


Abstract
The aim of this study was to compare survival of patients treated for unresectable hepatocellular carcinoma (uHCC) with 90Y transarterial radioembolization (TARE) using pretreatment partition model dosimetry (PMD). Methods: We performed a retrospective analysis of prospectively collected data on 77 patients consecutively treated (mean age ± SD, 66.4 ± 12.2 y) for uHCC (36 uninodular, 5 multinodular, 36 diffuse) with 90Y TARE (41 resin, 36 glass) using pretreatment PMD. Study endpoints were progression-free survival (PFS) and overall survival (OS) assessed by Kaplan–Meier estimates. Several variables including Barcelona Clinic Liver Cancer (BCLC) staging system, tumor size, and serum α-fetoprotein (AFP) level were investigated using Cox proportional hazards regression. Results: The characteristics of 2 groups were comparable with regard to demographic data, comorbidities, Child–Pugh score, BCLC, serum AFP level, and 90Y global administered activity. The median follow-up time was 7.7 mo (range, 0.4–50.1 mo). Relapse occurred in 44 patients (57%) at a median of 6 mo (range, 0.4–27.9 mo) after 90Y TARE, and 41 patients (53%) died from tumor progression. Comparison between resin and glass microspheres revealed higher but not statistically significantly PFS and OS rates in the 90Y resin group than the 90Y glass group (resin PFS 6.1 mo [95% confidence interval CI, 4.7–7.4] and glass PFS 5 mo [95% CI, 0.9–9.2], P = 0.53; resin OS 7.7 mo [95% CI, 7.2–8.2] and glass OS 7 mo [95% CI 1.6–12.4], P = 0.77). No significant survival difference between both types of 90Y microspheres was observed in any subgroups of patients with early/intermediate or advanced BCLC stages. Among the variables investigated, Cox analyses showed that only in the glass group, the BCLC staging system and the serum AFP level were associated with PFS (P = 0.04) and OS (P = 0.04). Tumor size was a prognostic factor without significant influence on PFS and OS after 90Y TARE. Conclusion: Comparison between resin and glass microspheres revealed no significant survival difference in patients treated for uHCC with 90Y TARE using pretreatment PMD. Further, larger prospective studies are warranted to confirm these findings.
Hepatocellular carcinoma (HCC) is the most common primary liver cancer and represents the second most common cause of cancer mortality worldwide (1). Despite new treatment options, HCC has a poor prognosis, with an overall 5-y relative survival rate of 18% (2). Moreover, more than 70% of patients present at an advanced stage, beyond potentially curative options (hepatic resection, liver transplantation, percutaneous ablation). The Barcelona Clinic Liver Cancer (BCLC) staging system was developed on the basis of a retrospective analysis of various studies of HCC patients with early, intermediate, and advanced terminal disease, which attempted to identify prognostically relevant variables for each group (3). For patients with early stage disease, survival was negatively correlated with portal hypertension and bilirubin levels greater than 1.5 mg/dL; for intermediate stages, the significant variable was a large multinodular tumor, and for advanced disease, deterioration of performance status and the presence of portal vein invasion (PVI), which is associated with a poor prognosis. In patients with PVI, studies have reported overall survival (OS) ranging from 2 to 4 mo, compared with 10–24 mo in HCC patients without PVI (3–5).
Given the hypervascularity of HCC, intraarterially injected microspheres will be preferentially delivered to the tumor-bearing area and selectively emit high-energy, low-penetration radiation to the tumor (6). Two Food and Drug Administration–approved 90Y microsphere products are currently used: resin microspheres (SIR-Spheres; SIRTex Medical) and glass microspheres (TheraSphere; BTG Biocompatibles Ltd.), which differ in several characteristics including size, the number of microspheres typically injected in a single treatment (<5 to 10–30 million) (7), and activity per microsphere (8).
Resin microspheres manufacturer–recommended 90Y activity prescription is based on a semiempiric formula including body surface area (9,10) and tumor burden. This approach can be refined using a 3-compartment partition model (11) including the lungs and tumoral (TV) and targeted nontumoral liver volumes derived from pretreatment 99mTc-macroaggregated albumin (99mTc-MAA) SPECT/CT. Glass microspheres 90Y activity prescription is based on a 2-compartment model (lungs and targeted liver regions) aiming to deliver an absorbed dose of 80–150 Gy in the target liver volume.
