


Visual Abstract

Abstract
The PET ligand 11C-PBR28 (N-((2-(methoxy-11C)-phenyl)methyl)-N-(6-phenoxy-3-pyridinyl)acetamide) binds to the 18-kDa translocator protein (TSPO), a biomarker of glia. In clinical studies of TSPO, the ligand total distribution volume, VT, is frequently the reported outcome measure. Since VT is the sum of the ligand-specific distribution volume (VS) and the nondisplaceable-binding distribution volume (VND), differences in VND across subjects and groups will have an impact on VT. Methods: Here, we used a recently developed method for simultaneous estimation of VND (SIME) to disentangle contributions from VND and VS. Data from 4 previously published 11C-PBR28 PET studies were included: before and after a lipopolysaccharide challenge (8 subjects), in alcohol use disorder (14 patients, 15 controls), in first-episode psychosis (16 patients, 16 controls), and in Parkinson disease (16 patients, 16 controls). In each dataset, regional VT estimates were obtained with a standard 2-tissue-compartment model, and brain-wide VND was estimated with SIME. VS was then calculated as VT − VND. VND and VS were then compared across groups, within each dataset. Results: A lower VND was found for individuals with alcohol-use disorder (34%, P = 0.00084) and Parkinson disease (34%, P = 0.0032) than in their corresponding controls. We found no difference in VND between first-episode psychosis patients and their controls, and the administration of lipopolysaccharide did not change VND. Conclusion: Our findings suggest that in TSPO PET studies, nondisplaceable binding can differ between patient groups and conditions and should therefore be considered.
PET with radioligands for the glial marker 18-kDa translocator protein (TSPO) has been extensively used over the past 2 decades to assess brain immune function in vivo (1). 11C-PBR28 (N-((2-(methoxy-11C)-phenyl)methyl)-N-(6-phenoxy-3-pyridinyl)acetamide) is a second-generation TSPO radioligand with signal-to-noise characteristics superior to those of the first-generation radioligand 11C-PK11195 (2). As with other second-generation TSPO tracers, the affinity of 11C-PBR28 to TSPO is affected by a single-nucleotide polymorphism on the TSPO gene (rs6971), and in clinical studies, TSPO genotype is used to classify subjects as low-, mixed-, or high-affinity binders (3,4).
PET ligand binding to TSPO is often quantified by fitting a 2-tissue-compartment model (2TCM), or variants thereof (5), to the PET time–activity curves, using parent radioligand concentration in arterial plasma as the input function. The 2TCM describes the ligand kinetics using 2 tissue compartments, one for ligand that is bound specifically to the target of interest and one for nondisplaceable binding. The nondisplaceable compartment includes both free and nonspecifically bound radioligand. The standard outcome measure reported using 2TCM is the total distribution volume (VT), which represents the ratio of total activity concentration in tissue to that in plasma at equilibrium. VT is the sum of the nondisplaceable and specific distribution volumes (VT = VND + VS). Some radioligands display negligible specific binding in a certain brain region (i.e., VS = 0). Such a region is usually referred to as a reference region and can be used to estimate VND, which is assumed to be constant throughout the brain. When a reference region is available, the binding potential with nondisplaceable uptake as a reference, BPND (=VS/VND), is typically the reported outcome measure. TSPO is expressed throughout the brain, and thus, no reference region exists for this target. It is therefore challenging to obtain reliable estimates of the relative contributions from the specific and nondisplaceable binding, leaving a degree of uncertainty about the interpretation of VT.
Recently, a method for simultaneous estimation of VND (SIME) (6) was developed to estimate VND for tracers without a reference region. SIME uses the assumption that nondisplaceable binding is constant throughout the brain and estimates a global value for VND by fitting a constrained 2TCM for several brain regions simultaneously. The performance of SIME with 11CPBR28 has been thoroughly tested in healthy human subjects (7). Using simulations, pharmacologic competition data, and test–retest data, SIME-derived estimates of VND and VS (calculated using 2TCM VT and SIME VND) were shown to be accurate and reliable (7).
