


Abstract
Nintedanib is an oral angiokinase inhibitor used as second-line treatment for non–small cell lung cancer. New radiotracers, such as 68Ga-DOTA-E-[c(RGDfK)]2, that target αvβ3 integrin might have an impact as a noninvasive method for assessing angiogenesis inhibitors. Methods: From July 2011 through October 2015, 38 patients received second-line nintedanib plus docetaxel. All patients underwent PET/CT with 68Ga-DOTA-E-[c(RGDfK)]2 radiotracer and blood-sample tests to quantify angiogenesis factors (fibroblast growth factor, vascular endothelial growth factor, and platelet-derived growth factor AB) before and after completing 2 therapy cycles. Results: Of the 38 patients, 31 had available baseline and follow-up PET/CT. Baseline lung tumor volume addressed with 68Ga-DOTA-E-[c(RGDfK)]2 PET/CT correlated with serum vascular endothelial growth factor levels, whereas baseline lung/liver SUVmax index correlated with platelet-derived growth factor AB. After treatment, the overall response rate and disease control rate were 7.9% and 47.3%, respectively. A greater decrease in lung tumor volume (−37.2% vs. –27.6%) was associated with a better disease control rate in patients (P = 0.005). Median progression-free survival was 3.7 mo. Nonsmokers and patients with a higher baseline lung tumor volume were more likely to have a higher progression-free survival (6.4 vs. 3.74 [P = 0.023] and 6.4 vs. 2.1 [P = 0.003], respectively). Overall survival was not reached. Patients with a greater decrease in lung SUVmax (not reached vs. 7.1 mo; P = 0.016) and a greater decrease in the lung/spleen SUVmax index (not reached vs. 7.1; P = 0.043) were more likely to have a longer overall survival. Conclusion: 68Ga-DOTA-E-[c(RGDfK)]2 PET/CT is a potentially useful tool for assessing responses to angiogenesis inhibitors. Further analysis and novel studies are warranted to identify patients who might benefit from this therapy.
Lung cancer is the leading cause of cancer death worldwide (1). Most patients are diagnosed with advanced disease, and most patients treated with first-line platinum-based chemotherapy will experience disease progression after 3–7 mo and require second-line therapy (2). Tumors grow by inducing endothelial proliferation to increase existing blood vessels in order to supply the tumor with oxygen and nutrients. Antiangiogenic tyrosine kinase inhibitors have demonstrated a cytostatic effect on tumor cells by slowing growth and preventing development of distant metastases. Nintedanib, an oral angiokinase inhibitor, targets the proangiogenic pathways mediated by vascular endothelial growth factor (VEGF) receptors 1–3, fibroblast growth factor receptor, and platelet-derived growth factor receptors α and β (3,4). Hypoxia is the most potent stimulus for their production by activating hypoxia-inducible factor 1α, which upregulates proangiogenic factors, resulting in rapid tumor growth (5). VEGF is the most studied and influential proangiogenic factor in the tumoral angiogenic process. Targeting VEGF has become relevant because of its potential for use of new drugs (6). Preclinical studies with nintedanib reported sustained blockade of VEGF receptor 2 in vitro and tumor growth arrest (3). In phase 1 and 2 clinical trials, nintedanib showed a manageable safety profile and antitumor activity in patients with solid tumors, including non–small cell lung cancer (NSCLC) (4,7). The LUME-Lung 1 study demonstrated that patients with adenocarcinoma histology experienced significant improvement in median overall survival (OS) and progression-free survival (PFS) with nintedanib plus docetaxel versus docetaxel alone (7,8). Importantly, the subgroup of patients who experienced progression within 9 mo after starting first-line therapy had a significantly longer OS, with a 3-mo increase.
Integrins play a major role in adhesion of cells to extracellular matrix proteins. They are also responsible for regulating removal from the cell cycle and cell migration (9). The αvβ3 integrin is a transmembrane protein constituting 2 subunits, α and β, and is generally expressed on mature endothelial and epithelial cells, as well as on tumor cells. It favors growth of several angiogenesis-dependent tumors (10). The αvβ3 integrin can bind to the arginine-glycine-aspartic acid (RGD) amino acid sequence present in extracellular matrix proteins, such as vitronectin, fibrinogen, and laminin (11). Because of this characteristic, αvβ3 integrin has been identified as a molecular target for noninvasive monitoring of malignant cells and treatment response assessment (12,13). Furthermore, Zannetti et al., using in vivo murine models, have shown that this peptide does not exhibit a cross-reaction with αvβ5, which confers high selectivity in nuclear imaging (14). Recently, significant progress has been made in the development of new imaging techniques, including 15O-labeled radiotracers such as 15O water and C15O, which have been used to quantify tumor perfusion that might be related to angiogenesis. In parallel, αvβ3-targeting radiotracers for the visualization of αvβ3 expression in tumors by PET/CT have been synthesized, resulting in the use of the generator-produced radionuclide 68Ga-DOTA-E-[c(RGDfK)]2 (10,13). The application of 68Ga-DOTA-E-[c(RGDfK)]2–labeled peptides has attracted interest in cancer imaging because of their physical characteristics along with improved tumor targeting (15,16).
Antiangiogenic therapy is a promising treatment for malignancies, including lung cancer. Because these are designed to inhibit tumor growth and dissemination instead of causing direct cytotoxicity, they cannot cause tumors to shrink rapidly in the short term; evaluation of response by CT or 18F-FDG PET/CT is therefore difficult (17). However, the 68Ga-DOTA-E-[c(RGDfK)]2 peptide is a suitable ligand for the noninvasive visualization of αvβ3 expression in vivo that can provide information on molecular processes such as angiogenesis and its correlation with chemotherapy response and prognosis (10,13,15). In the current study, we tested the ability of PET/CT with the radiotracer 68Ga-DOTA-E-[c(RGDfK)]2 to assess therapeutic responses to treatment with nintedanib plus docetaxel in lung adenocarcinoma. Furthermore, we evaluated the prognosis as determined by survival.
