


Visual Abstract

Abstract
We aimed to explore whether the imaging of antiporter system xC− of immune cells with (4S)-4-(3-18F-fluoropropyl)-l-glutamate (18F-FSPG) PET can assess inflammatory bowel disease (IBD) activity in murine models and patients (NCT03546868). Methods: 18F-FSPG PET imaging was performed to assess IBD activity in mice with dextran sulfate sodium-induced and adoptive T-cell transfer–induced IBD and a cohort of 20 patients at a tertiary care center in South Korea. Immunohistochemical analysis of system xC− and cell surface markers was also studied. Results: Mice with experimental IBD showed increased intestinal 18F-FSPG uptake and xCT expression in cells positive (+) for CD11c, F4/80, and CD3 in the lamina propria, increases positively associated with clinical and pathologic disease activity. 18F-FSPG PET studies in patients, most of whom were clinically in remission or had mildly active IBD, showed that PET imaging was sufficiently accurate in diagnosing endoscopically active IBD and remission in patients and bowel segments. 18F-FSPG PET correctly identified all 9 patients with superficial or deep ulcers. Quantitative intestinal 18F-FSPG uptake was strongly associated with endoscopic indices of IBD activity. The number of CD68+xCT+ and CD3+xCT+ cells in 22 bowel segments from patients with ulcerative colitis and the number of CD68+xCT+ cells in 7 bowel segments from patients with Crohn disease showed a significant positive association with endoscopic indices of IBD activity. Conclusion: The assessment of system xC− in immune cells may provide diagnostic information on the immune responses responsible for chronic active inflammation in IBD. 18F-FSPG PET imaging of system xC− activity may noninvasively assess the IBD activity.
Inflammatory bowel disease (IBD) consists of 2 types of chronic incurable intestinal disorders, ulcerative colitis (UC) and Crohn disease (CD). Tight monitoring of disease activity is essential throughout the course of the disease to guide therapeutic decisions and assess response to therapy and relapse (1,2). Although endoscopic mucosal healing is a long-term goal of therapy, endoscopic evaluation may not always be feasible because of lack of immediate availability, cost, need for bowel preparation, relatively poor patient acceptance, and complications. Less invasive markers of disease activity are therefore needed.
Key immune processes involved in the pathogenesis of IBD include cytokine production by activated dendritic cells and macrophages, and the development of effector T lymphocyte subsets (3). Targeting dysfunctional immune cells and their products has led to the development of new therapies that have benefited patients (3). Similarly, a noninvasive method that targets dysfunctional immune cells, distinguishing between active cell subsets and quiescent cell populations, may allow specific assessment of disease activity, rather than relying on nonspecific indicators of disease activity (4).
System xC− plays an important role in the regulation of the innate and adaptive immune systems (5) and is upregulated in activated macrophages (6,7). On antigen stimulation, proliferating T cells require sufficient glutathione levels to ensure proper reactive oxygen species balance, resulting in the induction of high levels of xCT for cystine uptake (8,9). An ex vivo study on patients with IBD has shown that intestinal lamina propria macrophages expressed xCT, which resulted in high glutathione levels and full T-cell receptor reactivity (10). All these results suggest that system xC− could be a specific indicator of disease activity in IBD. Research designed to characterize the functional relevance of system xC− in disease states with oxidative stress and inflammation might pave the way for diagnosing and treating IBD (5).
(4S)-4-(3-18F-fluoropropyl)-l-glutamate (18F-FSPG) is a 18F-labeled l-glutamate derivative that is specifically taken up by system xC− (11). An exploratory clinical study has shown that 18F-FSPG PET can detect inflammation of the lungs and sarcoidosis (12). The low background uptake of 18F-FSPG would be especially advantageous in detecting inflammatory lesions in the intestine (12,13), an organ in which the use of conventional 18F-FDG imaging may be limited because of physiologic uptake. 18F-FDG PET may also be limited in differentiating mildly active IBD from endoscopic remission (14,15), showing an adequate accuracy only for detecting moderate-to-severe endoscopic disease (16,17). The objective of this study was to evaluate whether the in vivo assessment of system xC− in immune cells provides information on the dysregulated immune responses responsible for chronic active inflammation in IBD, thereby assessing the disease activity. We first conducted animal experiments to investigate whether 18F-FSPG would have increased accumulation associated with xCT expression in immune cells. Second, we aimed to explore the diagnostic validity of 18F-FSPG PET/CT in patients. Finally, we assessed the association of 18F-FSPG uptake and xCT expression in immune cells with endoscopic markers.
