


Abstract
To determine whether the current 18F-FDG PET response criterion for skeletal involvement in Hodgkin lymphoma (HL) is suitable, we performed a systematic evaluation of the different types of skeletal involvement and their response on PET after 2 cycles of chemotherapy (PET-2). A secondary objective was to observe the influence of the initial uptake intensity (measured as qPET) and initial metabolic tumor volume (MTV) of skeletal lesions on the PET-2 response. Methods: The initial PET scans of 1,068 pediatric HL patients from the EuroNet-PHL-C1 trial were evaluated for skeletal involvement by central review. Three types of skeletal lesions were distinguished: PET-only lesions (those detected on PET only), bone marrow (BM) lesions (as confirmed by MRI or BM biopsy), and bone lesions. qPET and MTV were calculated for each skeletal lesion. All PET-2 scans were assessed for residual tumor activity. The rates of complete metabolic response for skeletal and nodal involvement on PET-2 were compared. Results: Of the 1,068 patients, 139 (13%) showed skeletal involvement (44 PET-only, 32 BM, and 63 bone). Of the 139 patients with skeletal involvement, 101 (73%) became PET-2–negative in the skeleton and 94 (68%) became PET-2–negative in the lymph nodes. The highest number of PET-2–negative scans in the skeleton was 42 (95%) in the 44 PET-only patients, followed by 22 skeletal lesions (69%) in the 32 BM patients and 37 (59%) in the 63 bone patients. Lesions that became PET-2–negative showed a lower initial median qPET (2.74) and MTV (2 cm3) than lesions that remained PET-2–positive (3.84 and 7 cm3, respectively). Conclusion: In this study with pediatric HL patients, the complete response rate for skeletal involvement on PET-2 was similar to that for nodal involvement. Bone flare seemed to be irrelevant. Overall, the current skeletal PET response criterion—comparison with the local skeletal background—is well suited. The initial qPET and MTV of skeletal lesions were predictive of the PET-2 result. Higher values for both parameters were associated with a worse PET-2 response.
Hodgkin lymphoma (HL) in childhood is a well-curable malignant disease, with long-term survival rates of more than 90% (1,2). The treatment concept consists of intensive chemotherapy and subsequent radiotherapy. However, the development of late sequelae after therapy, such as secondary solid tumors and cardiac diseases, is a major issue. The most important risk factor for the emergence of these sequelae is radiotherapy (3,4). Current clinical trials aim to avoid late effects while maintaining the excellent survival rates by using tailoring individual therapy according to early response (5–7).
The EuroNet-PHL-C1 (C1) study, which began in 2007, was one of the first large international trials for first-line treatment of children with classic HL (8,9). The pioneering approach of the study was to omit radiotherapy completely in patients with a negative result on early interim 18F-FDG PET.
Consensus criteria for PET response evaluation in lymphoma were defined for the first time in 2007 by the International Harmonization Project (10). These criteria were adopted for the C1 trial. Skeletal lesions (i.e., bone marrow [BM] and bone lesions) with a residual uptake higher than the surrounding background were considered PET-positive. The current standard is the Lugano classification, using the Deauville scale for nodal response assessment (11–13). However, the PET response of skeletal lesions is still assessed by comparison with the local background (14,15). Skeletal response assessment might be influenced by the bone flare phenomenon (16,17), which could affect response-adapted treatment decisions by causing-false positive results (18). HL is predominantly a lymph node disease; skeletal involvement is rare (19–22). Therefore, PET response assessment criteria for skeletal lesions have yet to be sufficiently evaluated.
The primary objective of this study was to systematically evaluate the different types of skeletal involvement and their interim PET response in pediatric HL patients. We aimed to answer the question of whether the current skeletal PET response criterion (comparison with the local background) is suitable. A secondary objective was to observe the influence of the initial uptake intensity (measured as qPET) and initial metabolic tumor volume (MTV) of skeletal lesions on the interim PET response.