MATERIALS AND METHODS
Patients
This study was performed at the Instituto Nacional de Cancerología in Mexico City. All patients were adults (>18 y old) who had histologically confirmed stage IIIB or IV lung adenocarcinoma failing to respond to platinum-based first-line chemotherapy, an Eastern Cooperative Oncology Group performance status of less than 2, and measurable disease according to RESIST (version 1.1). We excluded patients who had active brain metastases, received previous docetaxel, or had a recent history (<3 mo) of clinically significant hemoptysis or a major thrombotic or clinically relevant major bleeding event in the past 6 mo. All patients provided written informed consent. The study complied with the protocol and with the Declaration of Helsinki. The protocol was approved by an independent local ethics committee (015/007/ICI) (CEI/889/15).
Treatment Regimen
The patients received docetaxel, 75 mg/m2, on day 1 plus nintedanib, 200 mg twice daily orally, on days 2–21, every 3 wk. Four cycles were given in combination, and then nintedanib was given alone as maintenance therapy. Nintedanib and docetaxel were provided by Boehringer Ingelheim as part of the Compassionate Use Program for nintedanib. Treatment was continued until disease progression or unacceptable toxicity. All patients were assessed for toxicities before starting each cycle according to the Common Terminology Criteria for Adverse Events (version 4.0).
Imaging
Before and after 2 cycles of treatment, all patients underwent 68Ga-DOTA-E-[c(RGDfK)]2 PET/CT using an mCT Excel 20 PET/CT scanner (Siemens) consisting of a bismuth orthosilicate full scanner and a 20-detector-row CT scanner. Whole-body CT was performed 40–50 min after injection of 188.7 MBq of 68Ga-RGD (±1.2), and transmission data were acquired using low-dose CT (120 kV, automated from 100 to 130 mA, a 512 × 512 matrix, a 50-cm field of view, a 3.75-mm slice thickness, and a 0.8-s rotation time), extending from the base of the skull to the proximal thighs. After the CT acquisition, a whole-body PET scan was acquired in 3 dimensions (matrix, 168 × 168). For each bed position (16.2 cm; overlapping scale, 4.2 cm), we used a 3-min acquisition time with a 15.5-cm field of view. The emission data were corrected for randoms, scatter, and decay. Reconstruction was conducted with an ordered-subset expectation maximization algorithm with 3 iterations and 12 subsets, Gauss-filtered to a transaxial resolution of 6 mm in full width at half maximum. Attenuation was corrected using low-dose nonenhanced CT. A workstation (Multimodality Workplace; Siemens) providing multiplanar reformatted images was used for image display and analysis. The median tumoral volume and the SUVmax of whole-body tumors were measured with the isocontour tool of the TrueD Syngo software (Siemens) using a threshold of 20% of the SUVmax, with manual adjustment.
Radiopharmaceutical Preparation
68Ga-DOTA-E-[c(RGDfK)]2 was synthesized according to the method described by López-Rodriguez et al. (16)
PET/CT Interpretation Criteria
68Ga-DOTA-E-[c(RGDfK)]2 PET/CT was performed before the start of treatment and again after 2 cycles of treatment. Negative PET/CT results were defined as tracer confined to normal-uptake organs (spleen, urinary bladder, liver) and no other sites with uptake (16,18). Positive results (progressive disease) were defined as at least one focus of abnormally intense uptake, characterized by visual inspection or SUVmax measurements. PET/CT images were visually analyzed by experienced nuclear medicine physicians.
Determination of Serum Angiogenesis Factors
Two serum samples were collected at baseline and after 2 therapy cycles. Serum levels were determined using enzyme-linked immunosorbent assays, which were performed using Quantikine human fibroblast growth factor, VEGF, and platelet-derived growth factor AB immunoassay kits (DFB50, DHD00C, and DVE00, respectively; R&D Systems). All assays were performed in duplicate.
Outcomes
The primary endpoint was disease control rate (DCR) addressed by 68Ga-DOTA-E-[c(RGDfK)]2 PET/CT. Secondary endpoints included overall response rate, PFS, OS, and toxicity profile. DCR was defined as the percentage of patients with advanced or metastatic NSCLC who achieved a complete response, a partial response, or stable disease after treatment with nintedanib plus docetaxel. The overall response rate was defined as the percentage of patients with advanced or metastatic NSCLC who achieved a complete and partial response to nintedanib plus docetaxel. PFS was defined as the time from the start of treatment with nintedanib until disease progression or death, and OS was defined as the time from the start of treatment with nintedanib until the last follow-up or death.
Statistical Analysis
Continuous variables were summarized as mean with SD, categoric variables as frequency and percentage. The χ2 or Fisher exact test was used to assess the significance of differences among categoric variables. Patients were stratified by DCR, and the median values for the PET/CT parameters were addressed by paired t tests considering baseline and follow-up values. The percentage change (%Δ) was also calculated for baseline and follow-up PET/CT parameters.
Median OS and PFS were estimated using the Kaplan–Meier method. The median follow-up was 8.8 mo (range, 6.2–11.4 mo). The log-rank test was used for comparisons among subgroups. A multivariate Cox–proportional hazard model was used. All variables were dichotomized for the survival analyses. Statistical significance was determined as a P value of 0.05 or less using a 2-tailed test. SPSS software (version 21; SPSS Inc.) was used for all statistical analysis.
RESULTS
Study Design
Forty-six patients were assessed for eligibility, and 8 were excluded. The remaining 38 patients underwent PET/CT with 68Ga-DOTA-E-[c(RGDfK)]2. Five patients did not complete therapy because of unacceptable toxicity (n = 1) or early disease progression (n = 4). Therefore, at the final follow-up, there were 33 patients, but 2 were excluded from the final analysis because of missing data (Fig. 1).
