


Abstract
A landmark study from the Institute of Medicine reported that the assessment of cognitive difficulties in children with epilepsy is timely and imperative. Anticonvulsant-induced cognitive impairment could influence the quality of life more than seizure itself in patients. Although the monoaminergic system is involved in the regulation of cognitive process, its role in anticonvulsant-induced cognitive impairment remains unclear. Methods: To explore in vivo monoamine receptor binding activity in patients with anticonvulsant-induced cognitive impairment, each patient underwent PET imaging with both monoamine receptor binding agent 11C-N-methylspiperone and glucose metabolic agent 18F-FDG. Tests of intelligence quotient (IQ), including verbal IQ (VIQ), performance IQ (PIQ), and full-scale IQ (FSIQ), were performed in each patient. Results: Compared with the patients with monotherapy, patients with polytherapy had significantly lower VIQ, PIQ, and FSIQ (P < 0.01 in each comparison), as well as significantly lower monoamine receptor activities detected in the caudate nucleus, prefrontal cortex, dorsal anterior cingulate cortex, and amygdale (P < 0.05 in each comparison). However, regarding the glucose metabolism, there was no significant difference found in patients with monotherapy or polytherapy (P > 0.05). Conclusion: Monoamine receptor PET imaging could be a promising in vivo imaging biomarker for mapping anticonvulsant-induced cognitive impairment.
A landmark study from the Institute of Medicine reports that the chance of developing epilepsy at some point in our lives is 1 in 26 and recommends that the assessment of cognitive difficulties in children with epilepsy is timely and imperative (1). Cognitive impairment is the most common side effect of anticonvulsants, and the risk may accumulate when anticonvulsants are combined (2). Particularly, the developing brains of pediatric patients appear to be particularly sensitive to the cognitive adverse effects of anticonvulsants due to the age-related pharmacokinetic and pharmacodynamic features (3).
PET is ideally suited for monitoring cell/molecular events early in the course of a disease, as well as during pharmacologic or radiation therapy (4). Among PET radioligands for mapping postsynaptic monoamine receptors, 11C-labeled raclopride (11C-raclopride) is the most often used as a standard D2 dopamine receptor (D2DR) ligand (5). However, because the binding of 11C-raclopride to the D2DR in the striatum is competitive with that of endogenous dopamine and reversible in the time frame of a PET scan, it could not reflect the actual changes of postsynaptic receptor level. In contrast, the binding of 11C-N-methylspiperone (11C-NMSP; as a D2DR and 5-hydroxytryptamine receptor 2A [5-HT2AR] antagonist, not competitive with that of endogenous dopamine (5,6) and serotonin (7)) can directly reflect postsynaptic monoamine receptor levels more accurately than 11C-raclopride. Although the monoaminergic system is involved in the regulation of cognitive process, its role in anticonvulsant-induced cognitive impairment remains unclear (8,9). Therefore, we performed 11C-NMSP PET studies to examine the alteration of monoamine receptor activity in pediatric patients with anticonvulsant-induced cognitive impairment.
MATERIALS AND METHODS
Subjects
Twenty-five patients (13 males; mean age ± SD, 13.7 ± 2.0 y) diagnosed with epilepsy (10) were enrolled in this study (Table 1). Sixteen right-handed healthy control participants (9 males; mean age ± SD, 21.6 ± 1.3 y) with no history of neuropsychiatric disorders or receiving psychoactive drugs were included. The Institutional Review Board approved this study (ChiCTR-DDD-15007423), and written informed consent was obtained from each participant.
Clinical Characteristics and Comparisons Between Mono- and Polytherapy Groups
The patient inclusion criteria were as follows: clinical and electroencephalogram findings indicative of focal seizure, age 10–18 y, receiving at least 1 anticonvulsant and without alteration of its dosage in the 3 mo before this study, without developmental disabilities, without history of addictions or other psychiatric illnesses, and right-handedness. Patients were excluded if they had identified epileptic encephalopathies or had comorbidities including depression, anxiety, and attention deficit hyperactivity disorder rather than cognitive impairment. Other exclusion criteria were diagnosis of tuberous sclerosis, tumors, or major hemispheric deformity (such as hemimegalencephaly and porencephaly), becuase these lesions preclude the normalization of PET images.
