


Abstract
Complete resection is the treatment of choice for most pediatric brain tumors, but early postoperative MRI for detection of residual tumor may be misleading because of MRI signal changes caused by the operation. PET imaging with amino acid tracers in adults increases the diagnostic accuracy for brain tumors, but the literature in pediatric neurooncology is limited. A hybrid PET/MRI system is highly beneficial in children, reducing the number of scanning procedures, and this is to our knowledge the first larger study using PET/MRI in pediatric neurooncology. We evaluated if additional postoperative 18F-fluoro-ethyl-tyrosine (18F-FET) PET in children and adolescents would improve diagnostic accuracy for the detection of residual tumor as compared with MRI alone and would assist clinical management. Methods: Twenty-two patients (7 male; mean age, 9.5 y; range, 0–19 y) were included prospectively and consecutively in the study and had 27 early postoperative 18F-FET PET exams performed preferentially in a hybrid PET/MRI system (NCT03402425). Results: Using follow-up (93%) or reoperation (7%) as the reference standard, PET combined with MRI discriminated tumor from treatment effects with a lesion-based sensitivity/specificity/accuracy (95% confidence intervals) of 0.73 (0.50–1.00)/1.00 (0.74–1.00)/0.87 (0.73–1.00) compared with MRI alone: 0.80 (0.57–1.00)/0.75 (0.53–0.94)/0.77 (0.65–0.90); that is, the specificity for PET/MRI was 1.00 as compared with 0.75 for MRI alone (P = 0.13). In 11 of 27 cases (41%), results from the 18F-FET PET scans added relevant clinical information, including one scan that directly influenced clinical management because an additional residual tumor site was identified. 18F-FET uptake in reactive changes was frequent (52%), but correct interpretation was possible in all cases. Conclusion: The high specificity for detecting residual tumor suggests that supplementary 18F-FET PET is relevant in cases where reoperation for residual tumor is considered.
Central nervous system tumors are the most common solid tumors in childhood, with the highest incidence of cancer-related death in children and adolescents (1,2). Moreover, severe late effects of tumor and its treatment are frequently seen in this group (3). If possible, complete resection is the primary treatment for most tumor types, and it is widely accepted that the degree of resection has a significant impact on prognosis (4–6). MRI 0–72 h after surgery is the current method of choice for assessing the degree of resection. However, signal changes on postoperative MRI can also be caused by tissue reaction to surgery; for example, bleeding, hemostatic adsorbents, inflammation, edema, ischemia, or signal artifacts from metal implants can disturb the MRI interpretation. Addition of PET imaging may help differentiate residual tumor from postoperative changes. Although brain tumor imaging using the glucose analog 18F-FDG is hampered by a high physiologic uptake in gray matter, imaging with amino acid analogs such as 11C-methionine, 18F-fluoro-phenylalanine, or 18F-fluoro-ethyl-tyrosine (18F-FET) has been shown to delineate tumor tissue from normal brain tissue with a high accuracy, especially in non–contrast-enhancing lesions (7–10), and residual PET tracer uptake after operation predicts shorter survival in high-grade gliomas (11). However, significant uptake of amino acid analogs can also be observed in nonneoplastic and acute inflammatory lesions (12).
Several studies in adults found an increased sensitivity for residual tumor after surgery for glioblastoma using 18F-FET PET compared with MRI (13,14). Tscherpel et al. reported valuable diagnostic information of brain stem and spinal cord imaging using 18F-FET PET (15). In children, only 2 retrospective studies are available. A high clinical value of postoperative 11C-methionine or 18F-FDG PET was found in 20 pediatric patients with possible residual tumor (16), and Dunkl et al. reported agreement between MRI and 18F-FET PET findings postoperatively in another 10 children (17).