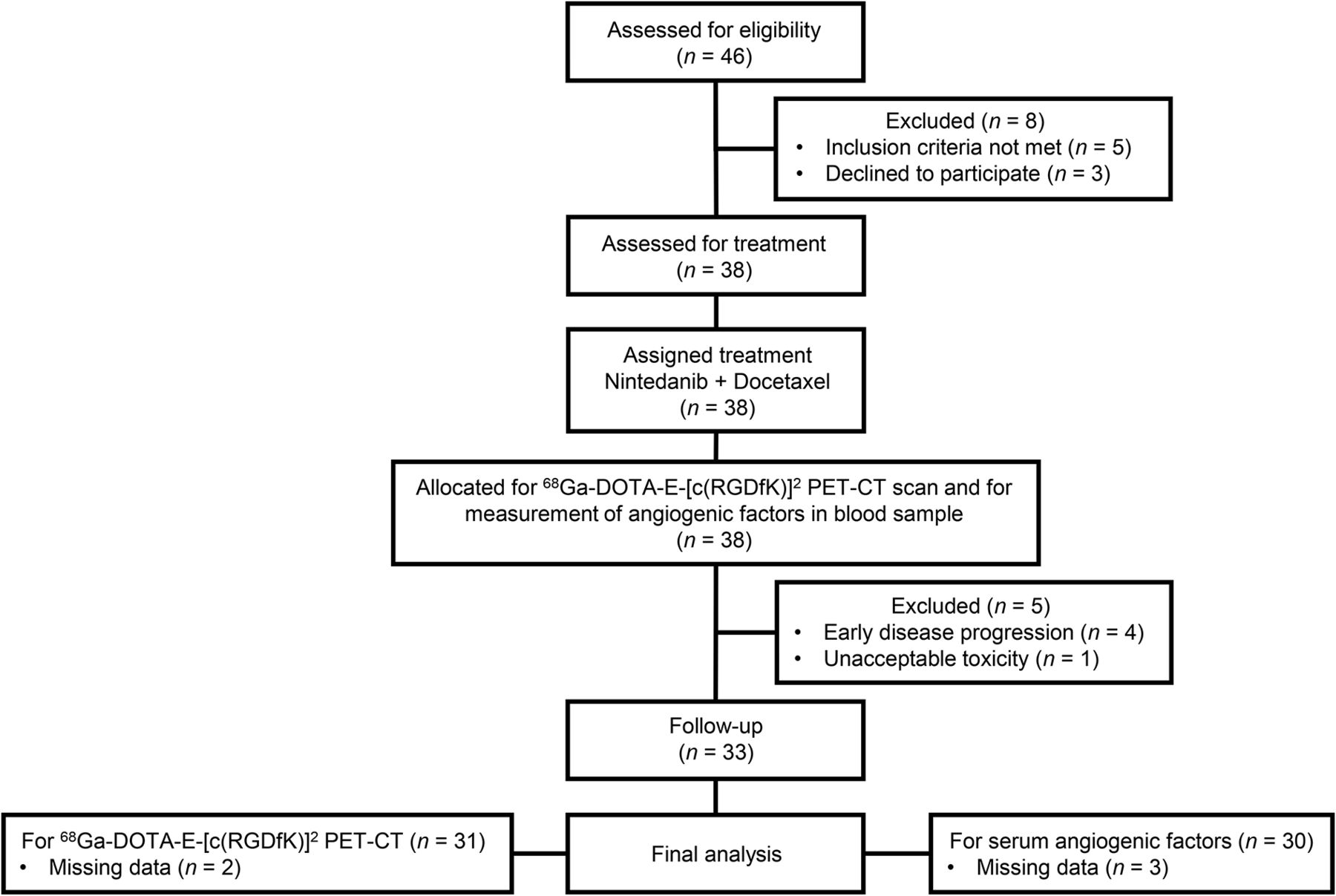
Flow diagram of patients included in analysis.
Characteristics of Patients
Among the 38 patients, 16% (6/38) had diabetes and 29% (11/38) had systemic hypertension at enrollment. Most patients had a good Eastern Cooperative Oncology Group performance status (<2) (97%; 37/38). The most common lung adenocarcinoma histologic subtypes were acinar (21%) and papillary (16%) The first-line overall response rate and DCR were 47% (18/38) and 74% (28/38), respectively (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org).
Treatment Characteristics
The overall response rate and DCR for nintedanib plus docetaxel were 8% (3/38) and 47% (18/38), respectively. When we analyzed the patients stratified by DCR with nintedanib, we did not find differences among them by sex, median age, exposure to tobacco, diabetes, number of metastases, histologic grade differentiation, or median carcinoembryonic antigen. The presence of systemic hypertension was associated with a better DCR (77.8 vs. 22.2), although the difference was not statistically significant (P = 0.125) (Supplemental Table 2).
Adverse Events
Only 34% (13/38) of patients experienced severe adverse events requiring hospitalization. The most frequent adverse events were anemia (68%), nausea (66%), leukopenia (63%), and dyspnea (61%). The most common severe adverse events (graded ≥ 3) were neutropenia (21%), dyspnea (18%), leukopenia (16%), and asthenia (13%).
Assessment of 68Ga-DOTA-E-[c(RGDfK)]2 PET/CT Radiotracer
Figure 2 shows the therapeutic response to antiangiogenic therapy. The 68Ga-DOTA-E-[c(RGDfK)]2 PET/CT scan before treatment showed intense avidity for the radiotracer in the right lung lesion and in the ipsilateral and contralateral mediastinal lymph nodes, with an SUVmax of 7.6. The follow-up PET/CT scan showed a significant reduction of avidity in the lung lesion and lymph nodes, with a decreased SUVmax of 3.5 (Fig. 2).
