


Abstract
Microbial culture is the gold standard for determining the effectiveness of tuberculosis treatment. End-of-treatment (EOT) 18F-FDG PET/CT findings are variable among patients with negative microbial culture results after completing a standard regimen of antituberculous treatment (ATT), with some patients having a complete metabolic response to treatment whereas others have residual metabolic activity (RMA). We herein determine the impact of findings on EOT 18F-FDG PET/CT on tuberculosis relapse in patients treated with a standard regimen of ATT for drug-sensitive pulmonary tuberculosis (DS-PTB). Methods: Patients who completed a standard regimen of ATT for DS-PTB and were declared cured based on a negative clinical and bacteriologic examination were prospectively recruited to undergo EOT 18F-FDG PET/CT. Images were assessed for the presence of RMA. Patients were subsequently followed up for 6 mo looking for symptoms of tuberculosis relapse. When new symptoms developed, relapse was confirmed with bacteriologic testing. Repeat 18F-FDG PET/CT was done in patients who relapsed. Results: Fifty-three patients were included (mean age, 37.81 ± 11.29 y), with 62% being male and 75% HIV-infected. RMA was demonstrated in 33 patients (RMA group), whereas 20 patients had a complete metabolic response to ATT (non-RMA group). There was a higher prevalence of lung cavitation in the RMA group (P = 0.035). The groups did not significantly differ in age, sex, presence of HIV infection, body mass index, or hemoglobin level (P > 0.05). On follow-up, no patients in the non-RMA group developed tuberculosis relapse. Three patients in the RMA group developed relapse. All patients who developed tuberculosis relapse had bilateral disease with lung cavitation. Conclusion: A negative EOT 18F-FDG PET/CT result is protective against tuberculosis relapse. Nine percent of patients with RMA after ATT may experience tuberculosis relapse within 6 mo of completing ATT. Bilateral disease with lung cavitation is prevalent among patients with tuberculosis relapse.
An estimated 1.7 billion people are infected with Mycobacterium tuberculosis globally, the microbial agent responsible for tuberculosis (1). About 3%–10% of these individuals harboring Mycobacterium tuberculosis in the form of latent tuberculosis will develop symptomatic tuberculosis in their lifetime. Tuberculosis is treated with multiple drugs for an extended period. For drug-sensitive pulmonary tuberculosis (DS-PTB), drug treatment is administered for 6 mo. The long duration of treatment with multiple drugs increases the risk of treatment-related side effects, drug–drug interaction, treatment nonadherence, and the development of drug resistance (2,3). In recent times, many studies have been performed to identify more effective chemotherapy agents that can be administered for shorter durations (4,5). Inadequate treatment through use of a less effective regimen or too short a duration leads to relapse. About 5% of patients with DS-PTB will experience relapse within 6 mo of completing treatment with a standard 6-mo antituberculous treatment (ATT), whereas up to 20% of patients treated with a 4-mo regimen may experience relapse (6,7). Tuberculosis relapse is caused by persisting slow-growing, metabolically active but nonculturable bacilli that are less sensitive to chemotherapy agents (8,9). It is crucial to have noninvasive biomarkers that are reliable in assessing sterilizing cure after ATT. The currently available biomarkers are not able to do this with acceptable accuracy.
PET/CT using 18F-FDG is a useful imaging modality more popular for its oncologic use. Accumulation of 18F-FDG, an analog of glucose, at sites of infection such as tuberculous granuloma is due to the high consumption of glucose by activated macrophages, the most abundant inflammatory cell in the granuloma. Our group and others have shown the clinical utility of 18F-FDG PET/CT in predicting response to ATT and in assessing response to ongoing treatment in patients with pulmonary and extrapulmonary tuberculosis (10–16). Accumulation of 18F-FDG in tuberculous lesions has been shown to correlate with the number of bacilli present (17). There is a lack of data on the significance of end-of-treatment (EOT) 18F-FDG PET/CT findings in predicting tuberculosis relapse after the completion of ATT. Robust data on the predictive ability of EOT 18F-FDG PET/CT may prove useful in the application of EOT 18F-FDG PET/CT as a noninvasive imaging tool in the development of more effective antituberculous chemotherapy for shorter durations. We hypothesized that patients who show residual metabolic activity (RMA) on EOT 18F-FDG PET/CT will be at increased risk of relapse of tuberculosis within 6 mo of completing a standard course of ATT for DS-PTB. In this study, we aimed to determine the impact of the findings on EOT 18F-FDG PET/CT on tuberculosis relapse in patients with DS-PTB treated with a standard 6-mo regimen of ATT.
