


Abstract
Imaging of myocardial fatty acid metabolism using 123I-betamethyl-p-iodophenyl-pentadecanoic acid (123I-BMIPP) SPECT is useful for identifying high-risk patients with known ischemic heart disease. However, its utility for patients who have nonischemic heart failure with preserved ejection fraction is not well known. This study aimed to evaluate the prognostic value of the 123I-BMIPP defect score in such patients. Methods: Of 804 consecutive patients who were admitted to the hospital because of acute heart failure and underwent 123I-BMIPP SPECT, we identified 133 (mean age ± SD, 73 ± 13 y) who had normal coronary arteries by invasive coronary angiography and preserved left ventricular ejection fraction (≥50%) by echocardiography. 123I-BMIPP defects were quantitatively scored to obtain summed defect scores in 17 segments of 123I-BMIPP SPECT images. The patients were divided into 2 groups based on their score. The multivariate Cox model was used to assess a possible correlation between a higher score (≥4, n = 46) and major adverse cardiac events, including cardiac death, cardiovascular events, and hospitalization for heart failure, compared with a lower score (<4, n = 87). Results: During a mean follow-up of 2.5 y, 35 major adverse cardiac events occurred. The median scores in the high-score and low-score groups were 7.13 ± 4.21 and 1.29 ± 0.80, respectively. By multivariate Cox analysis, a higher score was associated with increased major adverse cardiac events, compared with a lower score (hazard ratio, 11.04; 95% confidence interval, 4.93–24.74; P < 0.001). Conclusion: This study demonstrated that the defect score by 123I-BMIPP SPECT may have potential prognostic value in patients who have nonischemic heart failure with preserved ejection fraction.
Heart failure (HF) contributed to 1 in 9 deaths in 2009, and half of those patients who develop HF die within 5 y of diagnosis (1), regardless of whether left ventricular ejection fraction (EF) is reduced or preserved (2). Despite the high prevalence of patients who have HF with preserved EF (3), its prognosis has not improved during the past 2 decades (4). The most common cause is diastolic HF (5), and no pharmacologic treatment has been proven to improve survival or shown to be effective in large clinical trials (6,7).
Myocardial perfusion imaging plays an important role in the assessment of cardiovascular event risk among patients with suspected coronary artery disease (8,9). 123I-betamethyl-p-iodophenyl-pentadecanoic acid (123I-BMIPP) SPECT images are useful for the diagnosis and risk stratification of patients with coronary artery disease, and the prognostic value of 123I-BMIPP for patients with ischemic heart disease has been extensively studied (10,11). However, the prognostic utility of 123I-BMIPP defect score among patients with nonischemic HF has not been well examined (12). In the present study, we investigated whether the defect score is associated with major adverse cardiac events (MACE) in patients who have nonischemic HF with preserved EF.
MATERIALS AND METHODS
Patient Population
Among 804 consecutive patients who were admitted to our hospital because of congestive HF and underwent 123I-BMIPP SPECT between January 2010 and January 2014, we identified 202 with nonischemic HF and no history of coronary artery disease. We finally enrolled 133 patients who showed no obstructive coronary artery disease (<50% stenosis) by coronary artery angiography and preserved EF (≥50%) by echocardiography (Fig. 1). We assessed clinical characteristics such as age, sex, coronary risk factors, blood biochemical data, echocardiography data, and drug treatment. The institutional review board approved this retrospective study, and the requirement to obtain informed consent was waived (M16075).