For comparison of VT between groups to be meaningful, there must be an underlying assumption that VND is the same across the groups. Currently, there is limited scientific evidence to back up this assumption. Hence, our aim with this study was to investigate whether nondisplaceable binding can be a confounding factor in TSPO PET studies that use VT as an outcome measure. To achieve this aim, SIME was used to quantify VND in 11C-PBR28 data from 4 different published datasets. In the first dataset, an immune stimulator was administered to healthy subjects (8). The 3 remaining datasets contain controls and subjects with alcohol-use disorder (AUD) (9), first-episode psychosis (FEP) (10), and Parkinson disease (PD) (11).
MATERIALS AND METHODS
This study includes 4 datasets obtained at 2 PET centers. All subjects underwent a 11C-PBR28 PET scan in a high-resolution research tomograph (Siemens). Metabolite-corrected arterial input functions were collected for all scans. T1-weighted MRI scans were acquired to define regions of interest (ROIs). All subjects were genotyped for the rs6971 polymorphism, and low-affinity binders were excluded. In previous publications, VT has been the primary reported outcome measure. A list of the datasets, with subject information, is reported in Table 1, and the reader is referred to the original publications for further details on data acquisition and processing.
Dataset Summary
Lipopolysaccharide
The lipopolysaccharide dataset (8) was collected at the Yale PET Center. Eight healthy men were scanned twice on the same day, at baseline and 3 h after injection of lipopolysaccharide (dose 1.0 ng/kg), an acute immune stimulus. 11C-PBR28 was injected as a 1-min bolus, and the PET scan duration was 120 min.
AUD
The AUD dataset (9) was collected at the Yale PET center. It consists of 14 subjects with AUD and 15 age-matched control subjects. Five of the control subjects also participated in the lipopolysaccharide experiment. AUD subjects were imaged 1–4 d (in 1 case, 24 d) after intake of their last alcoholic beverage. 11C-PBR28 was injected as a 1-min bolus, and the PET scan duration was 120 min.
FEP
The FEP dataset (10) was collected at Karolinska Institutet. It consists of 16 FEP patients and 16 age-matched controls. All patients were naïve to antipsychotic drugs. 11C-PBR28 was injected as a 10-s bolus, and the PET scan duration was approximately 90 min.
PD
The PD dataset (11) was collected at Karolinska Institutet. It consists of 16 patients with PD and 16 age-matched controls. 11C-PBR28 was injected as a 10-s bolus, and the PET scan duration was 72 min.
SIME
The SIME method (6) works by first defining a grid of possible VND values. Then, for each value in the grid, a 2TCM is fitted to the time–activity curves with the constraint that K1 = VND⋅k2 in all ROIs, reducing the number of rate constants from 4 to 3. The residual sum of squares is then computed for all ROIs and frames, and the VND that yields the lowest residual sum of squares is selected as the estimate of a brain-wide VND.
For all datasets, we used a VND grid from 0.01 to 5, with steps of 0.01, based on previous studies with SIME and 11C-PBR28 (7,12). Initial evaluation of the data indicated that this range covers the cost function minimum. The residual sum of squares was weighted by the square root of the frame duration. Fractional blood volume was fitted for each ROI separately. SIME VND was calculated using time–activity curves from the cerebellum, parietal cortex, frontal cortex, occipital cortex, temporal cortex, putamen, caudate, and thalamus, thus covering various brain structures and tissue types.
Calculation of Outcome Measures and ROIs
In each ROI, VT was calculated using a standard 2TCM, including fitting of the fractional blood volume. VS (=VT − VND) was calculated from the 2TCM VT estimates and the SIME VND estimates. For all datasets except the PD dataset, we report ROI-specific outcome measures (VT, VS) in the cerebellum and frontal cortex. For PD, we report VT and VS in the striatum instead of the frontal cortex, because the striatum is considered a key region in the pathophysiology of PD and is more frequently reported in PET studies.
Statistical Analysis
Statistical analyses were performed using MATLAB (version 9.5; MathWorks). For the lipopolysaccharide data, a paired-sample t test was used for all outcome measures (VND, VT, and VS) to test for a difference between the pre- and postlipopolysaccharide scans. The percentage change in the outcome measures for each subject was calculated as 100⋅(pre − post)/pre. For the remaining datasets, a univariate 2-way ANOVA without an interaction term was applied for each outcome measure (VND, VT, and VS) to determine the group differences between controls and patients, with log-transformed outcome measures as a dependent variable and diagnosis and genotype as fixed factors, as described earlier (12). Using the regression coefficients, β, from the ANOVA, the percentage difference between patients and controls across genotypes was calculated as  . The α-level was set to 0.05. Reported P values were not corrected for multiple comparisons.