MATERIALS AND METHODS
Patients
This is a report on the 18F-FDG PET/CT imaging component of a prospective study evaluating imaging patterns from 18F-FDG PET/CT scans, transcriptomic and proteomic biosignatures, cell subset analysis, cytokine and chemokine patterns, and other nonspecific inflammatory markers as potential biomarkers of successful eradication of tuberculous disease and infection and for predicting the risk of persistence or relapse after treatment completion. We recruited patients who completed a standard 6-mo regimen of ATT for confirmed DS-PTB in clinics within Tshwane District. Participants were identified from the AitaHealth database managed by the Department of Family Health at the University of Pretoria. The primary care doctors at the participating clinics determined that prospective participants had completed a full course of treatment for DS-PTB as per South African guidelines (18). Inclusion criteria were known HIV infection status, age 18–65 y, GeneXpert (Cepheid)-positive at the start of treatment and culture-confirmed susceptible to first-line tuberculosis drugs, available pretreatment isolate, completion of the full course of treatment for DS-PTB and needing no further treatment (as deemed by the primary care physician), and residence in a household recorded on the AitaHealth database. Exclusion criteria were unknown HIV status, previous tuberculosis within 3 y of the index infection, positive sputum on Xpert (Cepheid) or culture at the end of treatment, any documented tuberculosis drug resistance, presence of tuberculosis symptoms, signs or symptoms of acute illness, diagnosis of malignancy, lack of feasibility of 6-mo follow-up after treatment, receipt of any investigational products or drug in the preceding 6 mo or of any investigational vaccine ever, receipt of an incomplete or nonstandard tuberculosis drug regimen, any clinical condition requiring systemic steroid or other immunosuppressive medication in the preceding 6 mo, uncontrolled diabetes mellitus, pregnancy or breastfeeding, anemia (hemoglobin < 7 g/dL), and a significant smoking history (>30 pack-years). All patients gave written informed consent to participate in the study. The human research ethics committees at the University of Pretoria and Sefako Makgatho Health Sciences University approved the study.
EOT Assessments
On completion of treatment, all study participants had the following assessments done: clinical history and physical examination, sputum microscopy for acid-fast bacilli, GeneXpert/RIF (Cepheid), culture and drug sensitivity testing, HIV screening, urinary pregnancy testing, and 18F-FDG PET/CT.
18F-FDG PET/CT Imaging and Analysis
All study participants had 18F-FDG PET/CT done within 14 d of treatment completion at the Department of Nuclear Medicine, Steve Biko Academic Hospital, the University of Pretoria, between December 2017 and September 2018. A minimum of 6 h of fasting was observed, and fasting blood glucose was less than 7 mmol/L in all participants. The activity of 18F-FDG administered was weight-based using the following formula: [(body weight ÷ 10) + 1] × 37 MBq. We performed a vertex to mid thigh unenhanced CT scan followed by PET imaging on a Biograph 40 TruePoint hybrid PET/CT scanner (Siemens Medical Solutions) after a 60-min uptake time. We performed PET imaging in 3 dimensions at 3 min per bed position. We reconstructed PET data using ordered-subset expectation-maximization iterative reconstruction (4 iterations, 8 subsets) with a gaussian filter applied at 5.0 mm in full width at half maximum.
