


Abstract
Congenital hyperinsulinism is characterized by persistent hypoglycemia due to inappropriate excess secretion of insulin resulting in hyperinsulinemic hypoglycemia. The clinical course varies from mild to severe, with a significant risk for brain damage. Imaging plays a valuable role in the care of infants and children with severe hypoglycemia unresponsive to medical therapy. 18F-6-fluoro-l-dopa PET/CT is the method of choice for the detection and localization of a focal lesion of hyperinsulinism. Surgical resection of a focal lesion can lead to a cure with limited pancreatectomy. This article reviews the role of 18F-6-fluoro-l-dopa PET/CT in the management of this vulnerable population.
Congenital hyperinsulinism (HI) is a rare, life-threatening disease with heterogeneity in clinical presentation, genetic mutations, and histopathology. The estimated frequency of the disease varies by population, with an estimate of 1 in 50,000 live births leading to an estimated incidence of 80 per year in the United States (1). In consanguineous populations, the frequency is as high as 1 in 2,500 (2). Evaluation of hypoglycemia by an experienced endocrinologist is essential for the identification of children who may have a focal lesion that can be cured surgically with limited partial pancreatectomy. Clinical subgroups can be divided into transient perinatal stress, monogenic HI, and syndromic HI. Once transient HI is excluded, the evaluation of the latter subcategories should focus on clinical evaluation and genetic analysis. The main histologic entities found in HI include focal adenomatous islet cell hyperplasia and diffuse β-cell nucleomegaly (3,4). Atypical lesions are found in a small subset of patients.
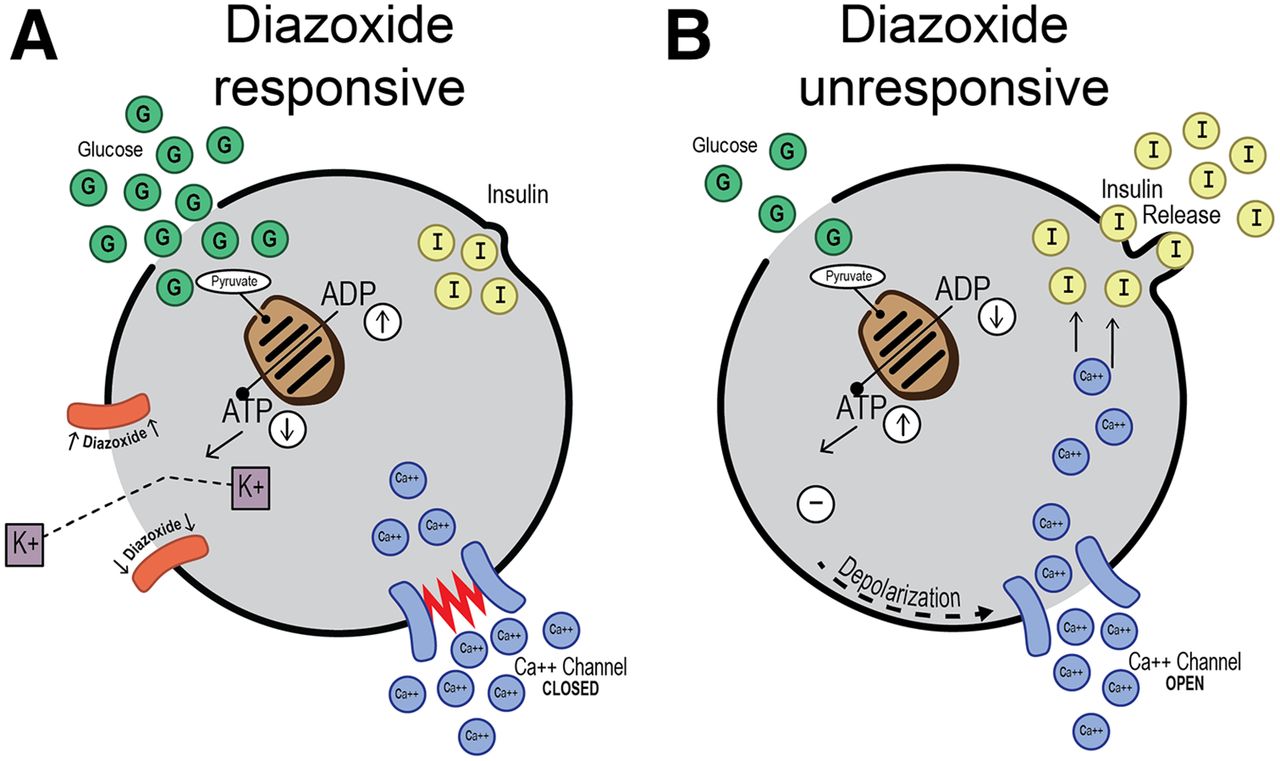
Genetic analysis has emerged as a valuable tool for the selection of patients who have severe hypoglycemia unresponsive to therapy and who can benefit from imaging with 18F-6-fluoro-l-dopa (18F-FDOPA). A genetic mutation is found in approximately 50% of cases of HI, with defects in the encoding genes of the B-cell adenosine triphosphate–sensitive potassium (KATP) channel to be most common in both focal and diffuse diseases (5). The KATP channel is composed of 4 sulfonylurea receptor 1 protein subunits encoded by the gene ABCC8 and 4 inward-rectifier potassium channel protein subunits encoded by the gene KCNJ11. The absence of normal KATP function resulting in unregulated insulin release can be identified by showing a lack of or a poor response to diazoxide, a KATP channel agonist and the first-line medical therapy for HI in infants (Fig. 1). Both KATP channel genes are localized on chromosome 11p15.1. A single recessive mutation of either gene predicts focal HI with a sensitivity of 97% and a specificity of 91%. Confirmation of paternal inheritance increases the specificity to 93% (6). The proposed mechanism for the loss of heterozygosity is a 2-hit mechanism with paternal mutation in all tissues followed by a somatic loss of maternal 11p15, including the KATP genes and growth regulatory genes. The result is uncontrolled islet cell proliferation forming a focal lesion (7,8).
