


Abstract
A fast-track pathway has been established in Denmark to investigate patients with serious nonspecific symptoms and signs of cancer (NSSC), who are not eligible to enter an organ-specific cancer program. The prevalence of cancer in this cohort is approximately 20%. The optimal screening strategy in patients with NSSC remains unknown. The aim of the study was to investigate whether 18F-FDG PET/CT was superior to CT as an initial imaging modality in patients with NSSC. In a randomized prospective trial, the imaging modalities were compared with regard to diagnostic performance. Methods: Two hundred patients were randomized 1:1 to whole-body 18F-FDG PET/CT or CT of the thorax and abdomen as the imaging modality. A tentative diagnosis was established after first-line imaging. The final referral diagnosis was adjudicated by the physician, when sufficient data were available. Results: One hundred ninety-seven patients were available for analysis because 3 patients withdrew consent before scanning. Thirty-nine (20%) patients were diagnosed with cancer, 10 (5%) with an infection, 15 (8%) with an autoimmune disease, and 76 (39%) with other diseases. In the remaining 57 patients (28%), no specific disease was found. 18F-FDG PET/CT had a higher specificity (96% vs. 85%; P = 0.028) and a higher accuracy (94% vs. 82%; P = 0.017) than CT. However, there were no statistically significant differences in sensitivity (83% vs. 70%) or negative predictive values (96% vs. 92%). No difference in days to final referral diagnosis according to randomization group could be shown (7.2 vs. 7.6 d). However, for the subgroups in which the imaging modality showed a suggestion of malignancy, there was a significant delay to final diagnosis in the CT group compared with the 18F-FDG PET/CT group (11.6 vs. 5.7 d; P = 0.02). Conclusion: Compared with CT, we found a higher diagnostic specificity and accuracy of 18F-FDG PET/CT for detecting cancer in patients with NSSC. 18F-FDG PET/CT should therefore be considered as first-line imaging in this group of patients.
In 2009, fast-track cancer patient pathways were introduced by the Danish Health and Medicine Authority for patients with nonspecific symptoms and signs of cancer (NSSC) in Denmark. The background for the implementation was that Danish patients experience poorer cancer survival rates than patients from other European countries and were diagnosed with an unfavorable delay (1–4). Since 2012, Diagnostic Outpatient Clinics (DOC) have been established in the Capital Region of Denmark for patients with NSSC because early diagnosis in cancer is of importance for a more favorable outcome (5–8). The criterion for referral to DOC was a suspicion from the referring physicians, in more than 95% of the cases the patient’s general practitioner, that the patient had an NSSC. The referral was typically prompted by one or more of the following observations: increasing health service–seeking behavior; weight loss; tiredness; or a group of unspecific symptoms, which did not fit into any of the organ-specific established cancer investigation programs. A cancer prevalence of 16%–18% was found in patients investigated at DOC for NSSC in Denmark (9,10).
Patients referred to DOC for NSSC are initially screened for occult malignancy with a physical examination and laboratory evaluation. If malignancy still is suspected, conventional CT of the thorax and abdomen is performed (in >95% of the referred patients older than 40 y). However, the optimal cancer screening strategy in these patients remains unknown. Integrated PET/CT with the glucose analog 18F-FDG has proven to be of high diagnostic value in staging and restaging of different malignant diseases such as colorectal cancer, lung cancer, breast cancer, head and neck cancer, and malignant lymphomas (11–13). The standard whole-body coverage simplifies staging and speeds up decision making on appropriate therapeutic strategies, which promotes 18F-FDG PET/CT as the imaging modality of choice for workup in the most common tumor entities as well as some rare malignancies (13). 18F-FDG PET/CT is more accurate in detecting cancer and provides fewer equivocal findings than 18F-FDG PET alone, CT alone, or separately acquired 18F-FDG PET and CT studies in a head-to-head comparison (13). Although these studies have suggested that 18F-FDG PET/CT might be more sensitive and specific for cancer detection than either modality alone, few of these studies support that 18F-FDG PET/CT should be used for cancer screening (14–19). Accordingly, in a study of 2,911 asymptomatic subjects who underwent both 18F-FDG PET and other examinations for multiple organs, including CT, the detection rate of cancer with 18F-FDG PET was 1% and sensitivity, specificity, and positive predictive value of 18F-FDG PET to detect cancer were estimated to be 18%, 95%, and 11%, respectively (20). The detection rate of cancer by 18F-FDG PET was higher than that of other screening modalities. However, the high false-positive (FP) rate makes 18F-FDG PET screening less useful in the general population with a low prevalence of cancer (21–25). In the so far largest 18F-FDG PET screening study performed at 233 facilities with inclusion of 155,456 subjects, positive 18F-FDG PET findings suggesting possible cancer were found in 10.9% of the cases. However, on the basis of further investigations the true-positive (TP) rate (positive predictive value) was only 32.3% (26). Accordingly, this large-scale study clearly demonstrated that 18F-FDG PET had a far-too-high FP rate to be applied as screening of the general population.