We performed image analysis and interpretation on a dedicated workstation equipped with Syngo.Via software (Siemens Medical Solutions). Two nuclear physicians with 6 and 12 y of experience reading 18F-FDG PET/CT scans for inflammation and infection interpreted the images independently. Areas of disagreement were resolved by consensus. We performed qualitative image interpretation. Any focal lung uptake greater than mediastinal background activity was considered significant RMA after treatment. On this basis, patients were classified as being in the RMA group if they had RMA on EOT 18F-FDG PET/CT and in the non-RMA group if they had a complete metabolic response to ATT (i.e., no significant RMA).
Patient Follow-up
Community health workers visited all study participants at their home every month for 6 mo after completion of treatment. During home visits, patients were assessed for symptoms of tuberculosis. Patients were counseled to visit or call the study center should they fall sick. At 3 and 6 mo after completion of treatment, participants visited the study center for tuberculosis symptom screening; collection of expectorated sputum samples for microscopy, GeneXpert analysis, and microbial culture; and updating of phone number and residential address.
Participants who experienced symptoms of tuberculosis were reevaluated as follows: medical history; physical examination; repeat point-of-care HIV testing; and microscopy, GeneXpert, microbial culture, and drug-sensitivity testing of expectorated sputum samples. Their consent was obtained for repeat 18F-FDG PET/CT, which was performed within 14 d of confirmation of tuberculosis relapse. Patient preparation, imaging parameters, and interpretation of repeat 18F-FDG PET/CT were as for EOT 18F-FDG PET/CT.