Using a hybrid PET/MRI system is preferable in children to reduce the number of scanning procedures. We evaluated the added clinical value of postoperative 18F-FET PET in children and adolescents after surgery for a brain or spinal cord tumor if possible using simultaneous acquisition in a hybrid PET/MRI system. Further, we analyzed if 18F-FET PET/MRI showed increased sensitivity, specificity, and accuracy for detecting residual tumor as compared with MRI alone. We hypothesized a higher sensitivity, specificity, and accuracy for the detection of residual tumor, which could assist a difficult clinical decision on whether to reoperate as well as the delineation of tumor or the identification of additional tumor lesions.
MATERIALS AND METHODS
The study is part of a larger study of 18F-FET PET/MRI on primary central nervous system tumors in children and adolescents in various clinical situations. The study was approved by the regional ethical committee (approval H-6-2014-095) and registered at clinicaltrials.gov (NCT03402425).
Patient Inclusion
Inclusion criteria were diagnosis of a central nervous system tumor before the age of 18 y and planned partial or total resection of the tumor. In the study period from March 2015 to October 2017, 28 children and adolescents were included prospectively and consecutively, and written informed consent was provided by all patients or their parents (in patients < 18 y). Six patients were excluded (because of discontinuation of the PET scan, unsuccessful tracer production, or preoperative 18F-FET PET showing no tracer uptake in tumor), leaving 22 children and adolescents (Table 1) with a total of 27 18F-FET PET scans performed early after surgery (median, 48 h; range, 1–15 d), as 5 patients had a reoperation. Anesthesia was necessary in 8 cases. When possible, preoperative 18F-FET PET/MRI was also performed (n = 18). During the study period, another 30 operations for a primary pediatric brain tumor were performed without inclusion in the study because of parents or child declining inclusion (n = 4), unavailability of anesthesia (n = 13), emergency surgery (n = 4), social problems (n = 4), or other reasons (n = 5).
Results of Early Postoperative 18F-FET PET and MRI in Children and Adolescents Undergoing Central Nervous System Tumor Surgery
Imaging
The MRI protocol for the hybrid PET/MRI system 3-T Siemens Biograph mMR included a 3-dimensional T1 magnetization-prepared rapid gradient echo sequence before and after contrast agent; T2 fluid-attenuated inversion recovery, diffusion weighted imaging; and T2 BLADE (proprietary name for periodically rotated overlapping parallel lines with enhanced reconstruction in MR systems from Siemens Healthcare). Supplemental Table 1 provides a detailed description of the MRI protocol (supplemental materials are available at http://jnm.snmjournals.org). Three postoperative scans and 9 preoperative scans were performed on standalone MRI systems at the Department of Diagnostic Radiology at Copenhagen University Hospital Rigshospitalet or the Department of Radiology at University Hospital Odense using similar protocols.
A 40-min dynamic PET emission scan in list mode was obtained using the PET/MRI system (n = 24) or a Biograph TruePoint PET/CT (n = 3) (Siemens) initiated simultaneously with a 3 MBq/kg injection of 18F-FET preceded by 4 h of fasting for proteins. To ensure compliance, 2 patients had the scan time reduced. An overview of hybrid PET/MRI protocols for brain or spinal tumors was previously published by Henriksen et al. (18). The static PET images (20–40 min after injection) were reconstructed into a 344 × 344 matrix (voxel size, 0.8 × 0.8 × 2 mm) using 3-dimensional iterative ordered-subset expectation maximization (4 iterations, 21 subsets) and applying a 5-mm gaussian filter. Low-dose CT of the brain (120 kV, 30 mAs, 5-mm slice width) was used for attenuation correction obtained on a separate PET/CT scanner (19). The spinal cord acquisitions were attenuation-corrected with standard MRI-based attenuation maps derived using the Dixon sequence (20). Movement registration during the scan was performed as described previously (18).