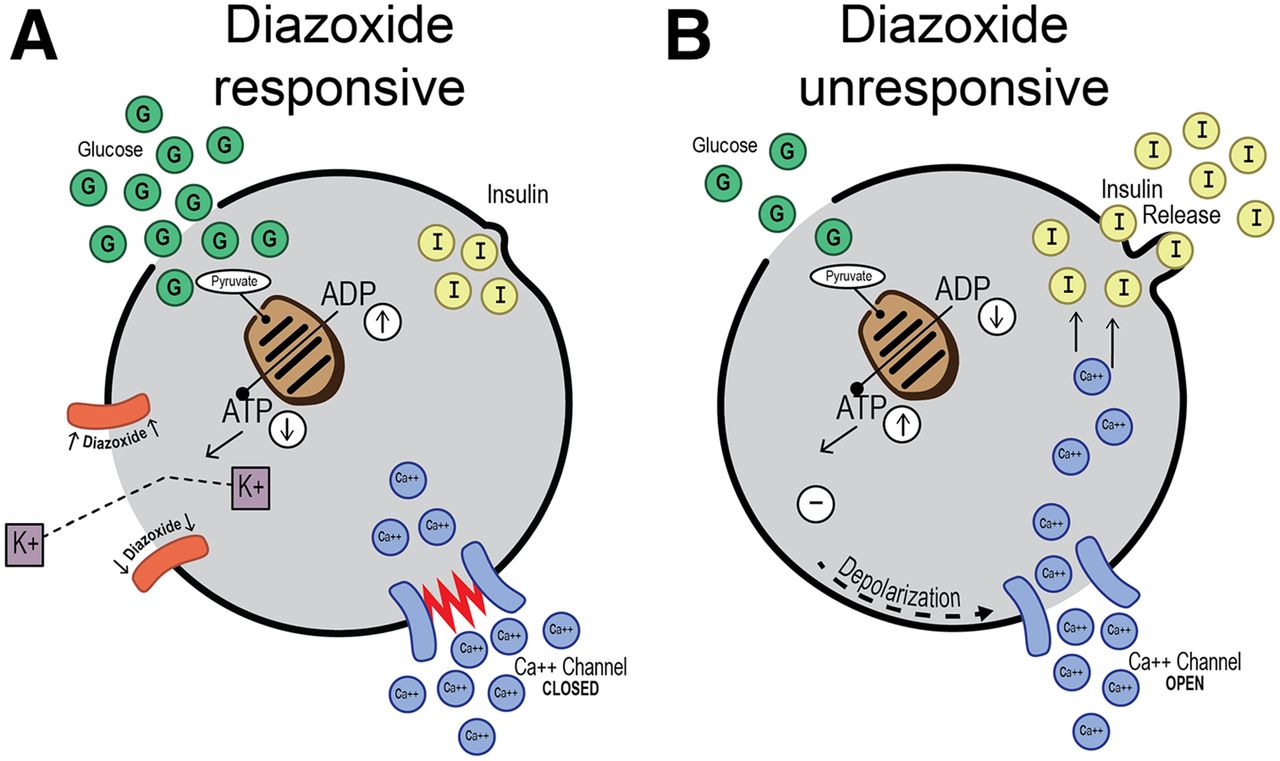
(A) Diazoxide-responsive β-cell with normal KATP channel (orange) shows diazoxide keeping channel open and causing hyperpolarization of membrane and inhibition of insulin release. (B) Diazoxide-unresponsive β-cell with failure of KATP channel assembly and tracking to plasma membrane because of ABCC8 or KCNJ11 mutation allows depolarization of membrane with opening of calcium channel causing influx of calcium and unregulated release of insulin. (Courtesy of Serene McLaughlin.)