Statistical Analysis
Descriptive statistics as absolute and relative frequencies, mean, and SD were used to characterize the study population. The non-RMA and RMA groups were compared using an unpaired t test or a χ2 test, depending on whether the parameters were discrete or continuous variables, respectively. Statistical analysis was done using MedCalc. Statistical significance was set at a P value of less than 0.05.
RESULTS
In total, 53 patients were included (33 male and 20 female), with a mean age of 37.81 ± 11.29 y. There were 18 smokers (33.96%). Forty participants were HIV-positive, with a median CD 4 count of 267 cells/μL (range, 14–670 cells/μL) and a median viral load of 12,500 copies/μL (range, 41–398,238 copies/μL). Table 1 shows the detailed baseline characteristics of the participants.
Baseline Characteristics of Study Participants (n = 53)
18F-FDG PET/CT Findings
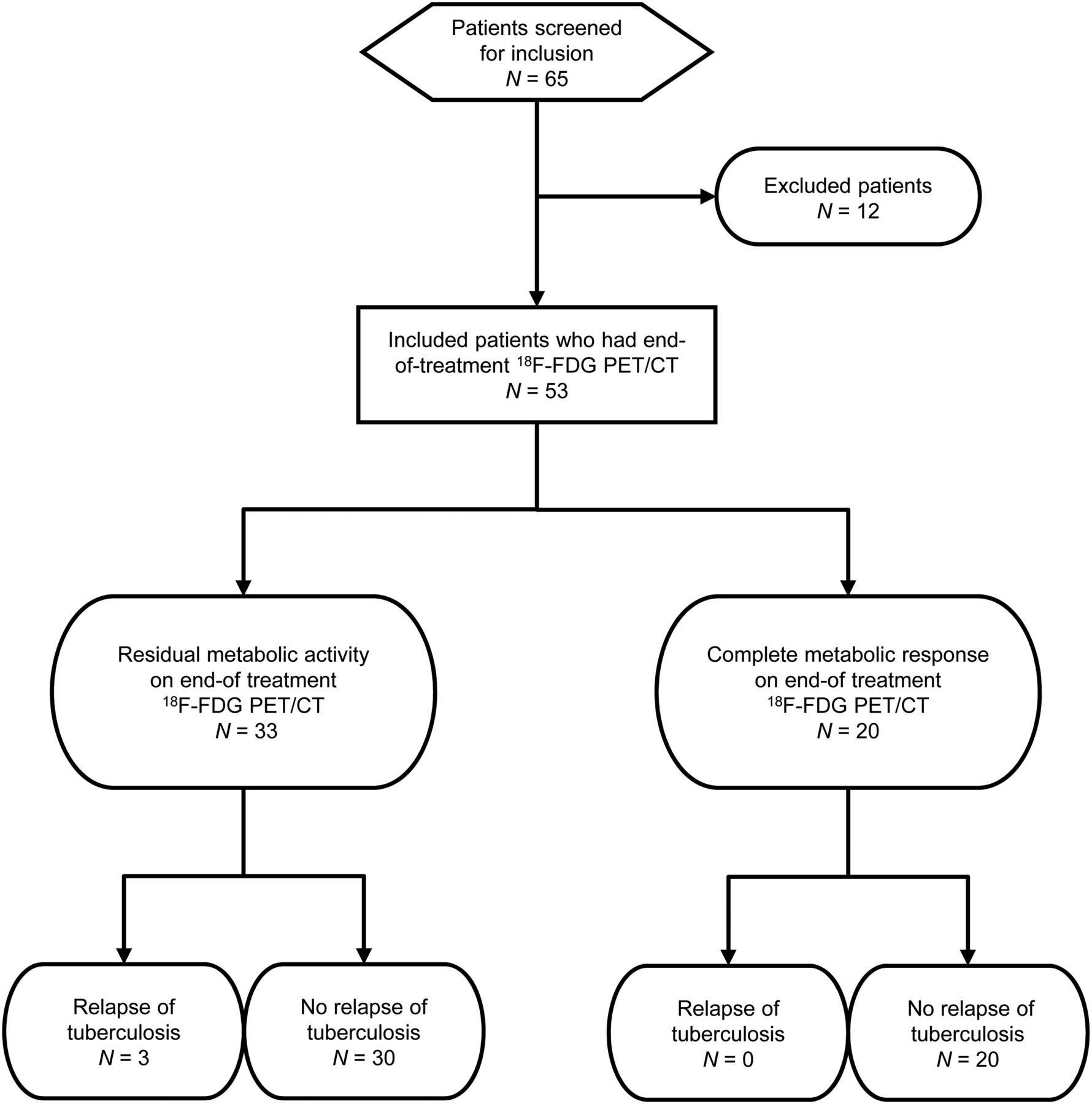
Thirty-three patients had RMA, and 20 patients had a complete metabolic response to ATT (non-RMA) (Fig. 1). We found a higher preponderance of cavitation among patients with RMA than among those without (18/33 vs. 5/20, P = 0.035). Other characteristics, including body mass index (BMI), C-reactive protein levels, hemoglobin levels, history of HIV infection, CD 4 count level, viral load level, and smoking history, did not significantly differ between the RMA group and the non-RMA group. Table 2 shows the significance of the various parameters compared between the 2 groups.

Flowchart showing selection of study participants and outcomes.