MATERIALS AND METHODS
Experimental IBD Models, 18F-FSPG PET Imaging, and Ex Vivo Analysis
The research protocol was approved by the Institutional Animal Care and Use Committee (registration numbers 2016-12-153 and 2017-12-017). All animal experiments conformed to the institutional guidelines. Experimental details are reported in accordance with the ARRIVE guidelines, version 2.0 (Animal Research: Reporting of In Vivo Experiments). Dextran sulfate sodium (DSS)–induced and adoptive T-cell transfer–induced IBD models were evaluated. Details of clinical disease activity, ex vivo analysis, and immunohistochemical staining for expression of xCT and cell surface markers are provided in the supplemental methods (supplemental materials are available at http://jnm.snmjournals.org).
Clinical Study Design and Patients
This was a prospective, nonrandomized, single-center cohort study. The study protocol, provided in the supplemental materials, was approved by the Ministry of Food and Drug Safety of the Republic of Korea and the institutional review board of Asan Medical Center (approval 2018-0262). This trial was conducted in accordance with the Declaration of Helsinki and institutional guidelines. All patients provided written informed consent before participation. The primary objective was to explore the validity of 18F-FSPG PET/CT for the diagnosis of patients with active IBD. The secondary objectives were to explore the validity of 18F-FSPG PET/CT for detecting bowel segments with active IBD; to assess the correlation of 18F-FSPG activity with clinical, endoscopic, and biologic markers of disease activity; to assess the interreader variability of visual 18F-FSPG PET/CT interpretation, and to evaluate the safety of 18F-FSPG PET/CT. Intended enrollment included 10 patients with UC and 10 with CD, numbers regarded as sufficient to obtain PET/CT imaging information while avoiding unnecessary exposure to ionizing radiation. The trial was registered at http://clinicaltrials.gov as NCT03546868.
Patients eligible for inclusion were consecutive adults aged between 19 and 79 y who had UC or CD, as diagnosed clinically, endoscopically, and histologically. The complete inclusion and exclusion criteria are listed in the supplemental methods. All cases were identified on the basis of presenting symptoms, as evaluated by 3 of the authors at the Department of Gastroenterology.
18F-FSPG PET/CT Imaging of Patients
Patients were asked to fast for at least 4 h before being administered 18F-FSPG (8 h if they were on a high-protein diet). A dose of 200 ± 20 MBq of 18F-FSPG was administered as a slow intravenous bolus injection for up to 60 s. Sixty minutes later, PET/CT was performed from the abdomen to the pelvis, with an acquisition time of 3 min per bed position, using a PET/CT scanner (Discovery PET/CT 690; GE Healthcare). The total radiation exposure from the CT examination did not exceed 1 mSv. Hyoscine butylbromide was administered intravenously before or during the PET/CT to reduce peristaltic movement. The safety assessment of 18F-FSPG is provided in the supplemental methods.
Images were interpreted independently by 2 board-certified nuclear medicine physicians who were masked to clinical and endoscopic data. 18F-FSPG intensity moderately higher than in the liver was considered positive for active disease. The SUVmax of each bowel segment was also determined, with the summed SUVmax being the sum of all segments. Disagreements between the 2 physicians were resolved by consensus. Details are provided in the supplemental methods (12,13).
Assessment of Disease Activity
Endoscopic assessment was considered a valid reference standard for disease activity and extent. Sigmoidoscopy or colonoscopy was performed by an experienced gastroenterologist masked to 18F-FSPG PET/CT results. The severity and extent of inflammatory lesions were evaluated using the UC Endoscopic Index of Severity (UCEIS) in UC patients and the CD Endoscopic Index of Severity (CDEIS) in CD patients (18). Segmental scores were determined in 5 bowel segments per patient using the UCEIS or CDEIS. For segmental CDEIS, the score for ulcerated or nonulcerated stenosis was imputed to the affected segment. Endoscopic evidence of active UC was defined as a UCEIS score of at least 2, whereas endoscopic evidence of active CD was defined as a CDEIS score of at least 3. Bowel segments with a superficial or deep ulcer were considered severe disease. Clinical and pathologic assessment are summarized as the supplemental methods (18).
Immunohistochemical Staining of Human xCT, GLUT1, and Cell Surface Markers
The immunohistochemistry study was approved by the institutional review board of Asan Medical Center (approval 2019-0260). Written informed consent was obtained again from all participants. The details are summarized in the supplemental methods (19) and Supplemental Table 1.