PATIENT SELECTION
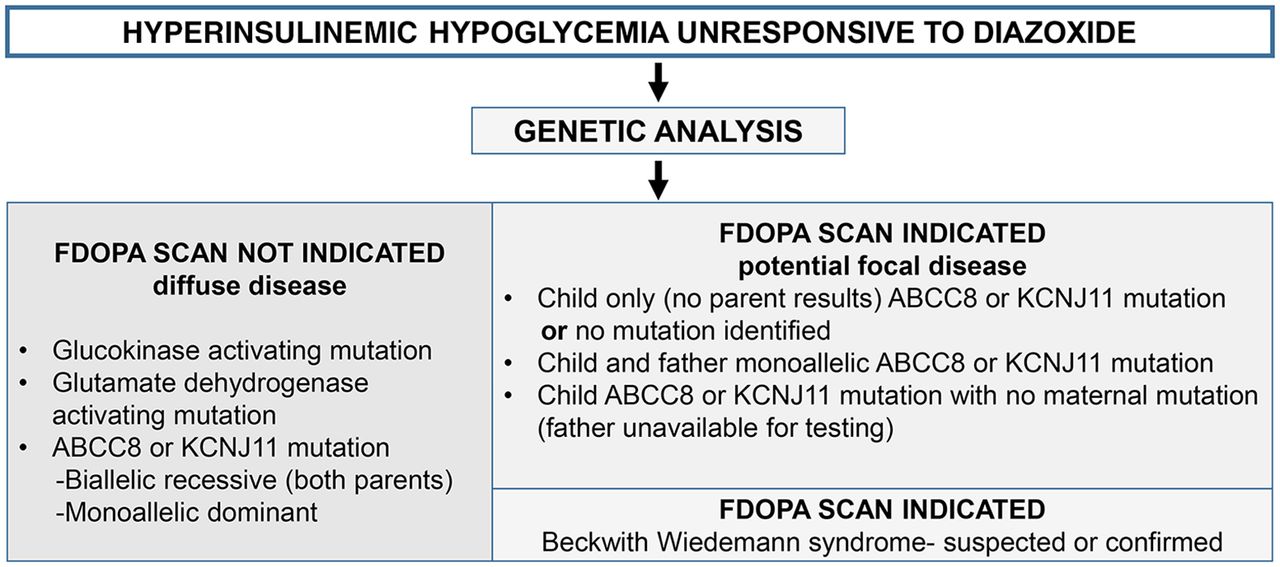
Guidelines for the management of congenital HI include 18F-FDOPA PET in a select group of patients. Once the diagnosis of HI is made, resistance to or the inability to tolerate diazoxide because of side effects is used to identify patients who can benefit from 18F-FDOPA imaging (9,10). The side effects of diazoxide include water and sodium retention, congestive heart failure, nausea, vomiting, and poor appetite (10). Genetic testing may predict the presence of a focal lesion, which can be further evaluated with 18F-FDOPA PET. The initial HI gene panel test includes evaluation for gene mutations in ABCC8 or KCNJ11, found in both focal and diffuse diseases, and gene mutations in GCK or GLUD 1, encoding the enzyme glucokinase or glutamate dehydrogenase, respectively, each a cause of diffuse disease. The finding of paternally inherited or nonmaternally inherited (if paternal results are not available) ABCC8 or KCNJ11 mutations or no identifiable mutations is an indication for imaging with 18F-FDOPA (Fig. 2). Genetic testing can prevent unnecessary scanning of infants with diffuse disease.

Indications for 18F-FDOPA PET/CT using genetic analysis.
18F-FDOPA MECHANISM AND HISTOPATHOLOGY
Localization of a focal lesion is the most important information that imaging can provide as it guides the surgical approach. 18F-FDOPA PET is more accurate in detecting and localizing a focal lesion and less invasive than arterial calcium stimulation with hepatic vein insulin sampling and transhepatic portal venous insulin sampling—both of which require hypoglycemia during blood sample collection (3,11).
The mechanism of uptake of 18F-FDOPA mirrors the metabolism of l-3,4-dihydroxyphenylalanine (l-DOPA), a large neutral amino acid precursor to neurotransmitters such as dopamine, norepinephrine, and epinephrine. The uptake of l-DOPA is seen in neuroendocrine cells, including pancreatic βη-cells. Once inside cells, l-DOPA is converted to l-dopamine by l-DOPA decarboxylase and is transported into vesicles for storage (12,13). 18F-FDOPA is similarly metabolized and trapped in vesicles, allowing imaging. Uptake in the islets of Langerhans in the pancreas peaks by 5 min after injection and remains fairly constant (14,15). Other sites of activity in the abdomen include the liver, gallbladder, kidneys, and bladder. Uptake may also be seen in pediatric growth plates.