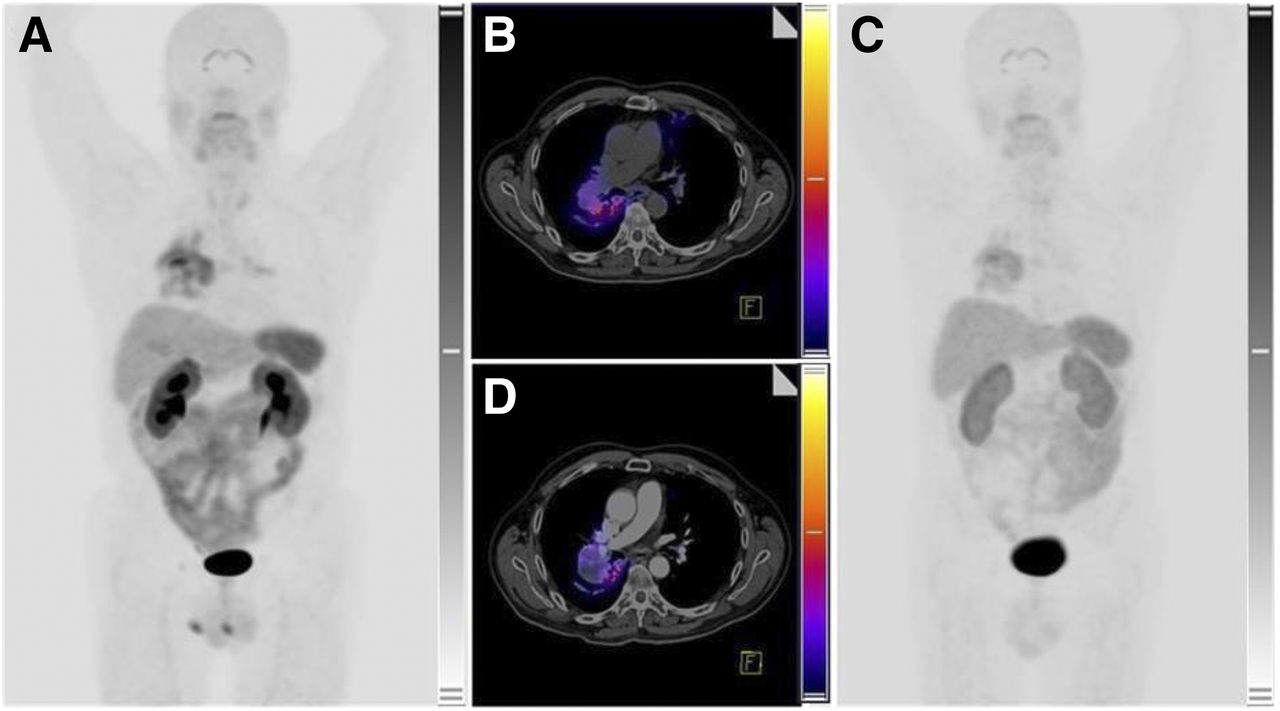
A 62-y-old man with lung adenocarcinoma. (A and B) 68Ga-DOTA-E-[c(RGDfk)]2 PET/CT before treatment with multikinase inhibitors shows intense avidity for radiotracer in right lung lesion and in ipsilateral and contralateral mediastinal lymph nodes. Tumor volume is 178 cm3, with SUVmax of 7.6. (C and D) PET/CT posttherapy images show significant reduction of avidity in lung lesion and lymph nodes, with tumor volume of 56 cm3 and SUVmax of 3.5 (scale, 0–10 SUV-body weight). PFS of this patient was 6 mo.
Baseline, Follow-up, and %Δ in 68Ga-DOTA-E-[c(RGDfK)]2 PET/CT Parameters and Angiogenic Factors
The assessment parameters for 68Ga-DOTA-E-[c(RGDfK)]2 PET/CT are shown in Table 1. After treatment with nintedanib plus docetaxel, the parameters that showed a statistically significant reduction were lung/spleen SUVmax index (%Δ, −13%; P = 0.022) and lung tumor volume (%Δ, −38%; P = 0.002). By contrast, the follow-up parameters that showed an increase after the antiangiogenic therapy were fibroblast growth factor (%Δ, 125%; P = 0.030) and platelet-derived growth factor AB (%Δ, 70%; P = 0.035) (Table 1).