Each patient underwent at least 1 prolonged (24 h) electroencephalogram monitoring to confirm the localization of the epileptic foci. Video-electroencephalography was performed in 5 patients who presented difficulties in lesion localization. Tests of intelligence quotient (IQ), including verbal IQ (VIQ), performance IQ (PIQ), and full-scale IQ (FSIQ), were performed using the Chinese version of the Wechsler Intelligence Scale for Children (C-WISC) or Adults (C-WISA).
PET Imaging with 11C-NMSP and 18F-FDG
The PET imaging studies were done using a clinical PET/CT scanner (Biograph mCT; Siemens Medical Solutions). Dynamic scans were obtained at 0–40 min after a bolus intravenous injection of 11C-NMSP (3.7 MBq/kg) (11). A 5-min static brain scan was acquired at 40 min after injection of 18F-FDG (3.7 MBq/kg) (12). Interictal PET studies were performed in patients at least 24 h after the last clinical seizure. A pediatric physician carefully monitored each subject during the entire PET imaging study.
PET Data Analysis
Regions of interest were drawn on both hemispheres in the stereotactically normalized images. Voxel-based analysis of asymmetry index (AI) was conducted according to the previous study using statistical parametric mapping (SPM8) (13). Briefly, AI images were calculated at each voxel according to the following formula: AI = (left − right)/([left + right]/2). In the case of the patients with epileptic foci in the right hemisphere, the orientation of AI images were flipped along to the sagittal plane. AI images of patients were then compared with the controls, using the 2-sample t test of the SPM software package, with an ANCOVA by each subject. Decreased or increased results were regarded as statistically significant if the uncorrected P value was under 0.001 (18F-FDG) or 0.01 (11C-NMSP), respectively, with cluster level above 100 voxels.
Statistical Analysis
The results are presented as mean ± SD. All data were analyzed by IBM SPSS Statistics (version 20.0; SPSS/IBM). Analysis of correlation was performed using Pearson correlation coefficients. Group differences in sex, age, age of onset, duration of epilepsy, MRI abnormality, epilepsy type, and IQ were tested using the 2-sample t test or Fisher exact test as appropriate. Stepwise multivariate linear regression analysis was conducted to determine the independent contribution of individual variables (sex, age, age of onset, duration of epilepsy, time since last seizure, seizure frequency, lateralization of epileptic foci, epilepsy type, MRI abnormality, and combination of anticonvulsant) to the IQ or radiotracer. A P value of less than 0.05 was considered statistically significant.
RESULTS
The clinical characteristics of the patients are summarized in Table 1. Twelve patients received 1 type of anticonvulsant, 12 patients received 2 types, and 1 patient required treatment with 3 types. All the patients were tested by C-WISC, except that 2 patients, aged 17.5 and 17.7 y, were tested by C-WISA. The most frequently used drug was oxcarbazepine (OXC; 16 patients), followed by topiramate (TPM; 9 patients), lamotrigine (LTG; 6 patients), levetiracetam (LEV; 4 patients), valproate (VPA; 3 patients), and clonazepam (CZP, 1 patient). The VIQ (Fig. 1A), PIQ (Fig. 1B), and FSIQ (Fig. 1C) in patients with monotherapy were significantly higher than those with polytherapy (P < 0.01 in each comparison). However, the VIQ, PIQ, and FSIQ were not influenced by the sex (P = 0.711, 0.934, and 0.879, respectively), age (P = 0.812, 0.948, and 0.906, respectively), age of onset (P = 0.856, 0.757, and 0.802, respectively), duration of epilepsy (P = 0.881, 0.857, and 0.837, respectively), time since last seizure (P = 0.534, 0.284, and 0.450, respectively), seizure frequency (P = 0.348, 0.338, and 0.424, respectively), lateralization of epileptic foci (P = 0.289, 0.889, and 0.482, respectively), epilepsy type (P = 0.535, 0.847, and P = 0.650, respectively), and MRI abnormality (P = 0.884, 0.638, and 0.769, respectively).
