


Abstract
The radiation dose delivered to pregnant patients during radiologic imaging procedures raises health concerns because the developing embryo and fetus are considered to be highly radiosensitive. To appropriately weigh the diagnostic benefits against the radiation risks, the radiologist needs reasonably accurate and detailed estimates of the fetal dose. Expanding our previously developed series of computational phantoms for pregnant women, we here describe a personalized model for twin pregnancy, based on an actual clinical scan. Methods: The model is based on a standardized hybrid pregnant female and fetus phantom and on a clinical case of a patient who underwent an 18F-FDG PET/CT scan while expecting twins at 25 weeks’ gestation. This model enabled us to produce a realistic physical representation of the pregnant patient and to estimate the maternal and fetal organ doses from the 18F-FDG and CT components. The Monte Carlo N-Particle Extended general-purpose code was used for radiation transport simulation. Results: The 18F-FDG doses for the 2 fetuses were 3.78 and 3.99 mGy, and the CT doses were 0.76 and 0.70 mGy, respectively. Therefore, the relative contribution of 18F-FDG and CT to the total dose to the fetuses was about 84% and 16%, respectively. Meanwhile, for 18F-FDG, the calculated personalized absorbed dose was about 40%–50% higher than the doses reported by other dosimetry computer software tools. Conclusion: Our approach to constructing personalized computational models allows estimation of a patient-specific radiation dose, even in cases with unusual anatomic features such as a twin pregnancy. Our results also show that, even in twins, the fetal organ doses from both 18F-FDG and CT present a certain variability linked to the anatomic characteristics. The CT fetal dose is smaller than the 18F-FDG PET dose.
In pregnant patients, it is critical that the benefit from radiologic examinations be carefully weighed against the possible radiation risk to the fetus. At fetal doses greater than 50–100 mGy, which are unlikely to be delivered by medical imaging, the potential hazardous effects of radiation on the fetus include death, intrauterine growth limitation, average intelligence quotient loss, mental retardation, organ malformation, and small head size (1). Although controversial (2,3), the linear no-threshold model is still the basis for radioprotection regulations. This model postulates that stochastic effects such as cancer might also occur at smaller doses (4–8). Because of this regulatory framework, and because health effects cannot be formally ruled out, the fetal absorbed doses should be known as precisely as possible. Estimating the fetal dose is, however, a challenging task, because of the difficulties associated with direct measurement of energy deposition and the irregular shape of the fetal body. Various approaches have been adopted to estimate the fetal dose, including Monte Carlo simulations using computational anthropomorphic models (7,9–17) and experimental measurements using physical phantoms with embedded dosimeters (18–21). However, these approaches inherently bear several limitations, such as the difficulty of constructing patient-specific computational models and of matching anthropomorphic physical phantoms to the size and location of the fetus within the maternal body (22). Because of these limitations, significant over- or underestimations of the fetal absorbed dose are possible. Monte Carlo calculations are considered the gold standard for dose estimation in diagnostic imaging (23), and their use in a clinical setting within a framework of patient-specific estimation of fetal dose from diagnostic procedures is highly desirable.
In this work, we expand on our previous set of anthropomorphic phantoms and describe the methodology for constructing patient-specific computational models for a pregnant female with twins. This model is based on a standardized hybrid pregnant-female-and-fetus phantom, derived from an actual 25 weeks’ pregnant patient who underwent an 18F-FDG PET/CT scan while expecting twins. The patient-specific maternal and fetal absorbed radiation doses from both 18F-FDG and CT were calculated and compared with the results provided by the OLINDA/EXM software (24) and the ImPACT CT (Impact Performance Assessment of CT, Bence Jones Offices, St. George’s Hospital, London) dosimetry calculator, respectively. The influence of fetal position on fetal absorbed dose was also investigated.
MATERIALS AND METHODS
Standardized Computational Model for Twins
Our standardized pregnant female model with twins at the 25th wk of gestation was based on the International Commission on Radiological Protection (ICRP) computational pregnant female phantom at the 25th wk of gestation (17), which was developed using the mother torso and internal organs of the Rensselaer Polytechnic Institute phantoms (RPI-P) (25), the fetal and mother numeric models of Telecom ParisTech (26), the Katja model (27), and the newborn model of Helmholtz Zentrum München (28). The 25th-wk twins phantom was based on the fetal and mother numeric models and the Katja model. The organs of the fetus were scaled from the Katja model to match the reference organ masses of the ICRP phantom (29). The maternal bladder, small intestine, and large intestine were manually adjusted using the Rhinoceros package (Robert McNeel and Associates). The model includes 35 maternal tissues (adrenals, urinary bladder wall, urinary bladder content, brain, breasts, esophagus, eyeballs, eye lenses, gallbladder wall, gallbladder content, heart wall, heart content, kidneys, large intestine wall, large intestine content, liver, lungs, ovaries, pancreas, small intestine, skeleton, skin, spleen, stomach wall, stomach content, thymus, thyroid, trachea, uterine wall, uterine content, placenta, umbilical cord, amniotic fluid, yolk sac, and remainder tissues) and 50 fetal regions (25 for each fetus). The fetal tissue compositions were obtained from ICRP publication 89 (29): bone density was set at 1.3 g/cm3 and soft-tissue density at 0.99 g/cm3.