Baseline, Follow-up, and %Δ in 68Ga-DOTA-E-[c(RGDfK)]2 PET/CT and Angiogenic Soluble Factors (n = 31)
68Ga-DOTA-E-[c(RGDfK)]2 PET/CT Parameters and Therapeutic Response to Nintedanib
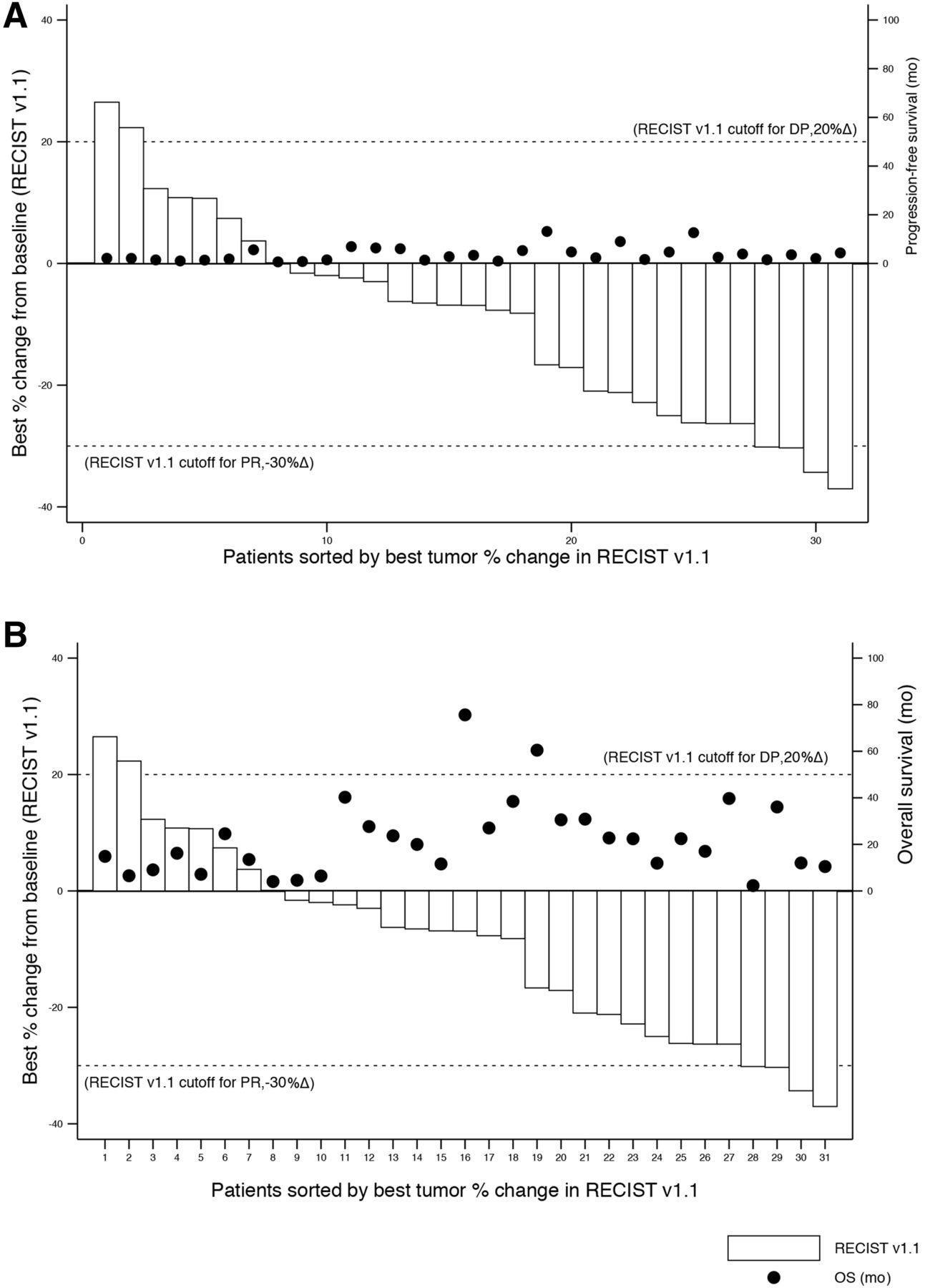
PET/CT parameters stratified according to DCR showed that patients who did not achieve disease control had a higher and significant (P = 0.008) %Δ reduction (−30%) in lung tumor/spleen SUVmax index, compared with patients who achieved disease control (−13%; P = 0.806). By contrast, patients who achieved disease control had a higher and significant decrease in lung tumor volume (−37%; P = 0.005) than patients who did not achieve disease control (−28%; P = 0.088). When we compared %Δ in lung tumor volume as assessed by RESIST with %Δ in baseline lung tumor SUVmax as assessed by 68Ga-DOTA-E-[c(RGDfK)]2 PET/CT, we found that most patients who achieved disease control had a decrease in %Δ in lung tumor SUVmax (Fig. 3).
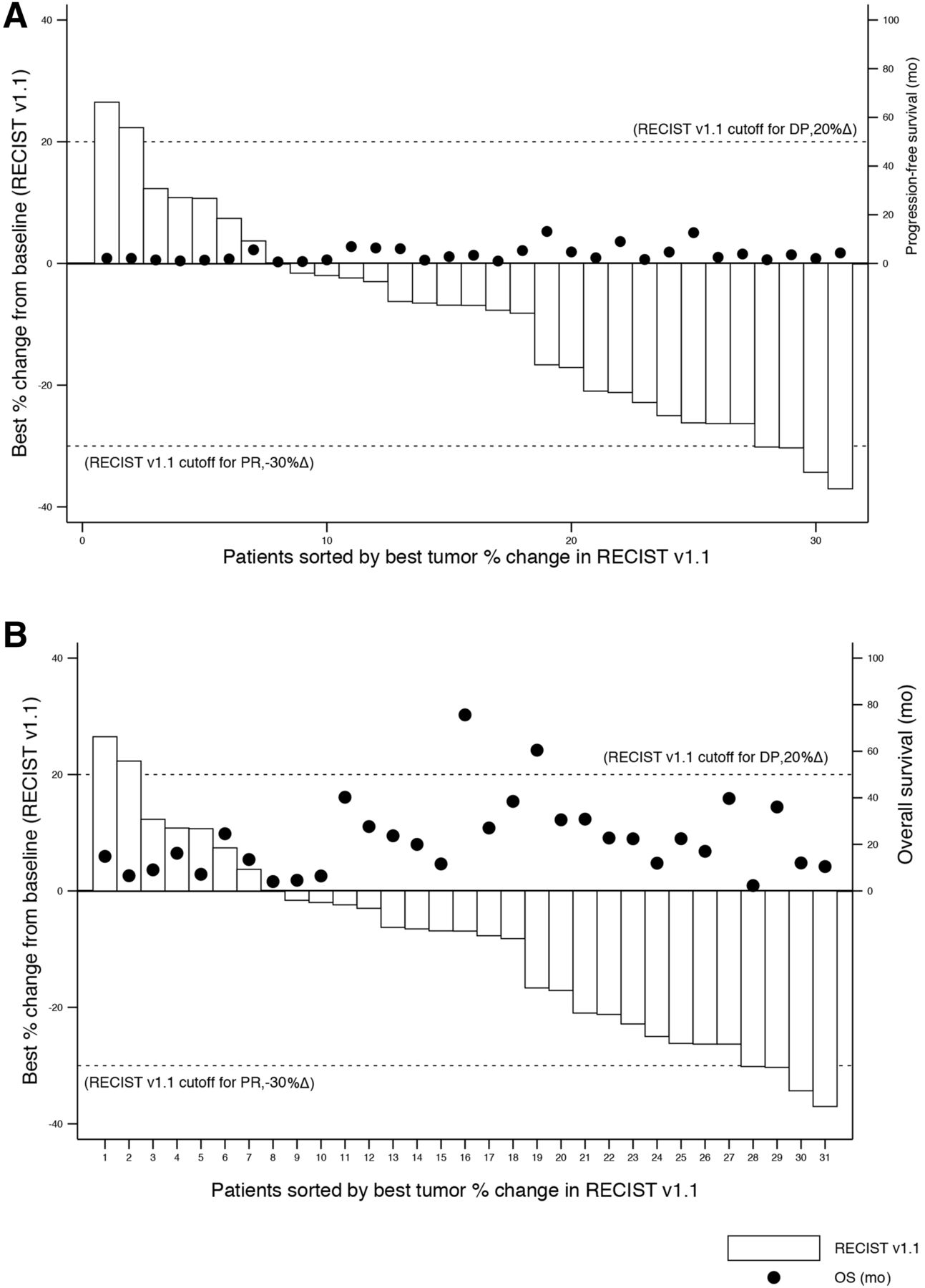
Waterfall plots of %Δ in tumoral volume by RECIST (A) and by lung tumor SUVmax measured with 68Ga-DOTA-E-[c(RGDfk)]2 PET/CT (B). PR = partial response.