MATERIALS AND METHODS
Patients
Between February 2007 and October 2011, 1,068 children and adolescents (<18 y old) with classic HL were consecutively enrolled into the C1 trial (23) after they or their guardians had given written informed consent. The trial was approved by the respective ethic committees and regulatory authorities. Before patient accrual began, the trial was registered at clinicaltrials.gov (NCT00433459). All original imaging data for staging and early response assessment were centrally reviewed by the multidisciplinary review team at the University of Halle and the University of Leipzig (24). The institutional review board approved the retrospective imaging data analysis and waived the requirement for additional informed consent.
Treatment Regime
Chemotherapy
All patients were treated with 2 induction cycles of OEPA (vincristine, etoposide, prednisone, and doxorubicin). Thereafter, depending on the treatment group and study arm, the patients received 2 cycles (intermediate-stage disease) or 4 cycles (advanced-stage disease) of COPP (cyclophosphamide, vincristine, prednisone, and procarbazine) or COPDAC (cyclophosphamide, vincristine, prednisone, and dacarbazine) or no further chemotherapy (early-stage disease).
Radiotherapy
No radiotherapy was performed on patients with a negative interim PET result (after 2 cycles of chemotherapy [PET-2]). After the end of chemotherapy, PET-2–positive patients received radiotherapy to all initially involved lymph node regions, extralymphatic organs, and bone lesions. BM lesions were not irradiated. All patients with a bad morphologic response of the lymphatic sites (no change or progression) underwent radiotherapy.
Initial Staging
Initial staging included a PET scan (PET-0) from skull base to upper thigh, a CT scan of the chest, and a CT or MRI scan of the neck, abdomen, and pelvis. Unilateral BM trephine biopsy of the iliac crest was recommended for all patients with an Ann Arbor stage of IIB or higher. Bone scintigraphy was done if skeletal involvement was suspected. Patients were assigned to 1 of the 3 treatment groups according to their staging result.
Early Response Assessment
After the second OEPA cycle, all patients underwent early response assessment by repeating the initial imaging. The PET-2 scan was evaluated visually in direct comparison with the PET-0 scan.
Skeletal lesions were PET-2–positive if their residual uptake was higher than the local skeletal background.
Within the C1 study, nodal involvement on PET-2 was assessed using the International Harmonization Project criteria. Lymph nodes were PET-2–positive if they showed residual uptake higher than the mediastinal blood pool (for lesions ≥ 2.0 cm) or the local background (for lesions < 2.0 cm). Retrospectively, all PET-2 scans were also evaluated according to the Lugano classification, which has represented the standard since 2014. PET-2–positive nodal lesions had to have a Deauville score of 4 or 5 (higher than liver uptake).
Types of Skeletal Involvement (BM Lesions, Bone Lesions, PET-Only Lesions)
Skeletal involvement in HL shows a focal or multifocal pattern (25,26). Diffuse enhanced skeletal uptake on PET is likely to represent paraneoplastic activation or inflammatory changes and was not considered skeletal HL involvement (27).
Skeletal involvement is the generic term for BM involvement and bone involvement. BM lesions are defined as tumor infiltration of the BM without infiltration of the bone matrix. Bone lesions are defined as tumor infiltration of the bone matrix. The distinction between BM and bone lesions was necessary because bone lesions were included in the radiation field but BM lesions were not. Patients with BM or bone lesions were classified as having Ann Arbor stage IV disease and assigned to the advanced-stage treatment group.
Different diagnostic modalities were used to identify and discriminate BM lesions from bone lesions (Fig. 1). PET shows focally increased glucose metabolism as a sign of skeletal tumor involvement, but distinction between BM and bone lesions is not possible on PET. BM lesions are visible on MRI (BM edema or contrast enhancement) and locally detectable by trephine biopsy. Bone lesions are detectable by CT (osteolytic or osteosclerotic lesions) and bone scintigraphy (increased osteoblastic activity). Neither method, however, is appropriate for detection of BM involvement.

Three types of skeletal involvement in 3 children with HL on transverse PET, MRI, and CT images. (A–C) First patient (PET-only lesion) had increased uptake in thoracic vertebra on PET (arrow, A) but no findings on MRI (B) or CT (C). (D–F) Second patient (BM lesion) had increased uptake on PET (arrow, D) and increased contrast enhancement on MRI (arrow, E) in right femur but no findings on CT (F). (G–I) Third patient (bone lesion) had increased uptake on PET (arrow, G), increased contrast enhancement on MRI (arrow, H), and osteolytic lesions on CT (arrow, I) in right iliac crest.