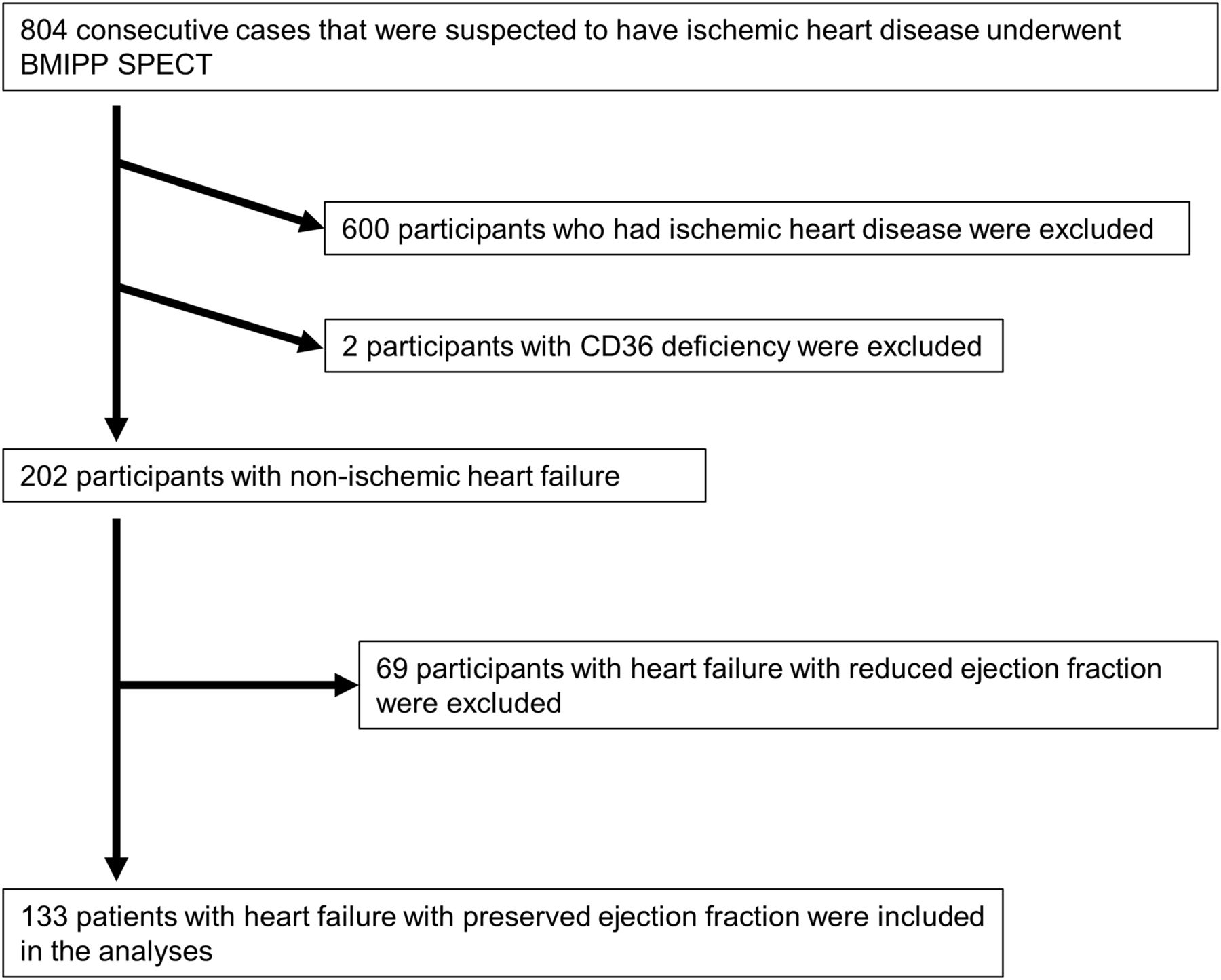
Flowchart of patient inclusion and exclusion criteria.
Invasive Coronary Angiography
All study participants underwent quantitative invasive coronary angiography, performed by experienced interventionalists in accordance with the American College of Cardiology/American Heart Association guideline (13). Coronary stenosis was defined as a decrease of more than 50% in arterial diameter as shown by invasive coronary angiography.
Echocardiographic Imaging
Echocardiographic images were obtained from the parasternal window for evaluation of left ventricular function (Vivid E9device; GE Healthcare). EF was calculated using the Teichholz formula (14). An EF of more than 50% was defined as a preserved EF.
123I-BMIPP SPECT
Patients were injected with 123I-BMIPP (111 MBq) while resting. The 123I-BMIPP SPECT data were acquired starting 20 min thereafter using a triple-head γ-camera (Prism IRIX; Philips) equipped with low-energy general-purpose collimators. The data were acquired over 360° in 72 steps of 37.5 s each in a 64 × 64 matrix. Images were processed using a Butterworth filter (order, 8.0; cutoff value, 0.25 cycle per pixel) and reconstructed by filtered backprojection.
Automated Quantitation of Myocardial SPECT Images
We used an automated program for myocardial SPECT (Heart Risk View-S software; Nihon Medi-Physics Co. Ltd.) to calculate the 123I-BMIPP defect score. The algorithm for generating a polar map was a hybrid 2-part sampling method (15) that operates in 3-dimensional space and uses short-axis images to generate count profiles from a 3-dimensional sampling scheme of short-axis slices. The software requires manual setting of the left ventricular cavity and then generates polar maps from myocardial SPECT data, which are divided into 17 segments based on American Society of Nuclear Cardiology guidelines to calculate the mean count in each segment (16). These mean counts were compared with the reference 123I-BMIPP database developed for Japanese patients by the Japanese Society of Nuclear Medicine working group (17,18). The mean percentage uptake in each segment was derived and then converted to scores using a 5-point grading system (0, normal; 1, mildly reduced; 2, moderately reduced; 3, severely reduced; and 4, absent). The scores in each segment were summed to obtain the total defect score per patient.
