


Abstract
Pretherapy PET with 86Y-DOTATOC is considered the ideal dosimetry protocol for 90Y-DOTATOC therapy; however, its cost, limited availability, and need for infusion of amino acids to mimic the therapy administration limit its use in the clinical setting. The goal of this study was to develop a dosimetric method for 90Y-DOTATOC using 90Y-DOTATOC PET/CT and bremsstrahlung SPECT/CT and to determine whether dosimetry-based administered activities differ significantly from standard administered activities. Methods: This was a prospective phase 2 trial of 90Y-DOTATOC therapy in patients with somatostatin receptor–positive tumors. 90Y-DOTATOC was given in 3 cycles 6–8 wk apart. In the first cycle of therapy, adults received 4.4 GBq and children received 1.85 GBq/m2; the subsequent administered activities were adjusted according to the dosimetry of the preceding cycle so as not to exceed a total kidney dose of 23 Gy and bone marrow dose of 2 Gy. The radiation dose to the kidneys was determined from serial imaging sessions consisting of time-of-flight 90Y-DOTATOC PET/CT at 5 h after therapy and 90Y-DOTATOC bremsstrahlung SPECT/CT at 6, 24, 48, and 72 h. The PET/CT data were used to measure the absolute concentration of 90Y-DOTATOC and to calibrate the bremsstrahlung SPECT kidney clearance data. The radiation dose to the kidneys was determined by multiplying the time-integrated activity (from the fitted biexponential curve of renal clearance of 90Y-DOTATOC) with the energy emitted per decay, divided by the mass of the kidneys. Results: The radiation dose to the kidneys per cycle of 90Y-DOTATOC therapy was highly variable among patients, ranging from 0.32 to 3.0 mGy/MBq. In 17 (85%) of the 20 adult patients who received the second and the third treatment cycles of 90Y-DOTATOC, the administered activity was modified by at least 20% from the starting administered activity. Conclusion: Renal dosimetry of 90Y-DOTATOC is feasible using 90Y-DOTATOC time-of-flight PET/CT and bremsstrahlung SPECT/CT and has a significant impact on the administered activity in treatment cycles.
- radiobiology/dosimetry
- radionuclide therapy
- 90Y-DOTATOC
- dosimetry
- neuroendocrine
- peptide receptor radiotherapy
Peptide receptor radionuclide therapy (PRRT) of neuroendocrine tumors (NETs) uses radiolabeled octreotide analogs to deliver targeted radiation to somatostatin receptor (primarily sstr-2)–positive tumor tissue. The most commonly used radiopeptides in PRRT of NETs are 90Y-DOTATOC and 177Lu-DOTATATE. 177Lu is both a γ-emitter and a β-emitter, with a maximum energy of 0.5 MeV and a maximum range of 2 mm for its β-particles, whereas 90Y is predominantly a β-emitter, with a maximum energy of 2.3 MeV and a maximum range of 10 mm (1,2).
Renal toxicity represents a major long-term potential adverse effect associated with PRRT, particularly with 90Y-DOTATOC. The radiolabeled peptides used in PRRT are filtered through the glomeruli and reabsorbed through the proximal tubules, a process mediated by the membrane protein megalin (3,4). The parenchymal retention of radiolabeled peptides increases radiation dose to the kidneys and can significantly reduce renal function and even lead to end-stage renal disease (5,6). The radiation dose to the kidneys can be reduced by the coadministration of positively charged amino acids, particularly d-lysine and l-arginine. These amino acids competitively block the renal tubular reabsorption and retention of the radiolabeled peptides, resulting in up to a 50% reduction of renal radiation dose (7–10). Despite the renal protection offered by the amino acid infusion, significant renal toxicity remains a concern with 90Y-DOTATOC, with grade 4 or 5 permanent renal toxicity reported in up to 9% of patients (11). Renal toxicity appears less common with 177Lu-DOTATATE, probably because of the lower-energy β-particle emission of 177Lu, with lower tissue penetration (1). Subacute and reversible grade 3–4 bone marrow toxicity has also been reported in 10%–13% of patients after PRRT, although long-term bone marrow toxicity is rare with typically administered activities (8,11).
PRRT with 90Y-DOTATOC and 177Lu-DOTATATE has been generally administered in fixed doses. These doses are established to provide a reasonable likelihood of tumor effect and a low likelihood of renal and bone marrow toxicity. The renal and bone marrow doses, however, can be highly variable among patients. With individual dosimetry, personalized treatment doses can be established to ensure that the total renal dose does not exceed the 23-Gy limit and the bone marrow dose remains below 2 Gy, thresholds generally accepted for radiation toxicity (12,13). For pretherapy dosimetry assessment of 90Y-DOTATOC, 86Y-DOTATOC PET/CT may be ideal, but the cost and limited availability of 86Y limit its routine use. Pretherapy dosimetry is preferably also done with coinfusion of amino acids to mimic the administration of the therapeutic drug. The amino acid infusion, depending on its composition, can, however, cause significant nausea and vomiting (14).