Patient-Specific Computational Model
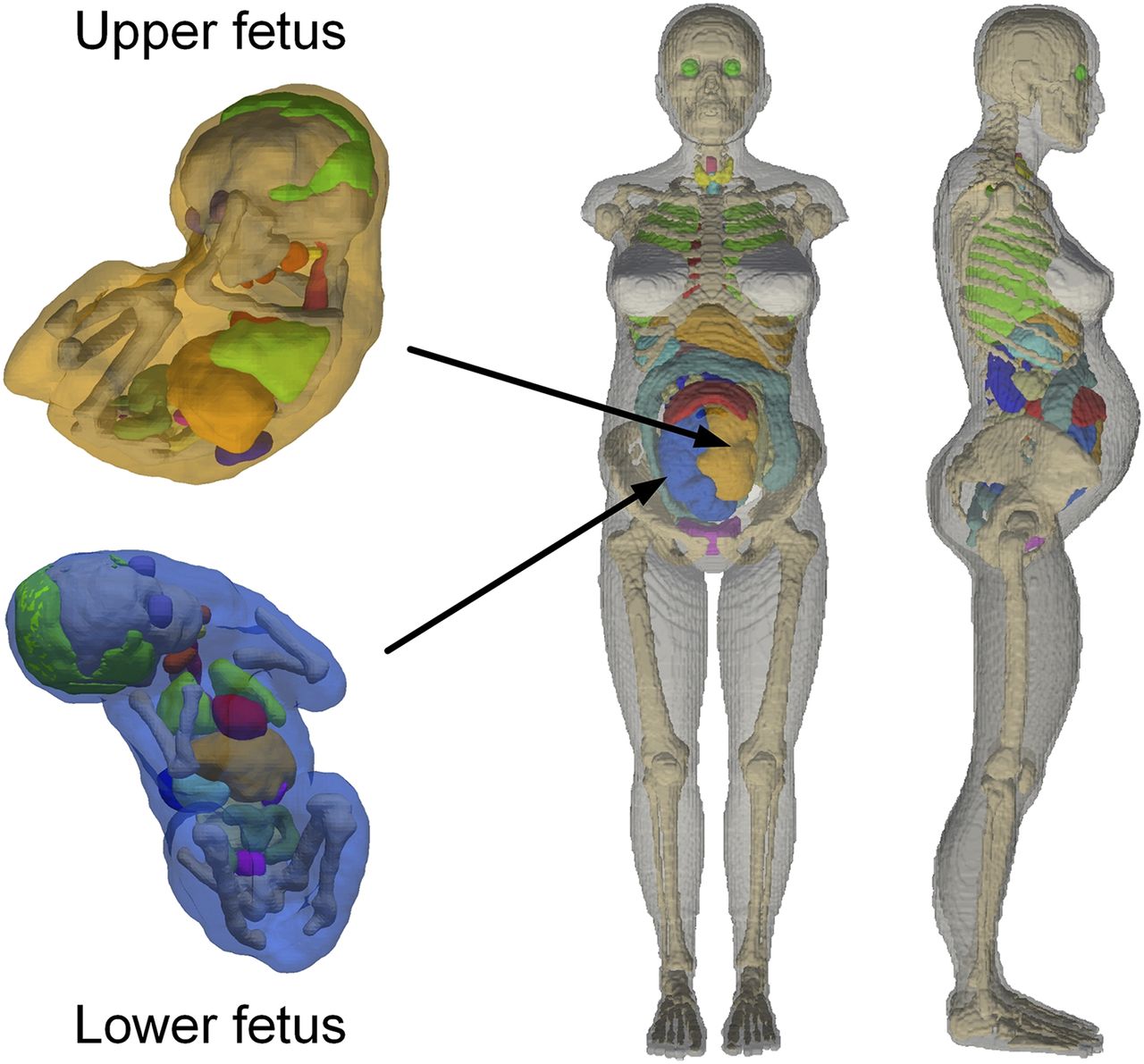
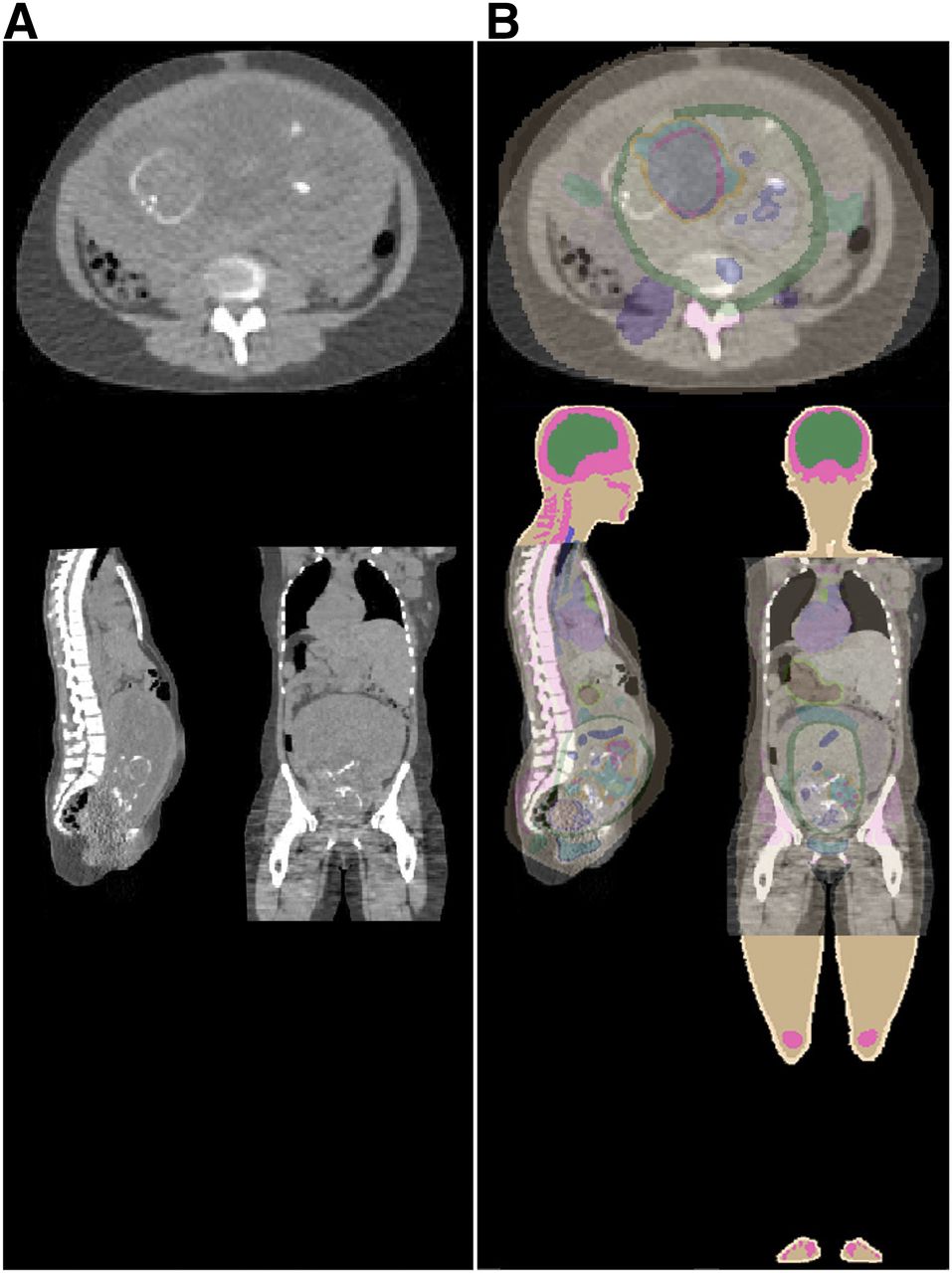
The CT images of the pregnant patient were segmented into body, lung, skeleton, and uterus for constructing the regional voxel matrix (Fig. 1). This retrospective study, which was reported in previous work (30), did not require additional institutional review board approval, and the requirement to obtain informed consent was waived. First, the standardized twins computational model was voxelated from the boundary representation model. Then, using automatic affine registration via the Insight Toolkit (31), it was registered to the constructed CT-derived regional patient-specific voxel matrix to produce a new personalized computational model with well-defined anatomic structures that match patient CT images. The developed patient-specific computational model was used as input for Monte Carlo calculations of the radiation dose to the fetuses and maternal body. Figure 2 shows the 3-dimensional visualization of the constructed patient-specific model with zoomed views of the upper fetus and lower fetus. Figure 3 shows the registration of representative CT images between the patient and the standardized computational phantom for construction of the patient-specific model.

(A) CT image with external body contour (red line) around perimeter of pregnant patient and uterus (blue line) containing twin fetuses at 25th wk of gestation. (B) Segmented CT image with external body contour, skeleton, and uterus.

3-dimensional views of computational pregnant female phantom at 25 weeks’ gestation, with zoomed views of embedded twins.

Representative slices showing image registration between abdominal CT images of patient (A) and computational phantom (B) for development of patient-specific pregnant computational models.
Monte Carlo Simulations
PET Component
The patient-specific computational phantom was imported to the Monte Carlo N-Particle Extended code (32) for radiation transport simulations. S values of uniformly distributed sources of 18F in maternal and fetal tissues were estimated. Calculation of the absorbed dose and effective dose delivered to both fetuses and the maternal organs from 18F-FDG was based on the MIRD formalism (33). The regions of interest used to calculate the activity concentrations in the fetuses were manually drawn on the bodies of the fetuses (30). The time-integrated activity coefficients for 18F-FDG in the maternal organs were obtained from ICRP publication 106 (34). Table 1 lists the total number of disintegrations (residence times) of 18F-FDG in the maternal organs and the 2 fetuses. It was assumed that the average activity concentration in fetal tissues was the same in both fetuses. The mean total number of disintegrations of 18F-FDG in the upper fetus and lower fetus were 0.0412 and 0.0434 Bq h/Bq, respectively.