Histopathologic analysis of surgical specimens requires an experienced pathologist for accurate diagnosis. A focal lesion is described as a cluster of abnormal β-cells, referred to as β-cell adenomatosis, and is histologically different from an insulinoma. Lesions consist of a localized area of endocrine islet cell proliferation within otherwise normal pancreatic lobules. The islet cells expand and often distort the involved lobules; however, ducts and exocrine (acinar) cells are observed within lesions. Lesions may have well-circumscribed borders or irregular borders with tentacles of tissue extending into normal tissue. The presence of tentacles can lead to incomplete resection. The histology of diffuse HI is characterized by an increased size of islet cell nuclei (nucleomegaly), measuring at least 3 times the size of neighboring endocrine cell nuclei and 4 times that of acinar cell nuclei, typically seen in islets throughout the pancreas without an overall increase in the volume of endocrine tissue (16–18). Localized islet cell nuclear enlargement is an atypical pathology with features of diffuse HI localized to a portion of the pancreas (6). There is no difference in the imaging characteristics of diffuse disease and those of localized islet cell nuclear enlargement (19).
Adzick et al. reported on 500 patients who had HI and who underwent surgery for clinical management (20). Approximately 246 of the 500 patients (49%) had focal disease, with most undergoing 2%–10% pancreatectomy and 97% being “cured.” Patients with diffuse disease most often underwent 98% pancreatectomy (20). Atypical disease was found in 37 of the 500 patients (∼7%) who underwent pancreatectomy and included 16 with localized islet cell nuclear enlargement and 21 with Beckwith-Wiedemann Syndrome (BWS) (20). Histopathology in BWS reveals pancreatic endocrine hyperplasia. 18F-FDOPA PET/CT findings may reveal pancreatic enlargement and uptake suggestive of a large lesion (21). Genetic analysis typically reveals a mosaic paternal uniparental isodisomy for chromosome 11p (UDP11p). Most patients do not have KATP channelopathy (22). Ectopic lesions with focal histopathology were seen in 1 of 415 18F-FDOPA PET scans performed in patients undergoing surgery at the Children’s Hospital of Philadelphia.
REVIEW OF LITERATURE
Review of the literature showed growing expertise and great success in the detection and localization of a focal lesion. The studies included in Table 1 were selected if patients underwent surgery and had histopathologic confirmation of focal or diffuse disease. The overall pooled sensitivity and specificity (Fig. 3) were both higher than 90%, with an accuracy of localization ranging from 92% to 100%.
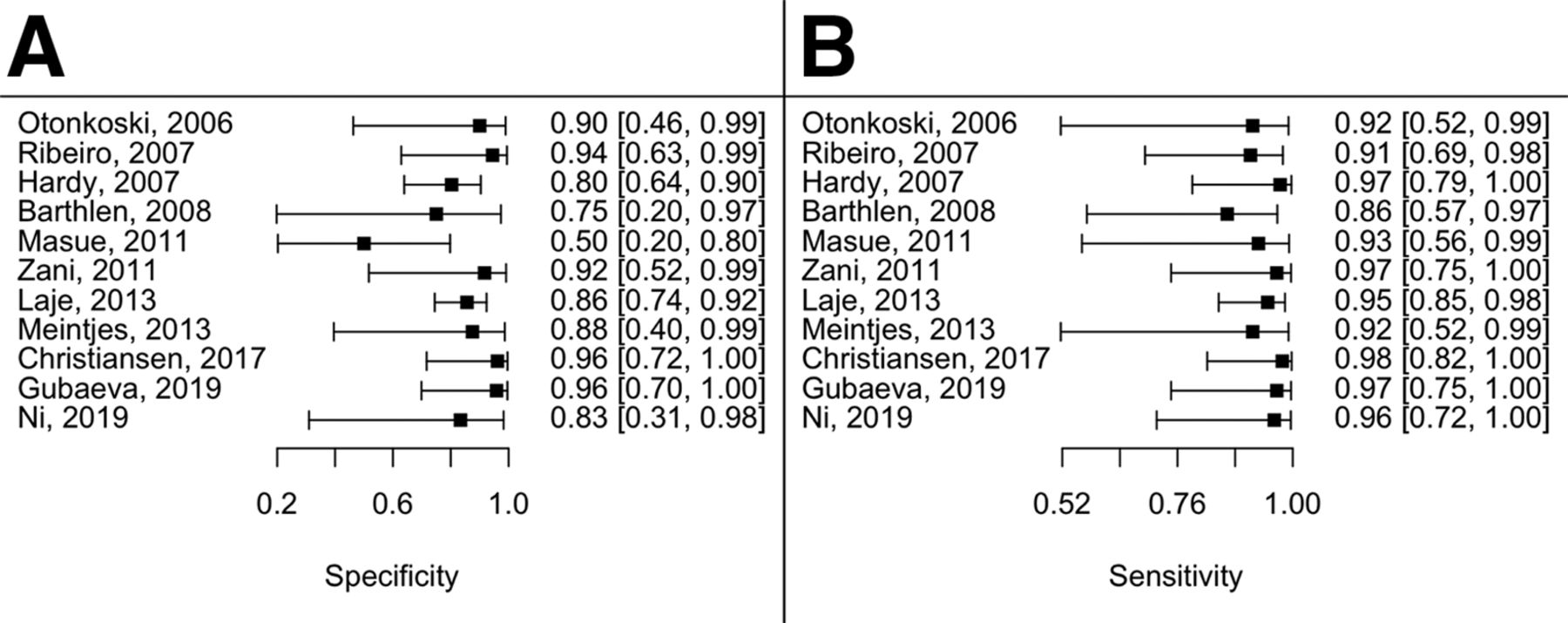
Specificity (A) and sensitivity (B) of 18F-FDOPA PET/CT for detection of focal lesions.