. The α-level was set to 0.05. Reported P values were not corrected for multiple comparisons.
RESULTS
For all datasets, the results obtained for VT are in accordance with those in the original publications. Below, we report the results for VT, VS, and VND for each dataset separately. The results for the ROIs presented below are consistent with the remaining ROIs included in the SIME calculation (Supplemental Tables 1–4; supplemental materials are available at http://jnm.snmjournals.org). Results were also unchanged when an interaction term was included in the ANOVA (Supplemental Tables 5–7) and when volume-based weights were used in the SIME analysis (Supplemental Tables 8–11).
Lipopolysaccharide
Lipopolysaccharide injection was associated with a significant increase in VT in both the cerebellum (mean, 40% [SD, 34%]; P = 0.016) and the frontal cortex (mean, 46% [SD, 23%]; P = 0.0012). VND was not affected by lipopolysaccharide (mean, 15% [SD, 40%]; P = 0.38). The mean increase in VS was 59% (SD, 51%) (P = 0.0052) in the cerebellum and 66% (SD, 35%) (P = 0.00026) in the frontal cortex. The results are summarized in Figure 1.

Change in outcome measures (VT, VS, and VND) between pre- and postlipopolysaccharide scans in cerebellum (A) and frontal cortex (B). Individual subjects are connected with a line. P values and percentage difference (perc. diff.) between pre- and postlipopolysaccharide scans are shown. HAB = high-affinity binder; MAB = mixed-affinity binder.