Statistical Analysis
The sensitivity of 18F-FSPG PET/CT for the diagnosis of endoscopic evidence of active disease was calculated as the probability of positive 18F-FSPG uptake in patients with active disease, as defined by the UCEIS or CDEIS. Specificity was defined as the probability of negative 18F-FSPG uptake when the disease was not present. Bowel segment–level sensitivity and specificity were determined according to segmental UCEIS and CDEIS scores. Bowel segments that were not assessed by endoscopy were excluded from the analysis. The details are provided in the supplemental methods.
RESULTS
In Vivo Animal Studies
Twelve of 15 DSS-treated mice and 11 of 15 mice that underwent adoptive T-cell transfer met the eligibility criteria and completed the study. The control groups consisted of 6 and 10 mice, respectively. Clinical disease activity of DSS-treated mice on day 7 (median, 1.8; range, 0.7–3.3) and T-cell–transferred mice 8–12 wk after transfer (median, 2.5; range, 1.0–4.0) was significantly higher than that of their respective control groups (P < 0.001; Supplemental Fig. 1).
In DSS-treated mice, an increased 18F-FSPG uptake in the colon was observed (Fig. 1). The SUVmax of 18F-FSPG was significantly higher in the colons of DSS-treated than control mice (median, 2.1 [range, 0.5–3.9] vs. 0.7 [range, 0.5–1.9]; P = 0.018), as was the pathologic score derived from colon tissue (median, 14.2 [range, 5.8–32.0] vs. 1.5 [range, 0–2.8]; P < 0.001). The SUVmax of 18F-FSPG uptake was positively associated with clinical disease activity (ρ = 0.57, P = 0.014) and pathologic scores (ρ = 0.65, P = 0.004; Fig. 1; Supplemental Fig. 2).

18F-FSPG imaging in DSS-treated mice. (A) Representative transaxial, coronal, and sagittal 18F-FSPG PET/MR images of murine DSS-induced IBD model. Arrows indicate positive 18F-FSPG uptake along colon. (B and C) Associations of colonic SUVmax with clinical disease activity (B) and pathologic score (C). Bl = bladder.
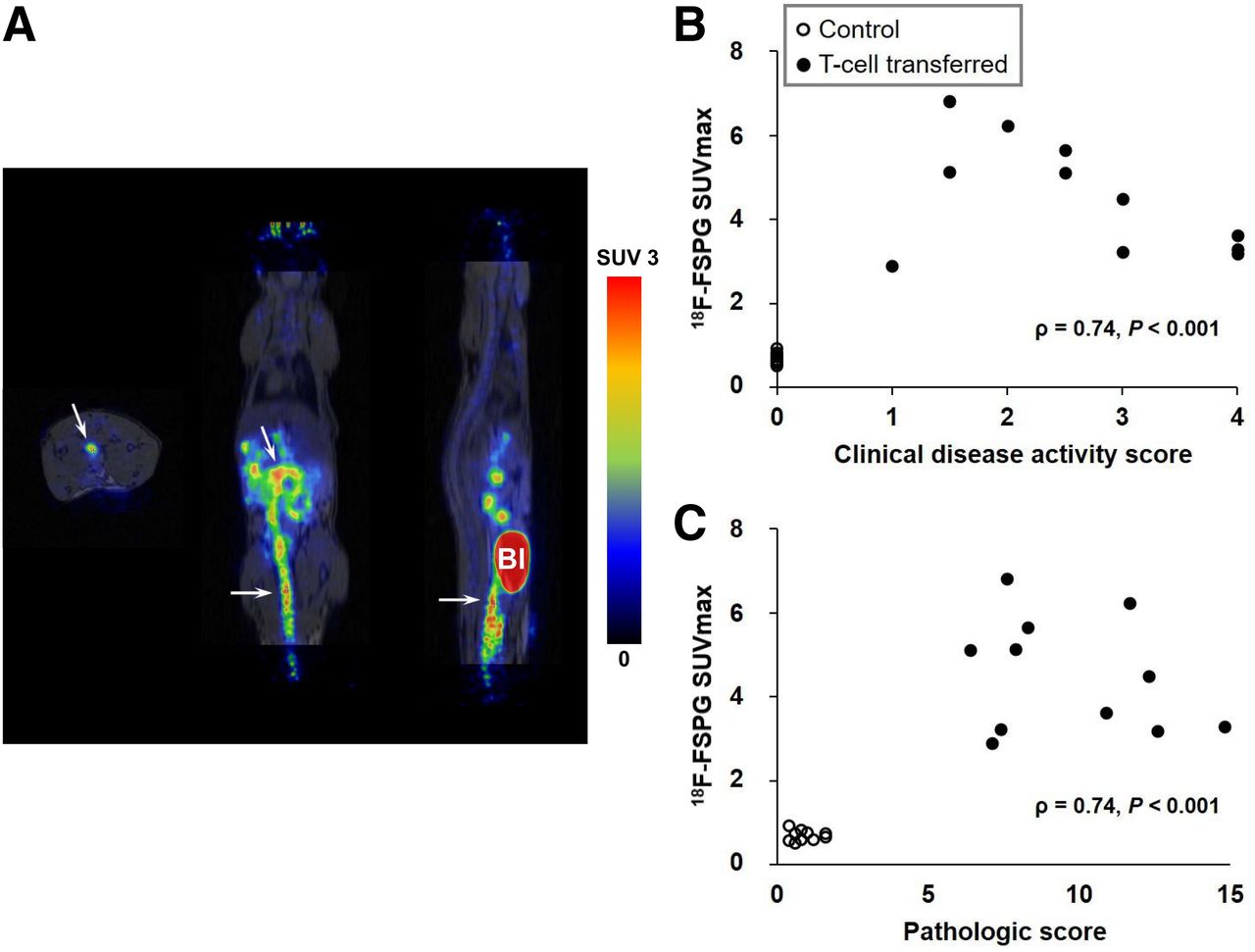
Similarly, the SUVmax of colonic 18F-FSPG uptake (median, 4.5 [range, 2.9–6.8] vs. 0.7 [range, 0.5–0.9]; P < 0.001) and the pathologic score derived from colon tissue (median, 8.3 [range, 6.4–14.8] vs. 0.8 [range, 0.4–1.6]; P < 0.001) were significantly higher in T-cell–transferred than in control mice (Fig. 2). The SUVmax of 18F-FSPG uptake showed positive associations with clinical disease activity (ρ = 0.74, P < 0.001) and pathologic scores (ρ = 0.74, P < 0.001; Fig. 2; Supplemental Fig. 3).