Publications with Surgical Histologic Confirmation of PET Results
PROTOCOL AND PREPARATION
In 2005, a standardized protocol guideline was created by survey to optimize image quality and minimize radiation (23). A sample protocol used at the Children’s Hospital of Philadelphia is depicted in Figure 4. Sedation or anesthesia is required for imaging. Nothing by mouth instructions depend on institution protocols. Withdrawal of glucagon 24 h before a scan has been recommended; however, in our experience at the Children’s Hospital of Philadelphia, we have not found it to interfere with uptake in the pancreas. Diazoxide and octreotide are not thought to interfere with uptake and may be continued if necessary. Infusion of glucose-containing fluids is necessary for continued maintenance of safe glucose levels during the scan. To avoid interruption of the glucose infusion, a separate intravenous line is required for tracer injection and iodinated contrast agent injection.
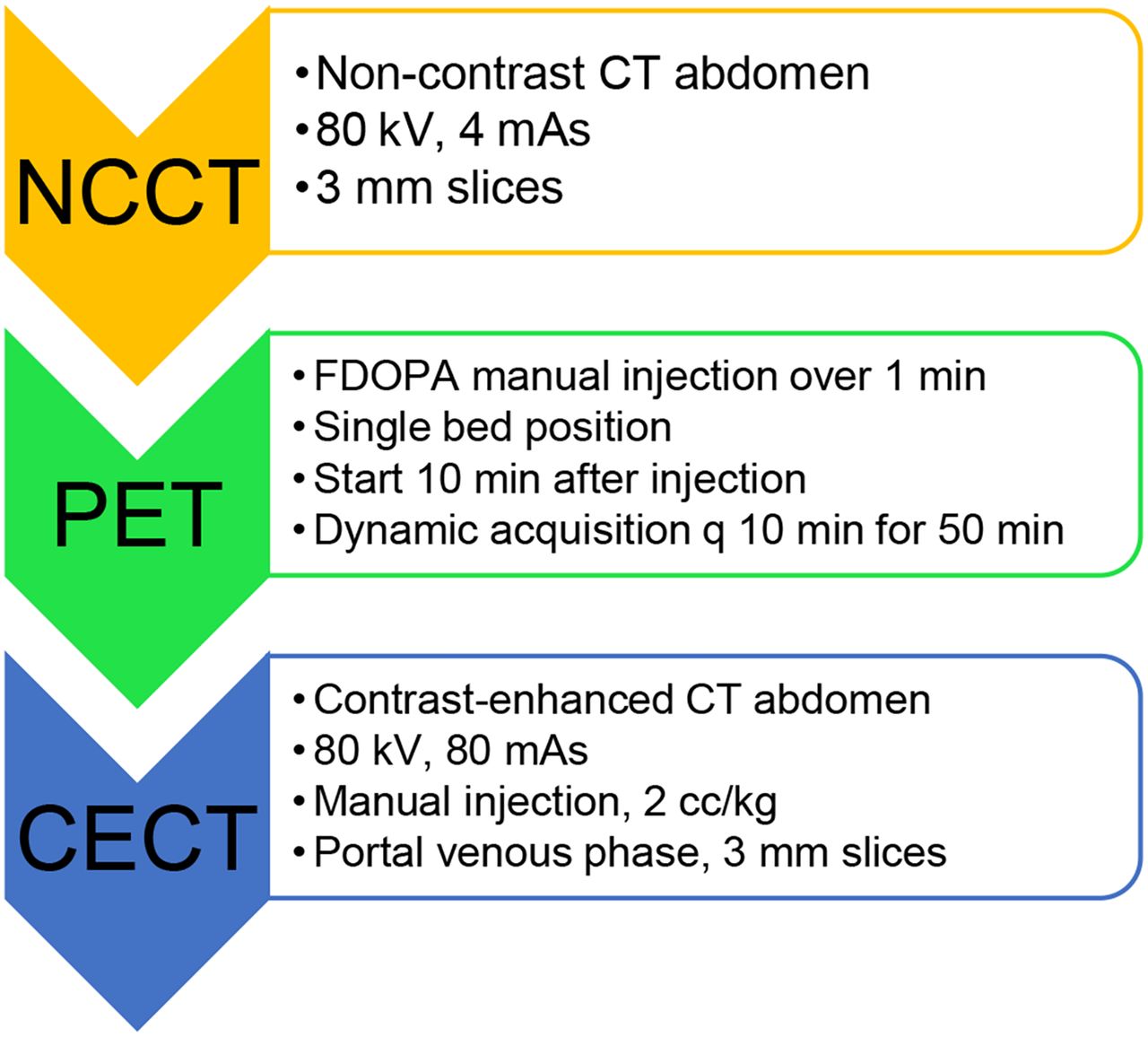
Sample imaging protocol. CECT = contrast-enhanced CT; NCCT = noncontrast CT.