AUD
VT was significantly lower in AUD subjects than in controls, both in the cerebellum (18%, P = 0.012) and in the frontal cortex (23%, P = 0.0048). VND was 34% lower in patients than in controls (P = 0.00084). VS did not differ significantly between the groups. These results are shown in Figure 2. Genotype had a significant effect on both VT and VS (P < 0.0005) but not on VND.
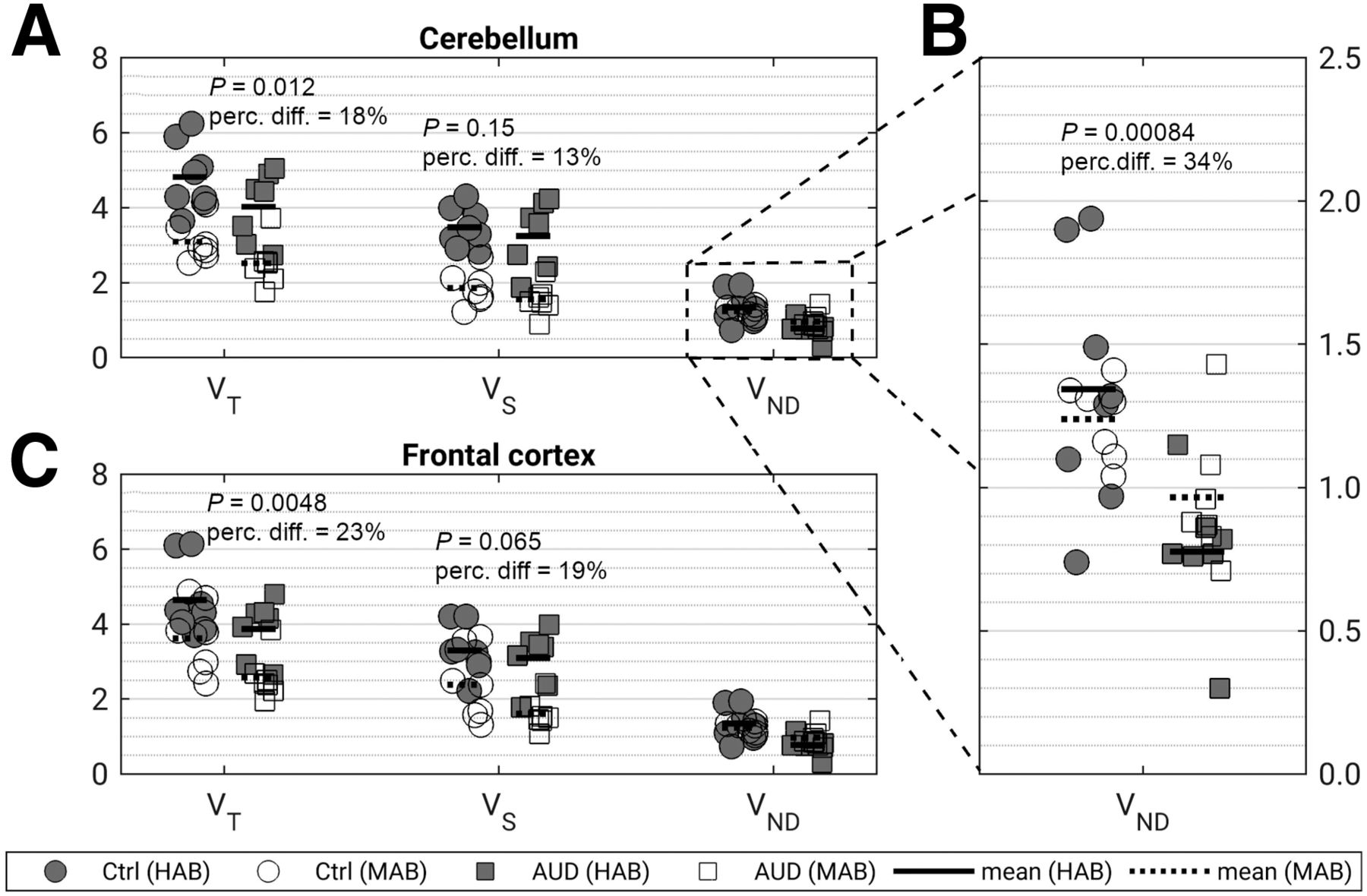
(A and C) Difference in outcome measures (VT, VS, and VND) between controls (Ctrl) and subjects with AUD in cerebellum (A) and frontal cortex (C). (B) Zoomed view of results for VND. P values and percentage difference (perc. diff.) between controls and patients are shown. HAB = high-affinity binder; MAB = mixed-affinity binder.
FEP
In the FEP dataset, VT was overall lower in patients than in controls (32%, P = 0.060 in the cerebellum; 36%, P = 0.045 in the frontal cortex). There was no significant difference in VND between patients and controls (P = 0.30). VS exhibited a larger percentage separation between patients and controls than that observed for VT in both the cerebellum (44%, P = 0.054) and the frontal cortex (57%, P = 0.033). The results are shown in Figure 3. The effect of genotype was statistically significant for VT in the cerebellum and frontal cortex (P = 0.011 and 0.017, respectively), for VND in the ▪▪▪ (P = 0.0043), and for VS in the frontal cortex (P = 0.017) but not in the cerebellum (P = 0.099).