Comparison Between Patients with RMA and Those with Complete Metabolic Response to Tuberculosis Treatment on EOT 18F-FDG PET/CT
Relapse
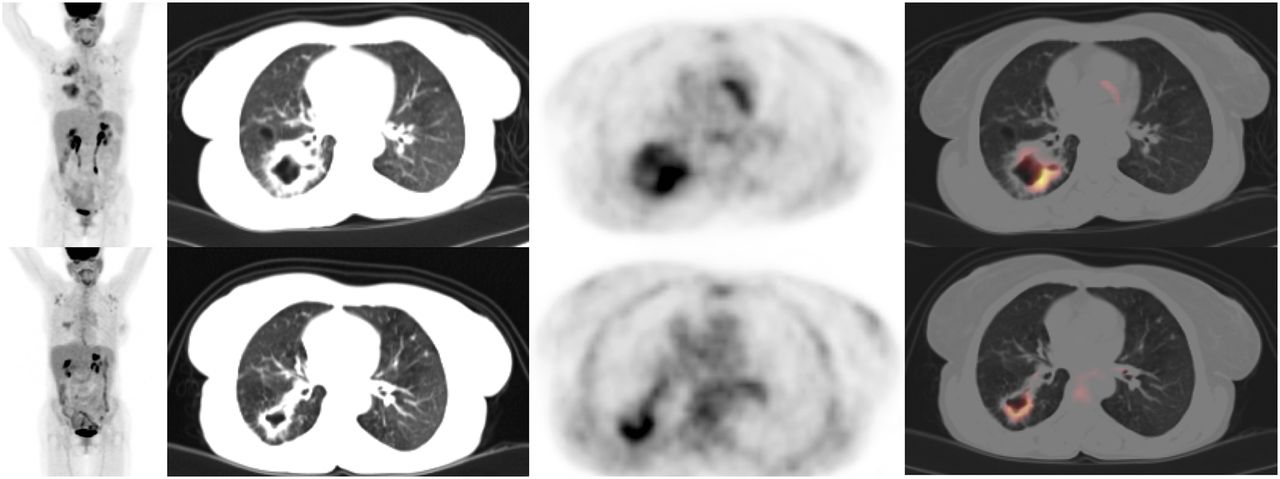
All study participants have completed a 6-mo follow-up. No participants in the non-RMA group experienced tuberculosis relapse. During follow-up, 3 participants in the RMA group developed symptoms of pulmonary tuberculosis (Table 3). Relapse of tuberculosis was confirmed on repeat microbial culture. All patients who experienced tuberculosis relapse were treated for tuberculous disease that involved both lungs and was associated with lung cavitation. The first patient who relapsed did so after 4 mo on follow-up. He was a 65-y-old male smoker, underweight and HIV-uninfected (Fig. 2). The second patient relapsed after 5 mo on follow-up. She was a 48-y-old HIV-infected female (Fig. 3). The third patient relapsed at 6 mo after completion of ATT. She was a 54-y-old underweight female who was HIV-infected (Fig. 4). In all 3 patients with relapse, follow-up 18F-FDG PET/CT localized sites of relapse to areas of RMA on the EOT 18F-FDG PET/CT.
Summary Characteristics of Patients Who Relapsed During 6-Month Follow-up

EOT (top row) and follow-up (bottom row) 18F-FDG PET/CT images of patient 1, 65-y-old male smoker, HIV-uninfected with RMA in right lung. He developed symptoms of tuberculosis relapse 4 mo after completion of treatment. Relapse was confirmed by positive microbial culture. Follow-up 18F-FDG PET/CT images obtained after confirmation of tuberculosis relapse localized site of recurrence to previously identified area of RMA.

EOT (top row) and follow-up (bottom row) 18F-FDG PET/CT images of patient 2, 48-y-old HIV-infected woman who developed tuberculosis relapse at 5 mo after completion of ATT. RMA is seen in left lung on EOT images. Relapse occurred at same site as demonstrated on follow-up 18F-FDG PET/CT done for tuberculosis relapse.

EOT (top row) and follow-up (bottom row) 18F-FDG PET/CT images of patient 3, 54-y-old HIV-infected woman with intense RMA seen in thick wall of right lung cavity on EOT 18F-FDG PET/CT. On relapse, which occurred at 6 mo after completion of treatment, metabolic activity remained in wall of right lung cavitation, suggesting tuberculosis relapse at this site.
DISCUSSION
We evaluated the association between the findings on EOT 18F-FDG PET/CT and tuberculosis relapse in patients with DS-PTB who completed a standard 6-mo regimen of ATT and found no relapse after a 6-mo follow-up in patients who achieved complete metabolic response to ATT. About two thirds of our study cohort had RMA after treatment. Three patients of those with RMA experienced disease relapse during follow-up, representing a relapse rate of about 6% of total patients included in this study. Our results show that a negative 18F-FDG PET result (complete metabolic response) at the end of treatment has an excellent negative predictive value and may indicate a sterilizing cure in the management of tuberculosis. This shows that 18F-FDG PET/CT holds potential for use to determine the adequacy of chemotherapy in the management of tuberculosis and, consequently, for use as a noninvasive surrogate to evaluate the efficacy of antituberculous drugs in new-drug development and in experiments designed to determine optimum treatment duration.
