


Visual Abstract

Abstract
The purpose of this study was to compare 18F-FDG PET/CT and CT performance in guiding percutaneous biopsies with histologic confirmation of lung lesions. Methods: We prospectively evaluated 341 patients, of whom 216 underwent 18F-FDG PET/CT–guided biopsy and 125 underwent CT-guided biopsy. The pathology results, lesion size, complications, and rebiopsy rate in the 2 groups were evaluated. Results: Of the 216 biopsies with PET/CT guidance, histology demonstrated 170 lesions (78.7%) to be malignant and 46 (21.3%) to be benign. In the CT-guided group, of 125 lesions, 77 (61.6%) were malignant and 48 (38.4%) were benign (P = 0.001). Inconclusive results prompted the need for a second biopsy in 18 patients: 13 of 125 (10.4%) in the CT group and 5 of 216 (2.3%) in PET group (P = 0.001). Complications were pneumothorax (13.2%), hemothorax (0.8%), and hemoptysis (0.6%). No life-threatening adverse events or fatalities were reported. The difference in complication rates between the 2 groups was not significant (P = 0.6). Malignant lesions showed a greater mean size than benign lesions regardless of the group (P = 0.015). Conclusion: PET/CT-guided biopsy of lung lesions led to fewer inconclusive biopsies than CT-guided biopsy, with similar complication rates.
Lung lesions represent frequent findings in clinical practice, both on radiography and in CT studies, causing concern in physicians and patients. Although pulmonary nodules might be related to conditions of low overall risk, in a nonnegligible number of cases they inspire more caution. An immediate question arises from doctors and patients alike: “Could it be cancer?” As expected, a great deal of anxiety toward the precise diagnosis is created.
Nearly 30,000 new lung cancer diagnoses were made in Brazil in 2018 and 2019 combined, representing the second most frequent cancer in men and the fourth in women (with the exception of nonmelanoma skin cancer). This rate translates into roughly 40 new reports of lung cancer in the country, daily (1).
Besides being highly prevalent, lung cancer is also responsible for the greatest number of cancer-related deaths worldwide—both in male and in female populations: around 1.8 million annual deaths (2). In Brazil, 82% of patients do not survive the 5-y period after initial diagnosis (3).
Offering patients adequate treatment relies heavily on appropriate tumor classification regarding several different features, including imaging and pathology evaluation (4). Lung cancer as an entity encompasses several different pathologic categories, which demand somewhat distinct treatment strategies. Hence, tumor sampling represents a cornerstone in the diagnostic and treatment decision (5,6).
The appropriate biopsy technique for sampling (open, transbronchial, or percutaneous) depends on a series of factors, perhaps the most important one being the tumor localization. In general, open biopsies tend to be avoided whenever possible, given their increased complexity and morbidity compared with other methods. Central and perihilar masses are routinely accessed through bronchoscopy, whereas percutaneous biopsy is generally preferred for more peripheral lesions.
Percutaneous biopsies guided by imaging methods are well-established procedures included in all major international societies’ lung cancer guidelines (7–12). These procedures yield optimal tumor sampling, with excellent performance and low complication rates (13).
PET/CT with 18F-FDG has been increasingly applied in the diagnostic workup of pulmonary lung lesions because of its ability to better stratify the risk of malignancy and the added value for correct staging of patients in whom malignancy is later confirmed (14,15).
For years, CT-guided biopsy has been widely accepted as an effective and safe method in the diagnostic workup in several different clinical settings. PET/CT-guided biopsy, which combines the anatomic information obtained from CT and the metabolic information from 18F-FDG PET, is a feasible procedure that may optimize the diagnostic yield of image-guided interventions (16,17).
After a thorough search of the medical literature, we were unable to find studies directly comparing the 2 different approaches to percutaneous lung biopsy (i.e., guided by PET/CT or by CT alone). In the present study, we aimed to evaluate the performance of both CT- and PET-guided biopsies.