As an alternative, dosimetry with 90Y-DOTATOC therapy administered with the amino acid infusion was investigated in this study as a means to estimate radiation dose to organs for subsequent cycles of the treatment. Although 90Y is predominantly a β−-emitter, a minor decay branch to 90Zr followed by β−β+-internal pair production allows coincidence imaging with time-of-flight PET/CT scanners (15). Thus, our goal in this study was to develop a dosimetric method for measuring the renal radiation dose in PRRT using 90Y-DOTATOC time-of-flight PET/CT and bremsstrahlung SPECT/CT and to determine whether dosimetry-based administered activities differ significantly from standard administered dosages.
MATERIALS AND METHODS
Study Design
This was a phase 2 PRRT trial of 90Y-DOTATOC in patients with somatostatin receptor–positive tumors. The somatostatin receptor targeting before PRRT is determined using 68Ga DOTATOC PET/CT. 90Y-DOTATOC PRRT consists of 3 cycles of therapy given 6–8 wk apart. All adults received 4.4 GBq of 90Y-DOTATOC for the first cycle; in children, the administered activity for the first cycle was 1.85 GBq/m2. The administered activities for cycles 2 and 3 were determined on the basis of renal doses from previous cycles not to exceed 23 Gy for the total renal dose. The administered activity for the second cycle was then calculated as 0.5 × (23 Gy − renal dose from cycle 1 [Gy])/renal dose per activity (mGy/MBq) × 1,000. The administered activity of 90Y-DOTATOC for the third cycle was then calculated as 1,000 × (23 Gy – summed renal dose from cycles 1 and 2 [Gy])/renal dose per activity from cycle 2 (mGy/MBq). The maximum dose per cycle was limited to 5.6 GBq. The dose escalation was also adjusted to a total blood dose of 2 Gy. No dose escalation was performed for pediatric patients.
Patients
Adults and children with nonresectable or metastatic NETs were prospectively enrolled. There were 6 inclusion criteria. The first was the presence of at least 1 target lesion that was confirmed by cross-sectional imaging and was determined to express somatostatin receptors by 68Ga-DOTATOC. The second and third were a life expectancy of at least 2 mo and an age of 6 mo to 90 y. The fourth was a performance status score of at least 50% as determined by the Karnofsky scale or the Lansky play scale. The fifth was normal organ and bone marrow function as determined by an absolute neutrophil count of at least 1,000/mm3, a platelet count of at least 90,000/mm3, total bilirubin no more than 3 times the upper limit of normal, and aspartate transaminase and alanine transaminase no more than 10 times the institutional upper limit of normal for age. The final inclusion criterion was normal kidney function. For children, normal function was defined as a glomerular filtration rate higher than 80 mL/min/1.73 m2 as determined with a nuclear glomerular filtration rate study. For adults, normal function was defined as a serum creatinine level of no more than 1.2 mg/dL or, if higher, a glomerular filtration rate of at least 80, 70, 60 and 50 mL/min/1.73 m2 for subjects aged, respectively, 40 y or younger, 41–50 y, 51–60 y, and older than 60 y.
The exclusion criteria were concomitant therapy for NETs, except for somatostatin analogs or bisphosphonates (somatostatin therapy was limited to short-acting subcutaneous doses between cycles, with discontinuation 12 h before each dose of 90Y-DOTATOC); pregnancy or breast-feeding; active treatment of another concurrent malignancy; and previous external-beam radiation therapy to both kidneys (scatter doses of <0.5 Gy to a single kidney or radiation to <50% of a single kidney was acceptable).
This research was approved by the University of Iowa Institutional Review Board, and all subjects gave written informed consent. The research was conducted according to the principles of the Declaration of Helsinki and good clinical practice. The trial was listed on clinicaltrials.gov (NCT02441088).