Image Analysis
The PET data were evaluated as part of daily routine by a nuclear medicine specialist experienced with neurooncology using a Leonardo workstation (Siemens). The static PET image was evaluated for 18F-FET uptake in tumor relative to unaffected gray matter as described previously (17). In short, the background 18F-FET activity uptake was estimated as the average activity concentration in a large cortical region at the level of the centrum semiovale. The maximal tumor-to-background ratio was estimated and the tumor delineated with a threshold for metabolic activity in tumor of 1.6 times the background (21). For spinal tumors, interpretation was based on visual analysis only as no cortical background region was available. For dynamic analysis, a volume of interest (0.2–0.6 cm3) was defined at the static image and transferred to the entire dynamic dataset to extract the time–activity curve. The curve pattern was rated as type 1 (steady increasing, benign lesion or low grade), type 2 (plateau after 20–40 min, intermedium), or type 3 (decreasing after an early peak < 20 min, malignant) as defined previously (17,22,23). The discrimination between postoperative treatment changes and active disease was an integrated decision based on all available information including the preoperative scan if available and the combined evaluation of PET and MRI, as described in the practice guidelines for amino acid PET imaging of gliomas (24). Reactive changes were deemed more likely when maximal tumor-to-background ratio was less than 2.0, curve pattern was type I, uptake was outside the preoperative tumor border, diffuse uptake was along the cortex or the margin of the resection cavity, or uptake was in areas of vascular structures or postoperative changes on MRI, including hemorrhages or infarcts. An additional masked reading was performed by a nuclear medicine specialist experienced with neurooncology to assess the interrater variability.
Evaluation
The added clinical value of the PET scan was assessed at a weekly multidisciplinary childhood central nervous system tumor board. Initially, possible residual tumor was assessed from MRI by neuroradiologists experienced with pediatric brain tumors, and a treatment plan was decided while masked to the results of 18F-FET PET. It was rated whether the MRI was sufficient for deciding the treatment plan or whether a supplementary 18F-FET PET scan was warranted, for example, because of equivocal MRI. Subsequently, the results from the 18F-FET PET imaging were revealed, and it was rated whether the 18F-FET PET scan had no impact, added new information (e.g., residual tumor mass, different tumor borders), or influenced clinical management. These initial scorings was corroborated at later review meetings between clinicians, a neuroradiologist experienced in pediatric neurooncology, and a nuclear medicine specialist to ensure the validity.
As biopsy or reoperation to remove possible residual tumor was performed only if this procedure was clinically indispensable, the existence of residual tumor was histologically confirmed only in 2 cases by immediate reoperation and in the remaining cases by clinical follow-up and MRI. In equivocal cases (n = 12), the final assessment of possible residual tumor was based on a consensus multidisciplinary evaluation of the course of disease.
Statistics
Sensitivities, specificities, and accuracies between MRI alone and PET/MRI were compared using McNemar testing based on the exact binomial distribution. To correct for a possible correlation between lesions belonging to the same patient, an additional nonparametric permutation test was performed. Bootstrap confidence intervals were computed by resampling patients 50,000 times. However, as the specificity of PET/MRI was found to be 100%, a confidence interval was obtained from the binomial distribution using the number of patients as a conservative estimate of the effective sample size. A Fisher exact test was used to test for significant differences of tracer uptake in reactive changes after 24 h versus later. All analyses were performed with R statistical software, version 3.4.1. Interrater variability was assessed with Cohen κ.
RESULTS
Diagnostic Accuracy
Table 1 shows the results. None of the PET scans were rated necessary for clinical decision making; that is, no clinically relevant information from the PET scan was prospectively anticipated. This rating was due to the lack of expected clinical consequences, as reoperation was not relevant in the 2 scans with equivocal MRI. In 14 (52%) cases, the patient had residual tumor based on immediate reoperation or follow-up leading to a sensitivity/specificity/accuracy of 0.79/0.92/0.85 for MRI alone and 0.71/1.00/0.85 for PET/MRI. Four subjects had more than one evaluated lesion, and the lesion-based sensitivity/specificity/accuracy with 95% confidence intervals can be found in Table 2. Figure 1 shows an example of a patient with more than one evaluated lesion.