MATERIALS AND METHODS
The present study was approved by the Institutional Review Board and was performed in accordance with pertinent ethical guidelines. In total, 341 patients were referred to Quanta Diagnóstico e Terapia for biopsy of suspected lung lesions: 216 underwent 18F-FDG PET/CT–guided biopsy, and 125 underwent CT-guided biopsy. The study followed a prospective approach, with a minimum follow-up of 6 mo for disease evolution.
PET/CT access was ultimately used as the randomization mechanism for our study, with patients not granted authorization for PET by their health-care providers (public or private) being allocated to the CT-only group. CT- and PET-guided biopsies were performed by the same physician using the same PET/CT scanner with a fluoroscopic imaging system. Written informed consent was obtained from all patients eligible for this study between 2018 and 2020. After biopsy, samples were analyzed histologically in the same reference laboratory. A complete blood count with platelet and coagulation evaluation was requested before each biopsy. Exclusion criteria were a platelet count of less than 100,000/μl, abnormal coagulation test results, or a clinical contraindication to the procedure.
Whole-body 18F-FDG PET/CT imaging was performed after an uptake period of 60–90 min after intravenous administration of 296–444 MBq (8–12 mCi) of 18F-FDG. Imaging was performed using an STE-16 PET/CT scanner (GE Healthcare) with a CT fluoroscopic imaging system. Areas of nonphysiologic increased 18F-FDG uptake over the background level were classified as positive for disease. The technical procedure was performed as previously described (6). Patients were positioned according to the lesion location and biopsy planning. Light sedation was preferentially used. After antisepsis, local anesthesia was performed. A coaxial guide needle was inserted under the guidance of CT fluoroscopic imaging. One-bed-position PET/CT images were acquired to confirm correct positioning of the coaxial needle (directing the needle toward the most accessible areas of high metabolism). Four to 6 specimens were collected under CT fluoroscopy. After removal of the needle, manual compression was performed at the puncture site. The patients were observed for at least 2 h after the procedure to ensure hemodynamic stability and to monitor the respiratory condition.
CT-guided biopsies were performed in the same way as the PET/CT-guided biopsy, except for the single 18F-FDG PET bed position. All other steps were basically the same.
The technical success rate (acquisition of a suitable sample for histopathologic evaluation) and complication rates (including pneumothorax, hemothorax, and hemoptysis) were compared between PET/CT-guided biopsies and CT-guided biopsies. The histopathologic results (malignant vs. benign lesions) were also compared between the 2 techniques, searching for different malignancy detection rates. Student t testing, χ2 testing, and 2-tailed and Fisher exact testing were applied for group comparisons of continuous and binomial variables, using statistical analysis software (Stata, version 11).
RESULTS
The study included 341 patients who underwent percutaneous biopsy of lung lesions. Patient demographics and main results are summarized in Table 1.
Patient Characteristics and Differences Between Groups
Among the lesions sampled in the first round of biopsies, malignant results were observed in 170 of 216 patients in the PET/CT group (78.7%; mean SUVmax, 11.8) and in 77 of 125 patients in the CT group (61.6%). Benign results were found in the remaining 46 lesions in the PET/CT group (21.3%; mean SUVmax, 7.2) and in 48 (38.4%) in the CT group (P = 0.001). The mean SUVmax for all PET lesions was 10.9, with malignant lesions presenting a higher mean SUVmax than benign lesions (11.8 × 7.2, P = 0.0006)
In selected patients, benign results were deemed questionable because of suggestive imaging features or clinical expertise and were thus considered inconclusive, prompting the need for a second biopsy. Such was the case in 18 of the 341 (5.3%) patients in this study, being 13 of 125 (10.4%) in the CT group and 5 of 216 (2.3%) in PET group (P = 0.001).
In the second round of biopsy, no statistically significant differences were observed between the 2 groups: in the CT group, 12 of 13 repeated biopsies returned positive results for malignancy, whereas the same was true for 5 of 5 repeated biopsies in the PET/CT group (P = 0.523). A summary of the main pathology results for benign and malignant lesions (including the second biopsies, totalling 359 procedures) is provided in Table 2.