Synthesis of 90Y-DOTATOC
90Y-DOTATOC was produced under a physician-sponsored Investigational New Drug approval using a single-use cassette specific for 90Y-DOTATOC, hermetically enclosed in a sterile acrylic glass–shielded synthesis unit (ModularLab PharmTracer; Eckert and Zeigler). DOTATOC was obtained commercially (ITG Isotope Technologies GmbH) and was manufactured under good-manufacturing-practice standards. 90Y-chloride produced per good-manufacturing-practice standards was also obtained commercially (PerkinElmer). Before synthesis, a freshly made solution of 50 mg of ascorbate buffer (Polatom) in 100 mL of sterile saline was prepared; 84 mL of this solution were passed through the final product-sterilizing filter into a weighed vented product vial as diluent and to prevent product radiolysis. The amount of DOTATOC precursor was scaled to the amount of activity received based on 115 μg of DOTATOC in 1.0 mL of ultrapure water for 7.4 GBq. Under computer control, the received 90Y-YCl3 (∼500 μL) was transferred to the reaction vessel. The 90Y-YCl3 vial was then washed with a solution of 50 mg of ascorbate buffer in 1.5 mL of ultrapure water and transferred to the reaction vessel. The reaction vessel was heated to 95°C for 25 min. The reaction mixture was transferred to and purified by trapping on a previously activated C-18 solid-phase extraction cartridge, followed by a 2-mL saline rinse of the reaction vessel. The product was eluted with 2.5 mL of 47.5% aqueous ethanol followed by 16 mL of saline into the final product vial to give approximately 100 mL of solution. The integrity of the final product-sterilizing filter was confirmed with a pressure test. After thorough mixing, samples were aseptically removed for endotoxin and sterility tests. A further sample was removed for purity testing by high-performance liquid chromatography and pH determination.
Drug Administration
A commercially available amino acid solution (Aminosyn II, 7%; Abbott Laboratories) that contains 0.713 mg of arginine and 0.735 mg of lysine per 100 mL in addition to a multitude of other amino acids was infused with each administration of 90Y-DOTATOC. In total, 1,600 mL of the amino acid solution were infused over 4–5 h depending on patient tolerability, beginning 30 min before infusion of the 90Y-DOTATOC. Because of the emetogenic effect of the amino acid solution, subjects were administered ondansetron (8–16 mg) or fosaprepitant dimeglumine (150 mg) and lorazepam (1 mg) intravenously 30 min before the start of the amino acid infusion. 90Y-DOTATOC was infused over 15 min, beginning 30 min after initiation of the amino acid infusion.
Bone Marrow Dosimetry
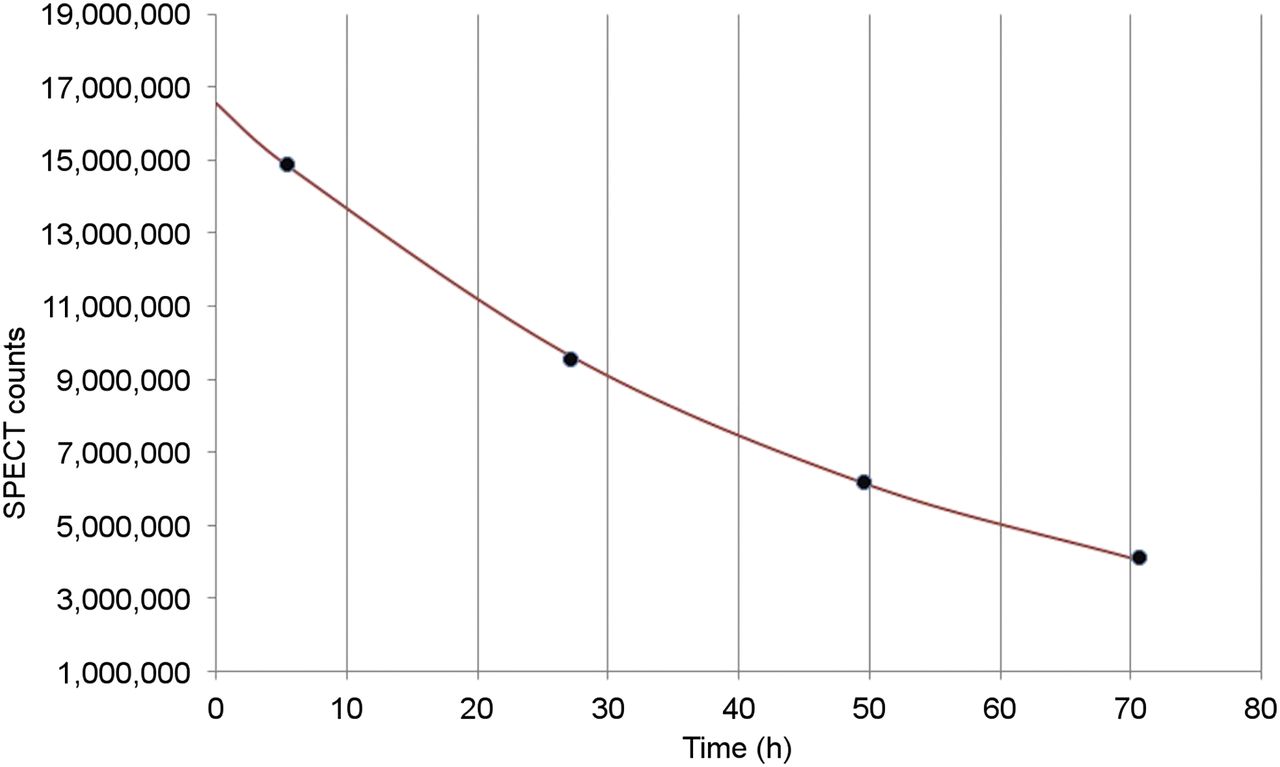
The radiation dose to the blood was measured as a surrogate for bone marrow dose. Blood samples were acquired at 1 h after administration of 90Y-DOTATOC and typically at 5, 24, 48, and 72 h after administration. For each patient, a 37-kBq 90Y standard source was prepared with a volume of 1 mL. After the last blood draw, duplicate 1-mL samples for each time point were made and were counted (5 min per sample) on an automatic multisample NaI(Tl) well counter along with the 90Y standard. Energy windows were set to collect bremsstrahlung radiation over the range of 100–300 keV. The average count rate for each time point was appropriately