Total Number of Disintegrations of 18F-FDG in Maternal Organs and Fetuses
CT Component
A GE Healthcare 750HD CT scanner model was created and validated using Monte Carlo–based techniques in our previous work (12,35). This CT source and geometry model is equipped with a Performix Pro VCT 100 x-ray tube with 56° fan-beam angle, a 7° target angle, and a measured half-value layer of 7.8 mm of aluminum at 120 kVp. The patient-specific computational model was integrated with the CT scanner model in the N-Particle Extended code (32). Simulated CT examinations were performed using the personalized model and the protocol parameters used in our institution for patient scanning with a helical source path and a total collimation width of 64 × 0.625 mm (12). The absorbed doses to maternal organs and fetal organs were calculated and normalized to the CT dose index (CTDIvol = 1.8 mGy) of the simulated examination (12).
Absorbed Dose Calculations
For the PET component, the absorbed radiation dose from 18F-FDG to the target tissue rT is given by Eq. 1where rS is the source organ,
Eq. 1where rS is the source organ,  is the cumulated activity in the source organ over the dose-integration period TD, and
is the cumulated activity in the source organ over the dose-integration period TD, and  is the S value describing the equivalent dose rate in the target organ per unit activity in the source organ.
is the S value describing the equivalent dose rate in the target organ per unit activity in the source organ.
For the CT component, the CTDIvol-normalized absorbed radiation dose from the simulated examination to the clinical examination is estimated using the following equation: Eq. 2where
Eq. 2where  is the CTDIvol of the patient in the simulated CT scanner,
is the CTDIvol of the patient in the simulated CT scanner,  is the calculated absorbed dose to the patient in the simulated CT scanner, and
is the calculated absorbed dose to the patient in the simulated CT scanner, and 
 are the absorbed dose and CTDIvol to the patient in the clinical CT examinations, respectively. The reported CTDIvol for the patient in the clinical CT examination was 1.04 mGy. For the same patient model, the coefficient of variation for the CTDIvol-normalized dose values across different scanners and protocols has been reported to be less than 10% (36).
are the absorbed dose and CTDIvol to the patient in the clinical CT examinations, respectively. The reported CTDIvol for the patient in the clinical CT examination was 1.04 mGy. For the same patient model, the coefficient of variation for the CTDIvol-normalized dose values across different scanners and protocols has been reported to be less than 10% (36).