BM lesions were defined as skeletal lesions detected on PET and confirmed by MRI or BM biopsy but without positive findings on CT or bone scintigraphy. Bone lesions were defined as skeletal lesions detected on PET and confirmed by CT or bone scintigraphy.
In 2005, when the C1 trial was designed, it was unclear how frequently PET-positive skeletal findings would occur. To avoid upstaging of patients compared with previous trials performed without PET, skeletal lesions detected on PET without confirmation by MRI, biopsy, CT, or bone scintigraphy were not considered to be BM lesions or bone lesions in the C1 trial. These PET-only lesions were prospectively documented for systematic evaluation.
Quantification of Skeletal Lesions
Each skeletal lesion was assessed quantitatively using the semiautomatic software TumorFinder (Hermes Medical Solutions).
The qPET in PET-0 and PET-2 was characterized as described previously (28). Briefly, qPET represents the quotient of the SUVmean of the 4 hottest connected voxels inside the tumor and the SUVmean of the liver. qPET is a patient-based normalized tumor SUV and is used instead of SUVmax to avoid inequalities in SUV measurement after multicentric data acquisition.
The MTV of each skeletal lesion was estimated using a 3-dimensional growing algorithm. The algorithm started at the voxel with the highest SUV inside the skeletal lesion and stopped at voxels with an SUV below 2.5. In special situations, a gradual manual adjustment of the MTV measurement was necessary for optimal visual fitting.
Follow-up
For follow-up, the C1 study protocol stipulated clinical examinations 4–8 times in the first to third years and 2 times in the fourth and fifth years, MRI of the involved regions 2 to 4 times in the first year and 1 or 2 times in the second to fifth years, CT of the thorax (in cases of lung involvement) 2 times in the first year and 1 time in the second year, and abdominal sonography 4 times in the first and second years and 2 times in the third to fifth years. PET was done only if relapse was confirmed. The median follow-up of our patients was 55 mo. All data were prospectively collected in a validated clinical database.
Statistical Analysis
Statistical calculations were performed with SPSS, version 20 (IBM), and R (R Core Team). The McNemar test was used to compare skeletal involvement to nodal involvement on PET-2. A 2-sample test for equality of proportions with continuity correction was used to compare patient characteristics. A generalized logistic mixed model was applied to model the PET-2–positive skeletal lesions as a function of MTV and qPET on PET-0.
RESULTS
Skeletal Involvement on PET-0
Of the 1,068 pediatric HL patients treated in the C1 trial, 139 (13%) showed skeletal lesions on PET-0. Compared with patients without skeletal involvement, patients with skeletal involvement had a higher frequency of being male, having B-symptoms, and having further extranodal involvement (Table 1).
Characteristics of the 1,068 Pediatric Patients with HL
Of the 139 patients with skeletal lesions, 44 (32%) had PET-only lesions, with no BM or bone involvement in the C1 trial. Of the 44 PET-only patients, 31 were classified as having advanced-stage disease, 5 as having intermediate-stage disease, and 8 as having early-stage disease, according to their extraskeletal staging result. Of the 139 patients with skeletal lesions, 32 (23%) showed BM lesions confirmed by MRI (26 patients) or BM biopsy (6 patients) and 63 (45%) showed bone lesions confirmed by bone scintigraphy (43 patients), CT (8 patients), or both (12 patients). All patients with BM and bone lesions were assigned to the advanced-stage group.
Overall, 432 skeletal lesions were detected (120 PET-only lesions, 171 BM lesions, and 141 bone lesions).
Response of Skeletal Involvement on PET-2
Of the 139 patients with skeletal lesions, 101 (73%) became PET-2–negative in the whole skeleton (42/44 PET-only patients [95%], 22/32 BM patients [69%], and 37/63 bone patients [59%]) (Fig. 2). Regarding lesion level, 343 (79%) of the 432 skeletal lesions presented a PET-2–negative result (112/120 PET-only lesions (93%), 137/171 BM lesions (80%), and 94/141 bone lesions (67%)).
