


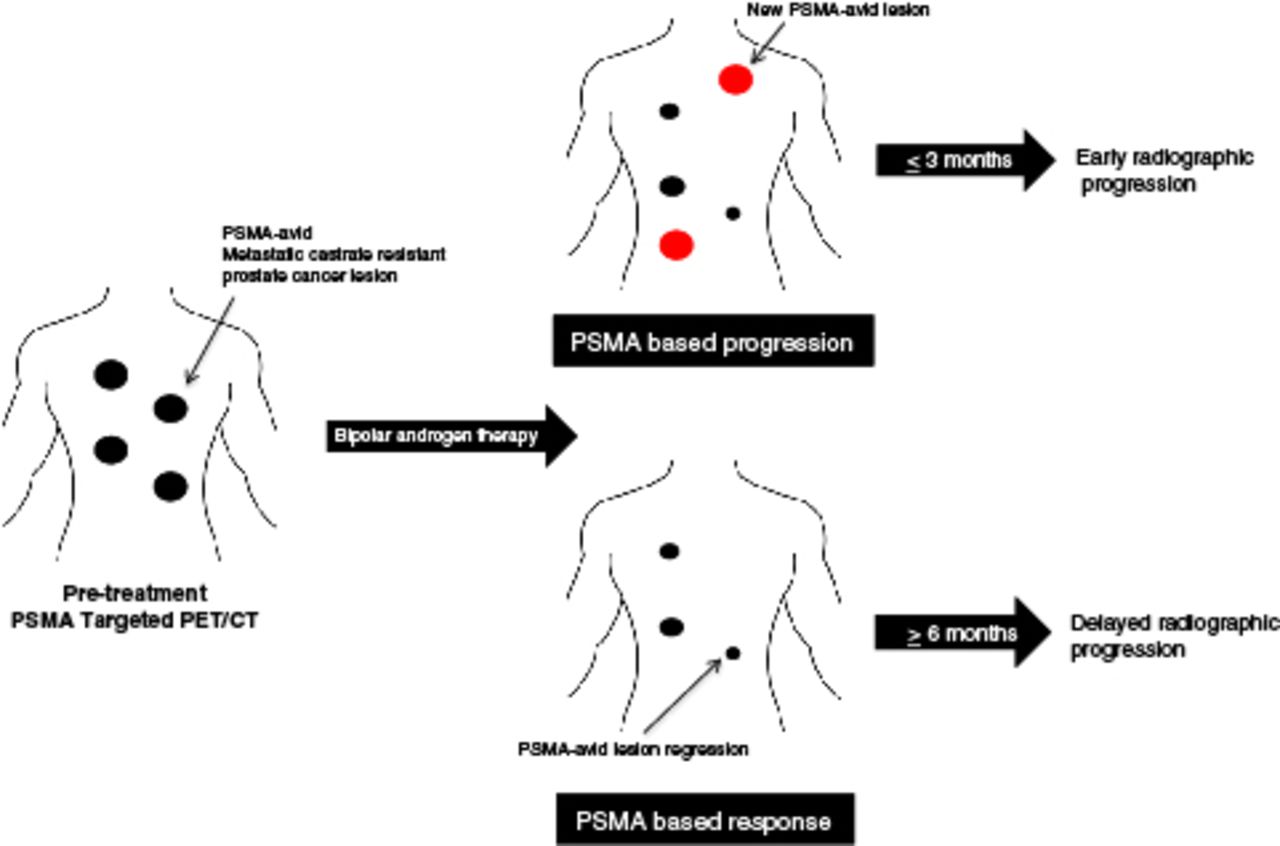
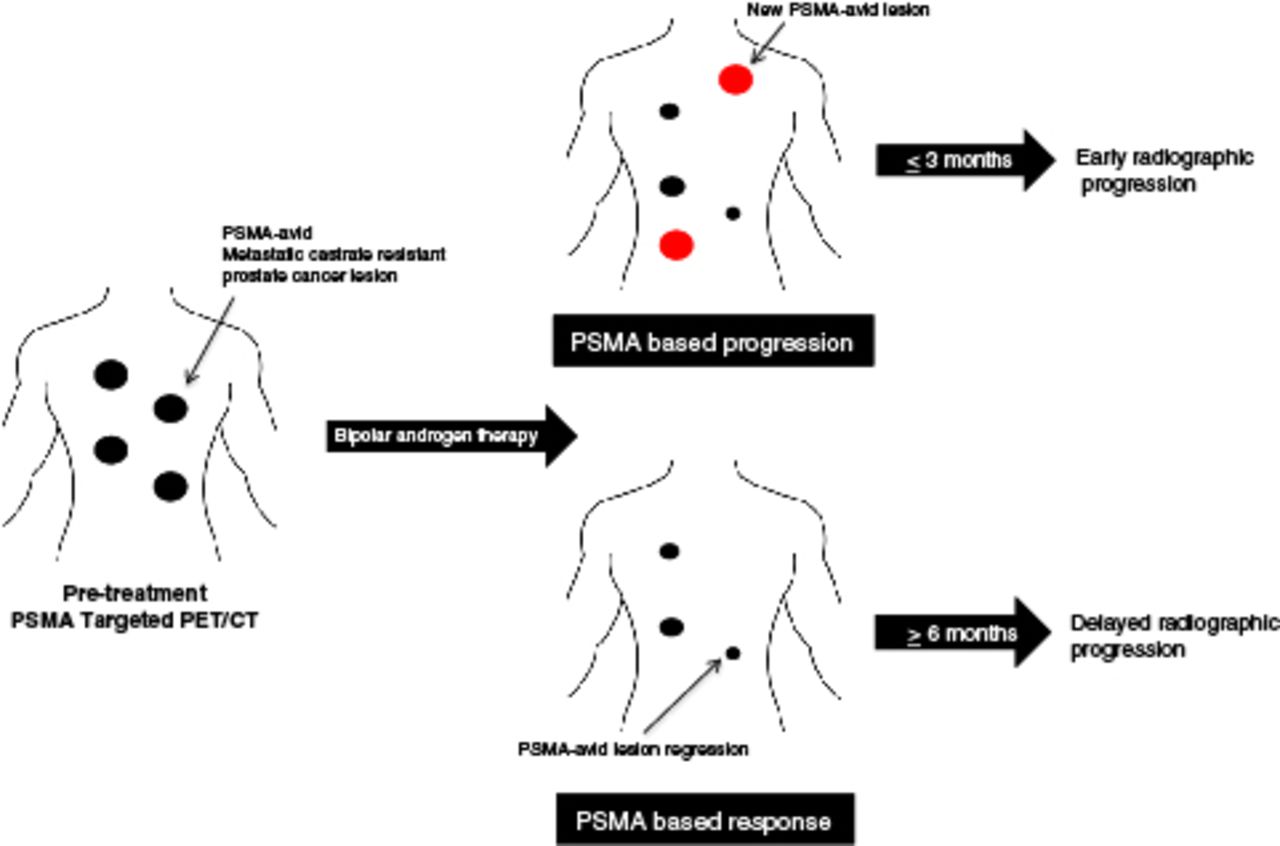
Visual Abstract
Abstract
Bipolar androgen therapy (BAT) is an emerging treatment for metastatic castration-resistant prostate cancer (mCRPC). 18F-DCFPyL is a small-molecule PET radiotracer targeting prostate-specific membrane antigen (PSMA). We analyzed the utility of 18F-DCFPyL PET/CT in determining clinical response to BAT. Methods: Six men with mCRPC receiving BAT were imaged with 18F-DCFPyL PET/CT at baseline and after 3 mo of treatment. Progression by PSMA-targeted PET/CT was defined as the appearance of any new 18F-DCFPyL–avid lesion. Results: Three of 6 (50%) patients had progression on 18F-DCFPyL PET/CT. All 3 had stable disease or better on contemporaneous conventional imaging. Radiographic progression on CT or bone scanning was observed within 3 mo of progression on 18F-DCFPyL PET/CT. For the 3 patients who did not have progression on 18F-DCFPyL PET/CT, radiographic progression was not observed for at least 6 mo. Conclusion: New radiotracer-avid lesions on 18F-DCFPyL PET/CT in men with mCRPC undergoing BAT can indicate early progression.
The imaging of prostate cancer in many parts of the world has recently been revolutionized by the introduction of small-molecule PET radiotracers that bind to prostate-specific membrane antigen (PSMA) (1). PSMA is a transmembrane glycoprotein that is expressed in most prostate cancers (2). Those agents, which include both 68Ga-labeled (e.g., 68Ga-PSMA-11 (3)) and 18F-labeled (e.g., 18F-DCFPyL (4)) compounds, have been shown to have high rates of detection of sites of prostate cancer in a variety of disease states (5).