18F-FSPG imaging in T-cell–transferred mice. (A) Representative transaxial, coronal, and sagittal 18F-FSPG PET/MR images of T-cell transfer–induced IBD model. Arrows indicate increased 18F-FSPG uptake in colon. (B and C) Associations of colonic SUVmax with clinical disease activity (B) and pathologic score (C). Bl = bladder.
Immunohistochemical staining of colon tissues revealed that xCT and GLUT1 were highly expressed in dendritic cells positive (+) for CD11c, in F4/80+ macrophages, and in CD3+ T cells in the lamina propria from mice with experimental colitis (Supplemental Fig. 4). In addition, immunohistochemical staining showed that xCT and GLUT1 were expressed in the epithelial cells of normal and inflamed mucosa.
Patients and 18F-FSPG PET/CT Procedure
Between August 2018 and January 2019, 23 patients with IBD were assessed for initial eligibility and invited to participate in this prospective study. Three patients withdrew their consent before the injection of 18F-FSPG. Finally, 10 patients with UC and 10 with CD were enrolled. All 20 patients completed 18F-FSPG PET/CT as planned. The median administered activity per patient was 199.8 MBq (range, 192.4–214.6 MBq), and the median administered mass dose was 0.82 μg (range, 0.21–1.86 μg). Nineteen patients underwent colonoscopy, and 1 underwent sigmoidoscopy 1 d after 18F-FSPG PET/CT. The demographic and baseline clinical characteristics are listed in Table 1. Six patients with UC (60%) and 8 with CD (80%) showed endoscopic evidence of active disease. Twelve (26%) of 47 bowel segments in patients with UC and 24 (59%) of 41 segments in patients with CD showed active inflammatory lesions.
Demographic and Clinical Characteristics
18F-FSPG Uptake in Patients
Readers determined that overall image quality was adequate for interpretation in all patients. The interreader agreements of visual assessment of 18F-FSPG accumulation had κ-values of 0.70 (95% CI, 0.49–0.92) for patient-level analysis and 0.65 (95% CI, 0.57–0.73) for bowel segment–level analysis. Two readers disagreed on the presence of 18F-FSPG accumulation in 2 (10%) of 20 patients and 10 (11%) of 95 bowels segments.
18F-FSPG PET/CT was positive in 4 (67%) of the 6 UC patients with endoscopically active inflammation (Fig. 3) and correctly diagnosed endoscopic remission in 2 (50%) of the 4 patients (Supplemental Table 2). The 2 false-negative patients had scores of 3 (Supplemental Fig. 5), and the 2 false-positives had scores of 4 (Supplemental Fig. 6). The sensitivity and specificity of 18F-FSPG PET/CT in identifying active bowel segments were 75% (9/12) and 86% (30/35), respectively. All patients (n = 2) and bowel segments (n = 5) with superficial or deep ulcers were correctly identified.