corrected for decay, and the total integrated activity was determined analytically from exponential curve fits. Specifically, the 1- and 5-h time points were used to determine a single exponential, whereas the 5-, 24-, 48-, and 72-h time points were fit to a biexponential model using the Microsoft Excel Solver Add In software (Fig. 1). The standard was used to convert the count rates into absolute activity. The radiation dose to the blood was determined by multiplying the time-integrated activity by the average 90Y energy emitted per decay per gram (1 mL). Because 90Y is essentially a pure β-emitter, blood was the only source organ contributing to the dose estimate.

Typical biexponential curve of renal clearance of 90Y-DOTATOC, with initial fast elimination followed by slow clearance.
Kidney Dosimetry
The radiation dose to the kidneys was determined from serial image sessions acquired at (nominally) 5, 24, 48, and 72 h after administration of 90Y-DOTATOC. At the completion of the amino acid administration (typically 5 h after administration of 90Y-DOTATOC), a 30-min PET/CT scan of the kidneys was acquired. The study was performed on a Siemens mCT PET/CT scanner using time-of-flight information that was calibrated to yield 90Y activity concentrations. A 6.7-MBq 90Y standard in a 100-mL volume was also imaged. The PET images were reconstructed with an ordered-subsets expectation-maximization iterative algorithm that incorporated time-of-flight information.
Immediately after the completion of the PET/CT scan, the patient was transferred to a SPECT/CT system, where a 15-min 90Y bremsstrahlung scan was acquired of the kidneys. The 100-mL 90Y standard was positioned on the patient in the SPECT field of view but superior to the kidneys. The bremsstrahlung energy window was centered at 150 keV with a window width of 50 keV, and 90 projections over 360° were acquired. A CT scan was acquired for attenuation correction at the completion of the SPECT study. Additional bremsstrahlung SPECT/CT studies were acquired at 24, 48, and 72 h after administration of 90Y-DOTATOC. All SPECT studies were reconstructed using iterative ordered-subsets expectation maximization with attenuation correction.
The volume of the kidneys was determined for each patient from regions of interest drawn on the axial CT slices from the PET/CT study. The kidney collecting system was not included as part of the kidney regions. Clearance of the 90Y-DOTATOC from the kidneys was determined by integrating the kidney counts in regions of interest drawn on each slice of the reconstructed SPECT images at each time point. All 4 of the SPECT studies for a given patient were manually coregistered so that 1 set of regions would suffice for all 4 time points. The kidney time–activity curve was fitted to a biexponential model using the Excel Solver Add In software.
The PET/CT data were used to calibrate the SPECT kidney clearance data. The absolute activity in the kidneys at 5 h was determined by integrating the concentration of 90Y activity in the regions drawn, slice by slice, over the entire kidneys visualized on CT and multiplying by the voxel size. Because the 5-h PET/CT and SPECT/CT studies were acquired at approximately the same time, the PET results were used to determine a 90Y activity calibration factor that was applied to all time points.