Once the patient is sedated or anesthetized, imaging is performed at a single PET bed over the abdomen. The scout image will confirm appropriate withdrawal of the radiopaque tip of the feeding tube, if present, outside the region of the pancreas. A dose of 4 MBq/kg, suggested by Garg et al. (14), falls within the range of doses used in the publications in Table 1. After the injection of a radiotracer, a noncontrast low-dose CT scan is performed for attenuation correction. PET acquisition starts approximately 10 min after radiotracer injection, with subsequent 10-min sequential acquisitions, for a total of 50 min. Manual injection of contrast agent is used to minimize the risk of extravasation of contrast agent. A contrast-enhanced CT scan of the abdomen performed after the completion of the PET acquisition and fused with the PET data provides a map for surgical planning. A shortened protocol performed with dynamic imaging starting 10 min after injection and using 10-min acquisitions over 30 min can provide similar results. In the United States, all patients are required to sign a written informed consent form before enrollment in an institutional review board–approved protocol under a Food and Drug Administration Investigational New Drug application.
IMAGE INTERPRETATION
Imaging review starts with the attenuation-corrected maximum-intensity projection (MIP) of the entire 50 min of data followed by viewing of the sequentially acquired 10-min MIPs. The 50-min summed MIP is used for image fusion with both noncontrast images and contrast-enhanced images. The lesion is often best detected on the MIP images compared with the fused images and should be seen on more than one 10-min MIP image. Focal lesions typically appear as a focus of increased activity greater than the uptake seen in the normal pancreas (Fig. 5). An abnormal pancreatic contour on CT images can aid in the confirmation of a focal lesion (Supplemental Fig. 1) (supplemental materials are available at http://jnm.snmjournals.org). Early images will have the most renal cortical uptake, which can obscure a lesion in the tail. Images performed at 50 min or later may have excretion into the common bile duct, which can be mistaken for a focal lesion in the pancreatic head.

Focal disease. 3-mo-old female with diazoxide-unresponsive HI with ABCC8 mutation. 18F-FDOPA 3-dimensional MIP image at 50 min shows 2 focal lesions, 1 within head (arrow) and other at pancreatic body/tail junction (arrowhead). Lesions were excised with 10% pancreatectomy. Finding 2 lesions is rare occurrence.
