative radiologic evaluation and intra- or postoperative histologic confirmation, complementing these technologies and offering improved outcomes for patients.
DISCLOSURE
Dr. Feredun Azari was supported by the training grant in Surgical Oncology by the National Institutes of Health (T32 CA251063), Society of Thoracic Surgeons Thoracic Surgery Foundation Research Award, and the Stephen C.C Cheung Award in Surgical Oncology. Dr. Edward J. Delikatny and Dr. Sunil Singhal were supported by the National Institutes of Health (R01 CA226412, R01 CA266234, and P01 CA254859). Dr. Gregory T. Kennedy was supported by the American Philosophical Society and the National Institutes of Health (F32 CA254210-01). No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 11, 2022.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 1, 2022.
- Revision received August 11, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.