A study examining the subgroup of patients with a malignancy and an unknown primary tumor found 18F-FDG PET/CT to be nonsuperior to conventional CT in the workup of identifying the primary tumor. Currently, 18F-FDG PET/CT is not recommended as the primary method for investigation in this group of patients (24). However, because the estimated prevalence of cancer in patients referred to DOC is approximately 10-fold higher than in the above-mentioned studies (9,10), the FP rate is expected to be substantially lower and 18F-FDG PET/CT cannot be ruled out as the best first-line imaging modality in a high-cancer-prevalence population. Furthermore, the most common noncancer findings in this population of patients are rheumatoid or infectious diseases for which 18F-FDG PET/CT has shown a better detection rate than routine CT (27).
The aim of this study was therefore, in a randomized prospective trial, to investigate whether 18F-FDG PET/CT was superior to CT as an initial imaging modality in NSSC, for which the prevalence of cancer is approximately 20%. The imaging modalities were compared with regard to diagnostic performance and the time from referral to adjudication of a diagnosis.
MATERIALS AND METHODS
Participants
Design
Two hundred consecutive patients were prospectively recruited at their first visit at the DOC, Hvidovre University Hospital, between August 14, 2013, and April 30, 2014. The criterion for referral to DOC was a suspicion from the referring physicians that the patient had an NSSC. The referral was prompted by one or more of the following observations: increasing health service–seeking behavior; weight loss; tiredness; or a group of unspecific symptoms, which did not fit into any of the organ-specific established cancer investigation programs. Inclusion criteria were age 18 y or older and signed informed consent. Exclusion criteria were pregnancy, including risk of pregnancy or lactation; alcohol or drug abuse hampering the ability to adhere to the protocol; claustrophobia; body weight above 150 kg; contraindications to CT due to allergy to contrast or impaired renal function defined as a P-creatinine level greater than 0.120 mmol/L; or deemed unfit due to performance status.
The patients were randomized at their first visit to either CT of the thorax and abdomen or 18F-FDG PET/CT based on a computer-generated list using a 1:1 ratio algorithm (GraphPad Software). Randomization was performed by a study nurse masked to patient history and before any laboratory testing.
Furthermore, patients were screened for disease with a physical examination and a laboratory evaluation. The 18F-FDG PET/CT or CT in combination with results from clinical laboratory testing guided the clinicians in diagnostic decisions. Experienced certified radiologists and nuclear medicine physicians evaluated the PET, fused PET/CT, and CT images side by side and a consensus was reached. All the CT scans of the thorax and abdomen were evaluated by the same experienced certified radiologist. All 18F-FDG PET/CT or CT scans were furthermore discussed at a multidisciplinary conference with the participation of the following board-certified specialist physicians: endocrinologist, gastroenterologist, nuclear medicine physician, radiologist, and an infection disease specialist. Oncologists were not part of the multidisciplinary conference team. However, if a malignant diagnosis was established or deemed most likely, then patients were referred to oncologists.
A total of 200 patients were randomized. A preliminary tentative diagnosis based on initial imaging and routine laboratory testing was given at the multidisciplinary conference when results of the 18F-FDG PET/CT or CT scans were available. A final referral diagnose was adjudicated after the patients had finished their full investigational program for disease at the DOC.
Ethics
All patients received oral and written information and gave written consent before inclusion in the study. The study was approved by the Scientific Ethics Committee of The Capital Region of Denmark (protocol no. H-4-2013-063) and complied with the declaration of Helsinki and Danish legislation.
PET/CT Imaging
After patients had fasted for at least 6 h, 18F-FDG (4 MBq/kg; range, 184–444 MBq) was injected intravenously, followed by a median resting uptake period of 71 min (intended, 60 min; range, 57–123 min). Blood glucose levels were tested in all patients before injection of 18F-FDG to ensure levels were below 7 mmol/L, which was the case in all patients.
