


Visual Abstract

Abstract
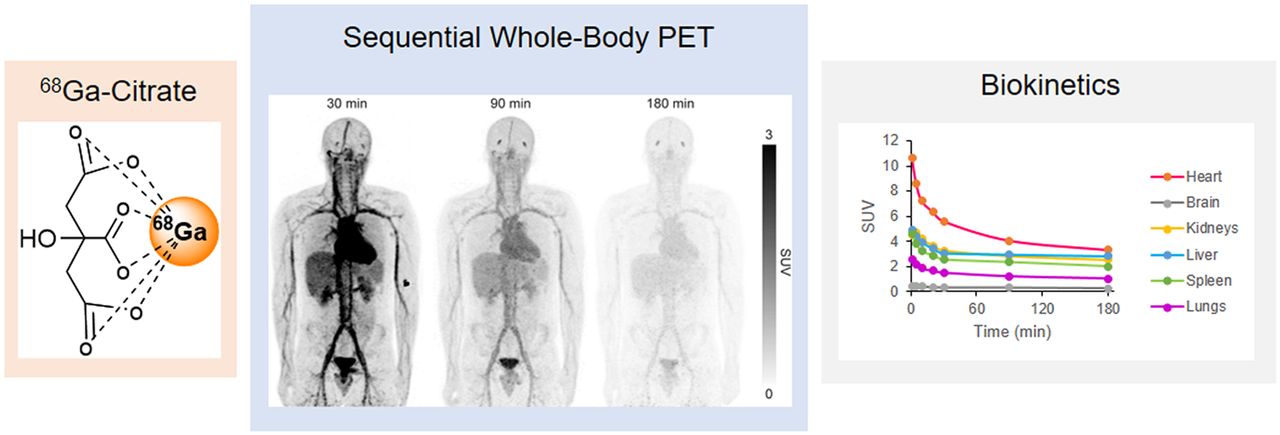
68Ga-citrate has one of the simplest chemical structures of all 68Ga-radiopharmaceuticals, and its clinical use is justified by the proven medical applications using its isotope-labeled compound 67Ga-citrate. To support broader application of 68Ga-citrate in medical diagnosis, further research is needed to gain clinical data from healthy volunteers. In this work, we studied the biodistribution of 68Ga-citrate and subsequent radiation exposure from it in healthy men. Methods: 68Ga-citrate was prepared with an acetone-based radiolabeling procedure compliant with good manufacturing practices. Six healthy men (age 41 ± 12 y, mean ± SD) underwent sequential whole-body PET/CT scans after an injection of 204 ± 8 MBq of 68Ga-citrate. Serial arterialized venous blood samples were collected during PET imaging, and the radioactivity concentration was measured with a γ-counter. Urinary voids were collected and measured. The MIRD bladder-voiding model with a 3.5-h voiding interval was used. A model using a 70-kg adult man and the MIRD schema was used to estimate absorbed doses in target organs and effective doses. Calculations were performed using OLINDA/EXM software, version 2.0. Results: Radioactivity clearance from the blood was slow, and relatively high radioactivity concentrations were observed over the whole of the 3-h measuring period. Although radioactivity excretion via urine was rather slow (biologic half-time, 69 ± 24 h), the highest decay-corrected concentrations in urinary bladder contents were measured at the 90- and 180-min time points. Moderate concentrations were also seen in kidneys, liver, and spleen. The source organs showing the largest residence times were muscle, liver, lung, and heart contents. The heart wall received the highest absorbed dose, 0.077 ± 0.008 mSv/MBq. The mean effective dose (International Commission on Radiological Protection publication 103) was 0.021 ± 0.001 mSv/MBq. Conclusion: PET imaging with 68Ga-citrate is associated with modest radiation exposure. A 200-MBq injection of 68Ga-citrate results in an effective radiation dose of 4.2 mSv, which is in the same range as other 68Ga-labeled tracers. This suggests the feasibility of clinical studies using 68Ga-citrate imaging in humans and the possibility of performing multiple scans in the same subjects across the course of a year.