The time-integrated activity was determined analytically from the biexponential fit parameters. The absorbed radiation dose to the kidney was determined by multiplying the time-integrated activity by the average 90Y energy emitted per decay, divided by the mass of the kidneys derived from CT-based kidney regions. Because 90Y is essentially a pure β-emitter, kidney was the only source organ contributing to the dose estimate. The kidney biological effective dose (BED) was calculated using the standard linear quadratic formulation:
where  is the dose to the kidney from the ith treatment,
is the dose to the kidney from the ith treatment,  is the corresponding measured effective half-life for the 90Y-DOTATOC in the kidney,
is the corresponding measured effective half-life for the 90Y-DOTATOC in the kidney,  is the sublethal damage repair half-time for kidney tissue, which was assumed to be 2.8 h, and the biologic response parameter (α/β) was assumed to be 2.6 Gy (16).
is the sublethal damage repair half-time for kidney tissue, which was assumed to be 2.8 h, and the biologic response parameter (α/β) was assumed to be 2.6 Gy (16).
Kidney and Bone Marrow Toxicity
Serum creatinine and blood counts were obtained at baseline, before each subsequent cycle of therapy, 3 mo after completion of therapy, 6–9 mo after completion of therapy, and at subsequent clinic follow-up visits. Toxicity was graded according to the Common Terminology Criteria for Adverse Events (version 4.0). Estimates and 95% confidence limits for hematologic and renal profiles were derived using mixed-effects regression models in SAS, version 9.4 (SAS Institute), to account for the longitudinally correlated nature of repeated laboratory assessments and unequal timing between visits.
RESULTS
Patients
Twenty-nine patients with NETs were prospectively enrolled, and 4 were excluded because of screen failure. The remaining 25 (14 male and 11 female patients ranging from 16 to 76 y old [median, 59 y], including 2 children and 2 young adults ranging from 16–28 y old) received at least 1 dose of 90Y-DOTATOC. The primary tumor sites were 14 small-bowel NETs, 5 pancreatic NETs, 1 pulmonary carcinoid, 3 NETs of unknown primary, and 2 paragangliomas. Twenty-two patients received all 3 cycles of 90Y-DOTATOC, and 3 patients received only 1 dose of 90Y-DOTATOC and then discontinued because of worsening of functional status.
Renal and Bone Marrow Dosimetry
The renal clearance of 90Y-DOTATOC could be fitted in every subject to a biexponential curve with an initial fast elimination of 90Y-DOTATOC followed by slow clearance (Fig. 1). The average renal clearance half-time for the initial fast clearance phase was 6.4 h (SD, 11.6 h; range, 1.4–77.0 h), followed by an average clearance half-time of 37.5 h for the subsequent slow clearance phase (SD, 12.5 h; range, 25.1–92.4 h).
The radiation dose to the kidneys per cycle of 90Y-DOTATOC therapy was highly variable, ranging between 0.32 and 3.0 mGy/MBq (mean ± SD, 1.46 ± 0.60 mGy/MBq). The renal doses in the second cycle differed by more than 20% from the first cycle in 10 of 22 patients. Figure 2 provides the distribution of renal doses for the 47 administrations of 90Y-DOTATOC. Table 1 summarizes the total absorbed dose and the BED to the kidneys for each subject. Several patients did not reach the absorbed dose threshold of 23 Gy to the kidneys because the maximum administered activity per cycle was limited to 5.6 GBq per protocol.
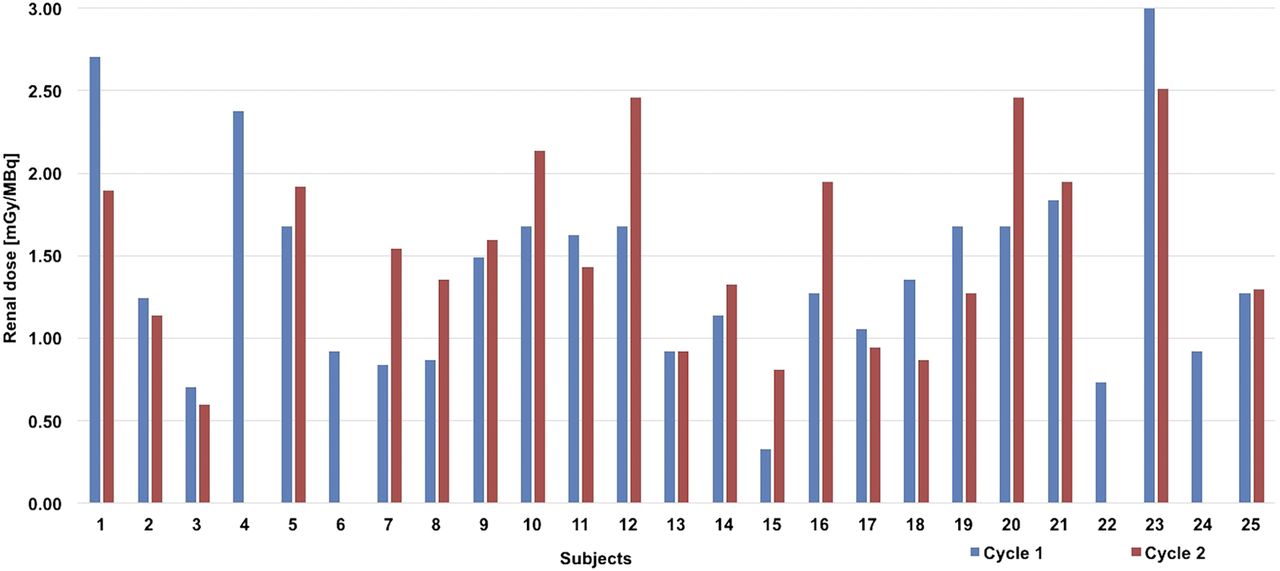
Distribution of renal absorbed doses from 47 administrations of 90Y-DOTATOC.