The first 50 of the 18F-FDG PET/CT scans were obtained on a PET/CT scanner (Biograph 40; Siemens) at Rigshospitalet. For the remaining 18F-FDG PET/CT scans, a Biograph mCT 128 4R scanner (Siemens Healthcare) was used at Hvidovre Hospital. All patients were scanned from the vertex to the proximal femora. The CT examination was enhanced by iodinated contrast agent given orally (Optiray [Covidien], 300 mg of iodine/mL, 20 mL in 500 mL of water 30 min before start) and intravenously (100 mL, 5 mL/s immediately before start). Depending of the weight of the patient, PET emission data were acquired for 2.5–5 min at each of 6 or 7 axial bed positions immediately after acquisition of the diagnostic CT images. Patients were instructed to breathe normally and were immobilized using cushions. PET data were reconstructed using 3-dimensional ordinary Poisson ordered-subset expectation maximization with resolution modeling (point-spread function), with 2 iterations and 21 subsets. Time of flight was used for the mCT scans. PET data were corrected for decay, scatter, and random events and attenuation corrected using the CT data. PET and fused PET/CT images were displayed on Siemens syngo.via workstations for analysis.
CT parameters were a tube potential of 120 kV, 2-mm slices with a collimation of 1.2 mm × 24, pitch of 0.8, CareDose4D on, quality reference mAs of 170, and varying tube current for dose reduction. CT data were reconstructed using filtered backprojection with a B40f medium kernel, slice increment of 1.0 mm, and 2-mm slices. CT images were reviewed on a PACS (Impax 5.3; AGFA Health Care). Images were interpreted according to clinical routine and reported as indicative of malignancy or not.
Experienced radiologists and nuclear medicine physicians in teams of 1 radiologist and 1 nuclear medicine physician evaluated the PET, fused PET/CT, and CT images side by side, and a consensus was reached. For malignant findings, interpretation included suggestion of potential primary tumor and the number of metastatic sites. Thus, a PET-negative but obviously malignant-looking tumor seen on the CT part of the PET/CT scan would be defined as a positive lesion, and an 18F-FDG PET–positive lesion without clear anatomic CT substrate was classified as negative. A written report on the PET/CT consensus was produced. The effective radiation dose for the 18F-FDG PET/CT scan was approximately 16 mSv, with 8 mSv from the 18F-FDG dose and 8 mSv from the CT scan.
Conventional CT
The diagnostic CT was performed with intravenous contrast enhancement (iomeron, 350 mg/mL; 1.2 mL/kg; flow rate, 4 mL/s). The CT scan was obtained with a multidetector CT scanner (4–64 slides; Brilliance [Philips Healthcare]). CT parameters were 120 kV and a reference of 225 mAs, using 3-mm-thickness scanning. All patients were scanned from the apex of the lungs to the proximal femora. The radiation dose from the CT scan was approximately 8 mSv.
Statistics
Continuous variables were compared between groups using the t test for independent samples whereas the Fisher exact test was used for categoric variables. A P value of less than 0.05 was considered significant. The sample size was based on the ability to demonstrate a difference between the expected PET/CT specificity of 95% and the expected CT specificity of 85%, with a type I error of 5% and a power of 70%. All statistical analyses were performed using SPSS 22 (IBM SPSS Statistics for Windows, version 22.0; IBM Corp.).
RESULTS
Patient Characteristics
Two hundred patients were randomized to either 18F-FDG PET/CT or CT as a first-line imaging modality. Three patients withdrew consent before being scanned. Accordingly, a total of 95 patients underwent 18F-FDG PET/CT, and 102 patients underwent CT (Fig. 1). Patient characteristics are summarized in Table 1. No significant differences were found regarding sex or age of patients randomized to 18F-FDG PET/CT versus conventional CT as a first-line imaging modality. Most of the patients were refereed to DOC from their general practitioner (78%). Referral diagnosis was suspicion of malignant disease (48%), weight loss (34%), suspicion of infection (2%), or other symptoms (16%). No difference in symptoms at referral was found between patients randomized to 18F-FDG PET/CT versus CT.

Flowchart of the study.