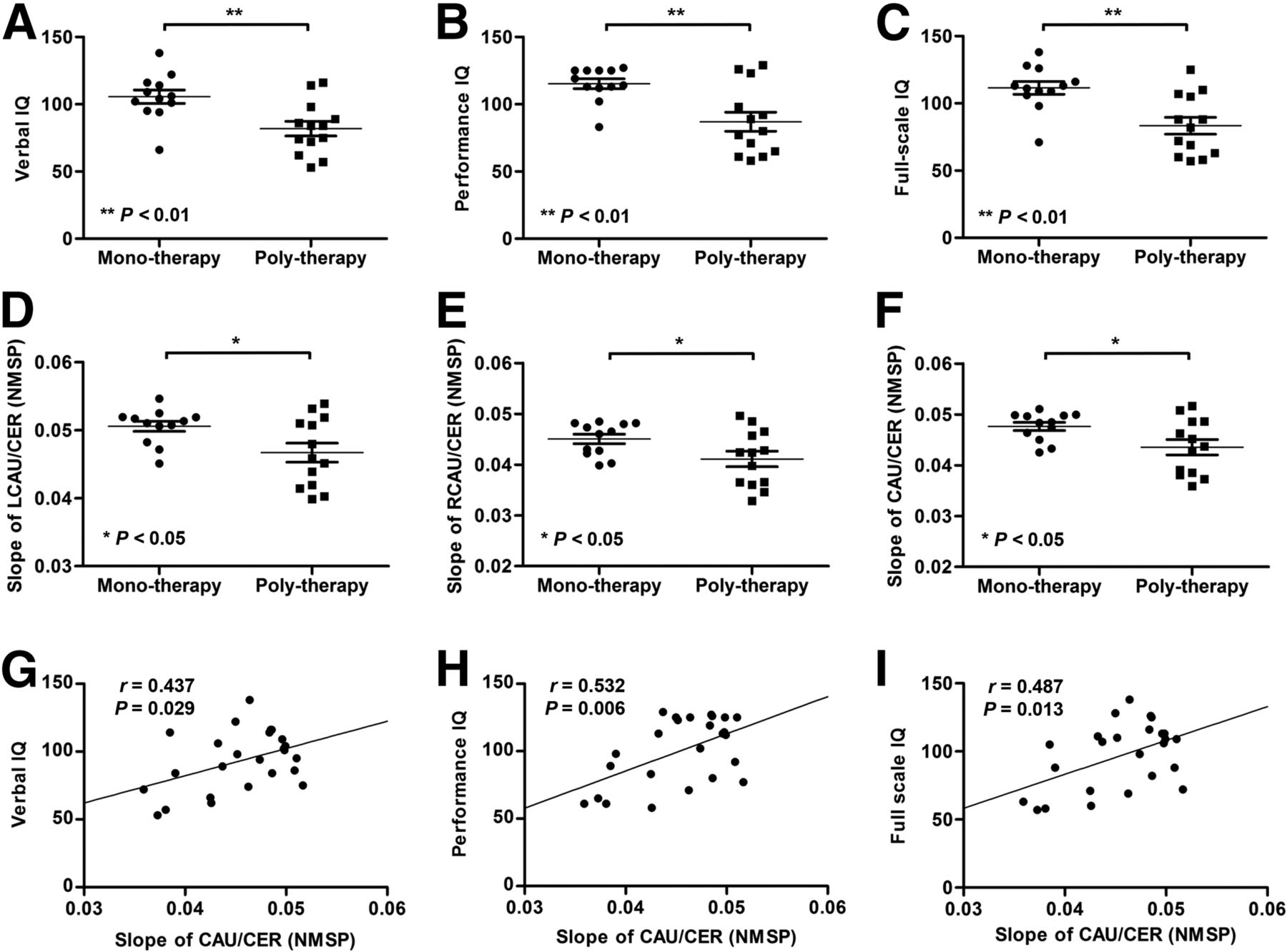
Anticonvulsant-induced cognitive impairment and alteration of monoamine receptor activity in caudate nucleus. (A–C) VIQ, PIQ, and FSIQ were significantly lower in patients with polytherapy compared with those with monotherapy (P < 0.01 in each comparison). (D–F) 11C-NMSP bindings in left, right, or entire caudate nucleus were significantly lower in patients with polytherapy than in those with monotherapy (P < 0.05 in each comparison). (G–I) VIQ, PIQ, and FSIQ were significantly positively correlated with 11C-NMSP binding in caudate nucleus (r = 0.437, 0.532, and 0.487, respectively, P < 0.05 in each comparison).
To determine the independent contribution of individual variables (sex, age, age of onset, duration of epilepsy, time since last seizure, seizure frequency, lateralization of epileptic foci, epilepsy type, MRI abnormality, and combination of anticonvulsant) to the IQ, stepwise multivariate linear regression analysis was conducted. Only the combination of anticonvulsant (mono- vs. polytherapy) was found as the significant contributing variable to FSIQ (B = −28.1; SEM = 8.0; P = 0.002).