Assessment of Clinical Outcome
The endpoint was defined as the occurrence of MACE, including cardiac death, which was defined as death caused by HF, acute myocardial infarction, lethal ventricular arrhythmias, or other definitive cardiac disorders, cardiovascular events (acute myocardial infarction, unstable angina), or severe HF requiring hospitalization. The event data were retrospectively gathered from patients’ records, including in-hospital and out-of-hospital reports.
Statistical Analysis
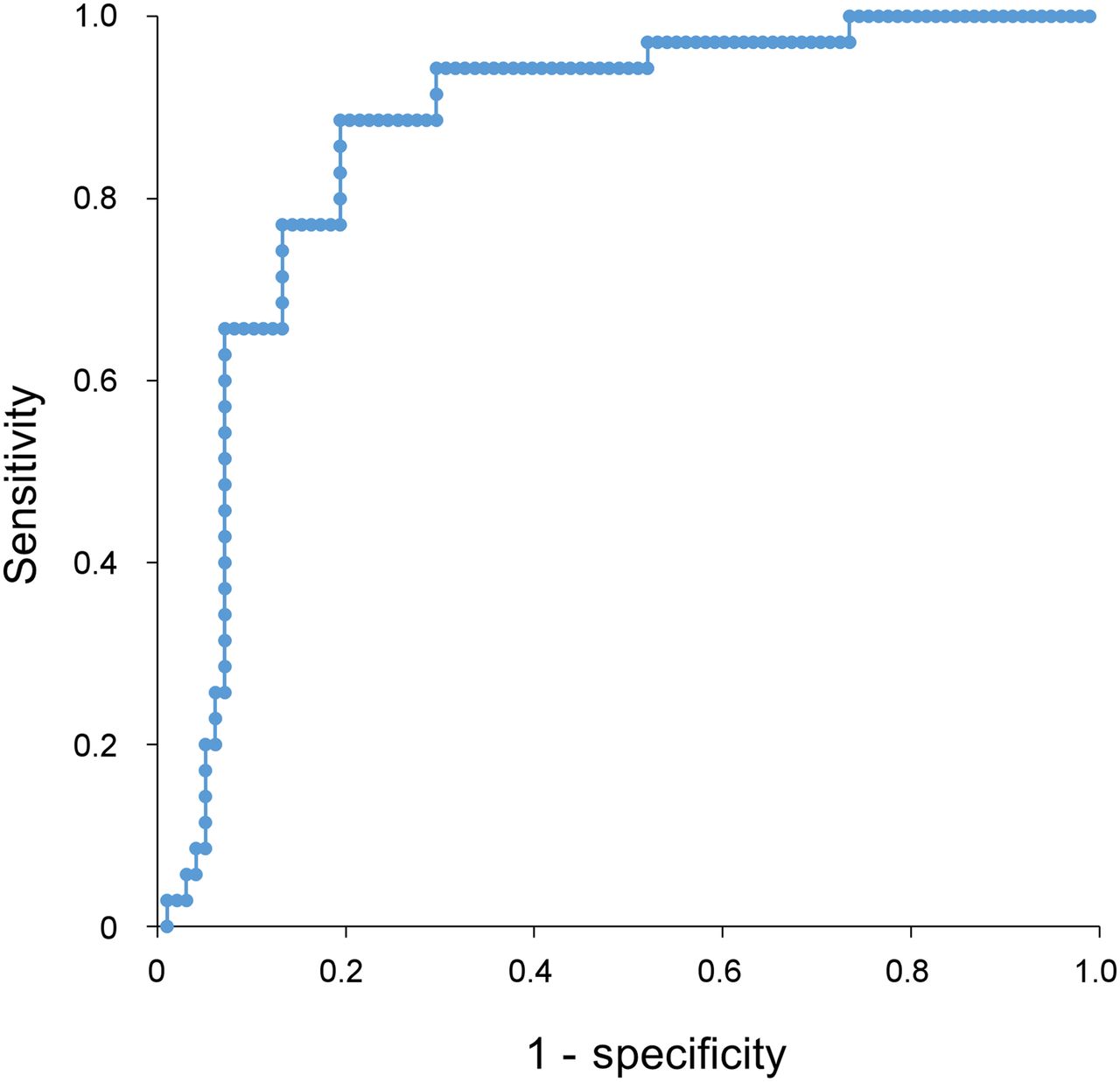
Data are expressed as the average ± SD of continuous variables. Continuous variables from patients with and without events were compared using a Fisher exact probability test or the Mann–Whitney U test as appropriate, and categoric data were analyzed using the χ2 test. To evaluate the clinical importance of the defect score, all patients were divided into 2 groups based on their scores. The cutoff value was determined using area under the curve by a receiver-operating-characteristic analysis based on MACE occurrences. The area under the curve was 0.86, and the cutoff for a high score was 4 (Fig. 2). Forty-six patients fell within the high-score group, and the remaining 87 fell within the low-score group. The proportion of event-free patients was estimated by the Kaplan–Meier method and compared between the high- and low-score groups using the log-rank test. The variables that ranked as the top 4 significantly probable values, as well as age and sex, were included in a multivariate Cox regression model to evaluate factors independently associated with the future occurrence of MACE. A P value of less than 0.05 was considered statistically significant. All statistical analyses were performed using StatMate IV software, version 4.01 (Advanced Technology for Medicine and Science).