Baseline Characteristics of Patients (n = 197) Included in the Study
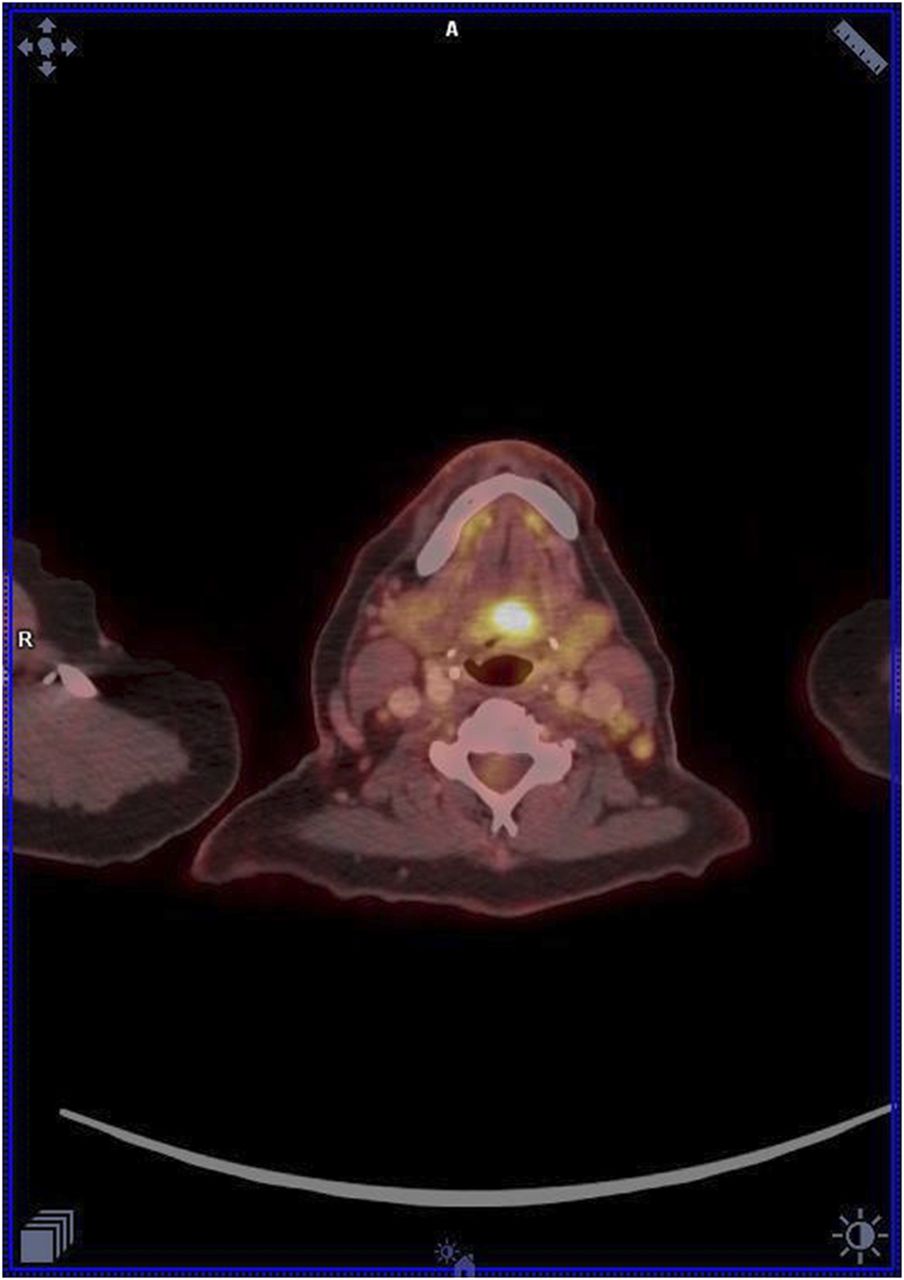
After the initial scan and a multidisciplinary conference, 18 (19%) of the patients randomized to 18F-FDG PET/CT were found to most likely have a malignant diagnosis compared with 26 (25%) in the group of patients investigated with CT as a first diagnostic modality. For 18F-FDG PET/CT, the image findings indicative of malignancy were lung cancer (5, of which 2 were disseminated), mammary cancer (1 localized and 1 disseminated), 2 sarcomas in the pelvic region, head and neck cancer (2) (Fig. 2), pancreatic cancer with carcinomatosis (1), esophageal cancer (1), rectal cancer (1), lymphoma (1), multiple bone metastases (1; most likely prostate cancer), and disseminated cancer with unknown origin (2). For CT only, the findings indicative of malignancy were lung foci (8), hepatobiliary metastases (7), bone metastases (3), enlarged lymph nodes (2), mammary tumor (1), pancreatic tumor (1), gynecological cancer (1), colon cancer (1), adrenal tumor (1), and disseminated cancer (1).