Monoamine Receptor Activity: Between-Group Differences (Monotherapy Versus Polytherapy)
11C-NMSP bindings in the left (Fig. 1D), right (Fig. 1E), or entire (Fig. 1F) caudate nucleus, were significantly lower in patients with polytherapy than in those with monotherapy (P < 0.05 in each comparison). No significant difference of 11C-NMSP binding was found between the 2 groups either in the putamen or in the pallidum (P = 0.085 and 0.920, respectively). Compared with those with monotherapy, patients with polytherapy were detected with significantly lower 11C-NMSP bindings in the right Broadman area 9 (BA9R; Fig. 2A), right Broadman area 10 (BA10R; Fig. 2C), right Broadman area 32 (BA32R; Fig. 2E), right Broadman area 45 (BA45R; Fig. 2I), left Broadman area 46 (BA46L; Fig. 2K), and amygdala (Fig. 2G) (P < 0.05 in each comparison).
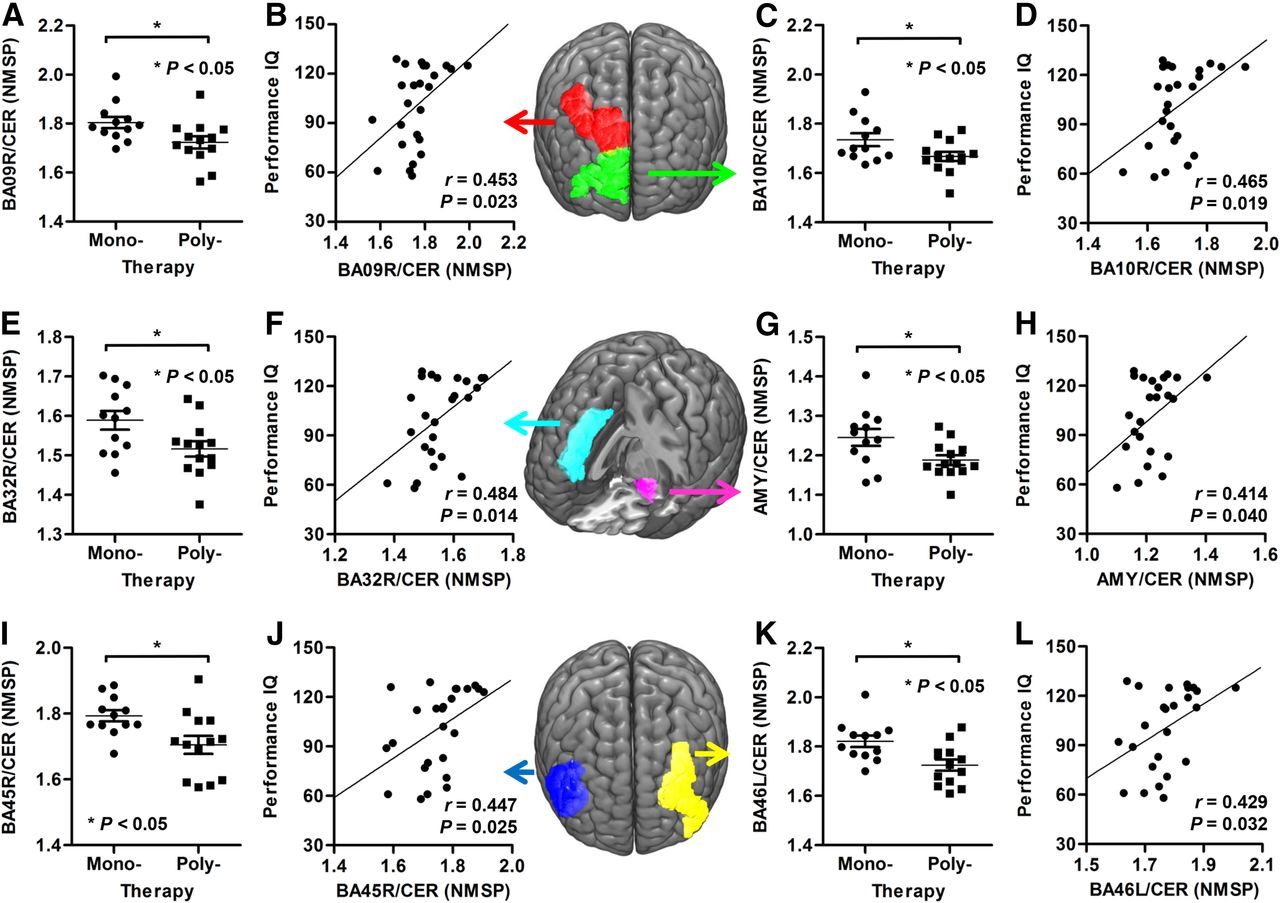
Anticonvulsant-induced cognitive impairment and alteration of monoamine receptor activity in cortex. (A, C, E, G, I, and K) Patients with polytherapy were detected with significantly lower 11C-NMSP bindings than those with monotherapy in BA9R, BA10R, BA32R, BA45R, BA46L, and amygdala (P < 0.05 in each comparison). (B, D, F, H, J, and L) 11C-NMSP bindings in BA9R, BA10R, BA32R, BA45R, BA46L, and amygdala were significantly positively correlated with PIQ (r = 0.453, 0.465, 0.484, 0.447, 0.429, and 0.414, respectively, P < 0.05 in each comparison).