RESULTS
Patient-Specific Computational Phantom
The accuracy of the registration between the regional voxel matrix of the patient and the generated patient-specific computational phantom was evaluated by calculating the Jaccard coefficient of similarity (37) for the corresponding segmented organs: 0.73, 0.60, 0.12 and 0.55 for total body, lung, skeleton and uterus, respectively. The low Jaccard coefficient for the skeleton was caused mainly by the mismatch of the ribs and hip bones between the anchor phantom and patient. The weight of the lower fetus matched well the ICRP-recommended fetal weight of 990 g at 25 weeks’ gestation, and the weight of the upper fetus was slightly lower (Table 2).
Organ Masses of Fetuses
Absorbed Doses from the PET Component
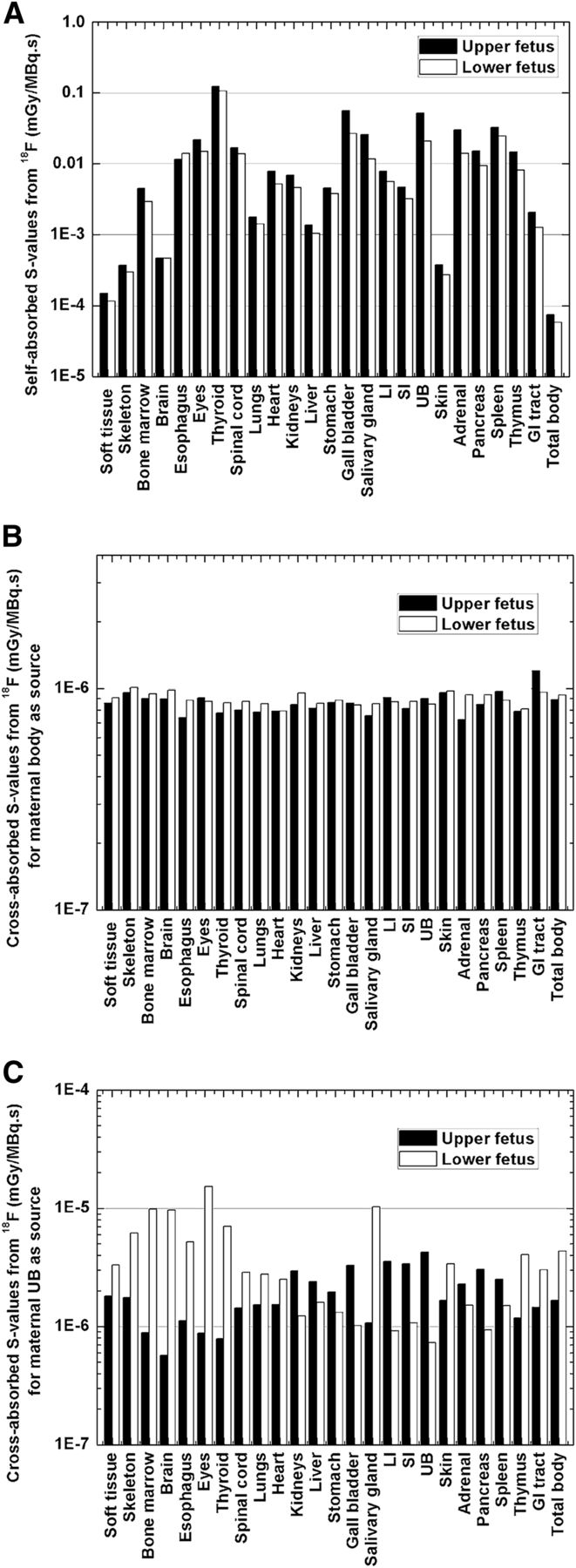
The coefficient of variation for 18F-FDG organ dose between the 2 fetuses was approximately 8.5%, with a minimum of approximately 0.3% (for the spinal cord) and a maximum of approximately 23.2% (for the eyes), whereas the mean differences in the fetal total-body dose between this work and the 2 versions of OLINDA/EXM were −55% and −40.5%, respectively (Table 3). As shown in Figure 4A, for the same organ, the estimated self-absorbed S value of the lower fetus was about 29% smaller than the value of the upper fetus. Indeed, the self-absorbed S values of fetal organs decrease when fetal weight increases (17). The cross-absorbed S values were obtained assuming uniform activity in all maternal source tissues. As shown in Figures 4B and 4C, the cross-absorbed S values for the maternal body irradiating the fetus were contributed mostly by the annihilation photons and presented a uniform distribution in different fetal organs. The mean absolute difference in cross-absorbed S values from the maternal body between the 2 fetuses was about 8%. The cross-absorbed S values from maternal urinary bladder were affected by the fetal position and presented a mean absolute difference of 112% between the 2 fetuses. Figure 5 illustrates the organ-absorbed doses in the 2 fetuses from 18F-FDG. In the upper fetus the gastrointestinal tract received the highest absorbed dose, whereas in the lower fetus the absorbed dose to the eyes and bone marrow was higher than in the other organs. The absorbed 18F-FDG doses to the upper and lower fetuses were 0.0201 and 0.0212 mGy/MBq, respectively. The absorbed dose to the maternal uterus was 11.4% and 16.2% lower than the total-body dose to the upper and the lower fetuses, respectively.
Total-Body Doses from 18F-FDG to Fetuses Compared with Those Obtained Using OLINDA/EXM 1.1 and OLINDA/EXM 2.0

Self-absorbed S values of 18F for fetal organs (A) and cross-absorbed S values of 18F from maternal body (B) and maternal urinary bladder (C), irradiating fetal bodies. GI = gastrointestinal; LI = large intestine; SI = small intestine; UB = urinary bladder.