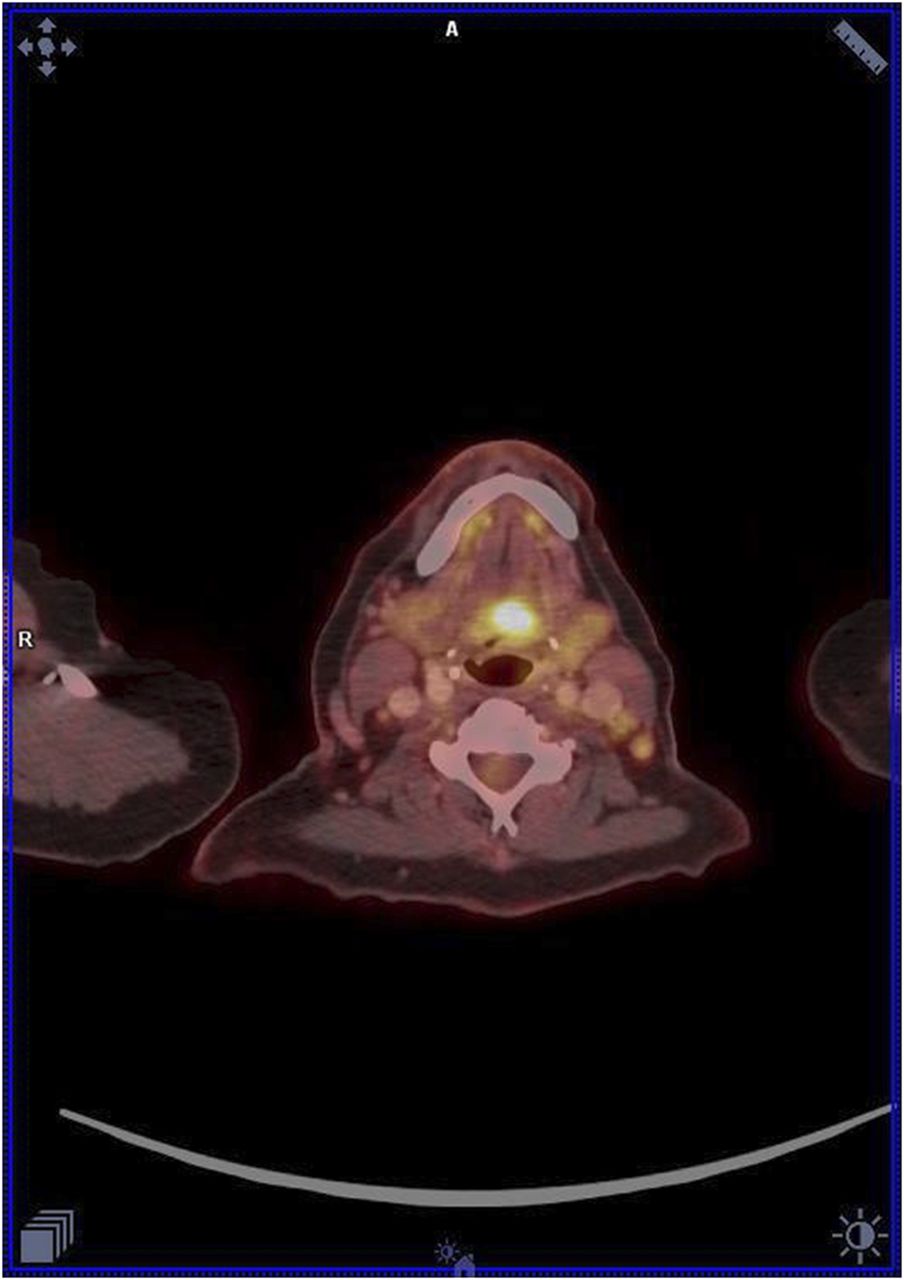
A 59-y-old woman, admitted to DOC due to weight loss of 5 kg, nausea, and diffuse pains in neck region. Tumor in oropharynx was visible on 18F-FDG PET/CT. Patient was diagnosed with cancer of the tongue.
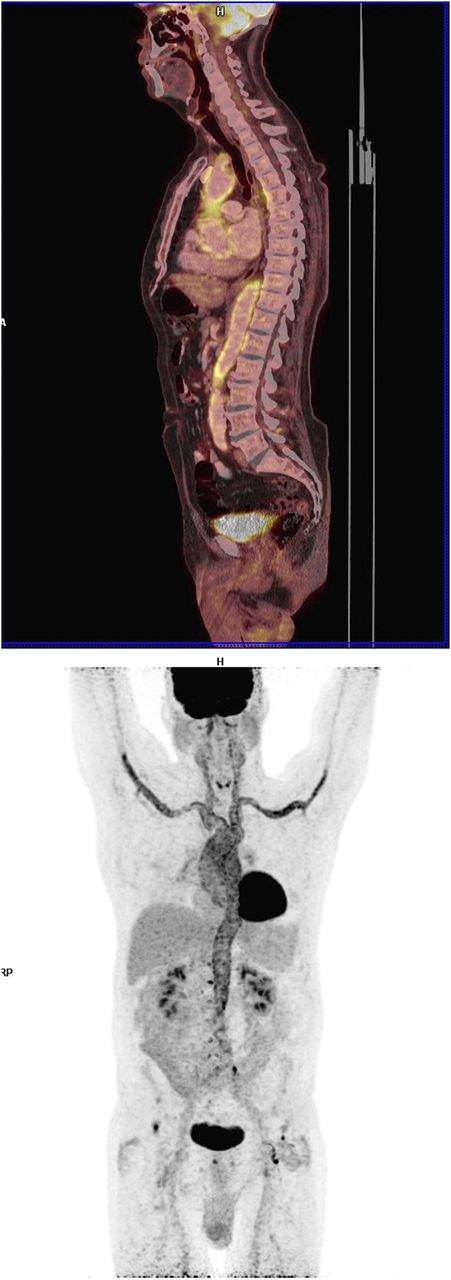
Infection was suspected on 5 18F-FDG PET/CT scans (3 pneumonia and 2 pharyngitis) and on 3 CT scans (2 pneumonia and 1 diverticulitis). Connective tissue disease was suspected on 3 18F-FDG PET/CT scans (2 sarcoidosis and 1 vasculitis) (Fig. 3) but not on any of the CT scans. Normal scans with neither malignant nor benign pathology were reported in 49 (52%) of the 18F-FDG PET/CT scans whereas this was the case in only 33 (32%) of the CT scans. Further investigations performed at the DOC after the initial scans in the patients suspected of malignant disease are listed in Table 2. A total of 26 additional procedures were performed in the 18F-FDG PET/CT group compared with 41 in the CT group.