In our study, only 3 patients developed tuberculosis relapse, representing 1 in 11 patients with RMA on EOT 18F-FDG PET. 18F-FDG uptake has been reported in lesions considered by morphologic imaging to represent old healed tuberculous lesions (19). Antituberculous drugs are most sensitive against rapidly replicating bacilli; hence, during treatment the rapidly replicating bacilli are quickly eliminated, leaving behind a subpopulation of slow-growing or dormant bacilli (8). The slow-growing bacilli do not grow readily on culture media, giving rise to a negative culture with a false assessment of a sterilizing cure. Persisting slow-growing bacilli are metabolically active and stimulate a host immune response, accounting for the 18F-FDG avidity seen in lesions after completion of ATT (9,20). The presence of replicating bacilli in metabolically active residual lung lesions in patients with a negative culture at the end of tuberculosis treatment was recently demonstrated in a large prospective study (21). Messenger RNA of Mycobacterium tuberculosis was demonstrated in the bronchoalveolar lavage samples of patients who were considered cured on the basis of negative findings on clinical and bacteriologic examinations. Messenger RNA of Mycobacterium tuberculosis isolated from patients in this study indicates the presence of replicating bacilli, in contradistinction to DNA of Mycobacterium tuberculosis, which may be shed by dead bacilli (21). Lipid components of the mycobacterial cell can persist long after the death of the bacilli. These cell lipids are highly immunogenic, causing continued invasion of the residual lesion by activated inflammatory cells (22). The inflammation within these residual lesions causes trapping of 18F-FDG within them. To date, no consistent threshold for 18F-FDG uptake in a residual tuberculous lesion has been defined as representing the presence of viable bacilli from uptake stimulated by dead or dying bacilli.
About 75% of our study participants were HIV-infected and hence at increased risk of other pulmonary inflammatory and infectious diseases. 18F-FDG targets the host immune response to tubercle bacilli and is not specific for tuberculous lesions (23,24). The HIV-infected patients in this study were mostly on regular antiretroviral treatment. Also, chest radiography was routinely done at treatment onset (18), and a thorough clinical history and physical examination were done during patient recruitment to identify patients who may have malignant or other inflammatory or infective conditions that may confound 18F-FDG PET/CT interpretation. We speculate that the RMA seen in our study patients was mostly due to inflammation caused by persisting slow-growing live bacilli or the bacterial cell-wall component from dead bacilli. We acknowledge that it is essential to discriminate between these 2 causes of RMA in treated patients, a task that cannot be accomplished either by 18F-FDG or by other similar probes that target the host inflammatory response to Mycobacterium tuberculosis. A role may therefore exist in the future for the use of bacterium-specific imaging targeting the component of the live bacilli. Most antituberculous agents have been successfully labeled with radionuclides for noninvasive targeted imaging of animal models of tuberculosis (25,26). Targeted imaging with radiolabeled antituberculous drugs not only offers a highly specific modality for imaging of tuberculosis but also may find utility in drug development, as biokinetics may be studied noninvasively and at a lower cost (27).