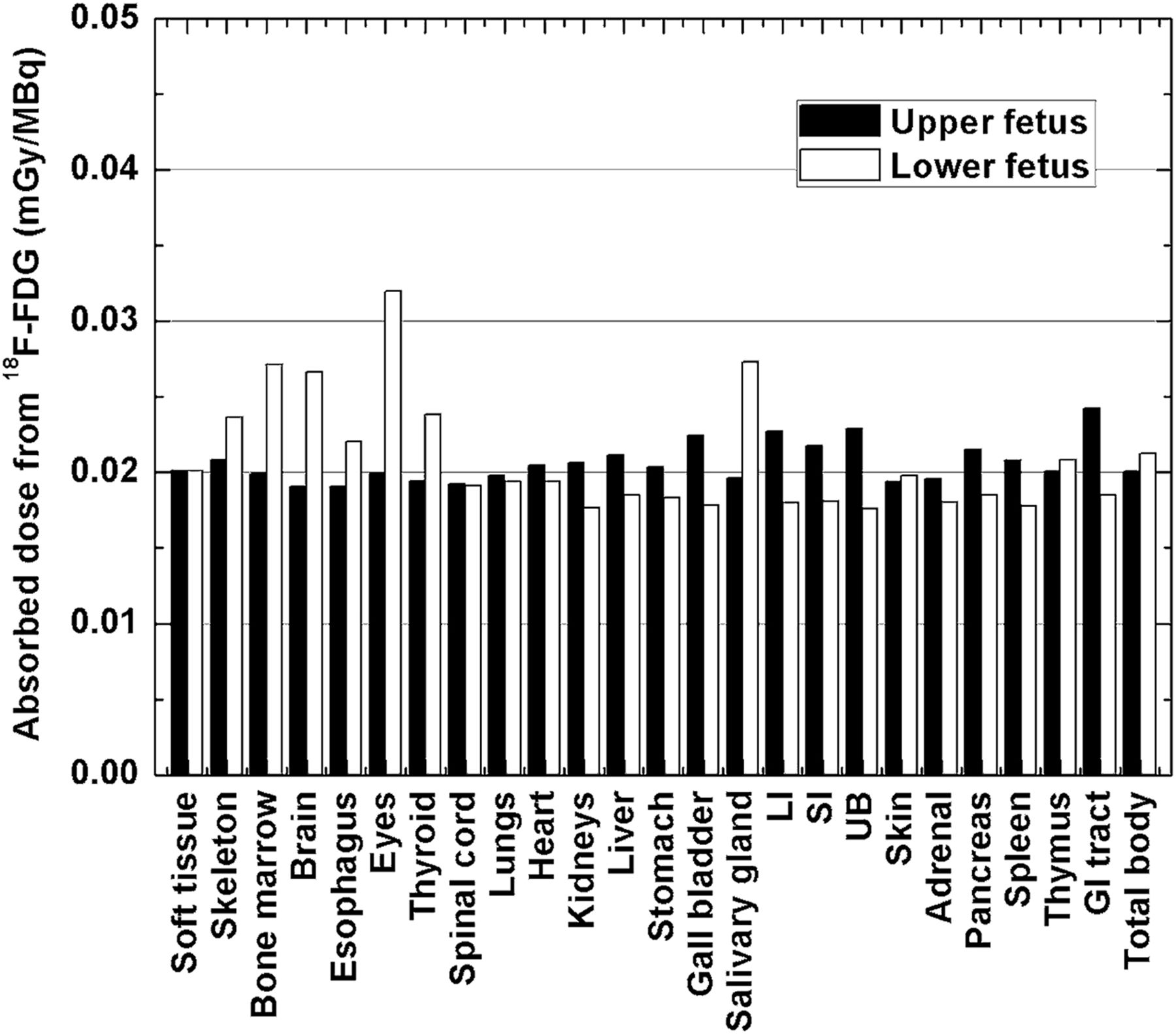
Absorbed doses to different organs of fetuses from 18F-FDG. GI = gastrointestinal; LI = large intestine; SI = small intestine; UB = urinary bladder.