68Ga-DOTA-E-[c(RGDfK)]2 PET/CT Parameters and Angiogenic Factors
When the relationship between 68Ga-DOTA-E-[c(RGDfK)]2 PET/CT parameters and angiogenic factors (fibroblast growth factor, VEGF, platelet-derived growth factor AB) was analyzed, a positive correlation was found between baseline lung tumor/liver SUVmax index and baseline platelet-derived growth factor AB (r2 = 0.418; P = 0.030). Likewise, baseline lung tumor volume and baseline VEGF showed a positive correlation with each other (r2 = 0.574; P = 0.003).
Factors Associated with PFS and OS
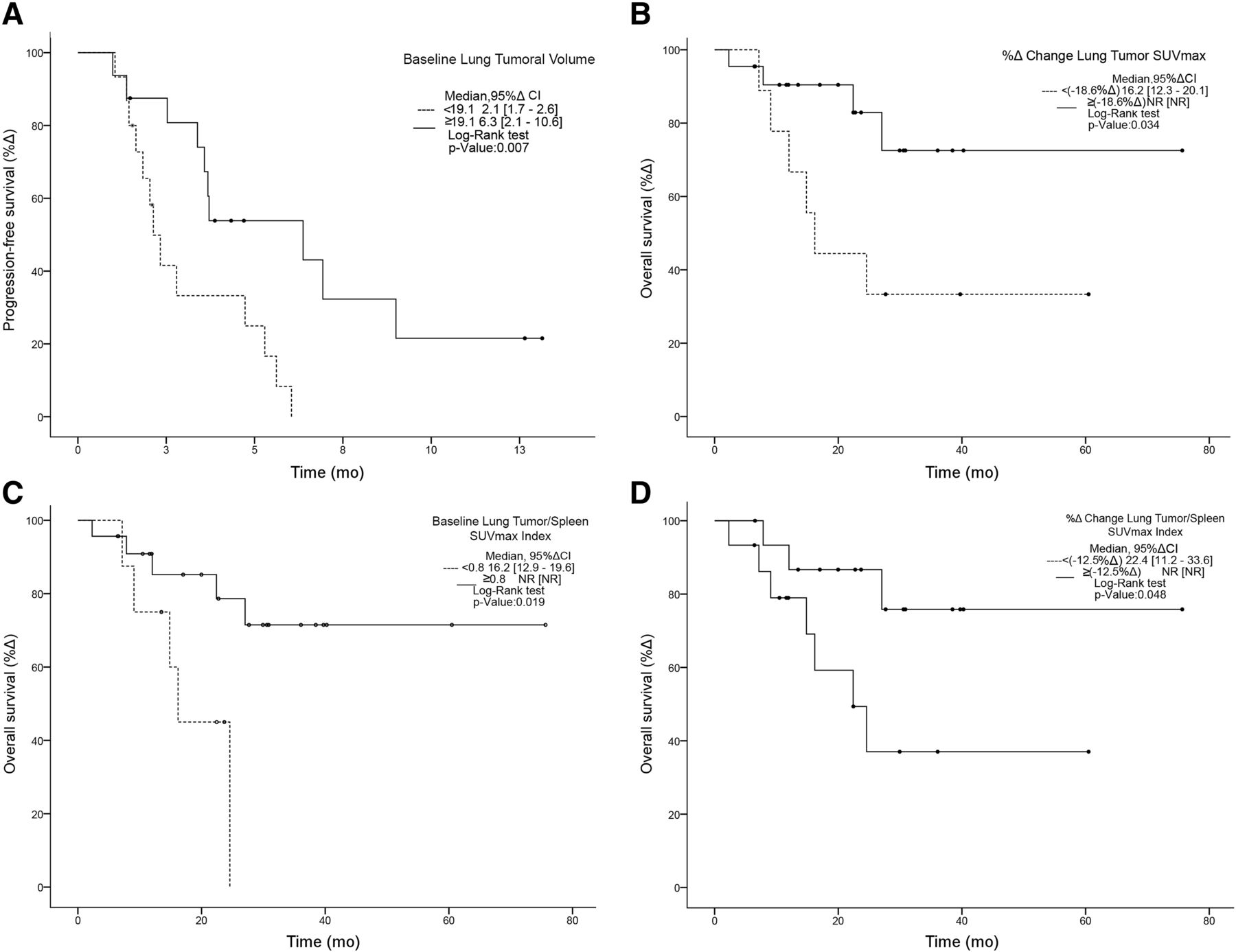
The median PFS was 3.7 mo. A greater baseline lung tumor volume (≥19.1 vs. < 19.1) was associated with a higher PFS (6.4 vs. 2.1; P = 0.007). (Fig. 4). In the multivariate analysis, systemic hypertension was associated with longer PFS (hazard ratio, 0.2; 95% confidence interval, 0.1–0.80; P = 0.021).