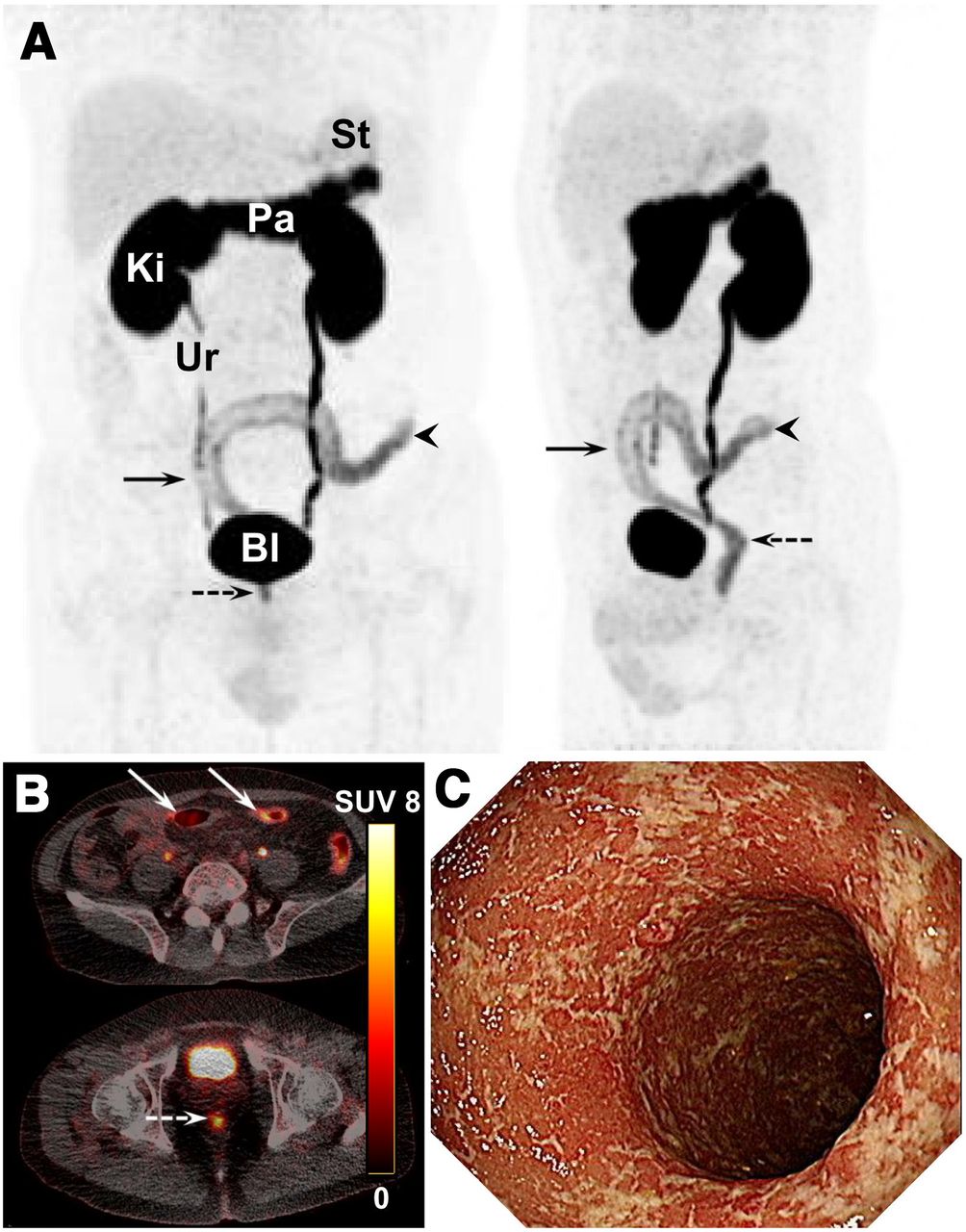
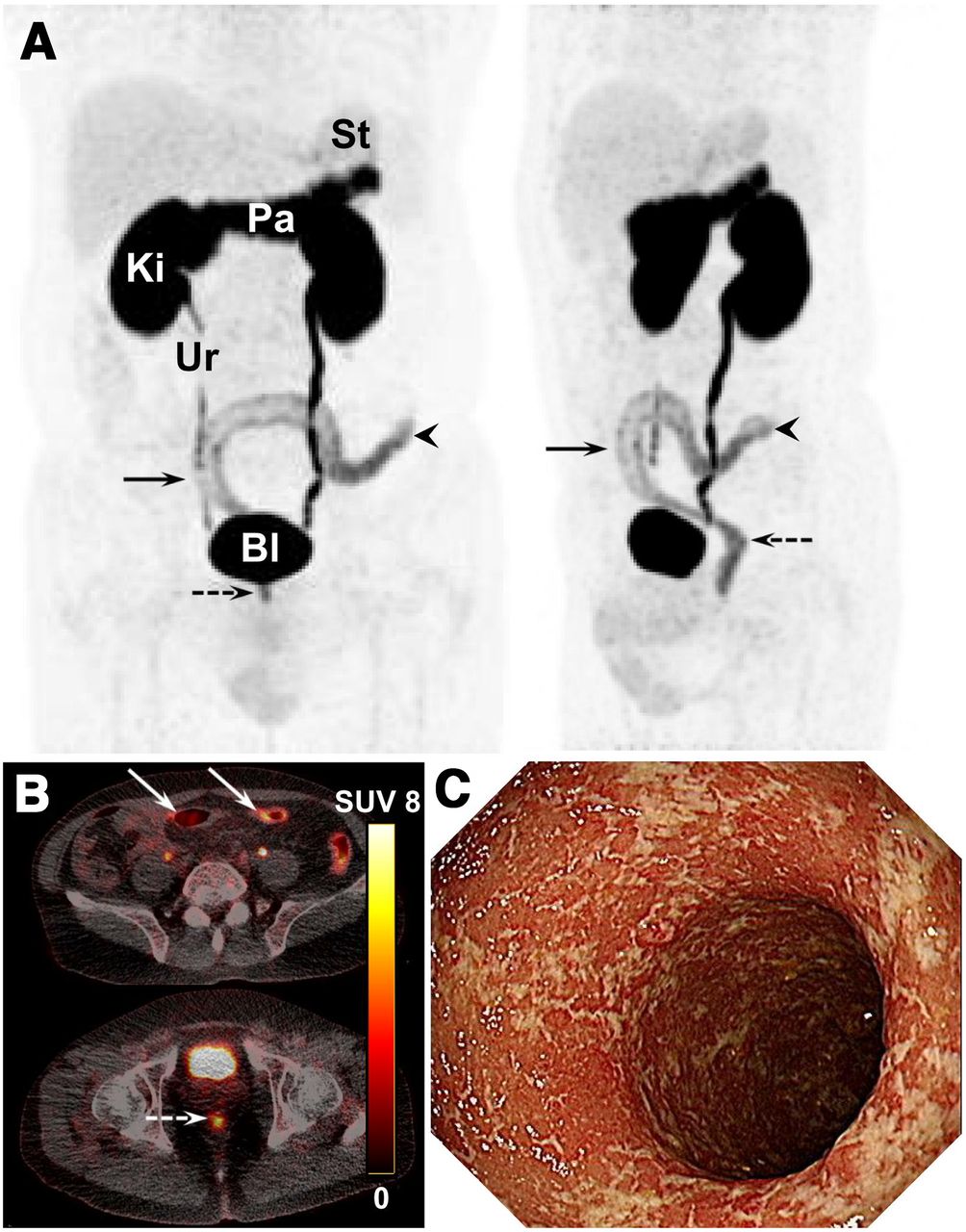
18F-FSPG PET/CT and endoscopic images of 55-y-old man with UC who presented with increased stool frequency, loose stools, hematochezia, and mild leukocytosis. His partial Mayo score was 4. (A and B) Maximum-intensity projection (A) and axial 18F-FSPG (B) PET show increased 18F-FSPG uptake along distal descending colon (arrowheads), sigmoid colon (arrows), and rectum (dashed arrows), with endoscopically active inflammation. (C) Endoscopic image of descending colon. Segmental UCEIS of ascending and transverse colon was 0, and that of descending colon, sigmoid colon, and rectum was 5. St = stomach; Pa = pancreas; Ki = kidneys; Ur = ureter; Bl = bladder.
All 8 CD patients with active inflammation (Fig. 4) and 2 with endoscopic remission were correctly diagnosed by 18F-FSPG PET/CT (Supplemental Table 3). In a segment-based analysis, 18F-FSPG PET/CT had a sensitivity of 71% (17/24) and a specificity of 94% (16/17), respectively. All 7 patients and 16 of 20 segments with superficial or deep ulcerations were correctly diagnosed.