There is an interplay between androgen signaling and PSMA expression in which blockade of the androgen-signaling pathway leads to upregulation of PSMA (6). Varying responses to androgen-axis–targeted therapies have been observed on serial PSMA-targeted PET studies (7), making it difficult to assess response to such therapies. To date, changes in serial PSMA-targeted PET have not been described in the context of bipolar androgen therapy (BAT).
BAT is being tested as a novel treatment for men with metastatic castration-resistant prostate cancer (mCRPC). Testosterone is administered to supraphysiologic circulating levels, which subsequently decrease over a 28-d cycle back to near-castrate levels (8). All men are maintained on androgen deprivation to suppress endogenous testosterone production from the testes. Several studies have demonstrated the efficacy of BAT as a treatment option for mCRPC patients (9–11). Measuring the clinical benefit of BAT using changes in prostate-specific antigen (PSA) is difficult because radiographic regression of disease has been observed, with stable or rising PSA values (10,11).
A novel imaging strategy to determine patients at high risk of progression on BAT is needed. In this pilot study, we examined changes in 18F-DCFPyL PET imaging after treatment with BAT in men with mCRPC.
MATERIALS AND METHODS
18F-DCFPyL PET/CT imaging was obtained as part of an Institutional Review Board–approved prospective substudy on 2 clinical trials for men initiating treatment with BAT (ClinicalTrials.gov identifiers NCT02286921 and NCT03554317). Written informed consent was obtained from all participants. All participants had mCRPC and prior treatment with at least 1 novel androgen receptor–targeted therapy. PET/CT images were acquired on either a Biograph mCT 128-slice scanner (Siemens Healthineers) or a Discovery RX 64-slice scanner (GE Healthcare) using 3D emission mode with CT-based attenuation correction. Scans were initiated 60 min after the intravenous infusion of 333 MBq (9 mCi) of 18F-DCFPyL with a field of view from the mid thighs through the skull vertex. Images were reconstructed with standard ordered-subset expectation maximization.
All 18F-DCFPyL PET/CT scans were interpreted by a single radiologist who was masked to the details of the patient’s disease status while on BAT. Radiotracer uptake outside the normal biodistribution of 18F-DCFPyL was categorized according to the PSMA Reporting and Data System, version 1.0, interpretive framework, and lesions that were category 3A/3B/4/5 were considered positive for prostate cancer (12). SUVmax was recorded for all lesions on baseline and follow-up scans (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org). According to the study protocol, patients underwent 18F-DCFPyL PET/CT imaging before starting BAT and again after 3 cycles. Clinicians were masked to the results of 18F-DCFPyL PET/CT imaging, and those results were not used in clinical management.
Comparisons were made between the pretreatment and on-treatment PSMA-targeted PET/CT imaging to determine progression. PSMA progression was defined as having one or more new lesions deemed by the interpreting radiologist to be consistent with radiotracer-avid prostate cancer. Radiographic progression on conventional imaging was defined by RECIST, version 1.1 (soft-tissue lesions), and by Prostate Cancer Clinical Trials Working Group 3 guidelines (clinical and bone lesions), and objective response was defined using RECIST (13,14).
RESULTS
Six patients were enrolled. Five of the 6 (83.3%) began BAT on the same day as their baseline 18F-DCFPyL PET scan, and the final patient started BAT the following day. The interval from initiation of therapy to follow-up PET was a median of 84 d (interquartile range, 83.25–87.75). At the time of the follow-up PET, repeat imaging was obtained with CT and bone scanning.