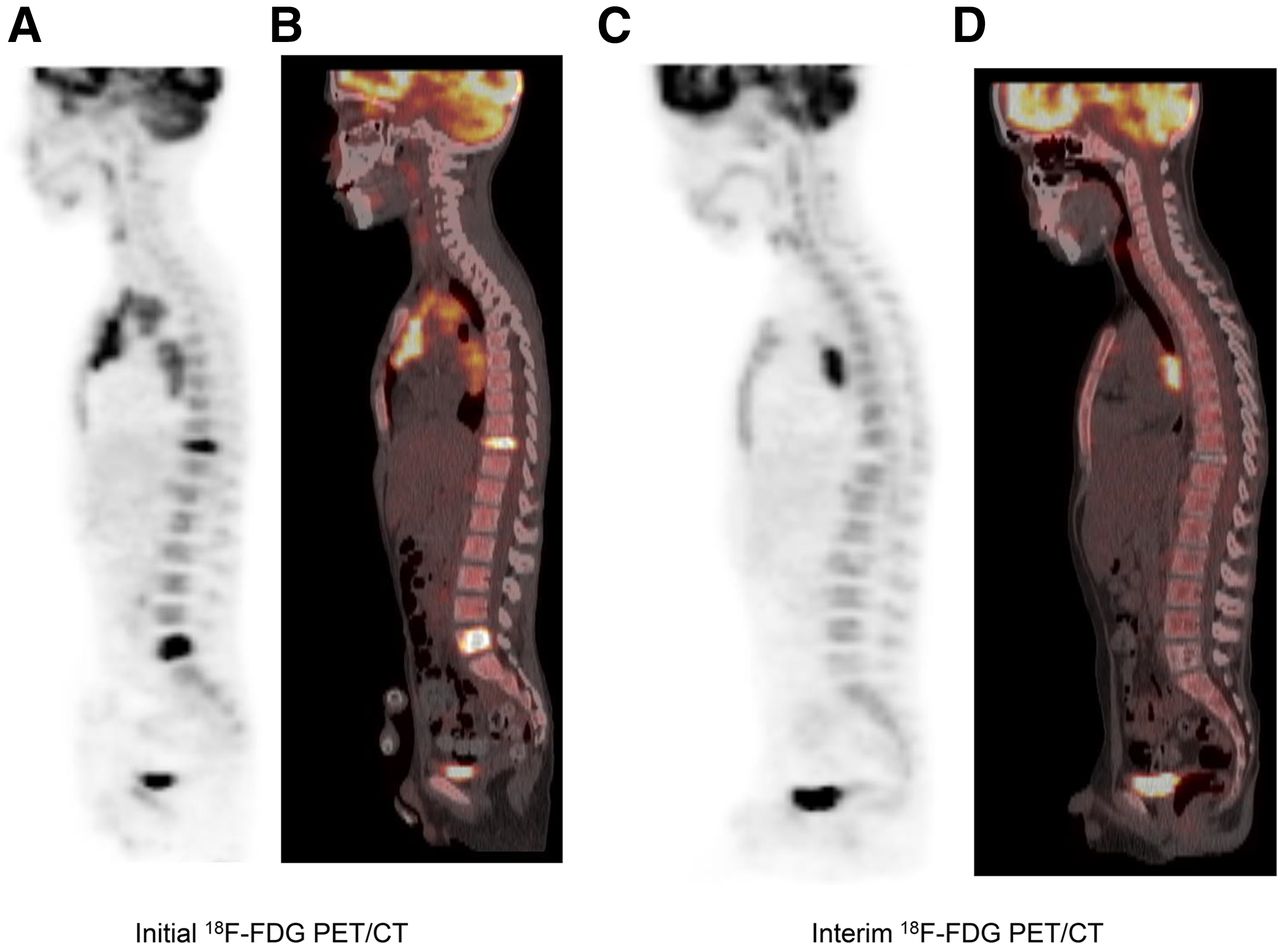
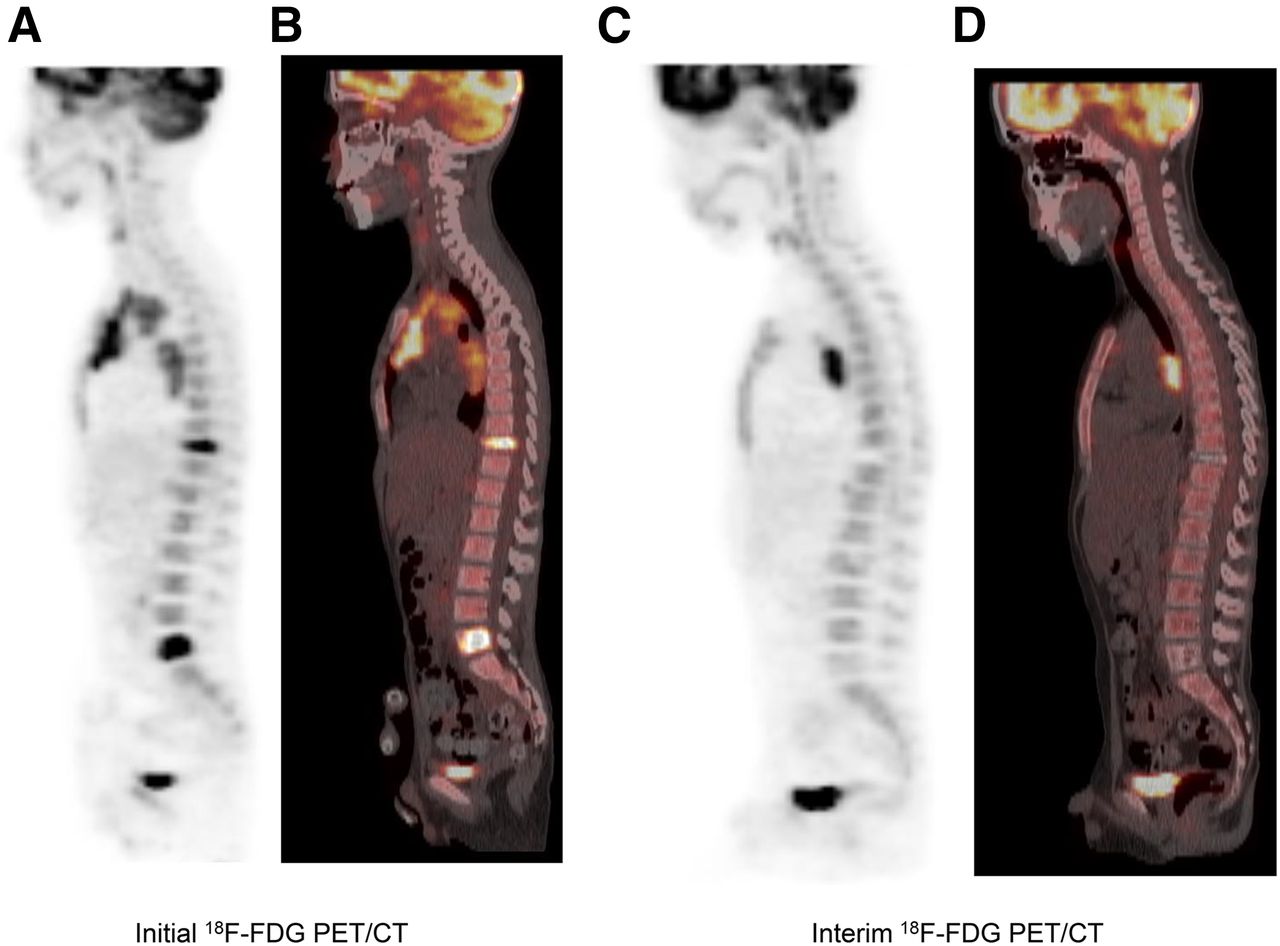
Response of skeletal and nodal involvement in pediatric HL patient on sagittal PET-0 (A) and PET/CT (B) images and on sagittal PET-2 (C) and PET/CT (D) images. Initial skeletal involvement was seen in thoracic vertebra 10 and lumbar vertebra 5, and initial nodal involvement was present in mediastinum. Both skeletal lesions became negative on PET-2, whereas mediastinal nodal lesions remained partially PET-2–positive.