Main Pathology Results for Malignant and Benign Lesions
No significant differences in lesion size were observed between the 2 groups in the first round of biopsies, although our data revealed statistically relevant differences in size between malignant and benign lesions regardless of the method by which they were examined. Lesions that required rebiopsy in the PET/CT group had a greater average size than those in the CT group (9.6 × 4.6 cm, P = 0.04).
All patients were followed for a minimum of 6 mo, during which at least 1 additional CT exam was performed and the evolution of each case was accessed through discussion with the referring physicians. All patients with initially benign pathology findings after biopsy (with the exception of those deemed inconclusive) were considered truly benign on follow-up after confirmation that the suspected lesions remained stable in size and characteristics on CT or had regressed.
All patients were followed for a minimum of 6 mo, during which at least 1 additional CT exam was performed, and the evolution of each case was accessed through discussion with the referring physicians. All patients with conclusive benign pathology findings were considered truly benign on follow-up after confirmation that the suspected lesions remained stable in size and characteristics on CT or had regressed.
The PET/CT group’s complication rate was 13.5% (29 patients), with 27 cases of pneumothorax (12.5%), 1 case of hemoptysis (0.5%), and 1 case of hemothorax (0.5%). Two patients had to be admitted to the hospital (1 for hemoptysis observation and 1 for hemothorax control). In the CT group, the complication rate was similar, at 16.8% (21 patients), which included 18 cases of pneumothorax (14.4%), 1 case of hemoptysis (0.8%), and 2 cases of hemothorax (1.6%). Three patients had to be admitted to the hospital (1 for hemoptysis control, 1 for hemothorax control, and 1 for observation of pneumothorax). There were no procedure-related deaths in either group.
DISCUSSION
To our knowledge, this comparison of 18F-FDG PET/CT and CT-guided biopsies of lung lesions was performed on the largest cohort published to date. We found higher rates of malignant lesions in the 18F-FDG PET/CT–guided group than in the CT-guided group (78.7% vs. 61.6%, P = 0.001). We hypothesize a selection bias regarding the distribution of patients between the 2 groups, with patients in the PET/CT group presenting a higher chance of having a malignancy, probably related to the better accuracy of PET/CT in the evaluation of lung lesions, most noticeably regarding nodules with an intermediate likelihood of malignancy and presenting areas of hypermetabolism. Performing the evaluation with PET/CT carries incremental value for patients for whom biopsy results will show malignancy, given PET/CT’s superiority to CT regarding all 3 descriptors of the TNM staging of non–small cell lung cancer and the recommendation that PET/CT be used in the workup for initial staging in all patients from stages I–IV (18,19).
Furthermore, we highlight that biopsy-inconclusive results differed between the 2 groups, being higher in the CT group, prompting the need for a second biopsy in 10.4% in the CT group and in 2.3% in the PET group (P = 0.001). Lung cancer lesions can be quite heterogeneous, especially in large masses where cancer cells are not present in the complete tumoral volume. The CT image of the lesion might contain inflammatory tissue, necrosis, and normal lung tissue represented by atelectasis, whereas an adequate biopsy specimen must represent an actual neoplastic area in which the evaluation of metabolism by 18F-FDG PET might improve results.
Once we integrate CT’s excellent anatomic information (especially important in evaluating vessels and essential structures related to the biopsy path) with the metabolic characterization provided by 18F-FDG PET images, sampling from the hypermetabolic portion of the apparently larger morphologic lesion seen on CT becomes feasible and is more likely to yield representative material for microscopic analysis (Figs. 1–3) (6,17,20–25).