Total Absorbed Radiation Dose and BED to Kidneys for Each Subject
The bone marrow dose ranged from 0.04 to 0.24 mGy/MBq and averaged 0.09 ± 0.04 mGy/MBq. The bone marrow dose in the second cycle differed by more than 20% from the first cycle in 9 of 22 patients. Figure 3 provides the distribution of bone marrow doses for the 47 administrations of 90Y-DOTATOC.
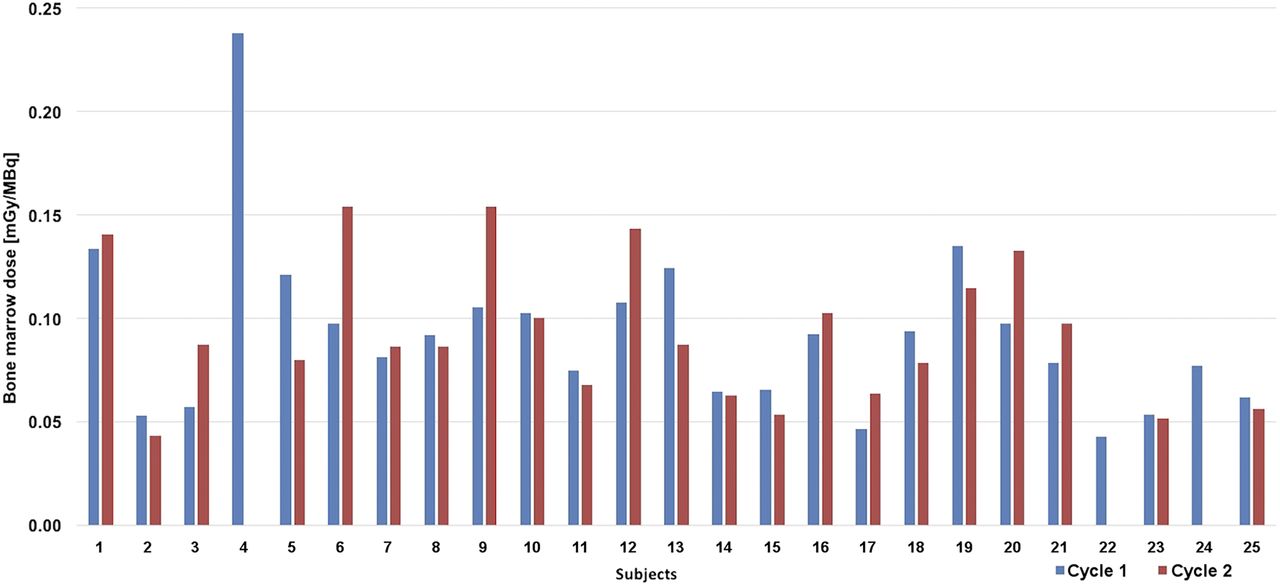
Distribution of bone marrow doses from 47 administrations of 90Y-DOTATOC.