For PET imaging, 68Ga is a transition metal that can be used as 68Ga-citrate or 68Ga-chloride and also in its chelated forms with biomolecules (e.g., chelator-conjugated peptides). 68Ga-labeled pharmaceuticals are frequently used in nuclear medicine and can conveniently be manufactured with kits and fully automated commercially available devices (1). 68Ga-citrate is one such 68Ga-radiopharmaceutical that has entered the clinical trial stage, and its use in PET is based on Ga3+ uptake and transportation mechanisms. Ga3+ is considered an analog of Fe3+ and binds to transferrin and other biomolecules in vivo. Although only a few human studies using 68Ga-citrate PET have been performed (2–13), 68Ga-citrate has already been shown to be a sensitive and specific PET tracer for the imaging of infection and inflammation, including inflammatory bowel disease (3), bone infection (4), intraabdominal infection (5), and prosthetic joint infection (12). In addition, we recently observed unexpectedly high 68Ga-citrate accumulation in atherosclerotic lesions in patients with Staphylococcus aureus bacteremia (8). Furthermore, patients with high-grade glioma, hepatocellular carcinoma, and prostate cancer have been imaged with 68Ga-citrate according to the hypothesis that Ga3+ uptake should increase in these tumors because of upregulated activity of transferrin receptor (7,9–11). Evidence from clinical and preclinical investigations (7,14,15) suggests that 68Ga-citrate has potential in several clinical applications and that further research is warranted.
The purpose of this clinical study was to determine the biodistribution of intravenously administered 68Ga-citrate in healthy male volunteers. This information will help to determine the optimal PET protocol for 68Ga-citrate imaging of inflammatory and infectious diseases and cancer. The whole-body imaging should allow identification of those organs that are most exposed to ionizing radiation and allow calculation of the dose absorbed by each organ.
MATERIALS AND METHODS
Chemicals and Reagents
All chemicals were purchased from commercial sources and were of reagent, analytic, ultrapure, or European Pharmacopeia grade.
Preparation of 68Ga-Citrate
68Ga-citrate (Fig. 1A) was produced according to an established protocol (3). Aqueous hydrochloric acid (0.1 M, 6 mL) was used to elute 68Ga radioactivity from a 68Ge/68Ga generator (IGG-100, 1,850 MBq; Eckert and Ziegler Isotope Products), and the 68Ga-eluate was passed through a cation-exchange cartridge (Strata X-C; Phenomenex Inc.). The retained 68Ga was eluted into a reaction vial with acidified acetone (800 μL, containing 0.02 M HCl and 3.25% water). The acetone was removed by evaporation for 4 min at 110°C, and sodium citrate buffer (4 mL) was added. After 4 min, the reaction mixture was sterile-filtrated into an end-product vial and diluted with saline (9 mg/mL, 6 mL). Radiochemical purity was measured by instant thin-layer chromatography with methanol/acetic acid (9:1, v/v) as a mobile phase.

(A) Chemical structure of 68Ga-citrate. (B) Quality control of 68Ga-citrate with instant thin-layer chromatography developed using methanol/acetic acid (9:1, v/v) as mobile phase and visualized and quantified by autoradiography.
Subjects
Six healthy male volunteers (age, 41 ± 13 y; weight, 75 ± 4 kg; height, 177 ± 4 cm) participated in this trial. 68Ga-citrate was injected via a catheter inserted into an antecubital vein, and blood samples were drawn through another catheter inserted into the contralateral arm.
Before the start of this clinical trial, approvals were obtained from the joint Ethics Committee of the University of Turku and Turku University Hospital, as well as from the Finnish Medicines Agency. Full informed consent was obtained in writing from all subjects beforehand. This study is registered at ClinicalTrials.gov (NCT01951300).
Questionnaires were used to assess the absence of significant medical, neurologic, and psychiatric history and of any history of alcohol or drug abuse. In addition, routine blood tests, electrocardiography, a physical examination, and a review of medical history were performed for each subject.
PET/CT Imaging
The biodistribution of 68Ga-citrate was imaged using a Discovery 690 PET/CT scanner (GE Healthcare). This scanner combines 64-slice CT with PET acquired using 24 rings of lutetium-yttrium-orthosilicate detectors, which provide 47 imaging planes with an axial field of view of 15.7 cm. A low-dose CT scan for attenuation correction and anatomic reference was acquired before the PET scan, using a voltage of 120 kV and current of 10 mA. Whole-body PET acquisitions were made 1, 5, 10, 20, 30, 90, and 180 min after an intravenous injection of 204 ± 8 MBq of 68Ga-citrate. The acquisition times per bed position were 20, 30, 65, 65, 120, 240, and 240 s, respectively. The scanning at 90 min after injection included 14 bed positions covering the range from the head to the toes, whereas all other scans used only 8 bed positions covering the range from the head to mid thighs.