Response of Nodal Involvement on PET-2
All 139 patients with skeletal involvement had nodal involvement as well. According to the International Harmonization Project criteria, 54 (39%) of the 139 patients became PET-2–negative for nodal involvement. Using the Lugano classification, 94 (68%) of the 139 patients had a PET-2–negative (Deauville score ≤ 3) nodal result.
Treatment Outcome
Three (2%) of the 139 patients with skeletal involvement showed progressive nodal disease before the end of treatment, with one of them showing new skeletal lesions. Within a median follow-up of 55 mo, 13 (10%) of the remaining 136 patients showed nodal relapse, with 2 of them also showing new or recurrent skeletal lesions (Table 2). Remarkably, 3 (38%) of the 8 PET-only patients treated in the early-stage group experienced disease relapse.
Treatment and Outcome of the 139 Patients with Skeletal Involvement
Quantitative Assessment
Of the 432 skeletal lesions, 426 were eligible for quantitative assessment (for 6 lesions, quantification was unfeasible). Of these 426 lesions, a median qPET of 2.87 and a median MTV of 3 cm3 were found on PET-0 (Table 3). PET-only lesions showed the lowest qPET and MTV, BM lesions were intermediate, and bone lesions were highest.
qPET and MTV of Skeletal Lesions
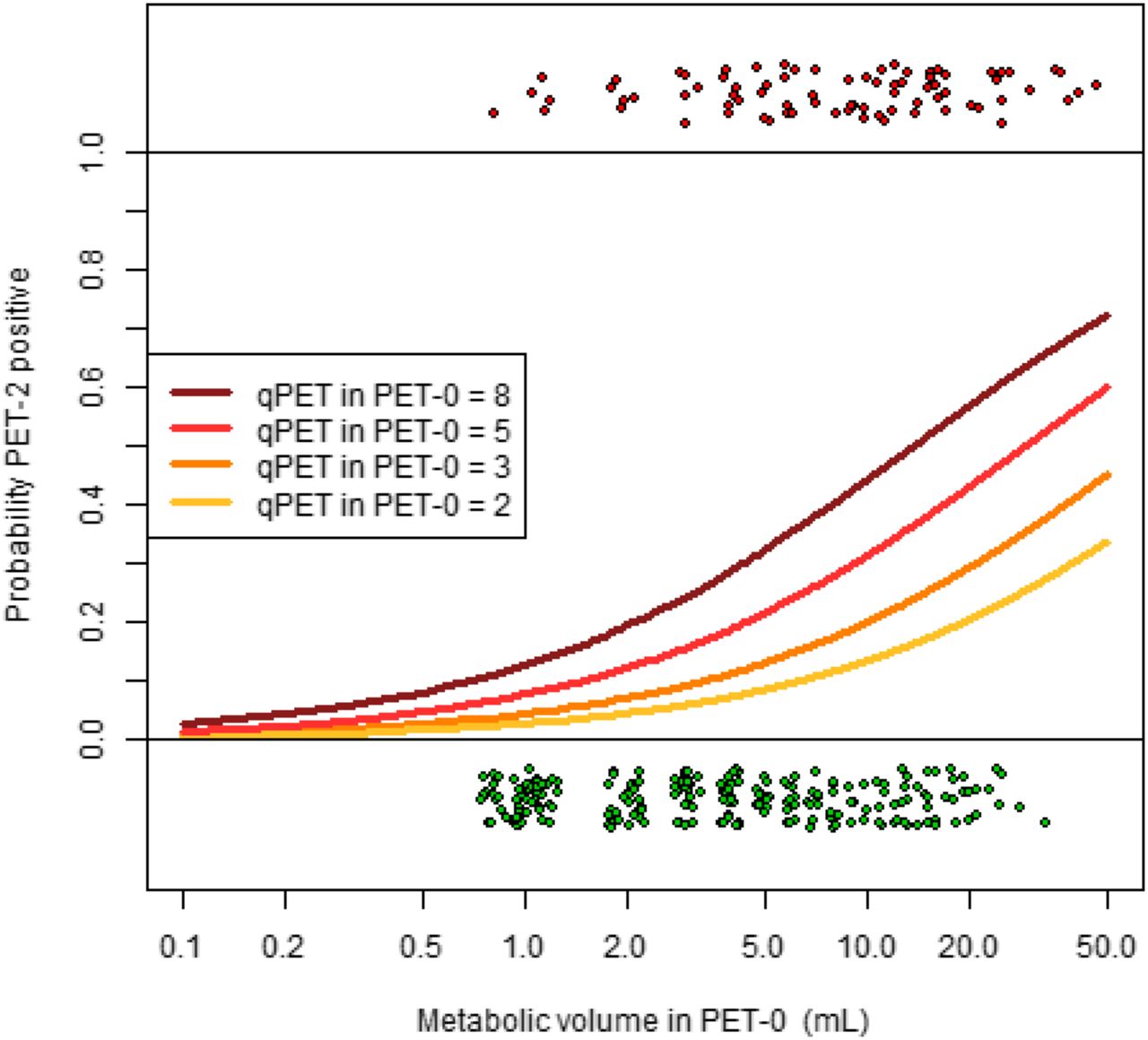
Skeletal lesions that became PET-2–negative had a lower median qPET (2.74) and MTV (2 cm3) than lesions that remained PET-2–positive (3.84 and 7 cm3, respectively). The probability that a skeletal lesion would remain PET-2–positive increased with increasing initial MTV and increasing initial qPET (Fig. 3).

