


TO THE EDITOR: Advances in PET/CT technology, such as the development of digital PET detectors, extended axial fields of view (total-body PET), and the use of resolution modeling during reconstruction, improve image quality, for example, by affecting sensitivity and spatial resolution. This results in enhanced lesion detectability and changes both visual and quantitative reads. These developments, however, pose challenges for multicenter studies and the application of previously validated interpretation criteria, such as the Deauville score (DS) in the clinical management of patients with lymphoma (1,2). These criteria are derived from studies performed on previous generations of PET/CT systems and do not necessarily translate 1-to-1 with data generated using the latest systems.
Recently, a shift toward more positive reads for 18F-FDG PET/CT studies in patients with Hodgkin lymphoma with clinical consequences was reported by Barrington et al. (3) This shift was found to coincide with the introduction of a new generation of PET/CT systems that incorporate resolution modeling during reconstruction (also called point-spread function [PSF] reconstructions). Such reconstructions are associated with increased SUV in (small) lesions, but not in large uniform organs such as the liver and blood pool (4). This nonuniform change in apparent 18F-FDG uptake may affect reads when based on comparing lesion 18F-FDG uptake with that of liver and mediastinal blood pool, as is the case when using the DS. PSF reconstructions have also been found to overestimate SUV in lung cancer patients (4,5). This upward bias seems also to depend on the size of the lesion or sphere, being the largest (sometimes up to 60%) for spheres and lesion of about 1.0–1.5 cm in diameter (i.e., the upward bias seems to be largest for this particular size). PSF reconstructions also introduce image artifacts, as illustrated in Figure 1 showing reduced uptake at the center of a uniformly filled sphere and increased uptake near the edge of this sphere. Clearly, in a sphere filled with a homogeneous 18F-FDG solution, reduced core uptake surrounded by increased uptake near the edges above the actual value (similar to the distribution observed in truly necrotic lesions in vivo) does not represent the real 18F-FDG distribution.

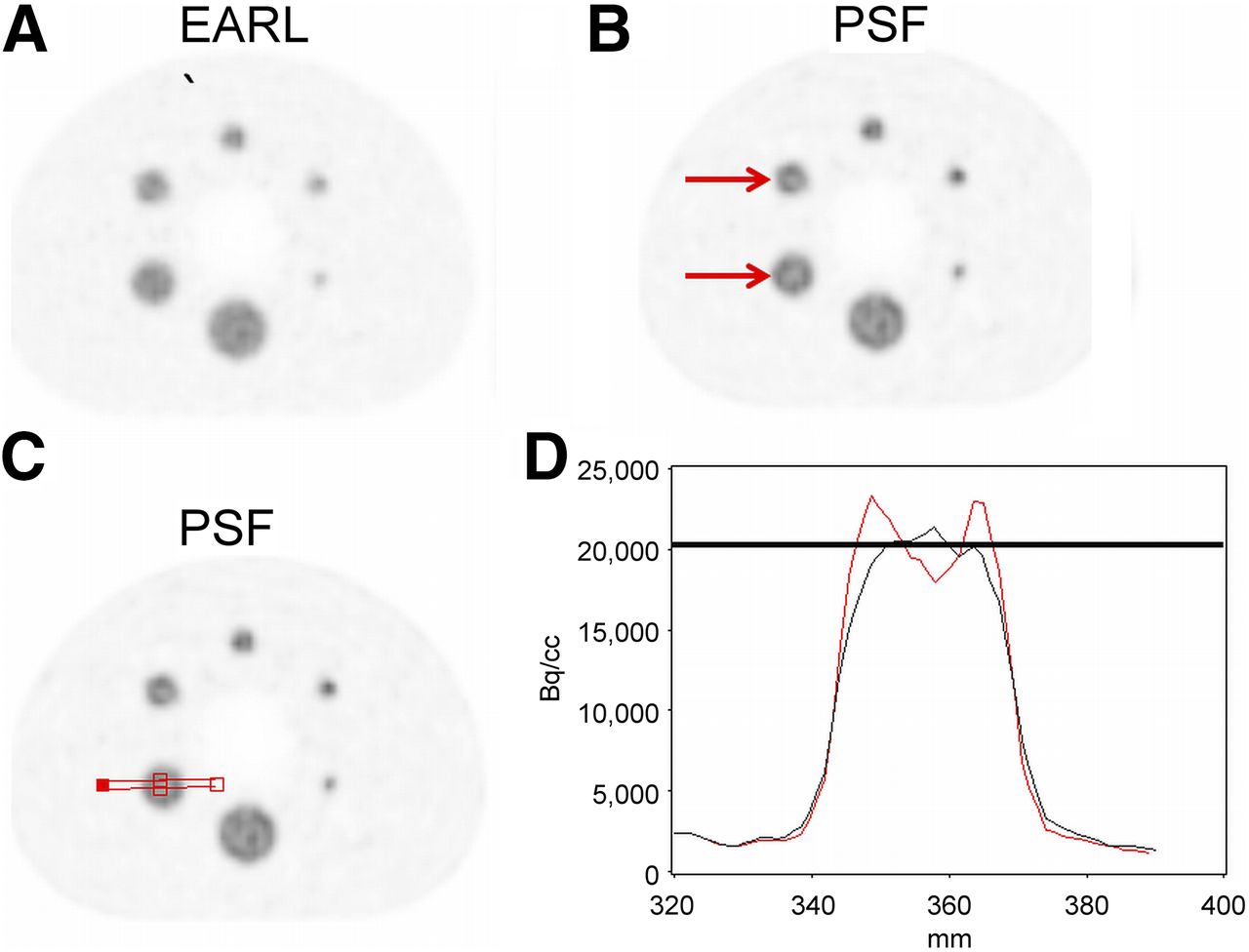
PET images (axial slice) of NEMA Image Quality phantom filled conforming with EARL instructions. (A) PET image reconstructed with EARL-compliant settings. (B) PET image reconstructed using resolution modeling (PSF). Red arrows point to typical PSF artifact showing increased uptake at edge of a sphere and reduced uptake at center of the sphere, which appear most strongly for 1- to 1.5-cm-diameter spheres. (C) Image illustrating location of activity profile (red line) as plotted in D. Red line in D indicates activity profile seen in PSF-reconstructed PET image, and black line indicates that of EARL-compliant reconstruction.