18F-FSPG PET/CT and endoscopic images of 26-y-old woman with CD who presented with abdominal pain and elevated C-reactive protein. Her CDAI was 102.47. (A and B) Maximum-intensity projection (A) and axial 18F-FSPG (B) PET show increased 18F-FSPG uptake in ileum (arrows), sigmoid and descending colon (arrowheads), and rectum (dashed arrows), which correlated well with endoscopic findings. Segmental CDEIS scores were 12 for ascending colon, 0 for transverse colon, 24 for descending and sigmoid colon, and 23 for rectum. Ileum was not assessed by colonoscopy. (C) Endoscopic image of rectum shows geographic and superficial ulcers, exudates, and streaks of coagulated blood. St = stomach; Pa = pancreas; Ki = kidneys; Ur = ureter; Bl = bladder.
Association Between 18F-FSPG Uptake and Disease Activity
In patients with UC, the median SUVmax was 3.1 (range, 1.8–8.2). The summed SUVmax was strongly associated with the UCEIS (ρ = 0.79, P = 0.006) but not with the partial Mayo score, C-reactive protein, and fecal calprotectin (Supplemental Fig. 7). The segmental SUVmax (median, 2.2; range, 0.8–8.2) also showed strong associations with UCEIS (n = 47, ρ = 0.66; P < 0.001) and the Robarts Histopathology Index (n = 23, ρ = 0.64; P = 0.001).
The median SUVmax in patients with CD was 5.6 (range, 2.8–7.6). The summed SUVmax was strongly associated with the Crohn’s Disease Activity Index (CDAI), C-reactive protein, fecal calprotectin, and the CDEIS (Supplemental Fig. 8). The segmental SUVmax (median, 2.9; range, 1.5–7.6) also showed a strong association with CDEIS (n = 41, ρ = 0.61; P < 0.001) but not with the Colonic and Ileal Global Histologic Disease Activity Score (n = 7, ρ = 0.33; P = 0.47).
Safety of 18F-FSPG PET/CT
No adverse events were observed in patients with UC. However, 4 patients (40%) with CD had adverse events with mild intensity, including diarrhea, upper respiratory infection, arthritis, and dizziness. No adverse events were related to the study drug, and none of the patients experienced any serious adverse events or any clinically relevant changes in safety parameters.
Association Between xCT Expression and Disease Activity
Immunohistochemical staining showed that CD68+, CD3+, or CD66b+ cells were present in the lamina propria of intestinal mucosa affected by UC (Supplemental Fig. 9) or CD (Supplemental Fig. 10). In addition, xCT was found to be expressed in the inflammatory and epithelial cells of all bowel segments. In patients with UC, the numbers of CD68+xCT+, CD3+xCT+, and CD66b+xCT-negative cells in 22 bowel segments showed positive associations with UCEIS and SUVmax (Supplemental Table 4). By contrast, cytokeratin+xCT+ was negatively associated with UCEIS and SUV. In patients with CD, only the number of CD68+xCT+ cells in 7 bowel segments showed a significant association with CDEIS (Supplemental Table 5). Other cell populations showed no association with CDEIS or SUV.
DISCUSSION
Using mice with experimental IBD, we found that 18F-FSPG accumulation in the colon was associated with disease activity indices and xCT expression in immune cells. Expansion of this study to patients, most of whom were clinically in remission or had mildly active IBD, showed that 18F-FSPG PET/CT was accurate in diagnosing endoscopically active IBD and remission in patients and bowel segments. All patients with superficial or deep ulcers were correctly identified. Quantitative 18F-FSPG uptake and xCT expression in immune cells were associated with endoscopic disease activity indices. 18F-FSPG PET/CT was well tolerated, with no study drug–related adverse events. Our results suggest that 18F-FSPG PET/CT can assess disease activity and distinguish between active IBD and mucosal healing, as determined endoscopically.
Although this study did not include participants across the entire range of disease activity, the subjects of this study may constitute a representative sample of those who would likely be the intended-use population for 18F-FSPG PET/CT. All patients were evaluated by endoscopy after 18F-FSPG PET/CT, with masked readers interpreting 18F-FSPG PET/CT. Thus, there are no potential risks of bias or applicability regarding the accuracy of data. False-positives and false-negatives were likely due to an indeterminate zone for decision making. Greater experience with refined classification criteria may reduce the likelihood of patient misclassification. The positive association between quantitative 18F-FSPG uptake and endoscopic assessment further supports the validity of 18F-FSPG PET/CT. In patients with UC, the absence of a significant association between 18F-FSPG uptake and conventional markers may be due to the inclusion of patients with mildly active disease and the small study sample.