It is now well established that 90Y TARE slows down disease progression and improves survival in patients with HCC (12). However, comparison of the survival of patients treated with both types of 90Y microspheres using partition model dosimetry (PMD) remains unclear in HCC. To the best of our knowledge, only a recent retrospective review (13) has compared the outcome of both types of 90Y microspheres in patients with unresectable HCC (uHCC), concluding in a survival benefit for glass microspheres. The aim of the current study was to compare progression-free survival (PFS) and OS between 2 groups of patients treated with 90Y resin and glass microspheres for uHCC using pretreatment PMD (14). Second, we compared PFS and OS of each type of 90Y microsphere according to early/intermediate (combining BCLC A and B) stages and the advanced (BCLC C) stage, which is associated with a poor prognosis.
MATERIALS AND METHODS
Patient Selection
We performed a retrospective analysis of prospectively collected data on 77 consecutively treated patients (67 men; mean age ± SD, 66.4 ± 12.2 y) with 90Y TARE (41 resin, 36 glass) for uHCC (36 uninodular, 5 multinodular, 36 diffuse) between 2010 and 2016. The guidelines of the American Association for the Study of Liver Diseases (15) were used to diagnose HCC. The BCLC staging system was used to stage HCC (3). Patients were considered for 90Y TARE when no curative options (resection or transplantation) were possible due to a locally advanced tumor, a multifocal disease, a poor liver reserve, a PVI, or an extrahepatic metastasis. Inclusion criteria consisted of patients aged 18 y or older with a liver-dominant or liver-only disease; an adequate hematologic, renal, and hepatic function; a good Eastern Cooperative Oncology Group Performance Status < 2; and a life expectancy > 3 mo. Patients with an inadequate liver reserve (bilirubin > 34 μmol/L, ascites), a poor Eastern Cooperative Oncology Group Performance Status ≥ 2, a higher lung shunt fraction > 20%, an estimated lung absorbed dose of >30 Gy per session and 50 Gy in total, and an uncorrectable extrahepatic flow on the pretherapy 99mTc-MAA SPECT/CT were immediately excluded.
All patients underwent 90Y TARE as standard care and gave their informed consent for the treatment. The local Ethics Research Committee of the State of Vaud took into account the retrospective analysis of our database, approved the protocol (no. 2016-00640), and waived the need for patient informed consent for the study analysis.
Data Collection
Demographic, clinical, biologic, imaging, treatment (before and after the 90Y TARE procedure), and 90Y TARE dosimetric data were collected retrospectively from patients treated for uHCC with 90Y TARE using pretreatment PMD between 2010 and 2016. All patients underwent CT or MRI scans before the 90Y TARE procedure to evaluate the tumor size (calculated by the longest diameter of all measurable tumors), number, and distribution of lesions and presence of ascites and PVI.
90Y Administered Activity Calculation
Resin microsphere dosimetry is based on a 3-compartment partition model aiming at keeping the absorbed dose to the targeted nontumoral volume below 70 and 50 Gy for lobar and total liver treatment, respectively, as recommended by Lau et al. (10). 90Y glass sphere activity determination is based on a 2-compartment model (lungs + targeted liver region) aiming at delivering an absorbed dose between 80 and 150 Gy in target liver volume. In analogy with the resin sphere dosimetry, we refined the 90Y activity determination by applying as a second step a partition model accounting for TV and nontumoral liver volume and differential particle distribution (tumoral-to-nontumoral ratio) estimated from 99mTc-MAA SPECT/CT to predict TV and targeted nontumoral liver absorbed dose. In line with the suggested threshold for OS by Garin et al., in lobar TARE, we kept the average predicted absorbed dose to the targeted nontumoral liver volume < 70 Gy provided that this allowed a predicted tumor-absorbed dose > 205 Gy (16).