In these brain regions, a combination of anticonvulsants was the only significant contributing variable to 11C-NMSP binding using stepwise multivariate linear regression analysis (Table 2, P < 0.05 in each region). However, regarding the glucose metabolism, there was no significant difference found in patients with monotherapy or polytherapy (P > 0.05).
Results of Multivariate Linear Regression: Independent Contributions to Monoamine Receptor Activity (Mono- Versus Polytherapy)
Correlation Between Monoamine Receptor Activity and Cognitive Function
Regarding the relationship between regional 11C-NMSP binding and VIQ (Fig. 1G), PIQ (Fig. 1H), or FSIQ (Fig. 1I), significantly positive correlations were found in the caudate nucleus (r = 0.437, 0.532, and 0.487, respectively, P < 0.05 in each comparison), but neither in the putamen (P = 0.262, 0.407, and 0.330, respectively), nor in the pallidum (P = 0.305, 0.853, and 0.520, respectively). The 11C-NMSP bindings in BA9R (Fig. 2B), BA10R (Fig. 2D), BA32R (Fig. 2F), BA45R (Fig. 2J), BA46L (Fig. 2L), and amygdala (Fig. 2H) were significantly positively correlated with PIQ (r = 0.453, 0.465, 0.484, 0.447, 0.429, and 0.414, respectively, P < 0.05 in each comparison), but not with VIQ (P = 0.122, 0.075, 0.129, 0.377, 0.064, and 0.201, respectively). The FSIQ was significantly positively correlated with the 11C-NMSP bindings in BA9R, BA10R, BA32R, and BA46L (r = 0.398, 0.437, 0.397, and 0.420, respectively, P < 0.05 in each comparison).
Correlation Between Monoamine Receptor Activity and Glucose Metabolism
In patients with rolandic epilepsy (RE), SPM analysis revealed significant reductions of 11C-NMSP binding in the ipsilateral postcentral gyrus, superior temporal gyrus, lingual gyrus, and rolandic operculum (Puncorrected < 0.01, cluster size > 100; Fig. 3A; Table 3) and found significant hypometabolism in the ipsilateral rolandic operculum, superior temporal gyrus, postcentral gyrus, and hippocampal gyrus (Puncorrected < 0.001, cluster size > 100; Fig. 3A; Table 4). Decreased monoamine receptor binding and glucose metabolism were found overlapped in the rolandic operculum, postcentral gyrus, and superior temporal gyrus (Fig. 3A). The 11C-NMSP binding in the ipsilateral rolandic operculum was significantly positively correlated with glucose metabolism (r = 0.651, P < 0.05; Fig. 3C).