Probability that skeletal lesions will remain PET-2–positive increases with increasing MTV and increasing qPET. Graph illustrates this dependence based on logistic linear mixed model (with random patient effect). PET-2–negative skeletal lesions (n = 339) are shown as green points and PET-2–positive skeletal lesions (n = 87) as red points. Points are jittered to avoid overprinting.
On PET-2, 343 skeletal lesions were no longer detectable. The other skeletal lesions were still PET-2–positive and showed a median qPET of 1.47 (range, 0.70–4.49). All these lesions presented a decreasing qPET compared with PET-0, with a median reduction of 65% (64% for PET-only lesions, 67% for BM lesions, and 65% for bone lesions).
DISCUSSION
To our knowledge, this study was the largest systematic analysis of the interim PET response of skeletal lesions in HL. Of the 1,068 pediatric HL patients treated in the clinical C1 study (with central reference reading and standardized treatment and follow-up), 139 (13%) showed skeletal involvement. This incidence agrees with other pediatric HL studies, which have reported 11%–18% skeletal involvement (19–22).
Comparison of Skeletal and Nodal Response
In many trials, the interim PET result for HL has been decisive in determining the intensity of therapy. Published data on interim PET response assessment have focused mostly on lymph node involvement (10,11,14), and evidence-based data on skeletal involvement are rare. The PET response assessment of skeletal lesions might be influenced by bone flare, a long-known phenomenon manifesting as an increase in osteoblastic activity on bone scintigraphy under successful treatment of tumorous skeletal lesions (17). Bone flare has also been described for PET and is defined as an increase in the metabolic activity of bone lesions despite a sufficient treatment response by the tumor, as attributed to bone-repairing processes (16,29). Thus, bone flare could lead to false-positive interim PET results and may initiate unnecessary treatment intensification.
In our study, 101 (73%) of the 139 patients with skeletal involvement on PET-0 were negative for skeletal involvement on PET-2, a response rate similar to that for nodal involvement (68%) using the Lugano classification. Therefore, we found no indication that bone flare increases the risk of delayed normalization of skeletal involvement on PET-2. The current PET-2 response criterion for skeletal lesions (comparison with the local skeletal background) seems suitable. This conclusion agrees with published results from smaller patient cohorts reporting remission rates of over 85% for skeletal involvement on interim- or end-of-treatment PET scans (19,30,31).
Comparison of Different Types of Skeletal Lesions
On PET-0, 432 skeletal lesions were detected. The 3 groups into which they were divided (120 PET-only lesions, 171 BM lesions, and 141 bone lesions) systematically differed in qPET, MTV, and PET-2 response. Bone lesions showed the highest qPET and MTV, and PET-only lesions the lowest. The PET-2–negative rate increased from 67% for bone lesions to 80% for BM lesions to 93% for PET-only lesions. These results are consistent with the theory of skeletal involvement as a consecutive process of hematogenic dissemination of HL tumor cells into the BM and subsequent expansion into the bone matrix (bone lesions) (32). PET-only lesions might represent an early phase of BM involvement in HL.