90Y TARE Planning and Procedure
All patients underwent a pretherapy SPECT/CT with 120–180 MBq of 99mTc-MAA 1–3 wk before the 90Y TARE procedure. Whenever necessary, coiling of the gastroduodenal, right gastric artery, or gastroduodenal branches was performed, and the 99mTc-MAA was injected into the hepatic artery selected. The patient was immediately (<20 min) transferred to the nuclear medicine department for SPECT/CT, whole-body, and planar imaging within 1 h. Lung shunting was evaluated on whole-body and planar images. The TV was assessed on SPECT/CT with morphologic information from any available imaging modalities (enhanced CT, MR, or 18F-FDG PET/CT) when needed. The TV estimated from the 99mTc-MAA SPECT/CT was used to determine the activity of 90Y microspheres to administer using our recently published PMD for TARE (14). Patients with small-tumor volumes were preferentially addressed to 90Y glass microspheres because of their higher specific 90Y activity and lower particle number aiming at avoiding lesion saturation and consecutive reflux to nontarget volumes. Post-TARE SPECT/CT was performed to confirm the distribution of 90Y microspheres. All 99mTc-MAA and 90Y TARE procedures were performed by experienced radiologists and nuclear medicine physicians.
Statistical Analysis
Continuous variables are described as median (with 25th–75th interquartile range in parentheses) and dichotomous data as percentages. The characteristics of populations were compared using the χ2 test, with the Pearson correction for discrete variables and t test or Mann–Whitney test for continuous variables. Study endpoints were PFS and OS. PFS was defined as the time from the date of 90Y TARE until the first occurrence of disease progression, which was determined by biologic and contrast-enhanced MRI (bidimensional response criteria of the World Health Organization and bi-dimensional of the viable portion of the tumors using the response criteria of the European Association for the study of the liver). OS was defined as the time from the date of the 90Y TARE until death from tumor progression. Survival functions were obtained from Kaplan–Meier estimates and compared using the log-rank test. The influence of several variables including BCLC staging system, tumor size, and serum α-fetoprotein (AFP) level was investigated using Cox proportional hazards regression in the entire cohort and in each group. All statistical analyses were performed using SPSS software (version 23 for Windows 2010; SPSS Inc.). P values of less than 0.05 were considered statistically significant.
RESULTS
Study Population
The characteristics of 2 groups were statistically comparable for demographic, clinical, and biologic data (Table 1). In the entire cohort, when the BCLC staging system was used, 5 patients (6%) were stage A, 30 (39%) stage B, and 42 (55%) stage C. Eleven patients (14%) had normal livers; all others (86%) had cirrhotic liver disease, including 51 patients with Child–Pugh A and 15 patients with Child–Pugh B (≤ B7). Five patients (6%) had a metastatic disease: to lymph nodes and lungs (n = 2), to peritoneum and lungs (n = 1), to lymph nodes and peritoneum (n = 1), and to adrenal glands (n = 1). Regarding 90Y TARE, the median 90Y administered activity was similar between the 2 groups, with 1.80 GBq (range, 0.50–5.46 GBq) and 1.81 GBq (range, 0.49–6.85 GBq) in resin and glass groups, respectively (P = 0.52, Table 2); when the TV was taken into account, the 90Y administered activity per unit of TV (expressed as MBq/cm3) was significantly higher in the glass group (P = 0.04, Table 2), explained by the higher number of segmental 90Y TARE in this group (P = 0.003, Table 2). There were 41 lobar, 13 whole-liver, 13 segment, 1 partial lobe, 6 lobar and segment, and 3 lobar and partial lobe treatments. Among the 77 patients, 48 (62%) were treatment-naïve and 29 (38%) had already received various procedures before 90Y TARE including targeted therapy by sorafenib or everolimus (n = 5), embolization (n = 6), transarterial chemoembolization (n = 19), radiofrequency ablation (n = 17), or ethanol ablation (n = 3), with an association of 2 or more treatment modalities in 12 patients (16%).