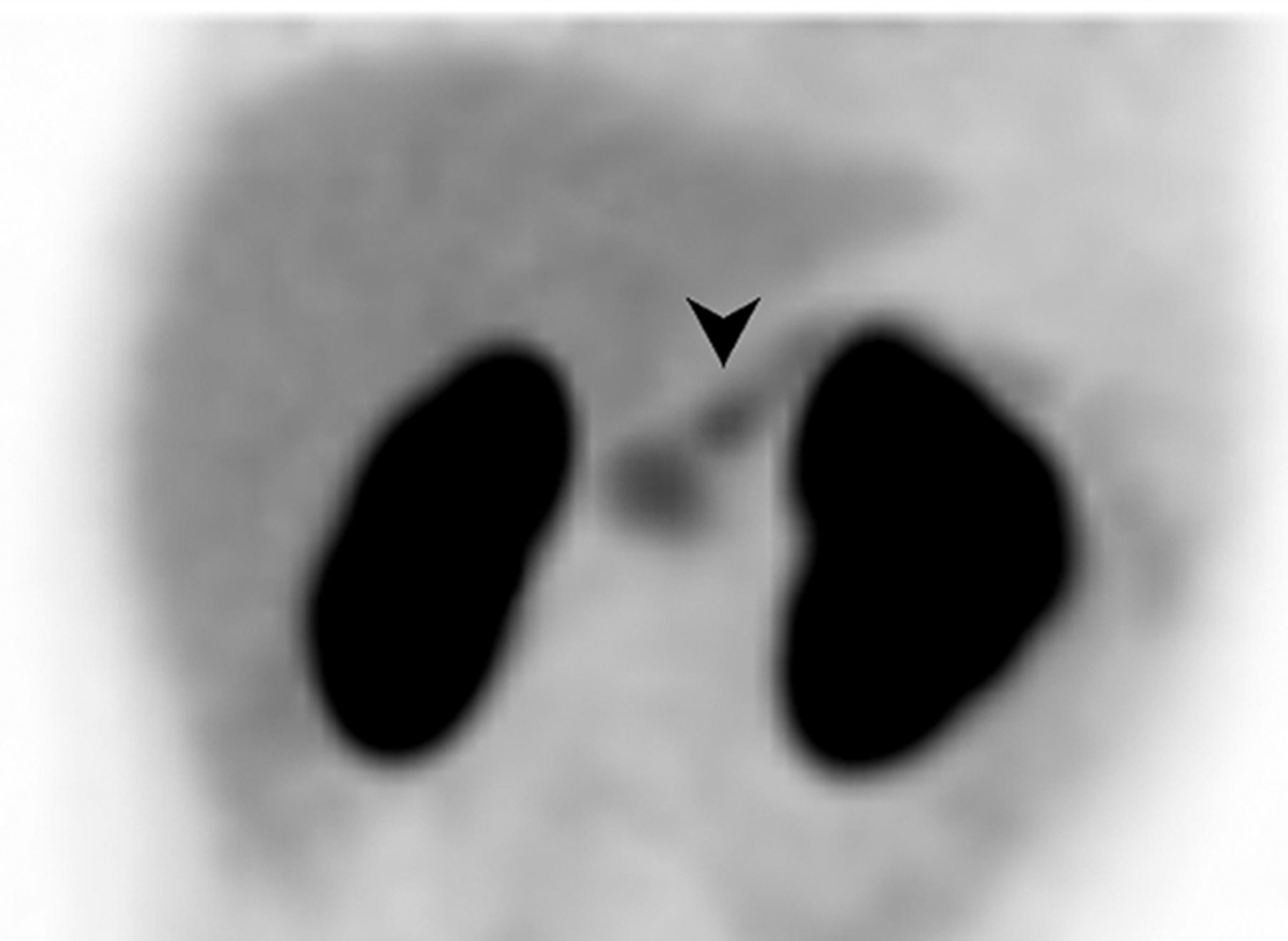
Diffuse disease most often will have homogeneous diffuse uptake (Supplemental Fig. 2). Sometimes, however, uptake can be heterogeneous or appear as multiple lesions (Supplemental Fig. 3) (24). The most common site for a focal lesion is in the head/neck region; this site was seen in 55% of cases by Adzick et al. (20). Difficulty in the detection of a focal lesion can be due to size, shape, and location. The smallest lesion reported as detected was 4 × 5 mm (25). Small lesions in the pancreatic head may be difficult to identify because of the large volume of tissue and background activity in normal tissue. Often, the activity in the pancreatic head is slightly higher than that in the rest of the normal pancreas; this finding is thought to be due to the volume of tissue. Increased activity in the pancreatic head, typically nonfocal, can be seen in the setting of a focal lesion in the body or tail and may be misinterpreted as 2 lesions (Fig. 6). The finding of multiple lesions is rare; however, the possibility should be discussed with the surgeon (Fig. 5). Thin “sheetlike” lesions have been described as missed lesions (26,27).

Focal lesion in pancreatic body. 3-mo-old female with ABCC8 mutation and paternal mutation. 18F-FDOPA 3-dimensional MIP image shows mild increased activity in pancreatic head and small lesion (arrowhead) in pancreatic body. Focal lesion was found in pancreatic body, abutting vasculature and requiring 50% pancreatectomy.
The location of the lesion is also important. Lesions in the pancreatic tail adjacent to the left kidney can be obscured or overlooked, especially in early images, when the intensity of the tracer in the renal cortex is highest (Supplemental Fig. 4) (28). Ectopic lesions in the small bowel may also be missed if not searched for (29,30). Giant lesions may have heterogeneous activity, with the detection of a focal area but with underestimation of the size and extent of the lesions (31). In addition, a large focal lesion can be confused with diffuse disease (27). Diffuse pancreatic enlargement should raise the possibility of BWS (Fig. 7; Supplemental Fig. 5). Atypical disease was reported in most of the studies in Table 1. Diffuse lesions most often have diffuse homogeneous uptake (Supplemental Fig. 6).

BWS. 1-mo-old male with suspected BWS and presenting with HI. 18F-FDOPA 3-dimensional MIP image at 10 min shows uptake within markedly enlarged pancreas, typical of BWS. Increased uptake within enlarged kidneys is also related to patient’s syndrome. Patient underwent 95% pancreatectomy.