Absorbed Doses from the CT Component
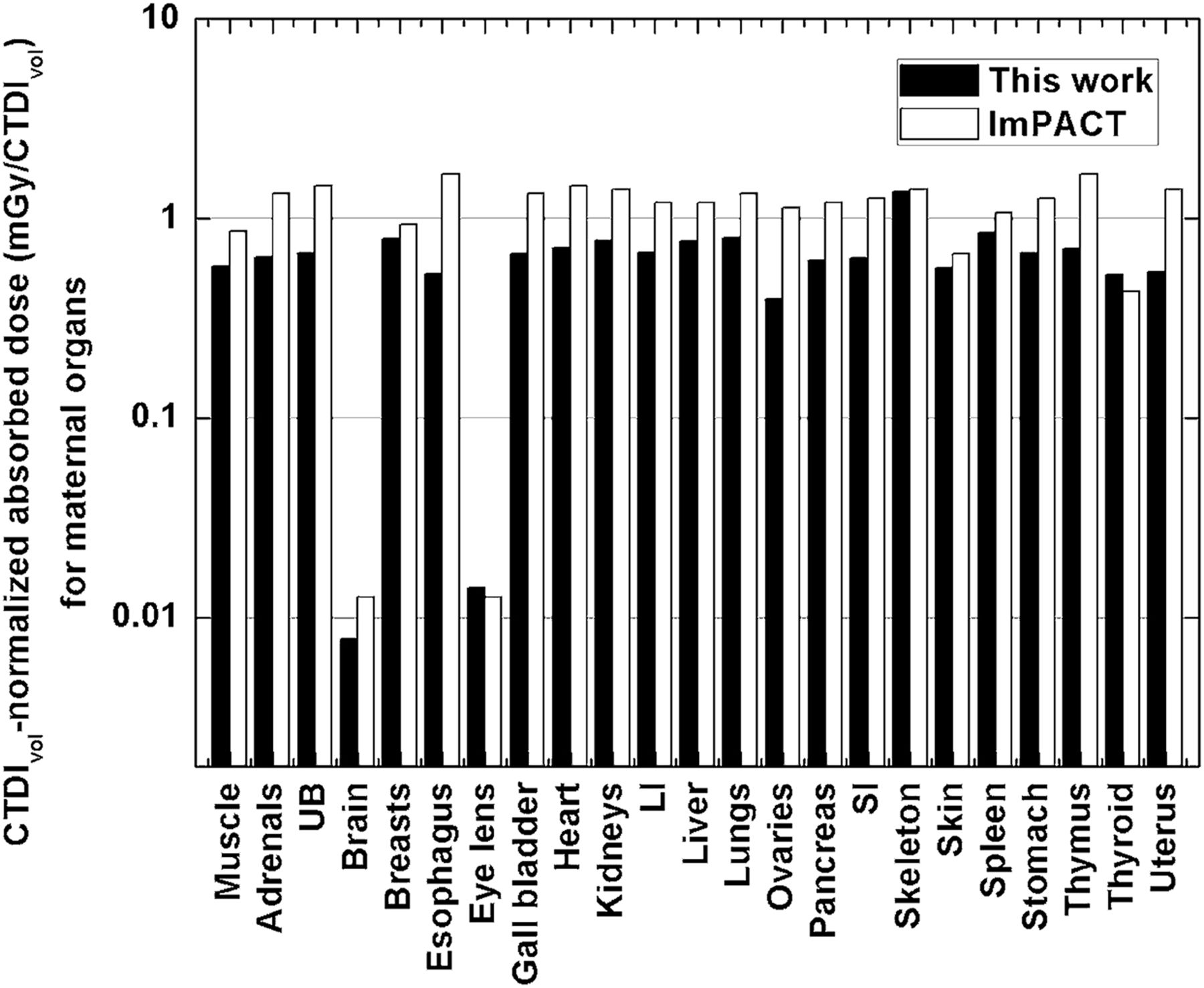
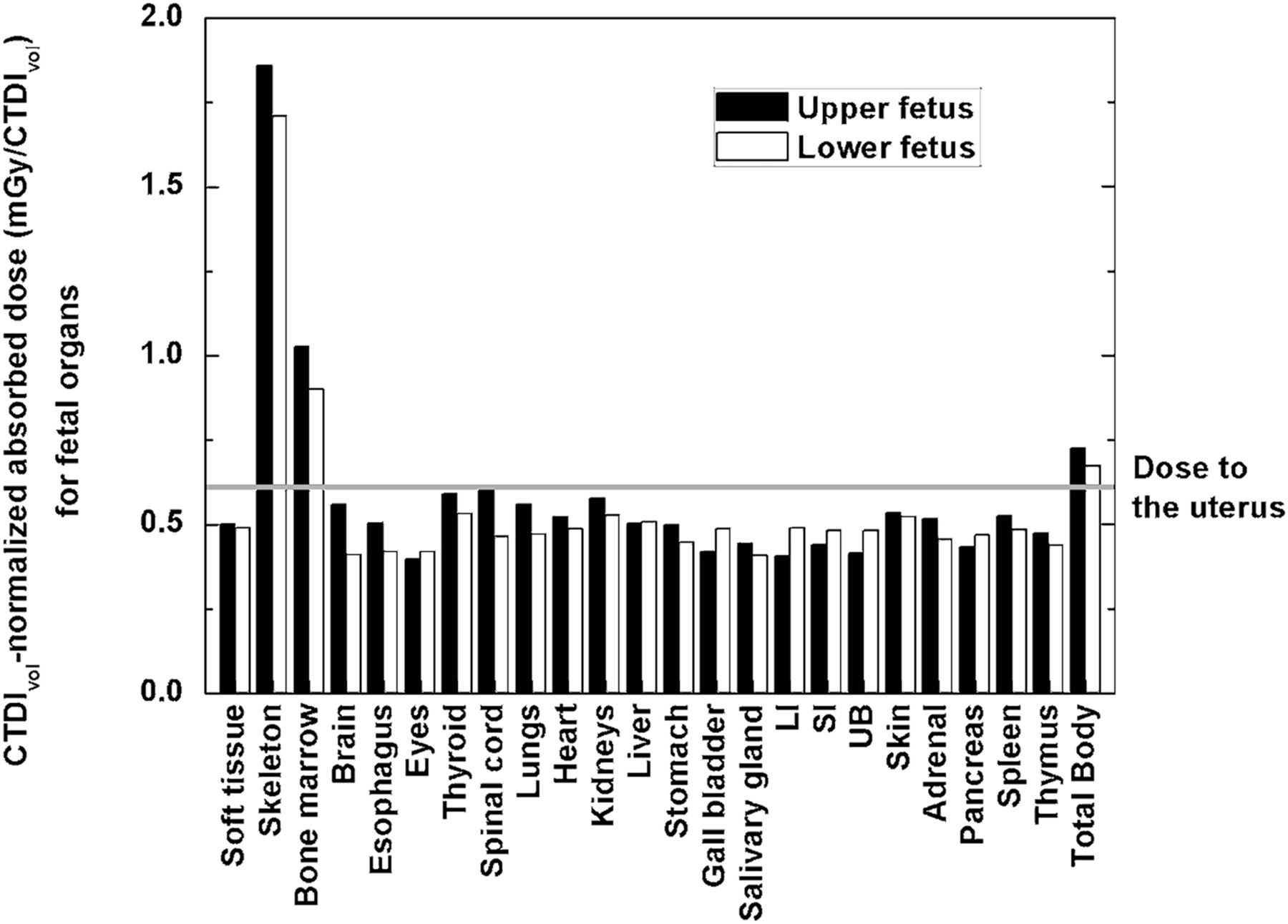
Except for the total body, skeleton, and bone marrow, the absorbed CT doses to other fetal organs were about 20% lower than the dose to the maternal uterus. The variation in organ CT dose between the 2 fetuses was approximately 5.7%, with a minimum of approximately 0.3% (for the liver) and a maximum of approximately 15.2% (for the brain). Figure 6 compares the CTDIvol-normalized absorbed dose for different maternal organs with estimates provided by the ImPACT CT dosimetry calculator. The mean absolute difference in dose to the maternal organs between this work and ImPACT CT was 40.3%. Figure 7 shows the CTDIvol-normalized absorbed dose from the CT component to fetal organs. The absorbed dose was nonuniformly distributed between fetal organs. For instance, the absorbed dose to the fetal skeleton and bone marrow was about 3.7 and 2.0 times higher, respectively, than that received by other fetal organs. Because a low-dose CT protocol was performed, the absorbed doses to the 2 fetuses were relatively low, at 0.73 and 0.67 mGy/CTDIvol, respectively, whereas the absorbed dose to the uterus was 0.61 mGy/CTDIvol.