Not only the PET-2–negative but also all PET-2–positive skeletal lesions showed decreasing metabolic activity compared with PET-0. Remarkably, even the 47 PET-2–positive bone lesions presented a median qPET reduction of 65%. This finding is a further sign that bone flare is irrelevant in interim PET scans in HL.
We found that the initial qPET and MTV of skeletal lesions were predictive of their PET-2 result. Higher values for both parameters were associated with a worse PET-2 response (Fig. 3). The risk that a 1-cm3 skeletal lesion with a qPET of 2.0 would remain PET-2–positive was below 5%. For a 10-cm3 lesion, the risk rose to about 10% if qPET was 2.0 but up to about 40% if qPET was 8.0. As a limitation, we have to mention that in some cases MTV measurement was adjusted manually for optimal visual fitting.
Outcome
That 13 patients (10%) showed nodal relapse agrees with the published data on other advanced-stage pediatric HL patients with adequate treatment (1,2). The relapse rate in the skeleton was low, with only 3 patients showing new skeletal lesions up to a median follow-up of 55 mo. This result indicates a good metabolic response of skeletal involvement.
PET-only lesions were not considered for treatment stratification. Therefore, 8 of the 44 PET-only patients were treated in the early-stage group and 5 in the intermediate-stage group. Interestingly, 3 of the 8 patients from the early-stage group showed nodal relapse. This relapse rate of 38% was remarkably higher than that of the PET-only patients treated in the intermediate- or advanced-stage group (3%) or that of the BM and bone patients (10%). This observation might suggest the clinical relevance of PET-only lesions for correct staging (33). However, all 3 early-stage patients with relapse responded well to relapse treatment and showed no suggestive findings on further follow-up.
CONCLUSION
In this study of pediatric HL patients, the PET-2–negative rate for skeletal involvement was similar to that for nodal involvement. Bone flare seemed to be irrelevant. Skeletal relapse was rare. Overall, the current skeletal PET response criterion (comparison with the local skeletal background) is well suited. A higher initial qPET and MTV for skeletal lesions were predictive of a worse PET-2 result.
DISCLOSURE
The EuroNet PHL C1 study was supported by grants from the Deutsche Krebshilfe and the Mitteldeutsche Kinderkrebsforschung. Judith Landman-Parker has a consulting role at Boeringer/Millenium. Jonas Karlen received travel expenses from Takeda. Ana Fernández-Teijeiro received honoraria and travel expenses from Takeda and has a consulting role at Takeda. Michaela Cepelova received travel expenses from Takeda. Alexander Fosså received honoraria and research funding from Takeda and has a consulting role at Takeda. Walentyna Balwierz has a consulting role at Novartis and received travel expenses from Medac. Roland Ammann received travel expenses from Elisa Pharma. Thierry Leblanc received travel expenses from Novartis. Osama Sabri received research funding from Bayer Healthcare, Piramal Imaging, and Siemens Healthcare. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank all participating centers of the EuroNet-PHL-C1 study group for providing the PET imaging data of their patients (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org). We also thank Prof. Adam Glaser, Dr. Andrew Scarsbrook, and Dr. Sue Picton, Leeds Teaching Hospitals, U.K.; Prof. Dr. Michael Schäfers, Prof. Dr. Matthias Weckesser, and Prof. Dr. Heribert Jürgens, University Hospital of Münster, Germany; Prof. Dr. Jörg Kotzerke and Prof. Dr. Manfred Gahr, University Hospital of Dresden, Germany; and Dr. Manlio Cabria and Dr. Alberto Garaventa, Genova, Italy, for providing images of pediatric patients with Hodgkin lymphoma. Furthermore, we thank our sponsors: Deutsche Krebshilfe, Mitteldeutsche Kinderkrebsforschung, Tour der Hoffnung, Menschen für Kindern, Hand in Hand for Children, Kinderkrebshilfe Oldtimer Markt, and the Elternverein für leukämie- und krebskranke Kinder in Gießen.
Footnotes
Published online Apr. 13, 2018.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication November 23, 2017.
- Accepted for publication February 23, 2018.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.