Receiver-operating-characteristic analysis used for determining cutoff score based on occurrence of MACE. Cutoff for high score was 4, and area under receiver-operating-characteristic curve was 0.85.
RESULTS
Patient characteristics, including coronary risk factors, New York Heart Association (NYHA) class, etiology of HF, brain natriuretic peptide, EF calculated by echocardiography, and defect score, are presented in Table 1. The mean age of the 133 patients was 73 ± 13 y, and 76 patients (57%) were men. Tachycardia-induced cardiomyopathy was the most common risk factor, at 20% (n = 26). Others consisted of valvular heart disease (n = 23), hypertensive heart disease (n = 20), atrioventricular block (n = 12), sick sinus syndrome (n = 10), dilated cardiomyopathy (n = 6), hypertrophic cardiomyopathy (n = 5), myocarditis (n = 4), pulmonary hypertension (n = 3), infective endocarditis (n = 2), pulmonary thromboembolism (n = 2), and unknown (n = 20). The median scores in the high- and low-score groups were 7.1 ± 4.2 and 1.3 ± 0.8, respectively. Although there were no differences in etiologies, there were significant differences in sex, hypertension, NYHA class, brain natriuretic peptide, and left atrial dimension between the high- and low-score groups.
Characteristics of High- and Low-Score Groups
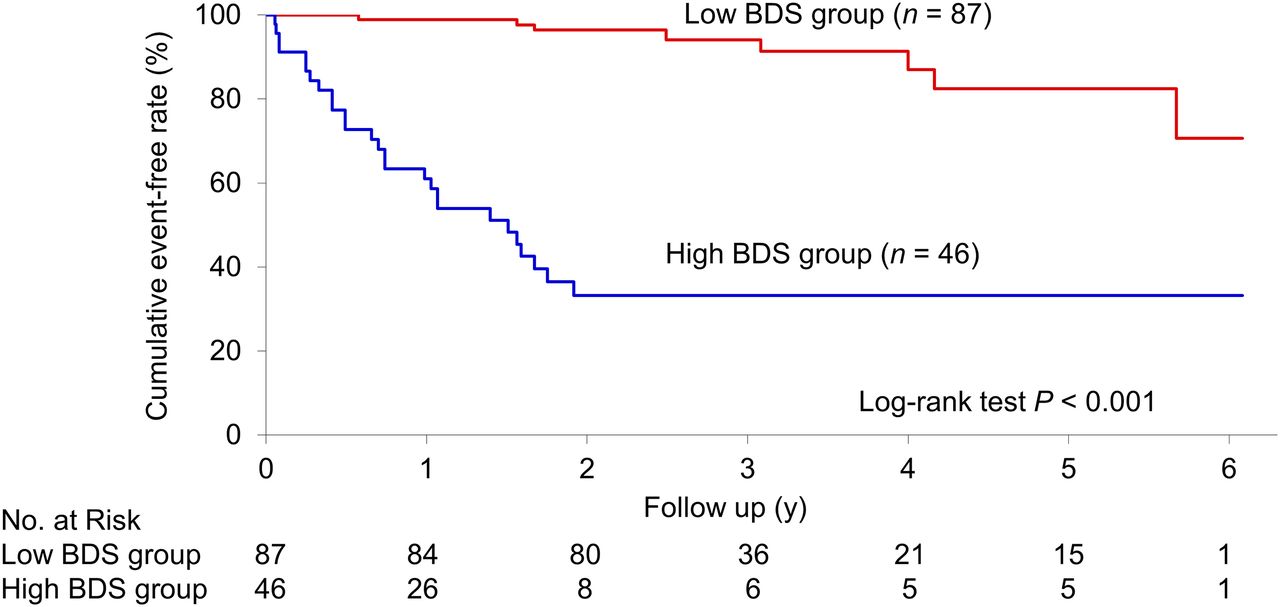
Overall, 35 patients (26%) experienced MACE during follow-up (a median of 908 ± 603 d). Cardiac death occurred in 4 patients (acute myocardial infarction in 2 patients and deterioration of HF in 2 patients), acute myocardial infarction in 5 patients, and severe HF requiring hospitalization in 26 patients. Of the 35 events, 27 fatal events occurred in the high-score group. The proportion of patients who experienced MACE was significantly higher in the high-score group than in the low-score group (59% [27/46] vs. 9% [8/87], P < 0.001) (Fig. 3). Table 2 shows that there were significant differences in NYHA class, brain natriuretic peptide, left atrial dimension, and defect score between participants with and without MACE. In the multivariate analysis, a high score was determined to be the most significant independent prognostic factor for MACE (P < 0.001) (Table 3).