Lesion-Based Outcome Parameters Corrected for Multiple Lesions Within Each Subject
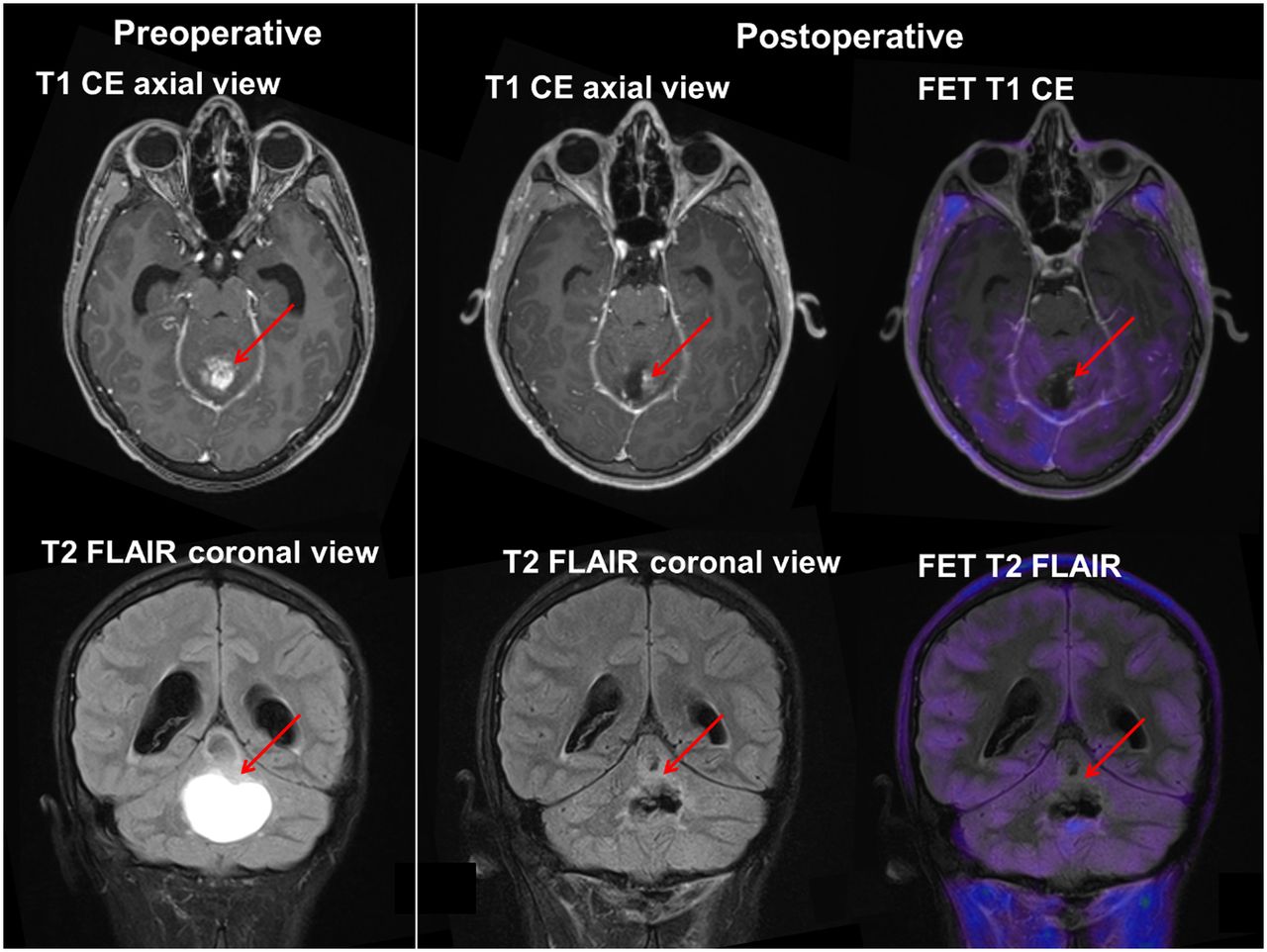
A 15-y-old boy (patient 16) operated on for pilocytic astrocytoma, WHO grade I. Preoperative scan shows contrast-enhancing (CE) and non–contrast-enhancing lesions and large cyst (arrows). Postoperatively, the 2 lesions are discordant on MRI and PET. Axial view shows contrast-enhancing lesion interpreted as residual tumor on MRI but without 18F-FET activity uptake. This lesion disappeared spontaneously after 3 mo. Coronal view shows non–contrast-enhancing residual tumor without 18F-FET uptake that persisted for 2 y. FLAIR = fluid-attenuated inversion recovery MRI sequence.