PET images were reconstructed using a time-of-flight 3D VUE Point algorithm (GE Healthcare) with 2 iterations, 24 subsets, and a postprocessing filter of 6.4 mm in full width at half maximum. Scatter correction, random counts, and dead-time corrections were all incorporated into the reconstruction algorithm. The final matrix size was 192 × 192 × 47 voxels. The plane thickness of the PET scanner was 3.27 mm, and the axial spatial resolution for 3-dimensional mode was 4.74 mm in full width at half maximum at a 1-cm offset from the center of the field of view (16).
Blood and Urine Measurements
Serial arterialized (the arm was heated with a wrapped heating pad) venous blood samples were collected into heparinized tubes at 1, 5, 10, 20, 30, 60, 90, 180, and 240 min after the injection of 68Ga-citrate. The radioactivity of the whole blood was measured with an automatic γ-counter (1480 Wizard 3″; EG&G Wallac). Plasma was separated by centrifugation (2,100g for 5 min at 4°C), and the plasma radioactivity was measured. The plasma concentration at baseline (C0) was estimated by fitting a monoexponential function to the plasma concentrations collected between 5 and 30 min.
The subjects were asked to urinate during 2 breaks in the PET imaging session and again after the session. The mean times for urination were 61 min after injection, 163 min after injection, and 218 min after injection. Urinary voids were collected, the total volume was measured, and a 2.5-mL sample was taken for radioactivity measurement with a VDC 405 dose calibrator (Veenstra Instruments).
Distribution Kinetics and Radiation Dose Estimates
Eclipse software (version 13.6; Varian Medical Systems) was used to define the radioactivity concentrations of the source organs at different time points. The source organ volumes either were defined on CT images or were the volumes of the organs of the reference man (17).
Residence times in source organs were calculated from area under the time–activity curves. The curves were defined by fitting a sum of 2 exponential functions. The MIRD bladder-voiding model (18) with a 3.5-h voiding interval was used. A model with a 70-kg adult man and MIRD schema (19) was used to estimate the absorbed doses in the target organs and the effective doses. Calculations were performed using OLINDA/EXM software, version 2.0. In addition, OLINDA 1.0 results were calculated.
RESULTS
Radiochemistry
The manufactured 68Ga-citrate fulfilled all the product quality specifications (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org) for clinical use. The radiochemical purity was at least 95%, pH was in the range of 3.0 − 7.0, and the acetone content was no more than 0.5%. An example instant thin-layer chromatography plot used to determine radiochemical purity is shown in Figure 1B.
Biodistribution and Biokinetics
Whole-body dynamic PET/CT imaging data were obtained from 6 subjects over a period of 180 min after 68Ga-citrate administration. Figure 2 shows representative images from a subject. The radioactivity concentrations in 20 organs or tissues of interest were quantified at time points of 1, 5, 10, 20, 30, 90, and 180 min, and the results are presented in Supplemental Table 2. At 30 min after injection, SUVs in the brain, heart contents, kidneys, liver, trabecular bone, and red marrow were 0.26 ± 0.04 (mean ± SD), 5.16 ± 0.48, 3.15 ± 0.46, 2.78 ± 0.25, 0.70 ± 0.15, and 1.80 ± 0.12, respectively. Figure 3 shows time–activity curves for the 20 organs or tissues, revealing the whole-body distribution kinetics of radioactivity over the 180 min after 68Ga-citrate administration.

Whole-body distribution of 195 MBq of 68Ga-citrate in healthy 22-y-old man (73 kg).

Time–activity curves of main organs. Circles represent each individual, and line is average.
The mean voided radioactivity at a mean void time of 61 min after injection (during a break between PET imaging session) was 1.76 ± 0.47 percentage injected dose (Fig. 4). All 6 subjects were able to urinate during the first PET imaging session break, 3 were able to urinate between imaging session 2 and 3, and 2 after the complete imaging session.

Percentage of injected 68Ga-citrate radioactivity dose (%ID) in urine as function of time.
Radioactivity clearance from the blood was slow (Fig. 5). The C0 in SUV units was 17.3 ± 1.8 g/mL (Supplemental Table 3). The inverse of C0, which is related to the total plasma volume, was 0.059 ± 0.006 L/kg. The plasma concentration at 4 h (n = 5) was 5.8 ± 0.6 g/mL, and its inverse, which may be related to the extracellular volume of the body, was 0.17 ± 0.02 L/kg.