We found that endoscopic assessment was positively associated with xCT expression by CD68+ and CD3+ immune cells in patients with UC and with xCT expression by CD68+ cells in CD but not with xCT+CD66b+ cells. Although the small number of assessed bowel segments with CD may have precluded a consistent association, these results confirm the role of CD68+xCT+ macrophages in the antioxidative microenvironment of IBD (10). Our results also demonstrate that xCT expression is upregulated in human CD3+ T cells, further strengthening the evidence for xCT expression and cystine uptake as regulators of T-cell function. These findings are consistent with results showing high initial rates of cystine and 18F-FSPG uptake followed by decreases during a later phase of inflammation (6,11,12). xCT expression and cystine uptake in immune cells might mirror cellular concentrations of reactive oxygen species as well as metabolic activity (20). Taken together, these findings suggest that in vivo 18F-FSPG PET/CT results may indicate broad changes in immune metabolism. Understanding of xCT in immune cells may also provide a pathologic tool to assess IBD activity.
Interestingly, the endoscopic assessment was negatively associated with xCT expression by cytokeratin+ cells in patients with UC. xCT was expressed on the apical surfaces of the epithelial cells (Supplemental Figs. 9 and 10), where absorption occurs (10,21). This localization to absorptive sites suggests that system xC− plays a role in intestinal cystine transport (21) but does not involve 18F-FSPG transport into the epithelial cells. The reason for the lack of association between GLUT1+ immune cells and endoscopic assessment is not apparent but may be related to the persistent glucose hypermetabolism in healing tissue after inflammation (22,23).
Radiation exposure is an important limitation in using 18F-FSPG PET/CT to assess disease activity, mainly because most of these patients are relatively young. Current guidelines recommend using cross-sectional imaging modalities that do not entail exposure to ionizing radiation when it is likely that serial examinations are required (1). A per-patient dose of 200 MBq of 18F-FSPG would result in a mean effective dose of 4.0 ± 0.2 mSv, including the dose from CT (24). These doses can be significantly reduced using highly sensitive PET/CT systems (25). Study protocols that allow a low dose of 18F-FSPG can reduce the radiation dose by as much as 75% without clinical detriment (26).
This study had several limitations. First, the diagnostic validity should be interpreted with caution because of the small number of included patients and the exploratory nature of the study. Additional studies on larger numbers of patients are required to validate our initial results. Second, the assessment of IBD activity was based on endoscopic findings. Thus, comparisons between endoscopy and 18F-FSPG PET/CT may be limited because the actual sites of endoscopic evaluation may not precisely match those of 18F-FSPG uptake, thereby underestimating the accuracy of 18F-FSPG PET/CT for evaluating bowel segments.
CONCLUSION
18F-FSPG PET/CT imaging of system xC− in immune cells can noninvasively assess IBD activity and remission of the entire bowel without the need for bowel preparation and safety issues related to invasive endoscopic procedures. Assessment of system xC− expression by immune cells may provide diagnostic information on the dysregulated immune responses responsible for chronic active inflammation.
DISCLOSURE
This research was sponsored by the Asan Foundation (Seoul, Republic of Korea) and financially supported by National Research Foundation grants NRF-2016M2A2A7A03913219 and NRF-2019R1A2C209022213 funded by the Korea Ministry of Science and ICT, Republic of Korea, and by the Korea Health Technology R&D Project through the Korea Health Industry Development Institute, funded by the Ministry of Health and Welfare, Republic of Korea (grant HI18C2383). The funders had no role in the conceptualization or design of the study; in the collection, analysis, and interpretation of the data; in the writing of the manuscript; or in the decision to submit the manuscript for publication. Norman Koglin and Andrew Stephens report personal fees from Life Molecular Imaging GmbH (employment) during the conduct of the study and are listed as coinventors on a patent application entitled “[F-18]-labeled L-glutamic acid and L-glutamine derivatives (I), their use and processes for their preparation; US 9,308,282”, which is owned by Life Molecular Imaging. Dae Hyuk Moon reports receiving grants from the National Research Foundation of Korea, the Korea Health Industry Development Institute, and Life Molecular Imaging GmbH. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Does in vivo assessment of system xC− in immune cells provide information on the dysregulated immune responses responsible for chronic active inflammation in IBD, thereby assessing the disease activity?
PERTINENT FINDINGS: System xC− expression in immune cells was associated with endoscopic disease activity indices. PET imaging of system xC− was accurate in diagnosing endoscopically active disease and remission in patients and bowel segments.
IMPLICATIONS FOR PATIENT CARE: PET imaging of system xC− may noninvasively assess disease activity and remission without the need for bowel preparation or the safety issues related to endoscopic procedures.
Footnotes
Published online Jan. 27, 2022.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 6, 2021.
- Accepted for publication January 18, 2022.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}