Population Characteristics
90Y TARE and Treatment-Associated Data
Survival Analysis
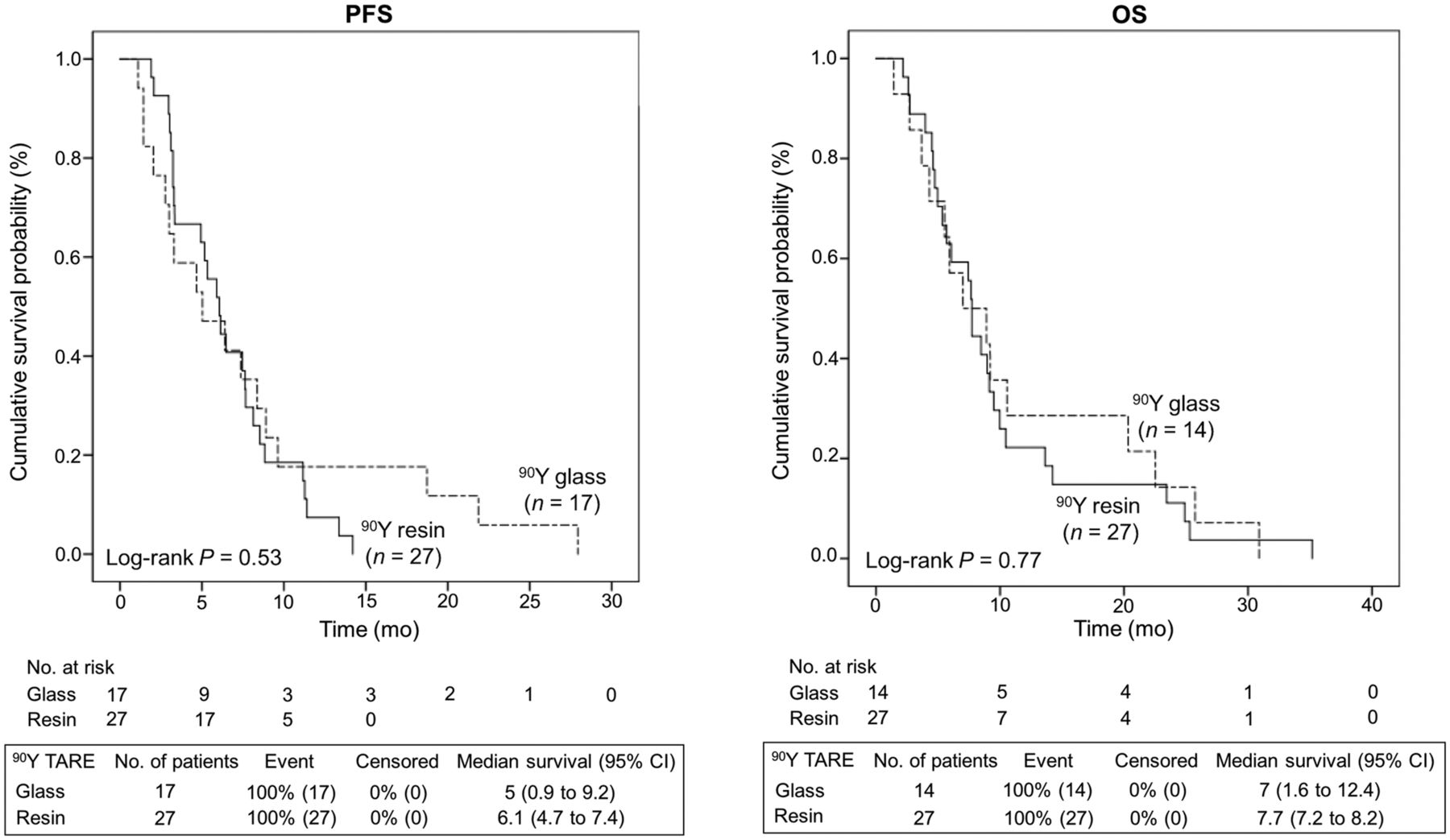
The median follow-up in living patients was 7.7 mo (range, 0.4–50.1 mo). Relapse occurred in 44 patients (57%) at a median of 6 mo (range, 0.4–27.9 mo) after 90Y TARE, and 41 (53%) patients died from tumor progression. As shown in Figure 1, comparison between resin and glass microspheres in the entire cohort revealed higher but not statistically significant PFS and OS rates for the 90Y resin group than the 90Y glass group (resin PFS, 6.1 mo [95% confidence interval (CI), 4.7–7.4 mo], and glass PFS, 5 mo [95% CI, 0.9–9.2 mo], P = 0.53; resin OS, 7.7 mo [95% CI, 7.2–8.2 mo], and glass OS 7 mo [95% CI, 1.6–12.4 mo], P = 0.77). PFS and OS rates at 6 mo, 1 y, and 2 y from the 90Y TARE were 52% and 63%, 7% and 22%, and 0% and 11% in the resin group and 47% and 57%, 18% and 29%, and 6% and 14% in the glass group.