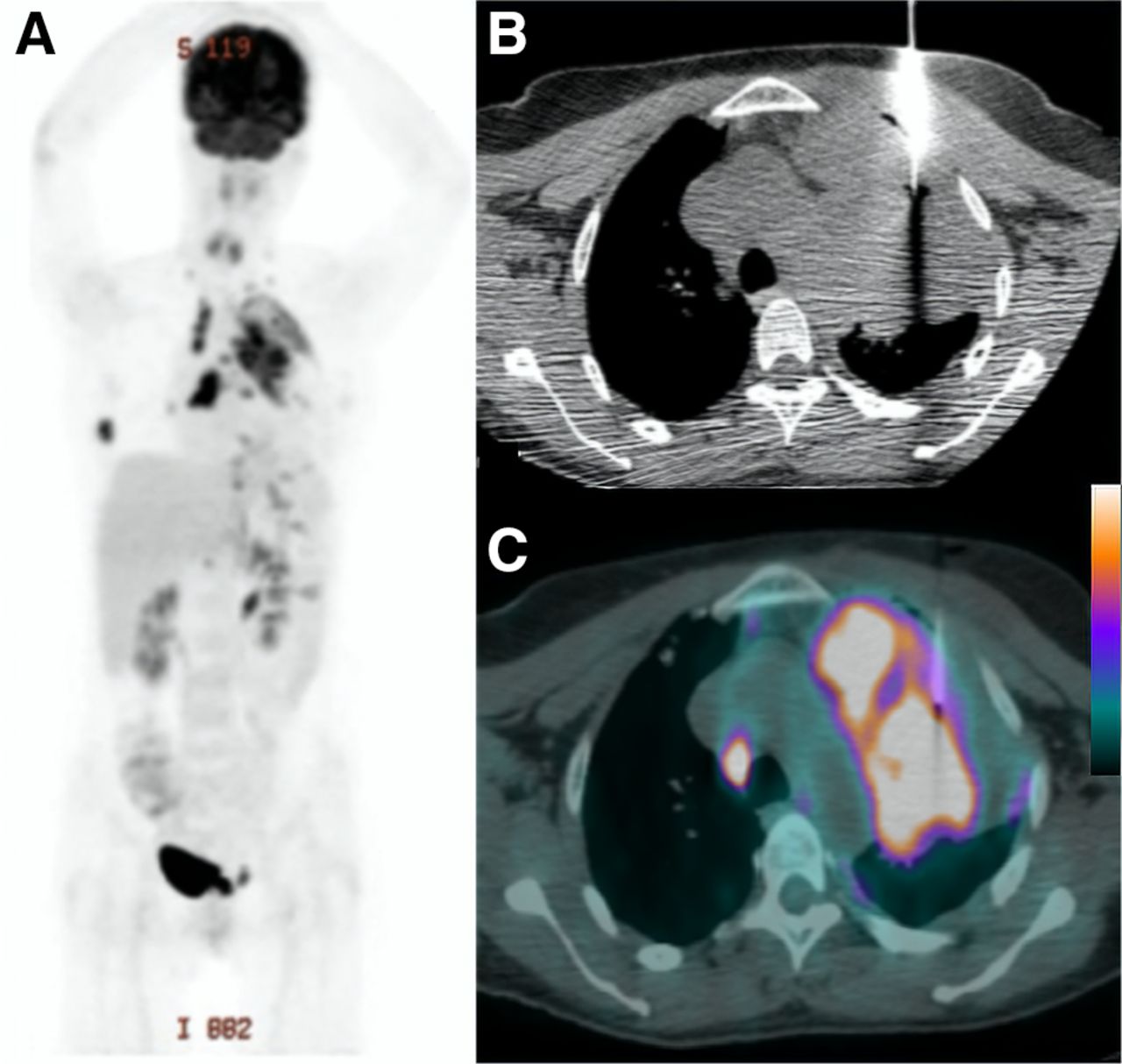
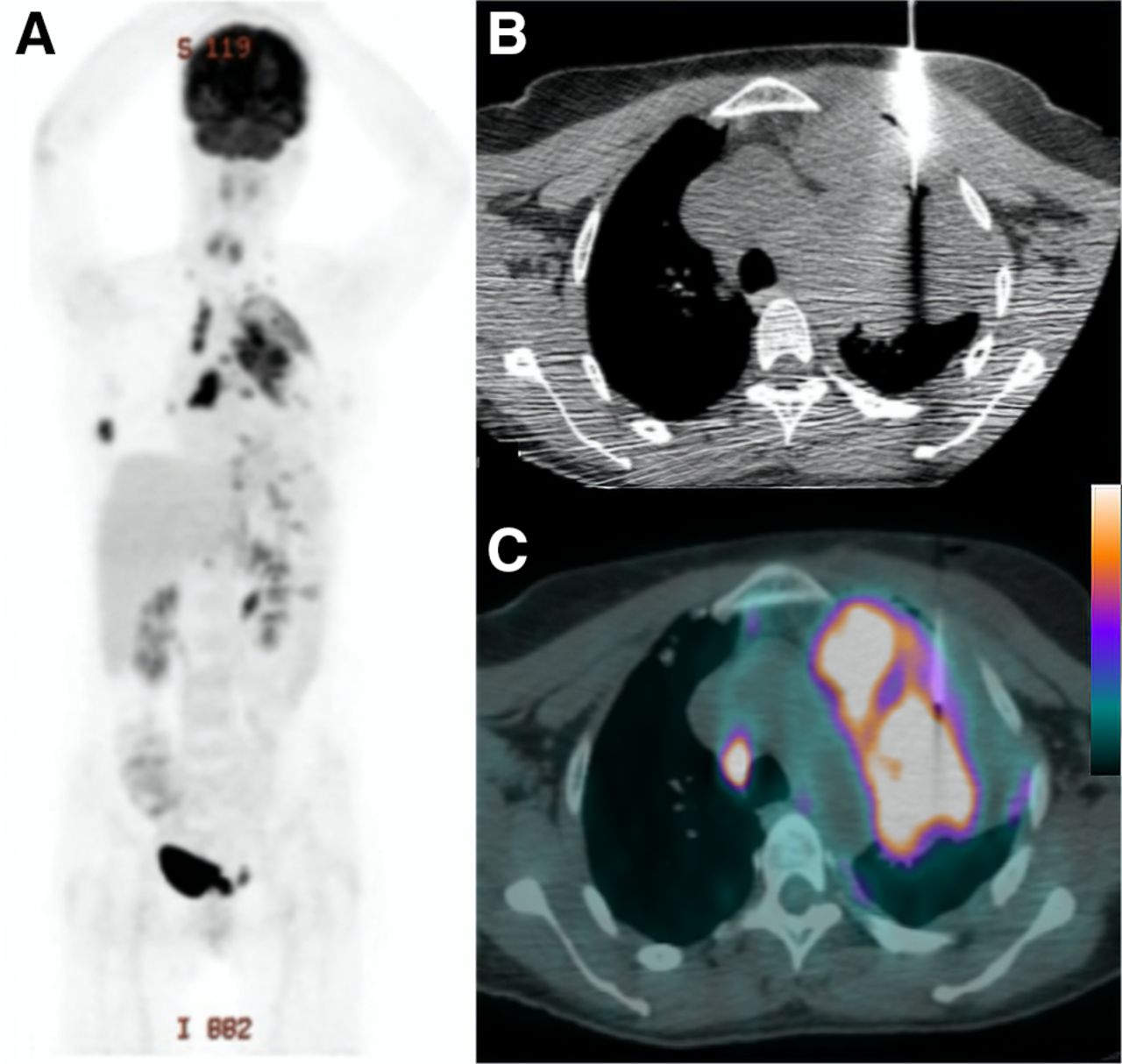
Patient with lung mass was referred for 18F-FDG PET/CT. (A) Maximum-intensity-projection PET image shows multiple lesions in left lung, lymph nodes, and bones. (B) Axial CT thoracic image shows placement of coaxial guide needle in lesion that does not differentiate atelectasis from metabolic active lung lesion. (C) Axial PET/CT image confirms that coaxial guide needle is appropriately positioned in metabolic border of lesion, ensuring that metabolically active specimens will be collected with semiautomatic needle that will be inserted 2 cm further. Pathologic analysis confirmed adenocarcinoma.