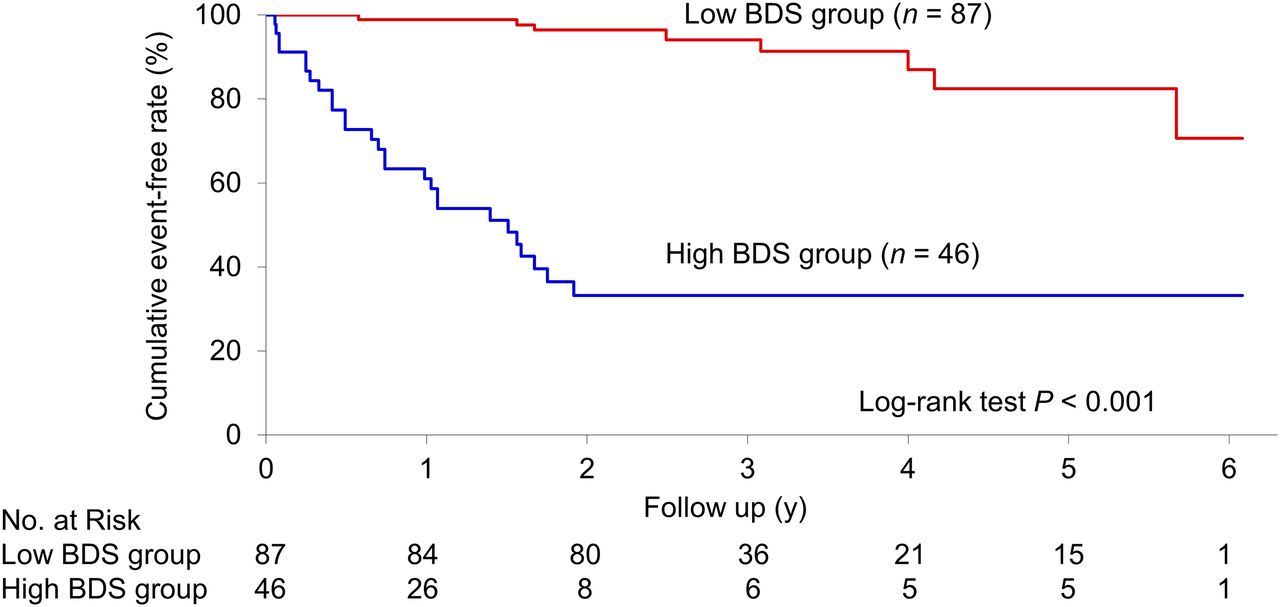
Kaplan–Meier curve in reference to MACE stratified by defect score. y-axis represents cumulative event-free rate; rate in low-score group was significantly higher than that in high-score group (log-rank test, P < 0.001). BDS = 123I-BMIPP defect score.