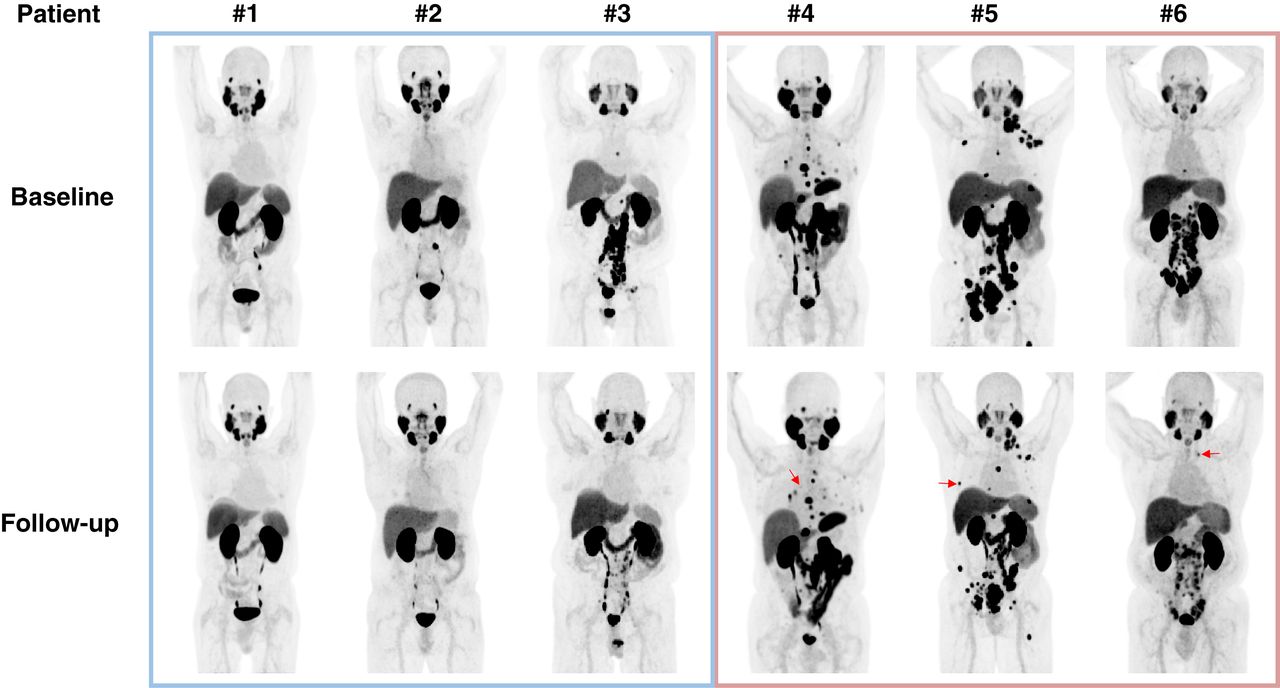
The best PSA and change in tumor response are listed for each patient in Table 1. Four of the 6 (66.7%) patients had a PSA50 (decrease in PSA level by 50% from baseline) response, and 1 patient achieved an objective response on conventional imaging. We assessed each patient for progression on PSMA-targeted imaging. Three of the 6 (50.0%) patients had progression on 18F-DCFPyL PET/CT. A description of each 18F-DCFPyL PET/CT lesion is provided in Supplemental Table 1. None of the patients had evidence of radiographic progression on conventional imaging at the time of the follow-up 18F-DCFPyL PET/CT. Two patients, who achieved a PSA50 response with stable disease on CT and bone scanning, had new lesions seen on 18F-DCFPyL PET. Neither patient with a PSA90 (decrease in PSA level by 90% from baseline) response had progression on 18F-DCFPyL PET/CT. Maximum-intensity projections of the 18F-DCFPyL PET/CT for patients before and during treatment are shown in Figure 1. Many radiotracer-avid lesions became less intense after BAT. For instance, patient 1 had a complete PSMA response to BAT (i.e., 100% reduction in SUVmax across all PSMA-avid lesions) in the clinical context of a rising PSA on therapy. Patients 4–6 had at least 1 new PSMA-avid lesion that developed on BAT. In all 3 cases of progression on PET/CT, most 18F-DCFPyL–avid lesions became less intense.

Changes in 18F-DCFPyL PET/CT imaging after 3 mo of BAT. Baseline and follow-up maximum-intensity-projection whole-body images are shown for each patient included in study. For patients 4–6, representative new lesions or sites of progression are demarcated with arrows. Additional new lesions may be hidden by normal uptake or other sites of disease.
Best Biochemical, Radiographic, and 18F-DCFPyL Response After 3 Months of BAT
We next explored the relationship between 18F-DCFPyL PET/CT findings and radiographic progression on conventional imaging. In the 3 patients who did not have progression on 18F-DCFPyL PET/CT, radiographic progression on BAT was not observed until 6–9 mo after the second PET/CT scan (Fig. 2). In contrast, all patients with progression on PET/CT had evidence of progression on conventional imaging by 3 mo. In all instances of early progression, the sites of progression on CT or bone scanning correlated with the PSMA-targeted PET findings.