Concentration of radioactivity in arterialized venous plasma as function of time after 68Ga-citrate injection. Dots represent each individual, and line is average.
Residence Times and Radiation Dose Estimates
The residence times (normalized numbers of disintegrations) were determined for the source organs and the remainder of the body of each subject, and their mean ± SD, range, and coefficient of variation are listed in Table 1. The coefficients of variation were in the range of 4%−49%. The largest residence times were in muscle (0.365 ± 0.043 h), liver (0.091 ± 0.017 h), lungs (0.079 ± 0.008 h), and heart contents (0.048 ± 0.006 h).
Residence Times (Hours) in Source Organs After Injection of 68Ga-Citrate
The organ dose estimates (Table 2) were calculated for a 70-kg adult man. The organs with the highest doses were the heart wall (0.077 ± 0.008 mSv/MBq), urinary bladder wall (0.039 ± 0.010 mSv/MBq), kidneys (0.036 ± 0.004 mSv/MBq), and lungs (0.036 ± 0.003 mSv/MBq). The lowest dose was in the brain (0.004 ± 0.001 mSv/MBq). The mean effective dose (International Commission on Radiological Protection publication 103) (20) was 0.021 ± 0.001 mSv/MBq. Thus, the effective dose from 200 MBq of injected radioactivity of 68Ga-citrate was 4.2 mSv.
Organ Doses and Effective Doses (mSv/MBq) After Injection of 68Ga-Citrate
Organ dose estimates according to OLINDA 1.0 are presented in Supplemental Table 4.
DISCUSSION
We previously studied 68Ga-citrate in experimental disease models, as well as in patients with infections (8,15,21). The current study was a basic investigation in healthy humans to collect data on whole-body distribution kinetics and radiation dose estimates, which will be useful in planning future clinical trials with 68Ga-citrate.
Preparation of 68Ga-Citrate
The radiopharmaceutical 68Ga-citrate was produced using a straightforward protocol (3). The acetone-based cation-exchange cartridge elution method is an effective option for concentrating 68Ga radioactivity eluted from a generator (1). In our hospital, this method is used to manufacture 3 radiopharmaceuticals, including 68Ga-citrate, in a fully automated manner. Citrate is a natural ligand that can coordinate some metal ions, including gallium. Because of the nature of the nuclear physics of 68Ga, the molarity of 68Ga in a batch of eluate from a 68Ge/68Ga generator is tiny. By contrast, the molarity of citrate (0.14 mmol) is in great excess to ensure efficient coordination, which is neither feasible nor typical in the production of many other 68Ga-radiopharmaceuticals. In this sense, citrate acts also as a vehicle, in addition to its role as a chelator. On instant thin-layer chromatography, the chromatography behaviors of 68Ga-citrate and free 68Ga show a clear difference (Fig. 1B); free 68Ga remains at the baseline whereas 68Ga-citrate migrates up on the instant thin-layer chromatography, with a retention factor of 0.93. As there is not a citrate dose limit set in the European Pharmacopeia; quantification of the citrate in the end-product formulation is not relevant in the quality control procedure.
PET Imaging and Biodistribution
In a typical 68Ga-radiopharmaceutical, the 68Ga-radionuclide is attached to a targeting molecule, such as a peptide, and the targeting molecule takes the radioactivity to the specific organs and tissues to be imaged. In the case of 68Ga-citrate, the imaging and biodistribution are most probably based on the biologic mechanisms of 68Ga3+, which can be chelated in vivo with biomolecules, including ferritins (13). This implies that in vivo transmetalation takes place, even though citrate has sufficient strength to coordinate 68Ga3+ in the manufacturing procedures. However, comparison studies have indicated that the imaging performance of 68Ga-citrate is better than that of intravenously injected 68Ga-chloride, at least as far as the limited available evidence shows (15), which might be an indication that citrate plays a role as a vehicle in the in vivo biodistribution. In this study, particular care was taken to ensure that the 68Ga-citrate injection did not involve any gallium colloids, which usually accompany the 68Ge/68Ga generator eluate or are formed if injected as 68Ga-chloride.