Characteristics of MACE and No-MACE Groups
Univariate and Multivariate Cox Regression Analysis for Occurrence of MACE
Case Presentations
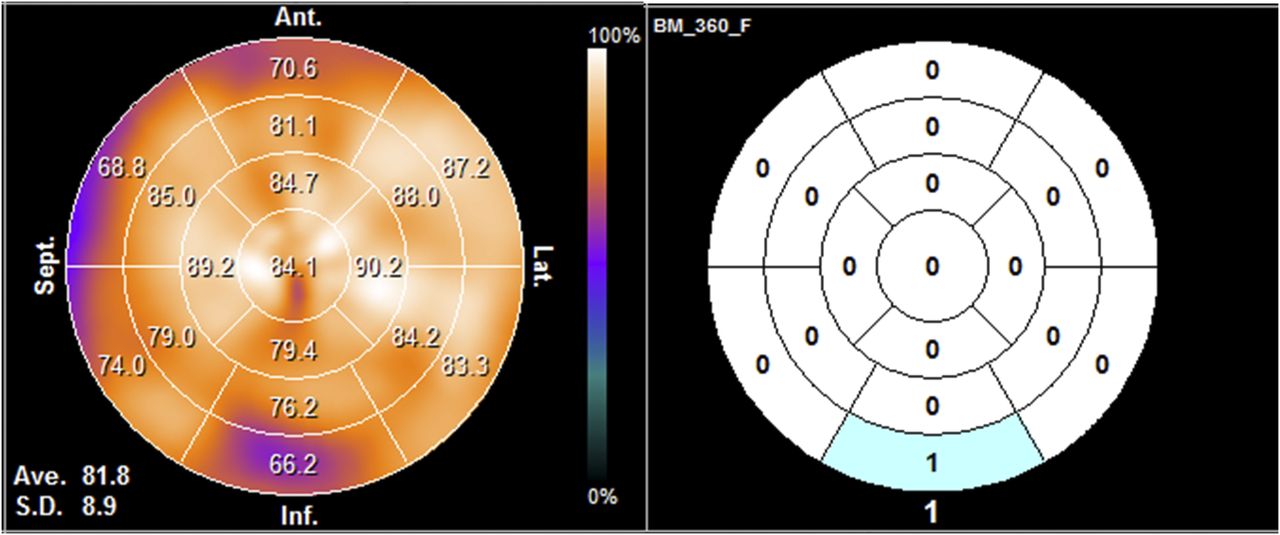
Figure 4 shows a typical patient in the low-score group. This 70-y-old woman had HF due to hypertensive heart disease (clinical scenario 1, NYHA class II, Nohria–Stevenson clinical profile: wet and warm). She had a history of hypertension, diabetes mellitus, and hyperlipidemia. She had a smoking habit. She underwent 123I-BMIPP SPECT, coronary artery angiography, and echocardiography because of suspected coronary heart disease. However, she had no coronary artery disease, and EF was 65%. The automated Heart Risk View-S software gave a defect score of 1. In this case, the patient remained event-free for 39 mo in the follow-up period.
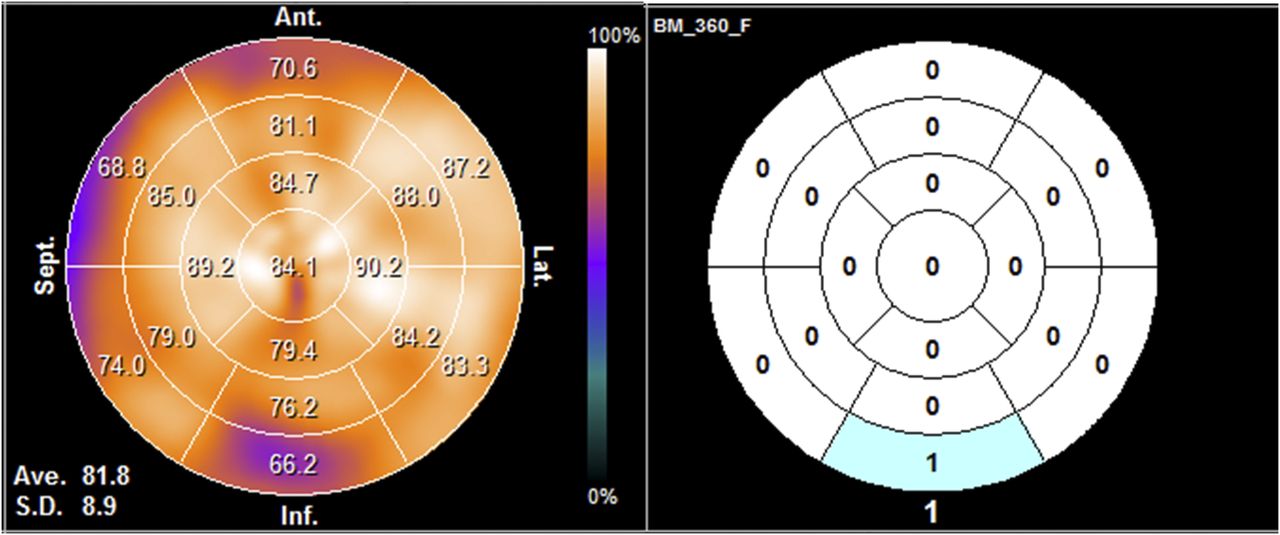
Polar map and heart-risk map of 123I-BMIPP images of patient in low-score group. This patient had HF due to hypertensive heart disease. Score was 1, and patient remained event-free for 39 mo.