Correlation between monoamine receptor activity and glucose metabolism. (A) SPM analysis on RE patients revealed significant decreases of 11C-NMSP binding in ipsilateral postcentral gyrus, superior temporal gyrus, lingual gyrus, and rolandic operculum (ROL) (Puncorrected < 0.01, cluster size > 100), and decreases of glucose metabolism in ROL, superior temporal gyrus, postcentral gyrus, and hippocampal gyrus (Puncorrected < 0.001, cluster size > 100). Decreased monoamine receptor binding and glucose metabolism were found overlapped in ROL, postcentral gyrus, and superior temporal gyrus. (B) As for TLE patients, significant decreases of 11C-NMSP binding were found in ipsilateral parahippocampal gyrus and inferior and middle temporal gyri (Puncorrected < 0.01, cluster size > 100), and decreases of glucose metabolism in ipsilateral inferior, middle, and superior temporal gyri; hippocampal gyrus; fusiform gyrus; and ROL (Puncorrected < 0.001, cluster size > 100). Monoamine receptor dysfunction overlapped with glucose metabolic abnormality in inferior and middle temporal gyri. (C) In RE patients, 11C-NMSP bindings in ipsilateral ROL were significantly positively correlated with glucose metabolism (r = 0.651, P = 0.016). (D and E) For TLE patients, 11C-NMSP bindings were significantly positively correlated with glucose metabolism in ipsilateral middle temporal gyrus (TEM-M) and parahippocampal gyrus (PAR) (r = 0.756 and 0.855, respectively, both P < 0.05).
Results of SPM Analysis on NMSP Binding (Epilepsy Patients Versus Control Group)
Results of SPM Analysis on 18F-FDG Uptake (Epilepsy Patients Versus Control Group)
For the temporal lobe epilepsy (TLE) patients, significant reductions of 11C-NMSP binding were found in the ipsilateral parahippocampal gyrus and inferior and middle temporal gyri (Puncorrected < 0.01, cluster size > 100; Fig. 3B; Table 3); in addition, hypometabolism presented in the ipsilateral inferior, middle, and superior temporal gyri; hippocampal gyrus; fusiform gyrus; and rolandic operculum (Puncorrected < 0.001, cluster size > 100; Fig. 3B; Table 4). Monoamine receptor dysfunction overlapped with the glucose metabolic abnormality in the inferior and middle temporal gyri (Fig. 3B). 11C-NMSP bindings were significantly positively correlated with glucose metabolism in the ipsilateral middle temporal gyrus (r = 0.756, P < 0.05; Fig. 3D) and parahippocampal gyrus (r = 0.855, P < 0.05; Fig. 3E).
DISCUSSION
We report that cognitive performance significantly positively correlated with the 11C-NMSP binding in the caudate nucleus, prefrontal cortex (PFC), dorsal anterior cingulate cortex (dACC), and amygdale. This result suggests that polytherapy-induced cognitive impairment is related to the reduction of monoamine receptor activity. To the best of our knowledge, this is the first study on the neural correlate between anticonvulsant-induced cognitive impairment and the alteration of monoamine receptor activity or glucose metabolism detected by in vivo PET imaging with 11C-NMSP and 18F-FDG in pediatric epilepsy.
Our study demonstrated that in patients with polytherapy, monoamine receptor activities decreased in the caudate nucleus, PFC (BA9R, BA10R, BA45R, and BA46L), dACC (BA32R), and amygdala. This is consistent with the preclinical study on anticonvulsant-induced impaired cognitive function in nonepileptic rats in which impaired cognition was found to be attributed to the increased hippocampal 5-HT levels for phenytoin (14), but to the decreased hippocampal dopamine levels for ethosuximide (15). However, phenytoin-associated elevated monoamine levels in the cortex and hippocampus could not justify the associated memory loss in a rat model of epilepsy (16). These discrepancies might be explained by the suggestion that increased or decreased release of monoamines depends on the concentration of anticonvulsants and the procedure used to evoke neurotransmitter release (17). In adult TLE patients, no significant effects of anticonvulsants on 5-HT1AR binding were observed using 18F-FCWAY PET imaging (18). The adverse effect of anticonvulsants on cognition could also be attributed to Na+ channel blockade, enhanced GABAergic activity, or decrement in glutamate-mediated excitation (19). On the basis of these findings and our results, we speculated that the interaction between multiple anticonvulsants in ion channels and neurotransmitter receptors might aggravate the anticonvulsant-induced cognitive impairment. Because the research on the mechanism of anticonvulsant-induced cognitive impairment is still in its infancy, with many issues that need to be addressed, elucidation of its mechanism has been appraised as one of the epilepsy research priorities (20).