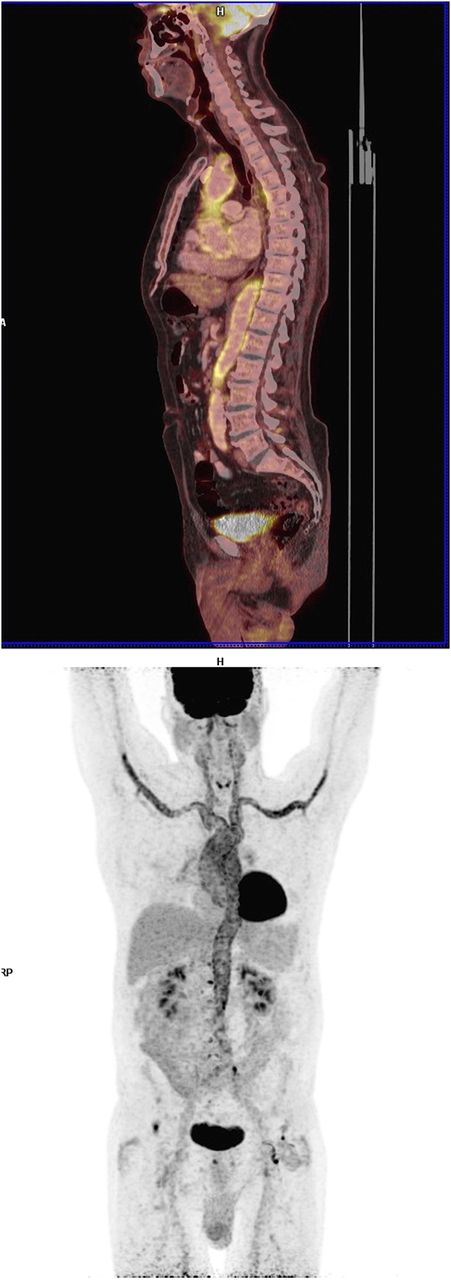
A 77-y-old man, admitted to DOC due to weight loss of 4 kg, tiredness, anemia, and chest pain. Erythrocyte sedimentation rate elevated to 58 mm. 18F-FDG PET/CT showed increased 18F-FDG uptake in vessel walls, and patient was diagnosed with large vessel vasculitis. Good clinical response to prednisolone.
Additional Examinations Performed at DOC in Patients Suspected of Malignant Disease Based on First-Line Imaging Modality
The final referral diagnoses established in the 197 patients are listed in Table 3. The final referral diagnosis is based on a clinical approach using data obtained from all examinations. A total of 39 patients (20%) were diagnosed with cancer, whereas 10 (5%) were diagnosed with infections: hepatitis C (n = 3), pharyngitis (n = 2), HIV (n = 1), pneumonia (n = 1), urinary tract infection (n = 1), Clostridium difficile gastroenteritis (n = 1), and diverticulitis (n = 1). A diagnosis of an autoimmune disease was established in 15 (8%). In 57 (28%) of the cases, patients were discharged from the DOC without any specific disease found. No difference between patients investigated with 18F-FDG PET/CT or CT was seen.