Several factors have been implicated in the predisposition of patients to tuberculosis relapse, such as HIV infection, smoking, and a low body mass index (28–30). The 2 most consistent factors seen in all patients who experienced tuberculosis relapse in our study were bilateral disease and pulmonary cavitation. Two patients were of low body weight, and two were HIV-infected. Tuberculous cavities are avascular; hence, there is poor drug penetration into them and intense 18F-FDG uptake in their walls due to hypoxia-induced enhanced glycolysis. Cavities cause permanent lung parenchyma destruction and may serve as a suitable nidus for colonization by other pathogens, such as Aspergillus species. In all 3 patients with tuberculosis relapse, relapse occurred at the sites of RMA on EOT 18F-FDG PET/CT, suggesting relapse rather than new infection. The appearance of new sites of metabolic activity when tuberculosis symptoms recur after previous successful treatment does not entirely rule out relapse (as opposed to reinfection). In a mouse model of tuberculosis, Murawski et al. performed an 18F-FDG PET/CT study of the spatial evolution of tuberculosis disease through infection, response to treatment, and development of relapse (31). Most relapses occurred in lesions identified before treatment, whereas some de novo lesions also developed at disease relapse.
Our study has many strengths, including the strict entry criteria we applied in selecting patients. Only patients who had a positive culture at diagnosis were included. We screened patients before study entry to eliminate confounding factors. Also, we followed up patients, including home visits monthly to screen for relapse. This report is a substudy of a larger trial in which strain typing of the Mycobacterium tuberculosis pathogen causing primary infection and relapse was determined. We were therefore able to discriminate relapse from reinfection. This is particularly important in a tuberculosis-endemic region such as ours, where the chance of reinfection is relatively high. Our study also has some limitations. Only 6% of patients experienced disease relapse, in agreement with previous reports (6). This limited number was not sufficient to perform any rigorous statistical analysis to determine imaging and nonimaging characteristics predictive of tuberculosis relapse in patients with RMA on EOT 18F-FDG PET/CT. Follow-up in our study was limited to 6 mo. Relapse of tuberculosis is still possible beyond this time. We therefore could have underestimated the relapse rate of our study population. In fact, it is possible that, on a longer-term follow-up, more of the patients with RMA could have been found to experience relapse.
CONCLUSION
Patients with a complete metabolic response to ATT at the end of therapy are not at risk of disease relapse within the 6 mo after treatment completion. About 9% of patients with RMA at the end of ATT may experience relapse within 6 mo after treatment. Lung cavitation and bilateral disease are common characteristics of patients who experience tuberculosis relapse.
DISCLOSURE
This work was funded with grants received from RePORT Africa (OISE-16-62054) and the South African Medical Research Council (TB HIV Collaborating Centre). Ismaheel Lawal is a PhD student at the Department of Nuclear Medicine, University of Pretoria. He receives a monthly stipend from the Nuclear Medicine Research Infrastructure (NuMeRI) hosted at the Department of Nuclear Medicine, University of Pretoria. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What are the implications of EOT 18F-FDG PET/CT findings on disease relapse in patients treated with a standard regimen of antituberculous chemotherapy for DS-PTB?
PERTINENT FINDINGS: Complete metabolic response to ATT is a protective biomarker against tuberculosis relapse for 6 mo after treatment. About 9% of patients who have RMA in their lungs at the end of ATT will experience tuberculosis relapse within 6 mo of completing treatment. Cavitation and bilateral lung involvement are common features seen in patients who experience tuberculosis relapse.
IMPLICATIONS FOR PATIENT CARE: 18F-FDG PET/CT is a useful noninvasive method to assess treatment efficacy in tuberculosis management. Findings on EOT 18F-FDG PET/CT are a valuable biomarker for assessing treatment adequacy and are predictive of disease relapse.
Acknowledgments
We acknowledge the important contributions of Chris Hikuam of the South African Tuberculosis Vaccine Initiative and Jerrold Ellner and Emily Douglass of the Boston University Medical Centre. We also thank the members of staff of the Department of Medical Microbiology and MeCRU, Sefako Makgatho University of Medical Science, and the Department of Nuclear Medicine at the University of Pretoria and Steve Biko Academic Hospital, Pretoria.
Footnotes
↵* Contributed equally to this work.
Published online Aug. 26, 2019.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 12, 2019.
- Accepted for publication August 5, 2019.





{kind=link}
{kind=link}
{kind=link}
{kind=link}