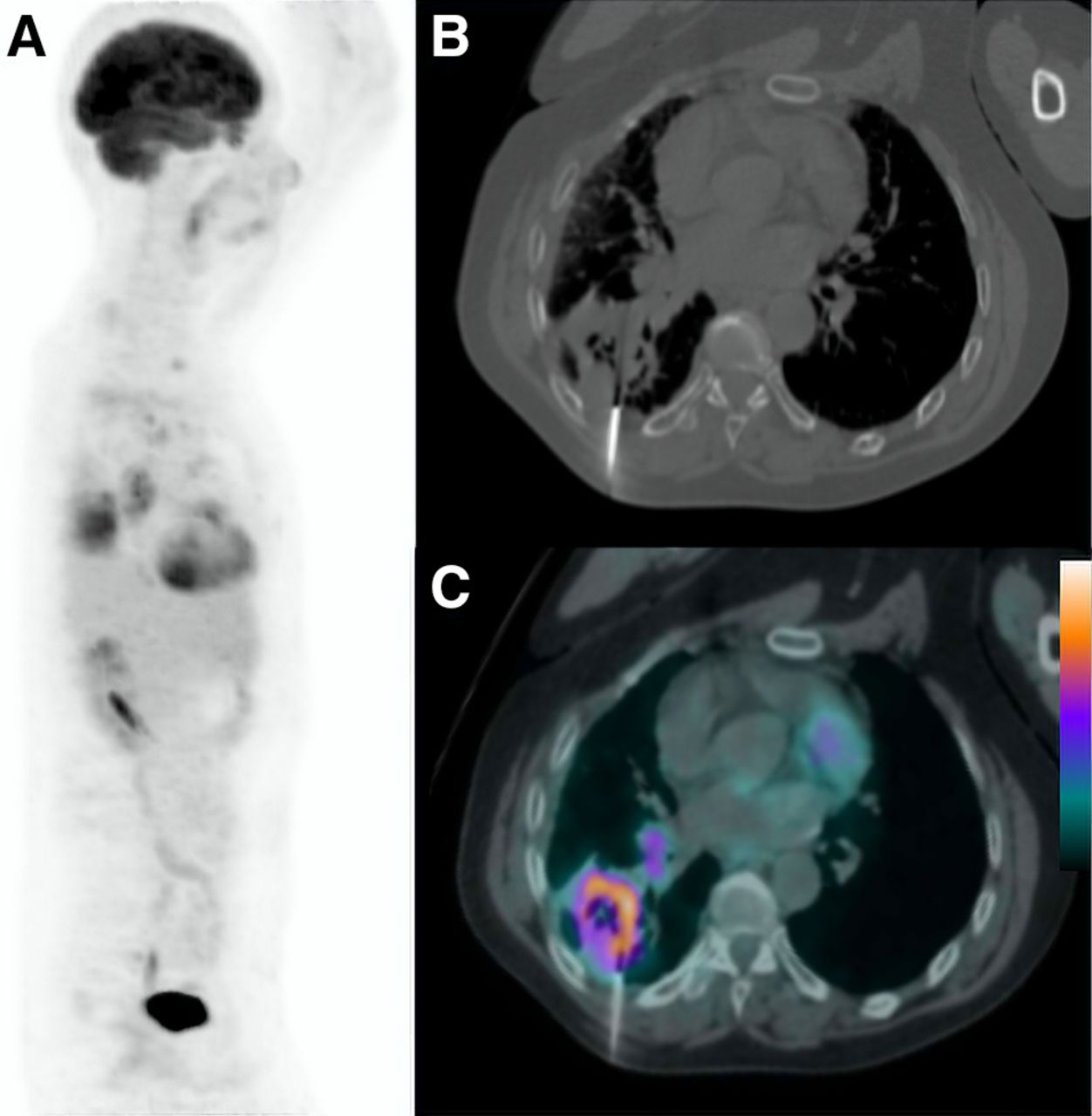
Patient with previous inconclusive biopsy presented with heterogeneous mass in left lung, with lateral part of lesion presenting area of severe 18F-FDG uptake and almost absence of 18F-FDG uptake in medial part of lesion. 18F-FDG PET/CT–guided biopsy was performed. Through anterior access, biopsy needle was directed to region with highest metabolism, thus improving odds of yielding representative neoplastic material for histopathologic analysis (in this case, results revealed adenocarcinoma). (A) Maximum-intensity-projection PET image. (B) Transaxial CT lung window. (C) Transaxial CT mediastinal window (intraprocedure). (D) Transaxial 18F-FDG PET/CT image (intraprocedure CT image fused with previously acquired PET/CT image).