Figure 5 shows a typical patient in the high-score group. This 70-y-old woman had HF due to valvular heart disease (clinical scenario 2, NYHA class III, Nohria–Stevenson clinical profile: wet and cold). She had a history of hypertension, atrial fibrillation, and aortic regurgitation. She had a smoking habit. She underwent coronary artery angiography and had no coronary artery disease. She underwent echocardiography, and EF was 55%. The automated Heart Risk View-S software gave a defect score of 12. In this case, the patient was admitted to the hospital because of deterioration of HF 150 d after 123I-BMIPP SPECT.
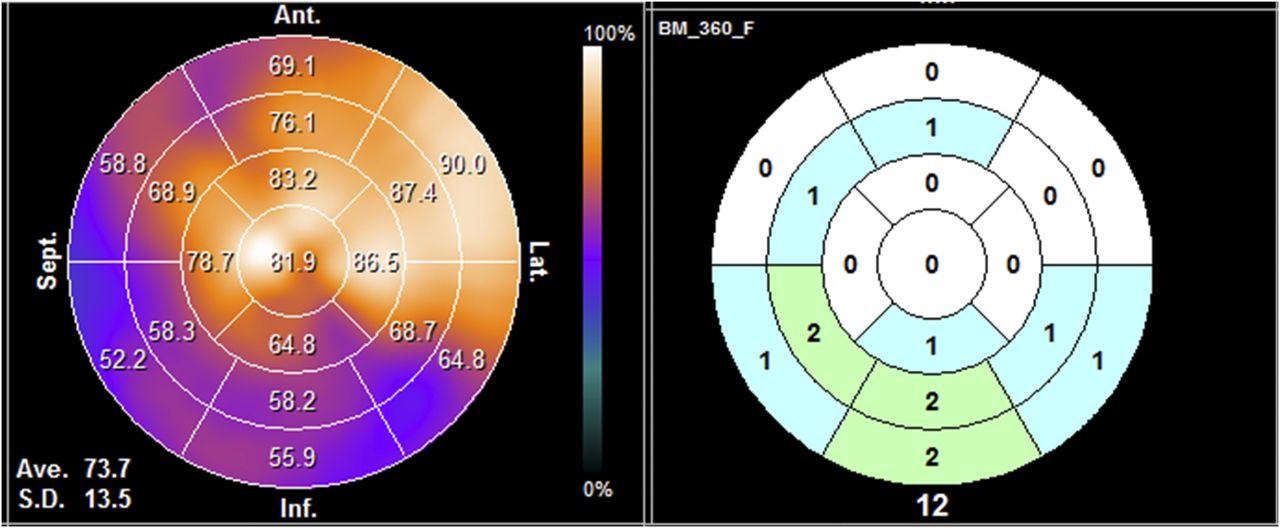
Polar map and heart-risk map of 123I-BMIPP images of patient in high-score group. This patient had HF due to valvular heart disease. Score was 12, and patient was admitted to hospital because of deterioration of HF 150 d after examination.
DISCUSSION
In the present study of patients with nonischemic HF and preserved EF, we demonstrated that 123I-BMIPP SPECT has a prognostic value that is generally used for risk assessment among patients with ischemic heart disease (10,11). We found that a higher defect score by 123I-BMIPP SPECT was associated with an increase in MACE.
Given the high-risk nature of nonischemic HF with preserved EF, prediction of future cardiac risk by noninvasive imaging modalities is essential. Several prior investigations demonstrated the prognostic utility of echocardiography (19) and cardiac MRI among patients who have HF with preserved EF (20). Mascherbauer et al. reported that the value of postcontrast T1 time by cardiac magnetic resonance correlated with extracellular matrix of left ventricular biopsies, and associated with cardiac events (20).
Several underlying mechanisms for our findings could be considered. First, a common pathophysiologic feature of HF with preserved EF is the accumulation of extracellular matrix material and fibrosis within myocardial tissue (21). Excessive extracellular matrix deposition is believed to be a major contributor to the impaired cardiac relaxation and stiffness that are the hallmarks of HF with preserved EF (22). In this regard, the 123I-BMIPP defect score could reflect the extracellular matrix material and fibrosis within myocardial tissue because 123I-BMIPP can accumulate only in the living myocardial cell (23,24). Second, 123I-BMIPP SPECT is believed to reflect intracardiac accumulation of acylated 123I-BMIPP in the lipid pool and the adenosine triphosphate content of the myocardium (23–27). Therefore, the score could reflect impaired use of adenosine triphosphate or a mitochondrial disorder in patients with myocardial degeneration. Mechanical stress to the heart by continued pressure or volume overloading that reduces the myocardial blood supply could be a factor impairing myocardial fatty acid metabolism (28). Therefore, the score could also reflect a myocardial microcirculatory disturbance in patients with a high-pressured left ventricle due to diastolic dysfunction, elastic recoil, and ventricular–arterial coupling associated with HF with preserved EF (29).