Kaplan–Meier estimates of PFS and OS in entire treated cohort.
Regarding the BCLC staging system, no significant survival difference between both types of 90Y microspheres was observed in subgroups of patients with early/intermediate or advanced BCLC stages (Fig. 2). However, there was a small but not significant survival benefit in PFS in patients with early/intermediate BCLC stage compared with those with advanced BCLC stage in the glass group (P = 0.06, Fig. 3).
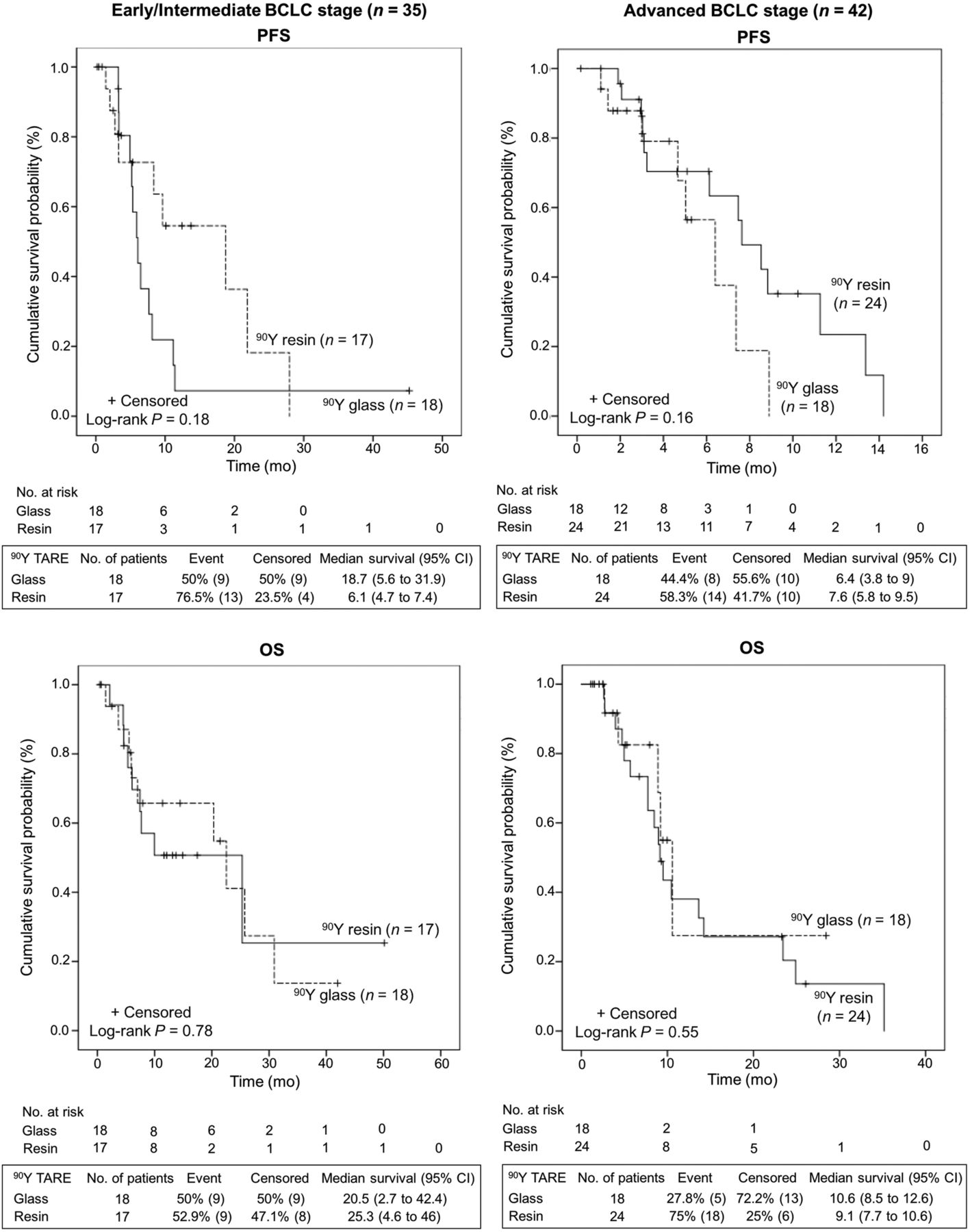
Kaplan–Meier estimates of PFS and OS in patients with early/intermediate BCLC and advanced BCLC.