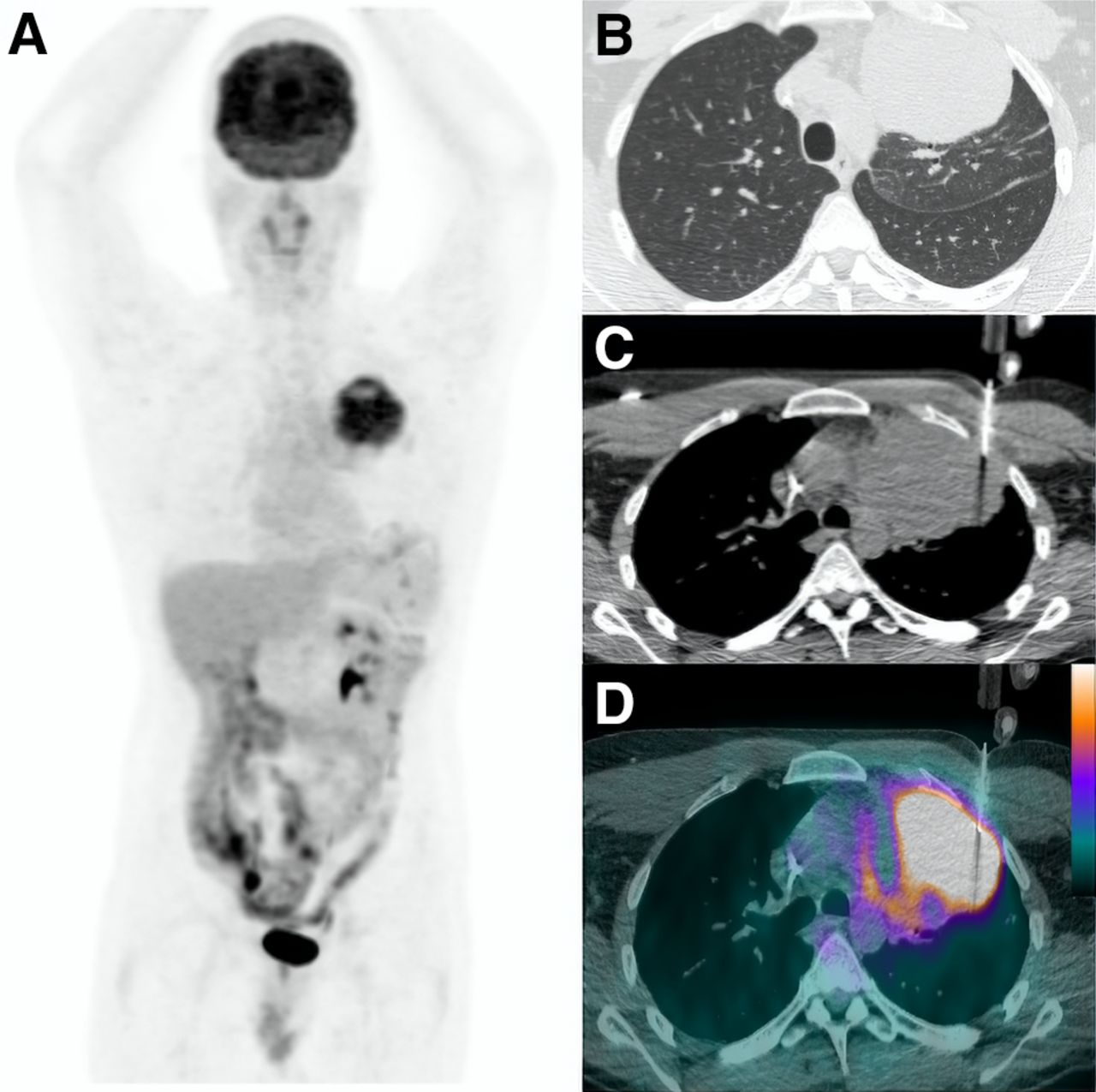
Patient with cavitated lung lesion was referred for 18F-FDG PET/CT. (A) Maximum-intensity-projection PET image. (B) Axial CT thoracic image showing semiautomatic needle placed at border of lesion. (C) Axial PET/CT image showing placement of coaxial guide needle in area with highest metabolism. Pathologic analysis confirmed primary adenocarcinoma of lung.
Another observation in our data is related to lesion size. We found malignant lesions to be larger, regardless of the group, with a mean size (measured in their greatest tridimensional diameter on CT) of 5.0 cm, against 4.0 cm for benign lesions (P = 0.015). Although there is statistical relevance related to this feature, we understand that such a narrow difference does not translate into a significant impact in clinical practice. A greater average size was observed in the lesions that required a second biopsy in the PET/CT group than in the CT group (P = 0.04), as might be related to tumoral cells’ representing a smaller proportion of the overall lesion composition in the case of large heterogeneous masses.
Lastly, we analyzed procedure safety and found similar complication rates in both groups, with no life-threatening adverse events or fatalities reported. Hence, given the size of our sample and the observed outcomes, we deem both methods quite safe overall. Regarding physician radiation safety, a similar exposure is expected between the 2 methods, since our approach did not require a repeat 18F-FDG injection during the biopsy procedure, as reported elsewhere (16).