Administered Activity
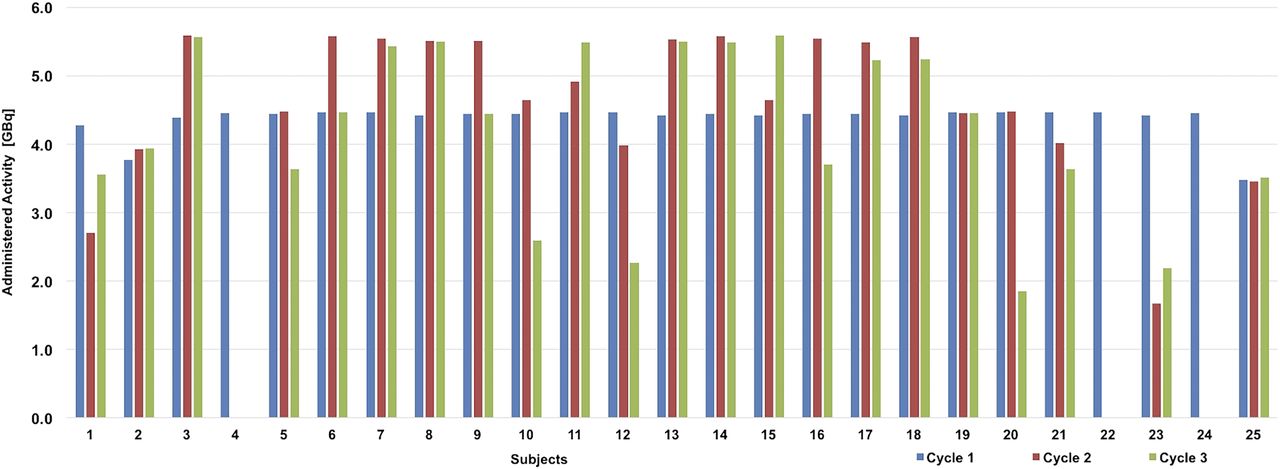
All adult patients were treated with 4.4 ± 0.04 GBq of 90Y-DOTATOC for the first cycle of therapy; 2 pediatric patients were treated with 1.85 GBq/m2. On the basis of the dosimetry of the preceding cycle of 90Y-DOTATOC, the administered activity was adjusted to 1.7–5.6 GBq for the second cycle and 1.9–5.6 GBq for the third cycle (per protocol, 5.6 GBq was the maximum dose per cycle). For 17 of the 20 adults who received the second and third doses of 90Y-DOTATOC, the dose was modified by at least 20% from the starting dose. No dose escalation was performed for pediatric patients, per the protocol. In 1 subject (patient 15), the full dose escalation for the second cycle could not be performed because of the unavailability of the radiopharmaceutical. The dose-limiting organ was the kidneys in all patients, although in 2 subjects (patients 6 and 9) the planned dose escalation for the third cycle based on favorable kidney dosimetry was not performed because the total bone marrow dose exceeded 2 Gy. The distribution of administered activity per cycle for each subject is in Figure 4.

Distribution of administered activity per cycle for each subject.
Renal and Bone Marrow Toxicity
The median follow-up from the first cycle of therapy in 22 patients who received all 3 doses was 15 mo (range, 5–26 mo). The change in serum creatinine, platelet, and neutrophil count over 3 treatment cycles and follow-up is summarized in Supplemental Figure 1 (supplemental materials are available at http://jnm.snmjournals.org). Only 1 subject demonstrated an increase in serum creatinine level from grade 1 to grade 2; no grade 3 or 4 renal toxicity was observed. There was no grade 3 or 4 neutropenia or thrombocytopenia.
DISCUSSION
The use of personalized dosimetry is critical to administer effective doses of therapeutic radiopharmaceuticals and minimize the risk of severe toxicity. Personalized dosimetry procedures should remain cost-effective and feasible in a busy clinical setting. Our proposed method of combining time-of-flight PET/CT and bremsstrahlung SPECT/CT for posttherapy dosimetry of 90Y-DOTATOC is feasible and provides critical renal dosimetry data that significantly impact the administered activity of subsequent cycles. The average renal dose in our study was highly variable among subjects and treatment cycles, ranging from 0.32 to 3.0 mGy/MBq. A significant dose adjustment was therefore required in 85% of patients, resulting in a wide range of administered activities per cycle, between 1.7 and 5.6 Gy. Interestingly, the renal radiation doses were also variable among cycles, resulting in a significant change in administered activity among cycles in 45% of patients.
The average renal dose from 90Y-DOTATOC administered with the amino acid solution was 1.46 ± 0.60 mGy/MBq, using our hybrid approach of 90Y-DOTATOC time-of-flight PET and bremsstrahlung SPECT. Using 86Y-DOTATOC PET with amino acid infusion, Helisch et al. reported similar renal dosimetry at an average renal dose of 1.71 ± 0.89 mGy/MBq, ranging from 0.6 to 2.8 mGy/MBq (17). Jamar et al. also reported highly variable renal doses for 90Y-DOTATOC using 86Y-DOTATOC PET, between 1.2 and 5.1 mGy/MBq, with significantly lower renal radiation doses in patients who received amino acids, particularly if amino acid infusion was prolonged over 10 h (18). The longer amino acid infusion may enhance renal protection over the slow component of renal clearance of 90Y-DOTATOC (Fig. 1).