Clinical Impact
PET directly influenced clinical management in one patient (patient 3), as an additional small lesion, not visible on MRI, was identified by PET (Fig. 2), prompting resection of an extra tumor site at reoperation. In an additional 10 cases (37%), PET added important clinical information or assisted a difficult clinical decision (Table 1), although no impact was anticipated beforehand. In most cases of residual tumor, no immediate reoperation was indicated because of a relative benign pathology or a position in vital or eloquent brain areas, and thus PET did not directly change clinical management even if additional important clinical information from PET was achieved.

A 3-y-old boy (patient 3) operated on for atypical teratoid/rhabdoid tumor, WHO grade IV. Large intraventricular contrast-enhancing (CE) tumor mass is seen preoperatively. Postoperatively, MRI identifies contrast-enhancing residual tumor inferiorly in resection cavity (yellow arrow). Additional small residual tumor (red arrow) was identified only by 18F-FET PET. Complete resection was obtained by removing both residual tumor masses. Patient received radiochemotherapy and is in long-term remission. FLAIR = fluid-attenuated inversion recovery MRI sequence.
Tracer Uptake in Reactive Tissue Changes
Reactive changes with a maximal tumor-to-background ratio above 1.6 were found in 52% of scans (Table 1). Reactive tracer uptake tended to be less likely if scans were performed within 24 h after surgery (31%) than if performed later (71%) (P = 0.06). By careful review, it was possible in all cases by forced decision to correctly differentiate tumor from postoperative changes because later MRI scans did not reveal tumor in any of the areas with 18F-FET uptake that had been interpreted as reactive changes. Preoperative PET was available in 18 cases and was important for interpretation of the postoperative scans in 13 cases (72%), as the preoperative scans assisted the identification of new venous infarctions or reactive changes postoperatively. Pre- and postoperative scans of the spinal cord tumor allowed for unambiguous interpretation (Fig. 3).

A 12-y-old girl (patient 22) with ganglioglioma, WHO grade I, in spinal cord. Preoperatively, contrast-enhancing (CE) tumor with high 18F-FET activity uptake is seen (arrows). Twenty-four hours postoperatively, resection cavity and changes are seen on MRI sequences. No significant 18F-FET activity uptake is present.
DISCUSSION
The exact clinical role of PET/MRI in oncology has been the subject of continuous discussion. Emphasis have been given to PET/MRI as a tool for comprehensive assessment of morphology and molecular phenotyping, particularly useful in the pediatric population as one of the key applications (25) to reduce radiation exposure, number of scanning procedures, and image misregistration and to limit the risk and cost of anesthesia (26). However, this is to our knowledge the first larger clinical study using PET/MRI in pediatric neurooncology and the second study in pediatric oncology (27) testifying to the work-flow complexities of this sensitive patient group.
Complete surgical tumor removal of a brain tumor improves the prognosis in most children and adolescents. However, in accordance with earlier reports (28,29) residual tumor was detected either by immediate reoperation or by clinical follow-up after 52% of the operations. Frequent contrast enhancement on postoperative MRI challenges the identification of true residual tumor, which can lead to unnecessary reoperations. The addition of 18F-FET PET for early postoperative imaging led to a lesionwise specificity of 1.00 as compared with 0.75. Thus, the addition of 18F-FET PET may diminish the risk of a reoperation based on false-positive residual tumor on MRI. The reported sensitivity and specificity for MRI is similar to earlier reports (30). Earlier studies of postoperative 18F-FET PET found a higher sensitivity for residual tumor by PET than by MRI (13,14), whereas a study of recurrent glioma in adults using 18F-fluorophenylalanine PET in line with our results reported a significant increase in specificity of 0.89 (PET), versus 0.44 (MRI) (9).