Quantitative analysis has been proposed using an SUVmean ratio (SUVmean of the lesion/SUVmean of normal pancreas) with a cutoff of >1.2 for a focal lesion (25,32,33) or an SUVmax ratio (SUVmax of lesion/SUVmax of normal pancreas) with a cutoff of 1.5 (15,34). Masue et al. reported a high percentage of lesions with irregular uptake or the appearance of multiple lesions (26). In these cases, a comparison of SUV analysis with visual analysis showed an increase in diagnostic accuracy from 50% to 75% (26). Christiansen et al. compared qualitative analysis with the SUVmax ratio, using a cutoff SUVmax ratio of 1.44 determined by receiver operating characteristic evaluation to predict focal disease (35). Visual criteria performed as well as qualitative criteria (35). Further study is recommended to determine whether quantitative analysis is helpful in equivocal or atypical cases.
SAFETY
18F-FDOPA has a favorable safety profile. No adverse events have occurred during the administration of 18F-FDOPA synthesized by the University of Pennsylvania cyclotron in 415 scans performed at the Children’s Hospital of Philadelphia and the Hospital of the University of Pennsylvania. In addition, no adverse events were found in 107 adult patients scanned for neuroendocrine tumor evaluation (36). In a dosimetry study, Garg et al. found a mean effective dose equivalent for 18F-FDOPA of 0.4 ± 0.04 mSv/MBq (14). In comparison, in newborns, the effective dose equivalent for 18F-FDG is 0.43 ± 0.15 mSv/MBq (37). An example given for a PET/CT effective dose using a 25-MBq 18F-FDOPA injection was 13.25 mSv, with 18F-FDOPA contributing 7.55 mSv and low-dose CT for attenuation correction contributing 5.7 mSv. The additional contrast-enhanced CT would include an additional radiation dose. The organs receiving the highest radiation within the field of view are the urinary bladder wall, pancreas, liver, and kidneys. Hydration is essential to minimize the bladder dose. Imaging with PET/MRI can decrease exposure to radiation, but access is currently limited. Alternatively, PET data can be fused with MRI data.
18F-FDOPA has been registered in the European Union since November 2006 (38). A new drug application filed in the United States in 2018 is in review by the Food and Drug Administration (39) and includes the nucleophilic technique as the proposed chemistry, manufacturing and control technique. This synthesis method produces a higher specific activity and a lower mass dose than the traditional electrophilic method and is a simpler procedure (14,40). 18F-FDOPA was approved in October 2019 for use in adults with Parkinson disease (41).
FUTURE CONSIDERATIONS
Carbidopa has been used as a tool to identify insulinoma in adults and has been proposed to decrease normal background activity, enhancing the visualization of a focal lesion (42,43). Christensen et al. compared 18F-FDOPA PET/CT with 68Ga-DOTANOC PET/CT and found 18F-FDOPA to be superior (35). The area under the receiver operating characteristic curve was 0.98 (0.93–1) versus 0.71 (0.43–0.95) (P < 0.03). Pitfalls of 68Ga-labeled somatostatin receptor imaging include increased uptake in the uncinate process in normal tissue and uptake in splenules, which can be confused with exophytic tail lesions. Intrapancreatic accessory spleen will also have increased activity in somatostatin receptor imaging (44,45) and can cause a false-positive result. Other radiotracers, such as glucagonlike peptide 1 receptor agonists labeled with 18F or 68Ga, have been studied for the evaluation of insulinoma (46–48) in adult populations and are being further explored to determine whether they could be of any value in the management of congenital HI.
CONCLUSION
18F-FDOPA continues to have limited availability in the United States and has not yet been approved by the Food and Drug Administration for the imaging of congenital HI. 18F-FDOPA PET is safe and has been adopted as a standard of care in cases of HI with a suspected focal lesion. The goals are identification and localization. Studies should be performed at sites with a multidisciplinary team with expertise in endocrinology, radiology, surgery, and pathology. A team approach is essential for optimal care of infants and children with HI.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: 18F-FODPA PET is the imaging method of choice for the identification and localization of a focal lesion causing congenital HI.
PERTINENT FINDINGS: Hyperinsulinism unresponsive to diazoxide therapy is an indication for 18F-FDOPA PET.
IMPLICATIONS FOR PATIENT CARE: A paternally inherited ABCC8 or KCNJ11 mutation with a loss of heterozygosity is highly predictive of the presence of a focal lesion.
ACKNOWLEDGMENTS
We thank the CHOP anesthesiologists and nuclear medicine technologists performing the studies and the University of Pennsylvania cyclotron staff for the production of all of our 18F-FDOPA radiotracer, with both electrophilic and nucleophilic syntheses. All of our images were obtained under a Food and Drug Administration Investigational New Drug application and a protocol described at ClinicalTrials.gov Identifier NCT01916148. Informed consent was obtained after full clinical evaluation by the Congenital Hyperinsulinism Center at the Children’s Hospital of Philadelphia under the leadership of Dr. Diva DeLeon.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 11, 2020.
- Accepted for publication December 8, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}