Final Referral Diagnosis in Patients Included in Study
Diagnostic Performance of PET/CT Versus CT for Detection of Cancer
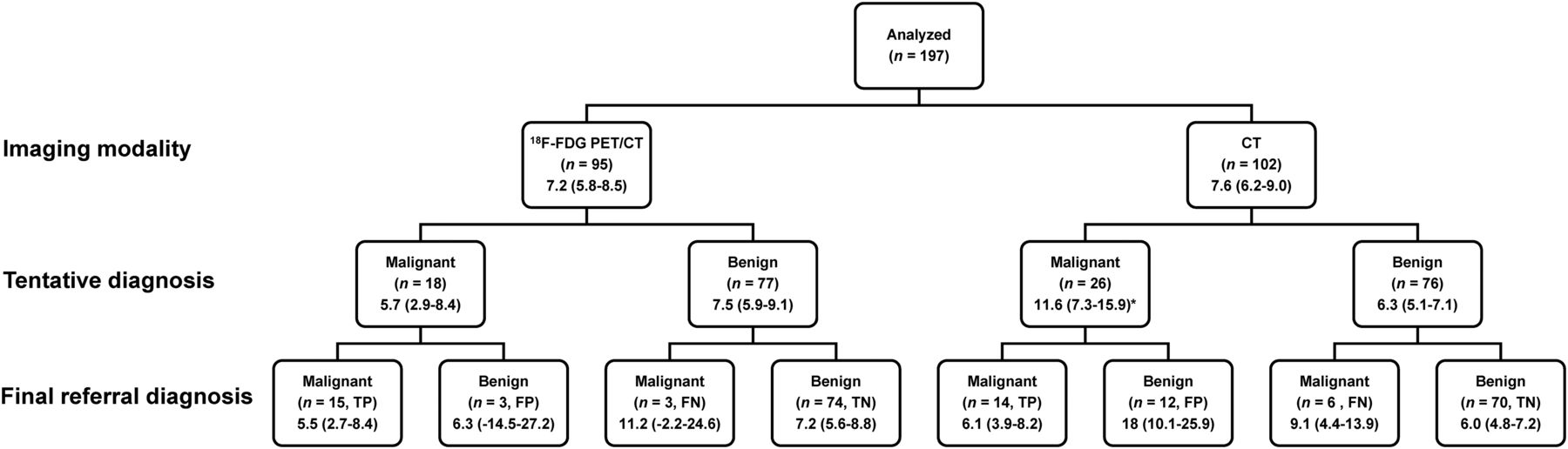
The results of 18F-FDG PET/CT and CT are shown diagrammatically in Figure 4. In brief, of 95 18F-FDG PET/CT scans, 15 (16%) were TP, 74 (78%) were true-negative (TN), 3 (3%) were FP, and 3 (3%) were false-negative (FN) with regard to the detection of cancer. For the 102 CT scans, 14 (14%) were TP, 70 (69%) TN, 12 (12%) FP, and 6 (6%) FN with regard to the detection of cancer.

Number of days to adjudication of final referral diagnosis according to randomization group (row 2; imaging modality) and results of 18F-FDG PET/CT or CT (row 3; tentative diagnosis). All numbers are given as mean with 95% confidence intervals in parenthesis. TP = true positive; FP = false positive; FN = false negative; TN = true negative.
The 3 patients found to be FN with 18F-FDG PET/CT were, based on further investigation, diagnosed with cancer coli (n = 2) and hepatocellular carcinoma (n = 1). Regarding CT as a first-line imaging modality, the 6 FN patients were diagnosed with colon cancer (n = 2), gastric cancer (n = 1), gallbladder cancer (n = 1), and chronic lymphocytic leukemia (n = 2). The 3 patients diagnosed as FP with 18F-FDG PET/CT were after the final workup diagnosed with a benign uterus fibroma, benign angiofibroma, and a Warthin tumor. Regarding the 12 patients classified as FP with CT as a first-line modality, patients were diagnosed with liver cirrhosis (n = 4), unspecific reaction in lymph nodes (n = 3), lipoma in the liver (n = 1), pneumonia (n = 1), sarcoidosis (n = 1), esophagus stricture (n = 1), or enlarged adrenal glands (n = 1).
The diagnostic performance for the detection of cancer of 18F-FDG PET/CT and CT as initial diagnostic imaging modalities is summarized in Table 4. Compared with CT, 18F-FDG PET/CT had a higher specificity (96% vs. 85%; P = 0.028) and a higher accuracy (94% vs. 82%; P = 0.017). However, there were no statistically significant differences in the sensitivity (83% vs. 70%) or negative predictive values (96% vs. 92%). The positive predictive value was borderline significantly higher in the 18F-FDG PET/CT group than the CT group (83% vs. 54%; P = 0.057). Overall, the better diagnostic performance in the PET/CT group compared with the CT group was driven by a much lower (3 vs. 12) number of FP cases.