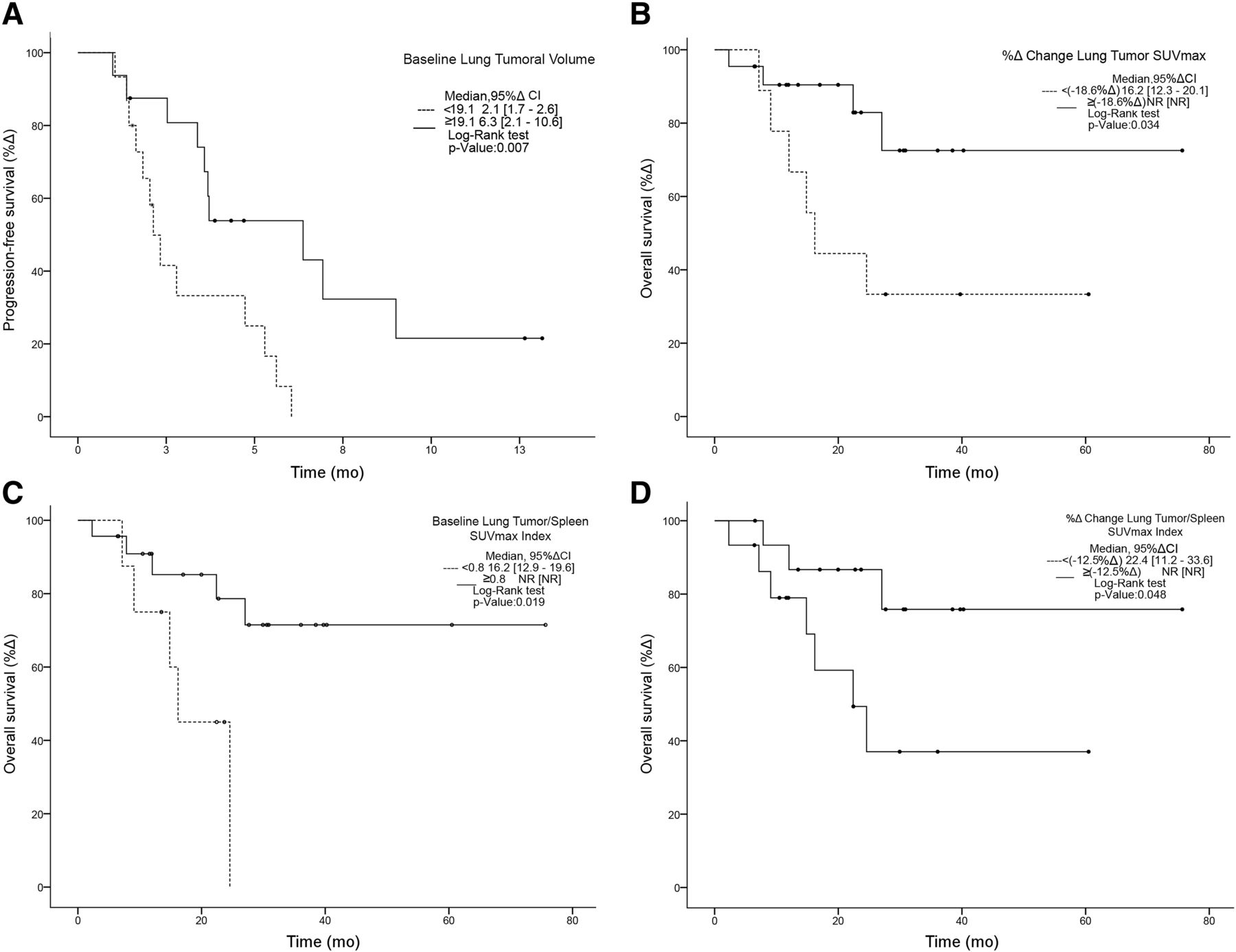
Kaplan–Meier curves for significant differences in PFS (A) and OS (B–D). CI = confidence interval; NR = not reached.
OS was not reached. A higher %Δ in lung tumor SUVmax (≥−19% vs. <−19%) was associated with a higher OS (not reached vs. 7.1; P = 0.016). Patients with a higher baseline lung tumor/spleen SUVmax index (≥0.8 vs. <0.8) were more likely to have a longer OS (not reached vs. 4.6 mo; P = 0.022). Moreover, a higher lung tumor/spleen SUVmax index (≥−13% vs. <13%) was associated with a higher OS (not reached vs. 7.8; P = 0.043) (Fig. 4). In the multivariate analysis, %Δ in lung tumor SUVmax was associated with a worse OS (hazard ratio, 3.1; 95% confidence interval, 1.0–9.8; P = 0.048).
DISCUSSION
Targeted therapies have changed treatment for lung cancer patients. Nevertheless, the treatment of most will progress to chemotherapy alone. Antiangiogenic agents have been studied in NSCLC with poor results. Bevacizumab, a monoclonal antibody against serum VEGF, improved prognosis in first-line settings in combination with paclitaxel or pemetrexed (17,19). NSCLC patients harboring an EGFR mutation have also shown a better PFS when treated with the combination of a tyrosine kinase inhibitor plus bevacizumab. In the JO25567 trial, erlotinib plus bevacizumab improved PFS versus erlotinib alone (16 vs. 9.7 mo; hazard ratio, 0.054) (17).
Phase III studies on second-line therapy, such as the ZODIAC study (vandetanib ± docetaxel), the ZEAL study (vandetanib ± pemetrexed), and the ZEST study (vandetanib vs. erlotinib), have tested the efficacy of antiangiogenics and reported a limited impact on OS for advanced NSCLC patients (20).
Despite these results, there are two antiangiogenic agents that show promise for improving OS after progression on first-line therapy: ramucirumab and nintedanib. Nintedanib is a triple-angiokinase inhibitor targeting fibroblast growth factor, platelet-derived growth factor AB, and VEGF; high levels of the last of these confer a poor prognosis in NSCLC (21). The LUME-Lung 1 study, a phase III trial, improved survival rates at 1 y (52.7% vs. 44.7%) and 2 y (25.7% vs. 19.1%) in patients with disease refractory to first-line therapy, especially those with adenocarcinoma. This finding sets the base for biomarker correlation analyses and stratified treatment response assessment (8).
Potential biomarkers for angiogenesis have been studied, particularly with anti-VEGF antibodies (22,23). A phase 2/3 trial with carboplatin and paclitaxel with or without bevacizumab reported that low VEGF levels may predict a better PFS (P = 0.04). Therefore, serum VEGF levels could potentially serve as a tool for identifying patients who might benefit from antiangiogenic inhibitors.