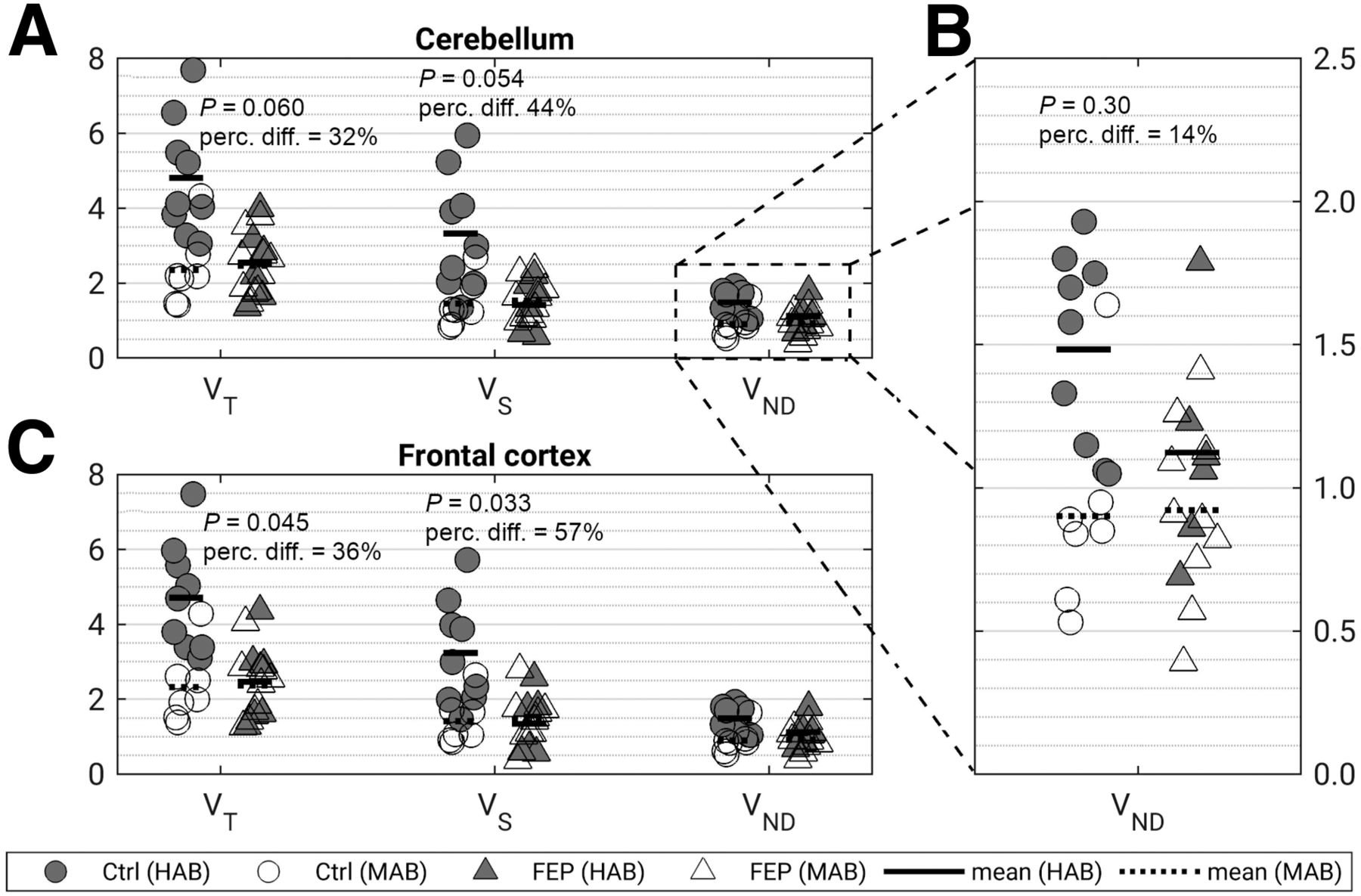
(A and C) Difference in outcome measures (VT, VS, and VND) between controls (Ctrl) and FEP patients in cerebellum (A) and frontal cortex (C). (B) Zoomed view of results for VND. P values and percentage difference (perc. diff.) between controls and patients are shown. HAB = high-affinity binder; MAB = mixed-affinity binder.
PD
In the PD dataset, we found no statistically significant difference in VT or VS between patients and controls, in either the cerebellum (P = 0.74 for VT, P = 0.11 for VS) or the striatum (P = 0.32 for VT, P = 0.42 for VS). VND was, however, lower in patients than in controls (34%, P = 0.0032). These results are shown in Figure 4. Across all outcome measures and ROIs, there was a significant effect of genotype (P = 0.012 for VND, P < 10−6 for VT and VS).

(A and C) Difference in outcome measures (VT, VS, and VND) between controls (Ctrl) and PD patients in cerebellum (A) and striatum (C). (B) Zoomed view of results for VND. P values and percentage difference (perc. diff.) between controls and patients are shown. HAB = high-affinity binder; MAB = mixed-affinity binder.
DISCUSSION
In this study, we used a new method to estimate VND in 4 clinical 11C-PBR28 datasets. We found that VND estimated with this method was lower in AUD and PD than in their matched controls, whereas no difference was found between FEP patients and their controls or in subjects before and after lipopolysaccharide injection. This was, to our knowledge, the first attempt to disentangle the extent by which differences in nondisplaceable binding may contribute to the observed differences in VT.