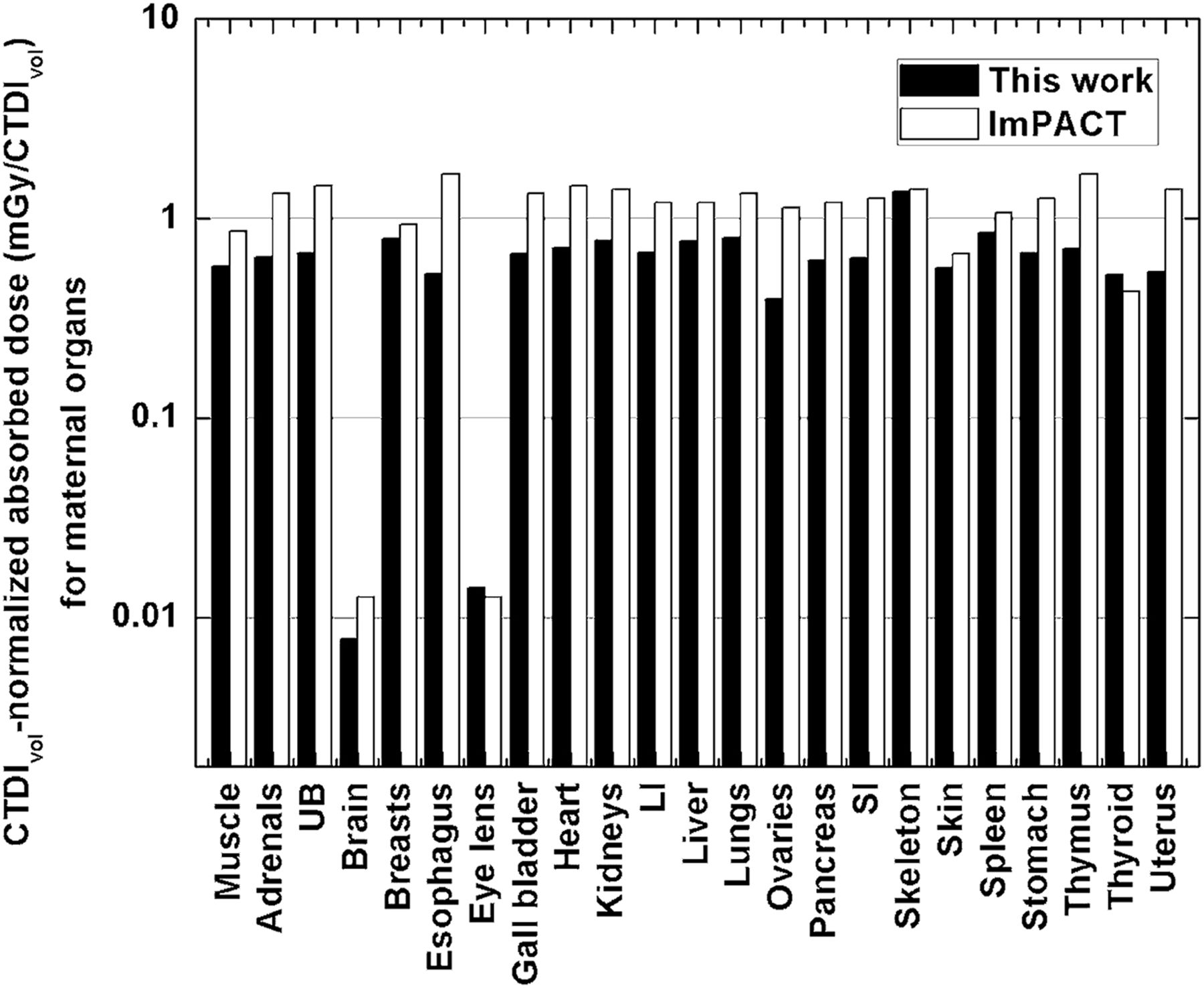
Normalized absorbed doses to different organs of pregnant patient from CT examination. LI = large intestine; SI = small intestine; UB = urinary bladder.

Normalized absorbed doses to different organs of fetuses from CT examination. LI = large intestine; SI = small intestine; UB = urinary bladder.