In the current study, our data explored whether 123I-BMIPP SPECT can potentially provide quantitative values for the extent and severity of myocardial damage, expressed by the defect score. Our findings suggest that a higher-level score of 4 or more was significantly associated with MACE and was predictive of high risk in patients who have nonischemic HF with preserved EF. In a limited study of the prognostic utility of the defect score in cases with dilated cardiomyopathy, Inoue et al. reported that the score was significantly higher in the cardiac event group (8.7 ± 4.6 vs. 3.5 ± 3.3, P < 0.05) (30). The cutoff value was higher in that study than in ours, but the potential significance of that difference is not so great.
123I-metaiodobenzylguanidine imaging is also known to have a high prognostic value for MACE in patients with HF with preserved EF. Katoh et al. reported that the sensitivity and specificity of the 123I-metaiodobenzylguanidine washout rate for the determination of MACE were 69.0% and 59.2%, respectively (31). In our study, the sensitivity and specificity of the defect score for the determination of MACE were similarly high, at 88.6% and 80.6%, respectively. It would be of great interest to make a head-to-head comparison of 123I-metaiodobenzylguanidine and 123I-BMIPP to identify MACE among patients who have HF with preserved EF; to our knowledge, such a comparison has not yet been done.
Comparison of 123I-BMIPP Defect Score with Echocardiography Findings
The cause of HF with preserved EF is regarded as diastolic HF (9); all participants in this study underwent echocardiography, and we calculated left ventricular end-diastolic volume index, left ventricular wall mass index, and left atrial dimension. Left ventricular relaxation depends on left ventricular end-diastolic volume index (32–34), and diastolic left ventricular dysfunction depends on left ventricular wall mass index and left atrial dimension (35,36). Furthermore, Tsang et al. reported left atrial dimension to be a strong predictor of cardiovascular events, with a higher predictive value than other echocardiographically derived indices (37). However, in the current study there was a significant difference in left atrial dimension between the MACE group and the no-MACE group, and no significant differences in the occurrence of MACE were found on multivariate Cox regression analysis. According to that analysis—and as the defect score is the sole independent factor associated with MACE—we may infer that this score is indeed a strong predictor of MACE. We believe that the 123I-BMIPP defect score could be a reliable prognostic marker for future events in patients who have nonischemic HF with preserved EF, regardless of coronary artery distribution. It is speculated that, in such patients, evaluation of the defect score enables early risk stratification and appropriate management of care.
Study Limitations
This study had several limitations. The number of patients was relatively small. However, our results clearly demonstrated that a higher defect score was significantly associated with MACE. Another limitation of the study was that the timing of 123I-BMIPP SPECT examinations differed among patients according to the severity of each patient’s HF, and patients who had severe HF with respiratory failure were not included in this study because they did not undergo the examination. Therefore, the value of the defect score, and the cutoff between high and low scores, might be underestimated. We did not have access to echocardiography parameters such as E/e′, which might be important in determining diastolic function. However, left ventricular wall mass index and left atrial dimension measured by echocardiography were included in the analysis and did not predict MACE over defect score. A further limitation was that because this study was a retrospective analysis of myocardial SPECT data, we could not separate the analysis by the etiology of the nonischemic HF with preserved EF. Future prospective studies of large populations are needed to confirm the prognostic value of the defect score in patients who have mild to severe nonischemic HF with preserved EF and to compare scores among etiologies. A final limitation of this study was that it did not compare the prognostic value of 123I-BMIPP with that of 99mTc-perfusion imaging. Further studies are needed to determine whether 123I-BMIPP imaging has any advantages over 99mTc-perfusion imaging.
CONCLUSION
This study found that the 123I-BMIPP defect score may have a high prognostic value for MACE in patients who have nonischemic HF with preserved EF. Quantitative assessment of the defect score may have predictive value for identifying future MACE among such patients.
DISCLOSURE
Takanori Ikeda received grant support through his institution from Daiichi Sankyo, Bristol-Myers Squibb, and Boehringer Ingelheim. He also received honoraria for lectures from Bayer Healthcare, Daiichi Sankyo, Bristol-Myers Squibb, Pfizer, Tanabe-Mitsubishi, and Ono Pharmaceutical. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the radiology technologists Tadashi Kokubo, Kazuhiro Tachiki, Nobutomo Ishii, and Takushi Ookubo for assistance with performing myocardial 123I-BMIPP SPECT. We are also grateful to Assistant Professor Roderick J. Turner for his editorial review of the manuscript.
Footnotes
Published online Aug. 3, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 8, 2017.
- Accepted for publication July 6, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.