Enilorac et al. (6) recently reported on the effects of using PSF reconstruction on Deauville scoring in lymphoma patients. The authors conclude that neither the DS nor risk stratification of diffuse large B-cell lymphoma (DLBCL) patients is affected by the choice of PET reconstruction. Specifically, the use of PSF is not an issue in routine clinical processes or in multicenter trials. Yet, the authors admit that their findings need to be confirmed. Their conclusions are in contrast with the observations of Barrington et al. (3) and with the large changes in 18F-FDG SUV seen in other studies and for other tumor types (4,5). When the data presented by Enilorac et al. (6) are considered more closely, a large fraction of the patient scans was evaluated as either DS1 or DS2, at interim (37%) and at the end of treatment (53%), using PSF reconstruction. This result is in line with the high response rate anticipated to treatment in most patients with DLBCL. As European Association of Nuclear Medicine (EANM) Research Ltd. (EARL)–compliant reconstructions typically result in lower lesion SUV, it is to be expected that moving from EARL-compliant to PSF reconstruction would not affect risk stratification for these patients. However, when patient scans with a DS of 4 using PSF reconstruction were considered, 4 of 31 (13%; 95% confidence interval = 5%–29%) at interim and 3 of 17 subjects (18%; 95% confidence interval = 6%–41%) at the end of treatment were scored as DS3 when EARL-compliant reconstructions were used. Or looking at the data in another way, 4 of 22 (18%) patients with interim scans were evaluated as DS3 using EARL but DS4 using PSF. Three of 18 (17%) patients had end-of-treatment scans evaluated as DS3 using EARL but interpreted instead as DS4 using PSF, simply by changing the reconstruction. This is of clinical importance because the cutoff between DS3 and DS4 is generally used to distinguish responders from nonresponders. Hence, whereas PSF may not have a major impact on PET interpretation for the overall study population, it could have potential consequences for approximately 1 in 6 patients who would be deemed responders using the standard EARL reconstruction but nonresponders using PSF. Additionally, changes in reconstruction would not be expected to alter the progression and overall survival of the whole population. The study by Enilorac et al. (6) was not powered to show such a difference, but even in large studies in aggressive non-Hodgkin lymphomas, such as the PETAL study (862 patients) (7), the risk stratification provided by PET did not alter patient outcomes. This is due to the ineffectiveness of current salvage treatment options for patients at high risk of relapse. This situation may change with more promising agents, which are currently being tested in relapsed/refractory patients with DLBCL. We believe this is a strong argument against altering the status quo in multicenter trials without further evaluation.
In clinical practice, we also consider that reads should be performed with caution using resolution modeling, in particular when patient scans are evaluated near the decision threshold between clinically negative and positive findings, that is, in lymphoma between DS3 and DS4, as using newer reconstructions tends to shift findings to produce more positive reads (3). This is also demonstrated by Enilorac et al. (6). The conclusion drawn by Enilorac et al. (6) is only correct when considering all patients in their study, dominated by the large fraction of DS1, DS2, and DS3 subjects seen with PSF reconstructions. However, the paper also demonstrates that the choice of reconstruction method (EARL vs. PSF) does affect DSs, in particular for patients being evaluated around the clinically relevant cutoff as DS3 with EARL or DS4 with PSF. An illustrative example was also shown in that paper in Figure 1. We believe that the use of PSF reconstruction is not detrimental but beneficial for lesion detectability (8,9) and should be further pursued. Yet, resolution modeling should be used with caution, in particular in small lesions (1.0–1.5 cm in diameter) having a DS of 3 or 4 and if treatment change is planned, until a revisit or update of the Deauville scoring system has been made to accommodate these new reconstruction approaches. Moreover, PSF reconstructions are not necessarily the same nor behave the same on each (type of) PET/CT system. Results obtained with one system can therefore not be generalized to all other systems. The different PSF implementations will therefore result in performance variabilities across systems. For multicenter studies, use of PSF reconstruction mandates an update of harmonizing performance standards. Recently, a first feasibility study for harmonizing performance of state-of-the-art PET/CT systems was published by Kaalep et al. (10). Once these new standards have been implemented, the impact of PSF reconstructions in multicenter studies on image interpretation, for example, Deauville scoring, can be determined in a standardized manner and may imply that interpretation criteria will need to be adapted, in particular for patients with scans evaluated as DS3 or DS4.
DISCLOSURE
Professor Barrington acknowledges support from the National Institute of Health Research (NIHR; RP-2-16-07-001). King’s College London and UCL Comprehensive Cancer Imaging Centre is funded by the CRUK and EPSRC in association with the MRC and Department of Health (England). Professor Boellaard is a member of the EARL scientific advisory board (unpaid) and has collaborative research programs with Philips and Siemens Healthcare. Professor Barrington receives research funding from Siemens Healthcare. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR, or the Department of Health. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 6, 2018.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.