Total Absorbed Doses from the Combined PET/CT Examination
The absorbed dose to the upper fetus was 0.76 mGy from the CT component and 3.78 mGy from the PET component, for a total of 4.53 mGy from the PET/CT examination, whereas the absorbed dose to the lower fetus was 0.70 mGy from the CT component and 3.99 mGy from the PET component, for a total of 4.69 mGy from the PET/CT examination. For the different fetal organs, the CT component contributed 8.4%–30.8% of the total absorbed dose whereas the PET component contributed 70%–91.6% of the total absorbed dose. For the patient, the injected 18F-FDG activity was 188 MBq, and the patient-specific CTDIvol performed in the CT examination was 1.04 mGy without tube current modulation. The calculated absolute doses to the patient and fetuses are summarized in Tables 4 and 5, respectively. The patient’s effective dose was 0.79 mSv from the CT component and 3.62 mSv from the PET component, resulting in a total of 4.41 mSv from the PET/CT examination.
Absorbed Dose and Effective Dose to Maternal Body from PET/CT Examination
Absorbed Dose to Fetuses from PET/CT Examination
DISCUSSION
We have described our methodologic procedure to create a computational patient-specific phantom enabling calculation of the fetal dose in the particular case of twin pregnancy. Our approach, which involves coregistration of clinical images to the computational phantom followed by Monte Carlo–based dose calculations, is suitable for individualized dose assessment in a clinical setting. The unusual anatomy of a twin pregnancy is a clear example of the adaptability of our methodology to disparate clinical situations.
In calculation of the fetal dose, there were 3 main sources of inaccuracy: from the geometric point of view, the registration of the standardized phantom to the clinical images; the uncertainty linked to Monte Carlo simulations; and the CTDIvol-based estimation of the dose to the organs. The uncertainty from the image registration process was by far the greatest source of inaccuracy, accounting for 27%–45% of the variability in the dose, whereas the error expected from Monte Carlo calculations and CTDIvol-based organ dose estimation was generally less than 5%. The CTDIvol and the dose–length product are the 2 metrics commonly conveyed in dose reports by commercial CT scanners and used to determine CT doses to pregnant patients and fetus (12).
The estimation of the CT dose showed that the fetal skeleton and bone marrow receive a substantially higher dose than soft tissues because of the higher density of the former. Although never proven for the range of doses received during medical examinations, radiation exposure of the bone marrow in childhood creates the hypothetical risk that malignancies will develop later in life, and this aspect should be considered when the acquisition protocol is designed for the CT component.
We investigated the influence of anatomic characteristics of the fetus on radiation dosimetry by comparing the organ dose of the 2 fetuses. For the PET component, the coefficient of variation across the 2 fetuses for a given organ ranged from 0.3% (for the spinal cord) to 23.2% (for the eyes), with a mean across all organs of 8.5%. For the CT component, the coefficient of variation across the 2 fetuses for a given organ ranged from 0.3% (for the liver) to 15.2% (for the brain), with a mean across all organs of 5.7%. These results indicate that, at the same stage of gestation, anatomic differences between the fetuses influence the estimation of the internal and external absorbed doses for any organ. The organ dose to a particular fetus would be within approximately 25% of the mean value across the whole fetus at the same stage of gestation. From a radiobiologic point of view, this difference in absorbed dose between the 2 fetuses is likely to be insignificant.
An important finding of our study was that the fetal doses estimated using either OLINDA/EXM 1.1 or 2.0 were about 50% smaller than the doses calculated using our patient-specific model. This discrepancy can be attributed mainly to the differences between the fetal weights and source-to-fetus distances used in our personalized computational phantom and patient images and those used in OLINDA/EXM 1.1 and 2.0, which are based on a stylized model (38) and the 6-mo voxel-based RPI-P model (25), respectively. When generic anthropomorphic phantoms, such as those included in both versions of OLINDA/EXM, are used, the final dose is heavily dependent on the characteristics of the phantom, such as the mass and the geometric arrangement of the organs. The use of a patient-specific phantom in a clinical setting allows more accurate dose calculation, which is of particular importance in cases such as pregnant women or pretherapeutic imaging. In radiation dosimetry, the absorbed dose to the maternal uterus is used as a conservative proxy for the fetal dose (39). This work showed that the mean fetal dose was about 15% higher than the uterine dose for both the PET and the CT components. For CT, the uterine dose may still be used as a conservative value for fetal soft tissues (i.e., except for the skeleton and bone marrow).
Our study showed that the 18F-FDG contribution to the total dose was much higher than the CT contribution, for both the mother and the fetuses (i.e., about 16%–18% vs. 82%–84%). In addition, the maximum contribution to the organ dose from CT was about 30% to the fetal skeleton, whereas the maximum contribution from 18F-FDG was more than 90% to the brain, eyes, and salivary gland. In total, the mean fetal dose from the PET/CT examination was 4.61 mGy. This level of radiation not only is well below the threshold of deterministic effects but also is below the threshold where stochastic effects have been documented in humans (40). In imaging of pregnant women, priority should be given to achieving an examination of diagnostic quality, because overly aggressive dose-reduction protocols may put the life of both the mother and the fetus in danger (41).
CONCLUSION
The proposed approach for constructing personalized computational models enables calculation of a patient-specific radiation dose during a combined PET/CT examination, even in complex, unusual situations such as a patient pregnant with twins. The fetal organ dose is particularly affected by the fetal position, among other factors. The calculated personalized 18F-FDG fetal dose was significantly higher than the corresponding CT dose and was about 40%–50% higher than doses reported by widely used popular internal dosimetry software.
DISCLOSURE
This work was supported by the Swiss National Science Foundation under grant SNSF 320030_176052. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Drs X. George Xu (Rensselaer Polytechnic Institute), Isabelle Bloch (Telecom ParisTech), and Maria Zankl (Helmholtz Zentrum München) for providing the computational models.
Footnotes
Published online Jan. 25, 2018.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication November 13, 2017.
- Accepted for publication January 12, 2018.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.