The current need for early diagnosis, stratification, and treatment response assessment has led to innovative techniques for nuclear medicine and molecular imaging. Medical imaging has an advantage as a biomarker by being a noninvasive method that can provide a variety of information about the tumor (24). Integrated PET/CT using 18F-FDG, the most widespread image radiotracer, can visualize tumor viability, tumor anatomy, and the surrounding normal tissues. The reported sensitivity, specificity, and accuracy of 18F-FDG PET/CT are 89%, 94%, and 93%, respectively (25). However, it lacks tumor specificity and has poor uptake in tumor-related neovascularization (18,26). Thus, new approaches and optimal imaging methods must be established for new drugs, such as antiangiogenic therapies.
An increased expression of αvβ3 integrin in tumoral endothelium and tumor cells is associated with invasion and metastasis (27). Furthermore, the 2-subunit composition of αvβ3 integrin makes it a suitable, although not exclusive, receptor for the RGD sequence in the 68Ga-DOTA-E-[c(RGDfK)]2 radiotracer. In fact, other integrins (e.g., αvβ5, αvβ6) are also related to RGD amino acid sequence binding (28,29). The αvβ3 integrin is targetable by various radiolabeled RGD peptides (30). Histologically, RGD peptides target tumor vasculature via RGD-integrin αvβ3 interaction, with little extravasation. Therefore, decreased αvβ3 integrin expression measured by this imaging method can be associated with proper antiangiogenic blockade (28). However, because tumor cells are also known to express several integrins, the overall uptake of an RGD peptide may very well be influenced by the expression of αvβ3, or other integrins, on the tumor tissue (27).
This study represents, to the best of our knowledge, the first evaluation of the response to nintedanib plus docetaxel in lung adenocarcinoma patients using 68Ga-DOTA-E-[c(RGDfK)]2 PET/CT as a surrogate biomarker. Our study also develops a prognostic model using dynamic molecular imaging. We demonstrate the relationship that exists between angiogenic metabolic volume and response to the multikinase inhibitor—a relationship that would follow from that between RGD peptide uptake and union to αvβ3 integrins. In this second-line study using a targeted agent with chemotherapy, we determined survival rates (OS and PFS), therapy response rates (overall response rate and DCR), and statistical correlations between PET/CT parameters and clinical characteristics.
For the overall response rate and DCR assessment by PET/CT, the results resembled those of the LUME-Lung 1 study, with no precedent of a tyrosine kinase inhibitor in combination with chemotherapy as second-line treatment, the response to which was measured using 68Ga-DOTA-E-[c(RGDfK)]2 PET/CT. The main parameter used to assess overall response rate was tumor volume, which showed a statistically significant reduction, mainly because of the metabolic decrease in target lesions after 2 cycles of nintedanib plus docetaxel. There were also significant differences in the uptake rate of 68Ga-DOTA-E-[c(RGDfK)]2 in DCR between responders and nonresponders. Another important finding was that variations in the RECIST measurement and the lung tumor %Δ in SUVmax seemed similar, which highlights that this study, one of the first of its class, could achieve the intended regulation for the use of 68Ga-DOTA-E-[c(RGDfK)]2 PET/CT as a method to monitor disease control for antiangiogenic drugs.
Additionally, when we assessed PFS, a higher baseline lung tumor volume was associated with a longer period until progression, which was consistent with previous results (16,31,32). Thus, a higher targetable metabolic area might be associated with a higher tumor burden and therefore with a potentially higher treatment efficacy. We also observed that a higher %Δ in lung tumor SUVmax and in lung tumor/spleen SUVmax index affected OS but not PFS. These findings suggest a high correlation with therapeutic response to nintedanib. Our observations are consistent with a previous study investigating a 68Ga-labeled pegylated RGD dimer (28). Validated by ex vivo immunohistochemistry, the authors found that the RGD radiotracer uptake was significantly reduced after antiangiogenic therapy, reflecting tumor response significantly earlier than is possible with 18F-FDG PET/CT. Contrary results were reported by Rylova et al., who studied 68Ga-NODAGA-RGD for the in vivo monitoring of bevacizumab monotherapy in human squamous cell carcinoma xenografts in mice (33). Despite a reduced αvβ3 integrin expression under VEGF inhibition, they observed an increased binding of 68Ga-NODAGA-RGD in the investigated A-431 xenografts. Rylova et al. therefore concluded that RGD radiotracer uptake might not reflect changes in αvβ3 integrin expression at the molecular level. They hypothesized that bevacizumab may activate αvβ3 integrin, causing a higher affinity to 68Ga-NODAGA-RGD and consequently increased radiotracer uptake in vivo (33). Assuming a high-affinity state of αvβ3 integrin, however, one would expect an increased binding of the primary anti–αvβ3 integrin antibody used in the immunohistochemical stainings and consequently false high αvβ3 integrin levels. However, in line with our results, the authors found a reduced αvβ3 integrin expression in the therapy group. In addition, VEGF is known to indirectly activate αvβ3 integrin (34).
Our study had limitations, such as sample size and the relatively immature data used for estimating OS. Nonetheless, our study had the advantage of being the first prospective clinical trial assessing therapeutic response with 68Ga-DOTA-E-[c(RGDfK)]2, which in the future might also become a delivering radiotracer for refractory patients. Additionally, our results showed a high concordance with those of the LUME-1 study, had a larger population-based clinical trial, and highlighted a similar therapeutic response among Caucasian, Asian, and Hispanic patients with adenocarcinoma treated with nintedanib plus docetaxel.
CONCLUSION
68Ga-DOTA-E-[c(RGDfK)]2 PET/CT is a potentially useful tool for assessing response to angiogenesis inhibitors. The present study may provide the clinical basis for future studies investigating RGD-based hybrid imaging for monitoring therapeutic responses to molecular cancer therapies. RGD-based hybrid imaging may allow for a noninvasive real-time molecular typing of lung adenocarcinoma under antiangiogenic treatment, adding complementary biomarkers of a therapeutic response to morphology-based and functional tumor response assessments.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Acknowledgments
This work was presented as a poster at the 2016 World Conference on Lung Cancer in Vienna, Austria.
Footnotes
Published online Aug. 17, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 28, 2017.
- Accepted for publication July 13, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}