PET imaging in this study indicated that the cognitive performance (VIQ, PIQ, and FSIQ) significantly positively correlated with the 11C-NMSP binding in caudate nucleus. Accumulated evidence has shown that the dopaminergic system, especially D2DR, is profoundly associated with cognition (8,21). D2DR makes a specific contribution to hippocampus-based cognition by influencing the striatum and limbic system, and their interactions (21). Another important finding in our study was that 11C-NMSP bindings in the PFC, dACC, and amygdala were positively correlated with PIQ. Apart from dopamine, 5-HT signaling at 5-HT2AR also has important effects on several behavioral and cognitive pathways, with the PFC as the central actor (9). In addition, activation of the 5-HT2AR in PFC has a modulatory effect on dopamine neurons, indicating that 5-HT can interact with other modulators of diverse cognitive processes (22). Though the amygdala lies at the center of much of our current thinking about emotion, its role is indeed quite broad and connected with cognitive functions according to amygdala–PFC interactions (23). Additionally, the dACC is also supposed to play a key role in fundamental cognitive processes, including motivation, decision making, and learning (24). Our data further highlighted the crucial role of D2DR and 5-HT2AR on cognitive function in pediatric patients with epilepsy.
In our current study, significant decreases in VIQ, PIQ, and FSIQ were found in patients with polytherapy compared with those with monotherapy. This finding is in line with a recent study that each additional drug increased the risk of cognitive side effects (2). Cessation of anticonvulsants was the strongest predictor of postoperative IQ increase, even after exclusion of patients with continuing seizures (25). Therefore, it is recommended that epilepsy patients should be treated with a single anticonvulsant wherever possible, and combination anticonvulsants should be considered only when attempts at a single anticonvulsant have not resulted in seizure freedom (26). Routine cognitive monitoring of anticonvulsants would be highly valuable to optimize outcomes and improve adherence to the prescribed medication (27). Apart from conventional IQ test, we suggested that 11C-NMSP PET imaging could be one potential evaluation approach for the cognitive monitoring in pediatric epilepsy.
18F-FDG PET imaging of brain glucose metabolism is a well-established and widely available technique for assessment of epilepsy, and the characteristic finding is a regional hypometabolism during the interictal period. Although hypometabolism has been ascribed to factors such as neuronal loss and diaschisis, its underlying neurobiology is not well understood (28). In the present study, deceased monoamine receptor activity and glucose metabolism were found overlapped in epileptic foci in patients with RE and TLE. The positive correlation between hypometabolism and the reduction of monoamine receptor binding in our study suggested that the abnormal cerebral metabolism might be associated with alterations in neurotransmitters and synaptic activity. The occurrence of epileptic seizures has been explained by an imbalance between excitatory (glutamatergic) and inhibitory (GABAergic) neurotransmission. Some other neurotransmitter systems are known to be involved in the epileptogenesis, including dopamine and 5-HT (29). PET studies revealed a reduction of D2R/D3R binding in TLE and juvenile myoclonic epilepsy (30,31) and reduction of 5-HT1AR binding ipsilateral to TLE foci (13). Our study further demonstrated that 5-HT2AR binding decreased both in RE and in TLE patients. This finding is inconsistent with the previous report (32). 5-HT has an anticonvulsant effect in epilepsy, and the 5-HT2ARs appear to play a major role. However, further studies are needed to understand the role of 5-HT2AR in epilepsy and its modulation of other neurotransmitter systems.
It is important to acknowledge the potential limitation in this study. First, the baseline cognitive function before anticonvulsant therapy, usually 5 y ago, was not considered in the current study. However, numerous studies have demonstrated that the cognitive impairment may cumulate when anticonvulsants are combined, regardless of the pretreatment assessment of cognitive function (2). Second, we did not find significant correlation between cognitive impairment and other clinical variables, including age of onset, duration of epilepsy, and seizure frequency, which might be due to the limited numbers in each category.
CONCLUSION
Our findings document that cognitive performance significantly positively correlated with the monoamine receptor binding in the caudate nucleus, PFC, dACC, and amygdale in pediatric epilepsy. These results indicated an important role of monoamine receptor dysfunction in anticonvulsant-induced cognitive impairment.
DISCLOSURE
This work is partly sponsored by grants from the National Key Research and Development Program of China (2016YFA0100900), National Key Basic Research Program of China (2013CB329506), National Science Foundation of China (NSFC) (no. 81425015, 81271601), and Zhejiang Provincial Natural Science Foundation of China (LR13H180001). No other potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Mar. 16, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication December 29, 2016.
- Accepted for publication February 27, 2017.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.