Clinical Impact
In 41% of the scans, additional important information was obtained, including one case (patient 3) of directly influenced treatment because an additional small tumor lesion identified on the 18F-FET PET scan was removed (Fig. 2), ensuring complete resection. The patient has no signs of recurrence of the atypical teratoid/rhabdoid tumor (WHO grade IV) 32 mo later. Another postoperative scan served as a necessary baseline for later clinical decision making. To our knowledge, this is the first report of prospectively and consecutively collected 18F-FET PET scans early after surgery for brain tumors in children. A previous study of early postoperative 11C-methionine PET or 18F-FDG PET with 20 children (16) showed a pronounced clinical impact of PET, with early second-look surgery in 11 patients. However, only children suspected of having residual tumor were included (70% had equivocal MRI results), in contrast to the present study, which included patients consecutively without selection based on MRI findings (7% had equivocal MRI; Table 1).
Reactive Tissue Changes
Postoperative tissue changes hamper the reading of the MRI, and the same is true for 18F-FET PET, with a high fraction (52%) of 18F-FET activity uptake in postoperative reactive changes, especially if the 18F-FET PET is performed more than 24 h after surgery. Frequent 18F-FET uptake in reactive changes due to inflammation is well known (12), but in the present study using forced decision, it was possible in all cases to discriminate between residual tumor and postoperative changes.
Limitations
The study contains a relatively high fraction of low-grade gliomas (mainly pilocytic astrocytomas, WHO grade I), for which a conservative approach in cases of residual tumor is common as opposed to high-grade tumors (WHO grade III–IV), in which complete resection is highly prioritized. This reduces the potential clinical impact of the study. Another limitation is the lack of biopsy confirmation of the possible residual tumors. As no clinical consequences were expected, it was deemed unethical to obtain biopsies. Instead we used clinical follow-up and, in difficult cases, consensus reading of the follow-up scans at a formal review meeting. The relatively small number of patients reduces the statistical power of the study, and although a much higher specificity of 1.00 as compared with 0.75 was observed, the difference was not statistically significant. Larger studies are, however, unlikely to be performed because of the challenging setup, and we find the conclusions to be genuine despite nonsignificant test results. Further, we did not manage to have identical MRI protocols pre- and postoperatively for all patients. However, the lack of preoperative 18F-FET PET and the use of varying MRI scanners pre- and postoperatively reflect the daily clinical routine and results from the study are thus transferable to a clinical setting.
CONCLUSION
This prospective clinical study shows PET/MRI as a powerful research tool that may help advance pediatric neurooncology in the future. Early postoperative 18F-FET PET combined with MRI showed a lesionwise specificity for discriminating tumor from treatment effects of 1.00 as compared with 0.75 for MRI alone. Consequently, if reoperation is considered on the basis of early postoperative MRI, our results support that additional 18F-FET PET could help discriminate treatment effects from true residual tumor, allowing for a conservative approach instead of immediate reoperation for whom 18F-FET PET does not suggest residual tumor.
DISCLOSURE
The Danish Childhood Cancer Foundation funded salary (Michael Lundemann and Lisbeth Marner) and anesthesia assistance for the project (2014-34, 2015-48). Copenhagen University Hospital Rigshospitalet funded a start-up grant. The Siemens mMR hybrid PET/MRI system at Copenhagen University Hospital Rigshospitalet was generously donated by the John and Birthe Meyer Foundation. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
The scanner assistance of technologists Karin Stahr and Marianne Federspiel and of radiographers Jákup Martin Poulsen and Nadia Azizi is highly appreciated. Andreas Høyby Ellegaard and Jakob Slipsager are thanked for their support with motion tracking.
Footnotes
Published online Jan. 25, 2019.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication September 12, 2018.
- Accepted for publication December 11, 2018.





{kind=link}
{kind=link}
{kind=link}