For the PET imaging, each subject was intravenously administered 204 ± 8 MBq of 68Ga-citrate. In a routine PET procedure performed in our hospital, such as one using the standard tracer 18F-FDG, the typical radioactivity dose is 4 MBq/kg of body weight. In this study, we used 204 ± 8 MBq (2.7 ± 0.2 MBq/kg) of 68Ga-citrate per subject, which is in the typical dose range of our 68Ga-radiopharmaceutical PET studies. The mass of gallium injected was negligible. It is noteworthy that when gallium is administered as a drug in high doses, the biodistribution is known to change (22,23).
The sequential whole-body imaging was performed for 180 min to monitor the tracer kinetics in vivo. For visualization purposes, we prepared representative PET/CT images from a 22-y-old man and scaled the SUVs from 1 to 3 (Fig. 2). These images clearly show that the radioactivity concentration was much higher in heart, liver, lungs, and kidneys than in other organs. At 180 min after injection, the whole-body radioactivity concentration became very low, an indication of a sufficient data collection time range. To further quantify the radioactivity concentration in the 20 organs of interest, time–activity curves were drawn from 0 to 180 min after administration (Fig. 3). Among the organs and tissues, the time–activity curves from gallbladder, lower large intestine (left colon and rectum), testes, and upper large intestine (right colon) were still increasing slightly at 180 min. It was not clear what factors might have caused the slight accumulations in these organs. In cortical bone, red marrow, small intestine, and trabecular bone, the time–activity curves showed a steady radioactivity residence along with time. In the urinary bladder, the general trend of radioactivity development was an initial increase and then a decrease. In the rest of the organs, the time–activity curves decreased to varying extents over the period.
The radioactivity concentration in plasma stayed at a high level (Fig. 5), similar to that reported previously for the 68Ge/68Ga generator eluate 68Ga-chloride in a study on rats (24); the slow decrease at 3–4 h prevents reliable estimation of the total area under the curve (from time zero to infinity) and total clearance. In previous animal studies, we found that the in vivo kinetics of 68Ga-citrate and 68Ga-chloride differed, possibly because the chelating properties of citrate prevent the precipitation of 68Ga(OH)3 (15).
Radiation Dose Estimates
To determine the radiation burden, we analyzed the kinetics of radioactivity concentration in the main organs of healthy men up to 3 h after an intravenous bolus injection of 68Ga-citrate. In addition to the SD and range, the coefficient of variation was used to indicate the precision and repeatability of the measurements among the 6 subjects. Our results revealed that the heart wall received the highest radiation dose, followed by the urinary bladder wall. This may be partially due to the relatively slow blood clearance and urinary excretion as the main clearance route. However, the relatively slow blood clearance was not a problem for target visualization in previous studies. The organ with the lowest radiation exposure was the brain (0.004 ± 0.001 mSv/MBq). Overall, the effective dose of 68Ga-citrate (0.021 ± 0.001 mSv/MBq) was comparable to that of widely used PET tracers, including 68Ga-DOTANOC (0.025 mSv/MBq) (25) and 18F-FDG (0.019 mSv/MBq) (26). For example, a 200-MBq dose of 68Ga-citrate may result in an effective dose of 4.2 ± 0.2 mSv.
CONCLUSION
The radiation burden from administration of 68Ga-citrate for PET imaging is comparable to that of other commonly used 68Ga-radiopharmaceuticals. The low radiation exposure of 68Ga-citrate would allow for studies with multiple scans in the same individuals over the course of a year.
DISCLOSURE
The study was conducted within the Finnish Centre of Excellence in Cardiovascular and Metabolic Diseases, supported by the Academy of Finland, University of Turku, Turku University Hospital, and Åbo Akademi University. The study was financially supported by grants from the State Research Funding of Turku University Hospital and the Sigrid Jusélius Foundation. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What are the distribution kinetics of 68Ga-citrate in healthy humans, and what is the radiation burden resulting from its administration?
PERTINENT FINDINGS: Six healthy men underwent dynamic whole-body PET/CT imaging with blood and urine measurements. 68Ga-citrate showed slow clearance from the blood circulation through renal excretion. The highest radiation exposure was to the heart wall. The effective dose of 0.021 mSv/MBq is similar to that of other commonly used 68Ga tracers.
IMPLICATIONS FOR PATIENT CARE: The characteristics of 68Ga-citrate are favorable for human studies involving multiple scans in the same subject over the course of a year.
ACKNOWLEDGMENTS
We thank the technical and nursing staff at Turku PET Centre for their assistance in this work, and we thank Timo Kattelus for preparing figures.
Footnotes
Published online Mar. 10, 2022.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication January 28, 2022.
- Accepted for publication March 7, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.