Comparison of Diagnostic Performance of 18F-FDG PET/CT Versus CT of the Thorax/Abdomen
Time to Diagnosis
The number of days to adjudication of a final referral diagnosis according to randomization group and results of 18F-FDG PET/CT or CT are shown diagrammatically in Figure 4. For the PET/CT and CT groups as a whole, no differences could be shown (7.2 vs. 7.6 d). However, for the subgroups in which the initial imaging modality showed a suggestion of malignant disease, there was a significantly longer time to final diagnosis in the CT group than in the 18F-FDG PET/CT group (11.6 vs. 5.7 d; P = 0.02). The long time to final diagnosis in the CT group was driven by an average of 18 d in the 12 FP patients.
DISCUSSION
The major finding of our study is that 18F-FDG PET/CT is superior to CT as the initial imaging modality in a population of patients referred to DOC with NSSC for which the true prevalence of cancer is 20%. The superiority of 18F-FDG PET/CT was due to a significantly higher specificity compared with that of CT for the detection of cancer. To the best of our knowledge, we are the first to demonstrate this in a randomized, prospective study.
In a previous study of 18F-FDG PET as the primary imaging modality, which was performed in a low-prevalence (1%) population, it was clearly demonstrated that 18F-FDG PET was of limited value because of the high FP rate (26). However, in the recently established nationwide DOCs in Denmark, the prevalence of cancer is much higher and around 16%–18% (9,10). Therefore, the FP rate will be much lower and 18F-FDG PET/CT potentially could be of value. In accordance with this, we found in our study a positive predictive value of 83%.
Currently, as standard workup in DOC, CT has been chosen as the initial imaging modality. However, this leads to relatively many FP cases that require secondary diagnostic procedures including second-line use of 18F-FDG PET/CT as seen in Table 2. Because of this, we hypothesized that in DOC it might be beneficial to use 18F-FDG PET/CT instead of CT as the initial imaging modality.
Indeed, our study seems to support this idea because 18F-FDG PET/CT was superior with respect to the diagnostic performance of CT, with a higher specificity and accuracy. The positive predictive value was 83% for PET/CT but only 54% for CT. The driver for the poorer performance of CT was, compared with 18F-FDG PET/CT, a high number of FP cases. These cases resulted in a long time to final diagnosis in the group initially suspected of having malignant disease based on CT. In addition, the high number of FP cases using CT led to an increased use of secondary diagnostic procedures (Table 2).
Because we obtained a diagnostic CT as part of the 18F-FDG PET/CT investigation and the scans were evaluated side by side by a radiologist and a nuclear medicine physician, it is probable that if low-dose CT is used the same performance is not to be expected.
It could be argued that our data are not generalizable and relate only to a Danish setting. However, first the concept of DOCs is now used in several countries in Europe. Moreover, our data are generalizable for any population enriched so the a priori probability of cancer is around 20%. From a cost-benefit point of view, it may be argued that 18F-FDG PET/CT is more expensive (16). However, the first-line use of 18F-FDG PET/CT instead of CT saved expensive additional procedures such as MRI and ultrasonography as well as secondary 18F-FDG PET/CT scans. When this increased use of additional procedures is combined with the almost 3 times longer time to final diagnosis of 18 d in the FP CT group, total costs may actually decrease using 18F-FDG PET/CT as a first-line imaging modality. However, the exact cost structure at the different institutions may influence the point of economical break-even. Regardless of economic factors, there are human costs of being falsely diagnosed with cancer and on average having an additional investigation for 18 d until proven not to have cancer.
CONCLUSION
With the results of the present study, implementation of 18F-FDG PET/CT as the first-line imaging modality instead of CT in NSSC patients referred to DOC should be considered. Nevertheless, additional randomized studies are encouraged to confirm our findings.
DISCLOSURE
Generous financial support from the John and Birthe Meyer Foundation, the Lundbeck Foundation, the Novo Nordisk Foundation, the Research Foundation of the Capital Region, the Research Foundation of Rigshospitalet, the Svend Andersen Foundation, the Arvid Nilsson Foundation, the Innovation Fund Denmark, and the Research Council for Independent Research is gratefully acknowledged. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank all patients for their participation and Bente Clausen and Jannie Laage-Petersen, Diagnostic unit, Department of Infectious Diseases, Copenhagen University Hospital, Hvidovre, for their skillful assistance. We thank the staff at Department of Clinical Physiology, Nuclear Medicine & PET for their kind help in performing the 18F-FDG-PET/CT scans.
Footnotes
Published online Jan. 12, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 9, 2016.
- Accepted for publication December 13, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Patients from general practice with non-specific cancer symptoms: a retrospective study of symptoms and imaging
- Diagnostic property of direct referral from general practitioners to contrast-enhanced thoracoabdominal CT in patients with serious but non-specific symptoms or signs of cancer: a retrospective cohort study on cancer prevalence after 12 months
- Randomized Trial on PET/CT Imaging Requires Adequate Follow-up