The bone marrow dose of 90Y-DOTATOC obtained from blood dosimetry was also highly variable among patients, ranging from 0.04 to 0.24 mGy/MBq and averaging 0.09 ± 0.04 mGy/MBq. Blood dose is considered a reliable surrogate for bone marrow dose because of the similar concentration of radiolabeled octreotide analogs in the blood and bone marrow and the lack of significant binding to bone marrow (19). Image-based bone marrow dosimetry may be prone to inaccuracies using our methodology, because identification of bone marrow regions may be challenging on 90Y-DOTATOC bremsstrahlung. Our bone marrow radiation dose data are similar to data reported by Helisch et al. using 86Y-DOTATOC and assuming a marrow-to-blood activity ratio of 1.0 (17). Förster et al. reported significantly lower bone marrow doses with 86Y-DOTATOC as a surrogate for 90Y-DOTATOC; however, the investigators assumed the bone marrow concentration of 90Y-DOTATOC to be only 25% of the plasma concentration (20). Even with a conservative approach assuming identical concentrations in blood and bone marrow, bone marrow is generally not the primary dose-limiting organ with 90Y-DOTATOC. In our study population, the administered activity was only slightly reduced in 2 cycles so as not to exceed the 2-Gy radiation threshold to the bone marrow.
The 23-Gy threshold that we used for absorbed radiation dose to the kidney comes from established toxicity data from external radiation therapy (21). The dose rate for PRRT is, however, significantly lower than that for external-beam radiation and further decreases over time because of decay of the radiopharmaceutical (13). The lower dose rate for PRRT and the fractionation of treatment allows for DNA repair, potentially reducing tissue damage and increasing the normal-tissue threshold. A BED that adjusts the absorbed dose for relative effectiveness may be a better predictor of radiation toxicity (12). Using the linear quadratic model revised for radionuclide therapy (22), Bodei et al. found a BED of 40 Gy to be the threshold for renal toxicity with PRRT in patients without risk factors; the threshold dropped to 28 Gy in patients with risk factors (23). In our population, the median BED was 22 Gy; the BED was above 28 Gy in 7 patients, and no patient received a kidney BED greater than 30 Gy. There was no grade 3 or 4 renal toxicity in our population after a median follow-up of 15 mo. Longer-term follow-up is, however, required to confirm the safety of the proposed dosimetry-based therapy, because renal toxicity may not become apparent until as late as 5 y after treatment (11,23). Furthermore, radiation dose to the kidneys is not the only determinant of renal toxicity after PRRT. Bodei et al. have demonstrated in a large cohort of 807 patients that a history of hypertension, other nephrotoxic risks, and hemoglobin toxicity during PRRT were associated with an increased risk of renal toxicity (24).
Our study had some limitations. It was not designed to evaluate the accuracy of the proposed dosimetric approach against the previously proposed standard with 86Y-DOTATOC; however, our dosimetry data are similar to the data reported in the literature for 86Y-DOTATOC. Statements about potential improvements in outcomes resulting from the use of the dosimetric approach over a fixed dose administration cannot be proven given the lack of a control group and the relatively small number of subjects in our study. However, the need for significant adjustment of the administered activity in most of our subjects suggests that, without dosimetry, patients are at a significant risk of being overtreated or undertreated. A significant impact of dosimetry on administered activity was also reported for 177Lu-DOTATATE, which in most patients allowed the administration of more than 4 treatment cycles of fixed doses with favorable dosimetry, although in 20% of patients the number of cycles had to be reduced because of a high renal dose (25,26).
CONCLUSION
Renal dosimetry of 90Y-DOTATOC is feasible using a combination of 90Y-DOTATOC time-of-flight PET/CT and bremsstrahlung SPECT/CT and can have a significant impact on the administered activity in subsequent treatment cycles.
DISCLOSURE
This work was supported by the National Cancer Institute, RO1 CA-167632 and P50 CA174521. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Mar. 9, 2018.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication September 27, 2017.
- Accepted for publication February 27, 2018.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Monte Carlo Simulations Corroborate PET-Measured Discrepancies in Activity Assessments of Commercial 90Y Vials
- Reimbursement Approaches for Radiopharmaceutical Dosimetry: Current Status and Future Opportunities
- Addition of 131I-MIBG to PRRT (90Y-DOTATOC) for Personalized Treatment of Selected Patients with Neuroendocrine Tumors
- Feasibility of Single-Time-Point Dosimetry for Radiopharmaceutical Therapies