To the best of our knowledge, this was the first study directly comparing the performance of PET/CT- versus CT-guided biopsies of lung lesions in separate groups. Our study presents a limitation of selection bias regarding the distribution of patients between the 2 groups. Access and reimbursement of PET/CT are far from being the best method for randomization but were the available method because of the Brazilian health-care system’s idiosyncrasies. Access to PET/CT examination is quite heterogeneous in Brazil. The public health-care system (Sistema Único de Saúde) applies several restraints to grant clearance for PET/CT studies. Private health insurance companies also differ greatly in requirements to cover PET/CT expenses. It is possible that this selection bias might have contributed to higher malignancy rates in the PET/CT group.
CONCLUSION
PET/CT-guided biopsy of lung lesions led to fewer inconclusive biopsies than CT-guided biopsy, with similar complication rates.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Are there any significant differences in performance between PET/CT- and CT-guided percutaneous biopsy of lung lesions?
PERTINENT FINDINGS: Among a cohort of 341 patients who were prospectively evaluated with percutaneous biopsy of suspected lung lesions, 216 underwent 18F-FDG PET/CT–guided biopsy and 125 underwent CT-guided biopsy. PET/CT-guided biopsy led to fewer inconclusive results than CT guided biopsy, with similar complication rates.
IMPLICATIONS FOR PATIENT CARE: Our results may influence the decision about the preferred method for guidance of percutaneous biopsy of lung lesions if both PET/CT and CT are available.
Footnotes
Published online December 31, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 24, 2020.
- Accepted for publication December 4, 2021.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.