Lipopolysaccharide
Although leading to a pronounced increase in VT, administration of lipopolysaccharide had no apparent effect on SIME VND. Lipopolysaccharide is a useful model to study an acute immune response, and upregulation of TSPO has been observed in vivo in several species, including mice (13), rats (14), pigs (15), and nonhuman primates (16). When using VS as an outcome measure, we observed a larger percentage separation between the pre- and postlipopolysaccharide scans, with mean differences of 59% and 66% in the cerebellum and frontal cortex, respectively, and with variability similar to that of VT (coefficient of variation [SD/mean] was 0.85 for VT and 0.86 for VS). This higher percentage difference occurred because VND is not affected by the challenge. In a scenario in which VND is unaffected by a particular disease, and VT consists of one third of VND and two thirds of VS, a 50% difference in specific TSPO binding translates to only a 33% difference in VT. In such a scenario, though the effect sizes might likely be the same, it follows that changes in VS more directly reflect changes in TSPO densities, whereas changes in VT are attenuated by the contribution from VND.
AUD
Both VT and VND were lower in AUD subjects than in their age-matched controls, with a similar trend in VS. This finding may explain a previous report in which mixed-affinity binders with AUD had a lower 11C-PBR28 VT than mixed-affinity binder controls across several brain regions, whereas no difference was seen in high-affinity binders (17), since VND composes a larger fraction of VT in mixed-affinity binders than in high-affinity binders. In a separate cohort, Kalk et al. reported a lower 11C-PBR28 hippocampal VT in alcohol-dependent subjects than in controls, across both genotypes (18). In the present analysis, although some of the differences in VT between AUD and controls were ascribed to differences in VND, frontal cortex VS still showed a sizeable (albeit nonsignificant) percentage difference between AUD subjects and their controls. We can only speculate why VND would be lower in AUD subjects; pharmacologic competition studies in this population would be needed to conclusively establish levels of specific and nondisplaceable radiotracer uptake. Chronic alcohol exposure induces brain tissue atrophy, reduces cerebral perfusion, and accelerates aging (19,20). Including gray matter volume as a covariate in the statistical analysis did not change the results, indicating that the findings are not driven by partial-volume effects (Supplemental Table 12). Age-related alterations in tissue composition have been proposed as an explanation for differences in VND observed with the 5-hydroxytryptamine receptor 2A ligand 18F-altanserin (21). Although these questions remain unanswered, the findings here reported illustrate how separation of VND and VS could change the interpretation of results from TSPO PET studies.
FEP
Patients with FEP had SIME VND estimates similar to those of their matched controls. Frontal cortex VT and VS values were lower in patients. Using VS as an outcome measure resulted in a larger percentage difference between the groups. Most previous TSPO PET studies of FEP and schizophrenia have found no significant differences in VT (22–24), whereas a recent metaanalysis, which pooled PET data from 5 studies on psychosis and schizophrenia using second-generation TSPO radioligands (152 subjects in total), found strong evidence for lower VT values in patients than in controls (25). If VS had been used as the outcome measure in previous TSPO PET studies of FEP and schizophrenia, it is possible that the power to detect the population effect of a lower TSPO also in the individual samples of patients would have been higher.
PD
We found that SIME VND was lower in PD patients than in controls, but we observed no significant differences in VT, consistent with findings in TSPO PET studies using another second-generation radioligand (26,27). One study, using 11C-PK11195 and a basis-function implementation of the simplified reference tissue model, found a higher BPND in PD patients than in controls (28). Since BPND is defined as VS/VND, and given our findings, it is possible that the higher BPND reported in the 11C-PK11195 study was due to lower nondisplaceable binding rather than higher specific binding. This possibility illustrates that VND is a potential confounding factor not only in studies using VT as an outcome measure but also in those reporting BPND. By using ratio-based methods to provide BPND in TSPO PET studies, one may mistakenly interpret a decrease in VND as an increase in TSPO binding. Similar to the finding in the AUD dataset, PD might be associated with increased global atrophy (29), and it is possible that altered tissue composition could explain the lower VND in PD patients. Further studies are required to establish the reason for this observed group difference.