Kaplan–Meier estimates of PFS and OS patients with early/intermediate BCLC and advanced BCLC according to both types of 90Y microspheres for TARE.
Multivariable Regression
Results of Cox proportional hazards regression performed in the entire cohort and in each group are given in Table 3. Among the several variables investigated including BCLC, tumor size, and serum AFP level, only in the glass group, the BCLC staging system and the serum AFP level were associated with PFS (P = 0.04) and OS (P = 0.04). Tumor size was a prognostic factor without significant influence on PFS and OS after 90Y TARE in the current study.
Prognostic Factors in Multivariable Regression for PFS and OS According to Entire Cohort and 90Y Resin and Glass Groups
DISCUSSION
We performed a retrospective analysis of prospectively collected data on 2 groups of patients treated with 90Y resin and glass microspheres for uHCC using pretreatment PMD. In brief, our study shows equal outcomes regarding PFS and OS in patients with uHCC.
There are 2 large phase II studies by the group of Sangro et al. (17) using resin and by Salem et al. (18) using 90Y glass microspheres. The study using resin microspheres revealed an OS of 24.4 mo in BCLC A, 16.9 mo in BCLC B, and 10.0 mo in BCLC C patients. The Salem et al. study reproduced these promising results of 26.9 mo in BCLC A, 17.2 mo in BCLC B, and 7.3 mo in BCLC C. However, again these studies were not comparable because the therapeutic 90Y administered activities were calculated differently. In the case of the glass microspheres study, 90Y activities were calculated aiming a target absorbed dose of 100–120 Gy to the target liver volume (19); the resin microspheres study published by Sangro et al. (17) used a combination of the body surface area method or modified PMD with a mean 90Y administered activity of 1.6 GBq, and the results of these studies were not directly comparable. In the glass group, our study revealed a median OS of 25.3 mo in early/intermediate BCLC stage and 20.5 mo in advanced BCLC stage (Fig. 2), which is in accordance with the study published by Sangro et al. (17) and Salem et al. (18) and shows that our patient population has been chosen according to published standards. The only small but not significant survival benefit was observed in patients with early/intermediate BCLC stage compared with those with advanced BCLC stage in favor of 90Y glass microspheres.
A recent retrospective analysis in uHCC patients with PVI claimed a superiority of glass versus resin microspheres. This report published a significantly higher OS in the 90Y glass group (P < 0.001) whereas PFS was not higher (P = 0.48) (13). However, the inaccurate body surface area method was used in the study by Biederman et al. (13) and may partly explain the improved OS observed in patients treated with 90Y glass microspheres. Here, we present the first study, to our knowledge, comparing resin microspheres and glass microspheres using pretreatment PMD and demonstrate that both approaches seem to be comparable in regard to PFS and OS. This finding is important because there is an ongoing discussion about how and which treatments to use for the types of HCC and which treatment might be superior. Others studies seem still to be warranted to investigate this question.
There are several limitations to this study. First, the current study was a retrospective and single-center study with a relatively limited number of patients. However, our study remains the second largest report after the study of Biederman et al. study (13) comparing groups of patients treated by both types of 90Y microspheres. Second, a further important potential bias was the tumor size. Indeed, patients with small tumor volumes were most often referred to glass microspheres. Although the difference in size was not statistically different between both groups, the tumor size is a well-known factor associated with outcome and may have had a direct impact on our survival results. This bias is consistent with the significantly higher number of segmental treatments and the significantly higher administered 90Y activity per tumor volume (and consequently the dose delivered to tumors) in the glass group and reflects the paradigm of radiation segmentectomy, which has been previously published using glass microspheres (20). Furthermore, a significant proportion of patients had undergone treatment before (38%) and after (32%) the 90Y TARE procedure, however, no statistical difference between either group was observed and this is a classic finding in modern studies in patients with several treatment possibilities.
CONCLUSION
Comparison between resin and glass microspheres revealed no significant survival difference in patients treated for uHCC with 90Y TARE using pretreatment PMD. Further larger prospective studies are warranted to confirm these findings.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 12, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 19, 2016.
- Accepted for publication December 20, 2016.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.