Swimmer plot showing radiographic response/progression on BAT. All patients were followed until radiographic progression. 18F-DCFPyL PET/CT imaging was performed before start of BAT and after 3 mo of treatment. Patients 1–3 had no progression noted with 18F-DCFPyL. Patients 4–6 had new 18F-DCFPyL–avid lesions. These data suggest that disease progression on PSMA-targeted PET imaging precedes detection on conventional imaging.
DISCUSSION
BAT and PSMA-targeted imaging both remain under clinical investigation for patients with prostate cancer. When testosterone binds to androgen receptor, it induces PSA expression, meaning there is an urgent need for the development of a biomarker that can identify early disease progression because rising PSA is unreliable.
We performed a pilot imaging study assessing the effect of BAT on 18F-DCFPyL PET/CT imaging. After initiation of treatment, most sites of radiotracer uptake had a decrease in SUVmax at the 3-mo time point. There are several possible explanations for this finding. One is that BAT induced regression of disease across multiple sites, as is consistent with the lack of radiographic progression after 3 mo of therapy. However, given the degree of change in SUVmax, one would expect to see more objective responses at that time point. A second explanation is that BAT inhibits the expression of PSMA protein. Prior studies have shown that androgen receptor inhibition increases PSMA expression and may cause a flare on PSMA-targeted PET (6,15). It is plausible that reengagement of androgen receptor via exogenous testosterone may downregulate PSMA expression while maintaining tumor viability. This artifact would result in a false-negative scan result. Alternatively, BAT may downregulate PSMA protein as an early event in apoptosis. It has been shown that PSMA may direct cellular growth through phosphatidylinositol-3′-kinase/protein kinase B signaling (16). Thus, decreasing PSMA expression may result in tumor regression. True radiographic progression did not occur for 9–12 mo after the 18F-DCFPyL PET scan, which would support the possibility that these findings indicate an early clinical response. Arguing against transcriptional inhibition of PMSA expression are the findings of new or worsening 18F-DCFPyL–avid lesions. That phenomenon was observed only in patients who experienced radiographic progression at their next restaging scan.
The utility of 18F-DCFPyL PET/CT imaging may be in identifying those patients at highest risk of progressing on BAT. Patients who demonstrate new 18F-DCFPyL–avid lesions all had early radiographic progression.
This study was limited by the small number of patients and the use of only 2 imaging time points. In addition, the fact that all scans were read by a single radiologist (although masked) could bias the results of the study. A larger prospective study is under way to confirm these findings (NCT04424654).
CONCLUSION
Treatment with BAT induced radiographic changes on 18F-DCFPyL PET/CT imaging. New radiotracer-avid lesions on 18F-DCFPyL PET/CT in men with mCRPC undergoing BAT can indicate early progression.
DISCLOSURE
This project was supported by the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins; by NIH grants P30 CA006973 and R01 CA184012; and by the Patrick C. Walsh, PCF Challenge, and Young Investigator Awards. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Cancer Institute or the National Institutes of Health. Martin Pomper is a coinventor on a U.S. patent covering 18F-DCFPyL and as such is entitled to a portion of any licensing fees and royalties generated by this technology. This arrangement has been reviewed and approved by the Johns Hopkins University in accordance with its conflict-of-interest policies. Steven Rowe is a consultant to Progenics Pharmaceuticals, the licensee of 18F-DCFPyL. Michael Gorin has served as a consultant to Progenics Pharmaceuticals. Martin Pomper, Kenneth Pienta, Michael Gorin, and Steven Rowe receive research funding from Progenics Pharmaceuticals. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Early progression on BAT is difficult to detect given the effect of testosterone on PSA expression and the limitations of conventional imaging.
PERTINENT FINDINGS: New radiotracer-avid lesions on 18F-DCFPyL PET/CT imaging were observed in mCRPC patients on BAT who experienced early progression on conventional radiography.
IMPLICATIONS FOR PATIENT CARE: PSMA-targeted PET/CT may identify mCRPC patients at risk of early progression on BAT.
Footnotes
Published online January 15, 2021.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 24, 2020.
- Accepted for publication January 3, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.