Effect of VND on Genotype
We observed a pronounced effect of genotype on SIME VND in both the FEP and the PD datasets but not in the AUD data. The observed effect, if true, complicates interpretation of our current understanding of the TSPO polymorphism, by implicating effects both on the tracer’s affinity to TSPO and on nondisplaceable uptake. When all the controls in this study were pooled, a difference in VND between genotypes was quite evident (P = 0.00016). We identify 3 potential interpretations for this observation. One possibility is that SIME-derived estimates of VND are artefactually contaminated by estimates of VS, so that high specific binding results in an overestimation of VND. However, this spillover across compartments has previously been tested and discarded using simulations (7). This finding is also supported by the lipopolysaccharide experiment, in which increased VS is not reflected in VND. A second interpretation is that the higher affinity of the radioligand in high-affinity binders leads to a higher nondisplaceable binding because equilibrium conditions are achieved at a later time for a high-affinity versus a low-affinity radioligand. The same mechanisms could potentially lead to higher nondisplaceable tracer binding in high-target-density brain regions than in regions with low target densities. For 11C-raclopride, it has been suggested that regional differences in observed occupancy could in fact be attributable to spatially varying nondisplaceable uptake (30,31). The third possibility is that SIME-derived VND estimates are affected by other features, which are, in turn, dependent on the genotype. For instance, it has previously been shown that VND estimated with SIME may be sensitive to the shapes of the arterial input function (32). The fact that input functions may differ between genotypes has been shown for both 11C-PBR28 (7) and the TSPO SPECT radioligand 123I-CLINDE (33), as is to be expected from the different levels of binding to TSPO in peripheral tissue (34). Irrespective of cause, estimates of VND (and, as a consequence, of BPND) may not be directly comparable across genotype groups, and their difference could itself be a confounder in clinical studies if the cohort is not balanced across genotypes. The datasets included in this study, however, are well balanced across genotypes; as such, a potential influence of differences in VND estimates is unlikely. Pharmacologic competition data would be needed to conclusively establish any effect of genotype on VND. However, previous 11C-PBR28 blocking studies have included only high-affinity-binder individuals (35) and therefore cannot provide insights into potential differences between genotypes.
Limitations
For any arterial input model, including SIME, VND estimates are sensitive to the input function shape. Further, similar to reference-tissue modeling, we did not consider spatial variations in VND. SIME was additionally executed on a larger set of ROIs, which resulted in close-to-identical findings (Supplemental Table 13). Yet, a formal procedure on how to establish a suitable ROI set for estimation of VND remains to be investigated.
CONCLUSION
Our findings suggest that VND may be a potential confounding factor in 11C-PBR28 PET studies. This outcome warrants further studies to establish the observed VND differences and, if possible, reveal their causes. We recommend the use of VS as an additional outcome parameter in TSPO PET studies since this measure more directly reflects binding to TSPO.
DISCLOSURE
Martin Schain was supported by a NARSAD young investigator grant from the Brain & Behavior Research Foundation. Pontus Plavén-Sigray was supported by the Lundbeck Foundation and the Swedish Society for Medical Research. Ansel Hillmer was supported by NIH grant K01AA024788. Simon Cervenka was supported by Swedish Research Council grant 523-2014-3467. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is nondisplaceable binding a confounding factor in 11C-PBR28 PET studies?
PERTINENT FINDINGS: Nondisplaceable uptake was estimated for 4 11C-PBR28 PET datasets. In 2 of these (AUD and PD) there was a significant difference in nondisplaceable uptake between patients and controls.
IMPLICATIONS FOR PATIENT CARE: The possibility of obtaining estimates of specific binding to TSPO may improve the interpretability of nuclear imaging studies addressing the role of neuroinflammation in several disorders.
Acknowledgments
The Karolinska Schizophrenia Project consortium consists of Lars Farde, Lena Flyckt, Göran Engberg, Sophie Erhardt, Helena Fatouros-Bergmann, Simon Cervenka, Lilly Schwieler, Fredrik Piehl, Ingrid Agartz, Karin Collste, Pauliina Victorsson, Anna Malmqvist, Mikael Hedberg, and Funda Orhan.
Footnotes
Published online Jul. 17, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 17, 2020.
- Accepted for publication June 23, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.